
Abstract
Abuse of older people (AOP) is a significant public health concern, and older adults with functional dependence may be particularly vulnerable to mistreatment. In this systematic review and meta-analysis, we searched 16 electronic databases without language restrictions to identify primary studies published from inception to December 17, 2024, reporting AOP prevalence estimates among functionally dependent older adults (aged ≥60 years) or comparative abuse risk versus independent counterparts. We included only studies assessing abuse occurring within the 1 year preceding data collection. Study quality was appraised using validated risk-of-bias instruments. The meta-analysis was restricted to self-reported data from community-dwelling older adults and employed random-effects models for synthesis. Sensitivity analyses and publication bias were thoroughly evaluated, and subgroup analyses along with meta-regression were conducted to explore heterogeneity. Institutional or proxy-reported studies are summarized separately. Of 14,124 records initially identified, 38 studies met inclusion criteria, with data for 15,782 BADL‑dependent, 3,756 IADL‑dependent, and 12,353 ADL‑dependent (dependence in at least one BADL or IADL item) older adults. In total, 28 studies provided data for prevalence meta-analysis and 20 for risk meta-analysis. The pooled prevalence of AOP was 26.2% (95% CI [18.1, 35.2]) for BADL dependence, 26.0% (95% CI [9.1, 47.8]) for IADL dependence and 23.2% (95% CI [14.5, 33.2]) for ADL dependence, with significant heterogeneity but no significant covariates. Compared with independent counterparts, BADL‑dependent (pooled AOR = 1.53, 95% CI [1.26, 1.85), IADL‑dependent (pooled AOR = 1.63, 95% CI [1.33, 1.98]), and ADL‑dependent elders (pooled AOR = 1.87, 95% CI [1.52, 2.30]) had higher odds of abuse. These findings underscore the urgent need for targeted interventions to prevent AOP and protect vulnerable, functionally dependent seniors.
Introduction
The explosive growth of the global elderly population has magnified the health and social challenges faced by older adults (WHO, 2024b). The Decade of Healthy Ageing: Baseline Report stresses that more than 142 million older people, or 14% of all people aged 60 years and over globally, are currently unable to meet all of their basic daily needs (WHO, 2020). Functional dependence in daily activities often leads to markedly reduced social participation (Lexin et al., 2019). Compared to independent older adults, they exhibit higher reliance on caregivers, lower ability to seek help or protect themselves, which may expose them to a greater risk of abuse (X. Q. Dong, 2015; W. Li, 2011; Pillemer et al., 2016). Meanwhile, caregivers of functionally dependent older adults often face overwhelming burdens, including physical exhaustion, emotional strain, low self-worth, lack of social activities, and limited access to social support, factors that may collectively trigger or exacerbate abusive behaviors (Lexin et al., 2019; Minfei, 2020). Multiple, multi-level factors have been shown to influence the risk of abuse among older adults who require assistance with activities of daily living (ADL) (Feng, 2011; Johannesen & LoGiudice, 2013; Orfila et al., 2018). Victim-level factors include marital status, poor physical health or frailty, low income or wealth, trauma or past abuse, functional dependence (requiring ADL assistance), psychiatric illness or psychological problems, problematic behavior, and cognitive impairment. Perpetrator-level factors include caregiver burden or stress, psychiatric illness or psychological problems, education level, and caregivers’ perception of aggressive behavior in the care recipient. Relationship- and social-level factors such as family disharmony or conflictual relationships and low social support are also important risk factors.
Abuse of older people (AOP), a serious yet often overlooked public health issue, has emerged as a major challenge that healthcare systems worldwide are striving to address (WHO, 2022). Yon et al. (2017) found that approximately one in six older adults globally have experienced any form of abuse in community settings in the past year. Kitaw et al. (2025) found large geographic variation in AOP prevalence, ranging from 0.7% to 90.4% across six continents, which may be attributable to differences in study design, cultural and social factors, and regional economic contexts. (Cooper et al., 2008), in a best evidence synthesis, found that over 6% of the older general population reported significant abuse in the last month, one-quarter of dependent older adults reported severe psychological abuse, and one in five dependent patients presenting to emergency departments experienced neglect. (Johannesen & LoGiudice, 2013) identified functional dependence as a risk factor in general population studies, for example, OR = 1.30 and OR = 4.39. In Dong’s systematic review, odds ratios for the association between physical functional impairment and AOP ranged from 0.67 to 13.53 (X. Q. Dong, 2015). With rapid population ageing, AOP is expected to increase (WHO, 2024a). Affecting millions globally, AOP carries severe social, economic, and health consequences (Pillemer et al., 2016). Abusive behavior poses a severe threat to the health of older adults, potentially triggering emotional issues and post-traumatic stress disorder (PTSD), as well as increasing the risks of suicide, mortality, morbidity, and healthcare utilization (X. Dong & Simon, 2013; Nobels et al., 2023; Santos et al., 2019; Yunus et al., 2019). Moreover, AOP imposes a substantial drain on healthcare resources. Victims of AOP have higher risks of hospitalization, increased annual emergency department visits and greater utilization of behavioral health services compared with non-abused peers (X. Dong & Simon, 2013; Schonfeld et al., 2006; Yunus et al., 2019). This phenomenon may place additional financial strain on society and result in medical resources wastage (X. Dong & Simon, 2013). Functionally dependent older adults who experience abuse are likewise subject to these adverse outcomes, and abuse may further exacerbate the severity of their functional dependence (Wong & Waite, 2017a). Yet it remains a low global priority, receiving limited attention from international and national organizations and relatively few resources (WHO, 2022).
Definitions of Functional Dependence and AOP
Functional dependence refers to an individual’s inability or difficulty in performing the daily tasks required for independent living in a social environment (Kelley-Moore et al., 2006), and is typically measured by basic and/or instrumental activities of daily living (BADL, IADL). In this study, functional dependence was classified into three categories: BADL, IADL, and ADL. BADL dependence was defined as the inability to independently perform at least one of the following tasks: feeding, dressing, toileting, bathing, mobility, transferring between bed and chair, grooming, climbing stairs, bowel control, and bladder control (Mahoney & Barthel, 1965). IADL dependence was defined as the inability to independently perform at least one of the following tasks: food preparation, shopping, housekeeping, laundry, financial management, using of telephone, using of transportation, and medication management (Lawton & Brody, 1969). ADL dependence was defined as dependence in at least one BADL or IADL item. According to the WHO, AOP, or elder abuse (EA), was defined as a single or repeated act, or lack of appropriate action, occurring within any relationship where there is an expectation of trust, which causes harm or distress to an older person (WHO, 2024a). The U.S. Centers for Disease Control and Prevention has defined six common subtypes of AOP, namely physical abuse, psychological or emotional abuse, financial abuse, sexual abuse, and neglect (National Center for Injury Prevention and Control (U.S.). Division of Violence Prevention, 2015). Overall abuse encompasses any combination of the abuse subtypes reported in the studies.
Aims, Objectives, and Research Questions
In recent years, multiple studies have identified functional dependence as a significant risk factor for AOP (X. Q. Dong, 2015; Storey, 2020; WHO, 2024a). However, quantitative syntheses of this issue remain scarce. To address this gap, we formulated the research question using a PEO framework: Among community-dwelling older people with dependence in BADL, IADL, or ADL, what are the pooled prevalence estimates of AOP and its subtypes? Understanding of the magnitude of AOP against affected groups is the first step in the public health approach to violence prevention (Krug et al., 2002). Therefore, we conducted a systematic review and meta-analysis of existing global studies to: (a) estimate the past-year prevalence of major abuse types (overall, physical, psychological or emotional, financial, sexual, neglect) among functionally dependent older adults population worldwide; (b) compare risk of abuse between functionally dependent and independent older adults. This study aims to provide robust epidemiological evidence to inform targeted interventions, policy, and resource allocation for this high-risk group, thereby supporting the United Nations Decade of Healthy Ageing 2021–2030.
Methods
Search Strategy and Selection Criteria
The reporting of this systematic review and meta-analysis conformed to the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) 2020 guideline (Page et al., 2021). A comprehensive search was performed in the following 16 academic databases from inception to December 17, 2024: PubMed, EMBASE, CINAHL, PsychINFO, Web of Science Core Collection, Cochrane, ProQuest Criminal Justice, Nursing & Allied Health, Public Health Database, Publicly Available Content Database, Social Science Database, Sociology Database, Dissertations & Theses Global, CNKI, Wanfang Data, ERIC. An adaptive search strategy was devised for each database by combining free-text keywords with controlled vocabulary (i.e., MeSH terms). No language restrictions were applied to either the search process or its resulting records. Some of the search terms include: “disabl*,” “disabilit*,” “amputee*,” “handicapped,” “activities of daily living,” “ADL,” “dysfunction*,” “dependen*,” “elder*,” “older adults,” “aged,” “senior*,” “frail elderly,” “elder abuse,” “elder neglect,” “elder mistreatment,” “elder maltreatment,” “domestic violence,” “intimate partner violence,” “abus*,” “neglect,” “maltreat*,” “mistreat*,” “aggression,” “aggressive behavior,” “assault,” “violen*,” “crime,” “prevalence,” “incidence,” “epidemiology,” “morbidity,” “rate.” Search terms and database selection were informed by prior meta-analyses (Hughes et al., 2012; Yon et al., 2017; Zhang et al., 2022). We ran pilot searches to optimize the strategies, consulted a research librarian, and finalized the search based on co-author feedback. Detailed search strategies for each database are presented in appendix (p1–11). We reviewed reference lists of relevant papers to identify additional studies. For relevant gray literature records identified (e.g., government publications, conference abstracts), we conducted targeted web searches to verify whether full texts were available.
Screening at all stages was conducted independently by two reviewers, including the search, title and abstract screening, full-text screening, and manual retrieval. Following the search, all identified records were imported into EndNote version 21, duplicates were removed, and the remaining records were screened according to prespecified inclusion and exclusion criteria. Any discrepancies were resolved through discussion with the third reviewer. For studies with overlapping data sources (e.g., when multiple studies utilize data from the same survey), we selected the one providing the most comprehensive data for further synthesis. However, we retained all studies that used the same data source yet reported different types of abuse to enable further analysis by abuse type.
Studies included in this systematic review and meta-analysis must meet the following criteria: (a) be cross-sectional, case-control, or cohort (including longitudinal) studies; (b) define older adults as individuals aged 60 years and above (WHO, 2015); (c) assess abuse against functionally dependent older adults or measure AOP while providing subgroup data on functionally dependent individuals; (d) report measurement methods used to assess AOP and functional dependence (subjective measures, validated or non-validated instruments, or single-item questions were acceptable); (e) report the types of AOP and functional dependence; (f) report prevalence or adjusted odds ratios (AORs), or supply raw data for recalculation; (g) assess abuse occurrences within the past-year period preceding the study. This final criterion was intended to minimize reverse causality risks (i.e., individuals who became functionally dependent as a result of abuse). However, compared to lifetime prevalence, focusing solely on recent prevalence may yield lower estimated rates.
Studies conducted in community settings and based on self-reported data from older adults were included in the primary meta-analysis. Studies set in institutions or relying on proxy-reported data were summarized descriptively. We excluded studies without available full texts, and those focusing on self-neglect, homicide, or on specific populations (e.g., immigrant ethnic minorities, homeless or prison populations, or individuals with substance use disorders). For the review on abuse risk, we further excluded studies that treated functional dependence as a continuous variable or used other functional dependence types as control or historical populations.
Data Extraction and Quality Assessment
Two reviewers independently extracted data and assessed the risk of bias, with cross-checking to ensure accuracy. Any discrepancies were resolved through consensus discussions with a third reviewer. A standardized data extraction form was developed to capture the following information: author, year, country, WHO region, study design, data collection method, sampling approach, data source, characteristics of the study population, number of events, total sample size, type of functional dependence, type of abuse, measurement instruments and time frames, as well as the prevalence or proportion of AOP within the population. To estimate comparative risk, we also extracted AORs along with their standard errors (SE) or confidence intervals (CI) comparing abuse risk among functionally dependent versus independent older adults. We made repeated attempts to contact the authors of the relevant studies to obtain additional information, thereby supporting a rigorous review and analysis.
Because some studies reported AOP data for both BADL- and IADL-dependent elders, we conducted separate meta-analyses for BADL, IADL, and ADL dependence to maintain statistical independence, rather than pooling all three. Our primary outcomes of interest were overall abuse and its specific subtypes, namely physical abuse, psychological/emotional abuse, financial abuse, sexual abuse, and neglect. Proxy reporters such as caregivers, knowledgeable relatives, or institutional staff may only disclose abuse cases they perceive as “severe” or socially acceptable, potentially overlooking or deliberately concealing less obvious or covert incidents. To mitigate this potential source of bias, we conducted a separate analysis for data obtained from proxy reports.
For studies reporting abuse prevalence, two independent reviewers assessed study quality using Hoy’s risk of bias tool (Hoy et al., 2012). The tool comprises 10 items plus a summary assessment and was specifically designed for population-based prevalence studies. Total scores were categorized as low risk (8–10), moderate risk (5–7), or high risk (0–4) (Hertanti et al., 2025). For studies providing AORs of abuse, quality was independently evaluated by two reviewers using the Agency for Healthcare Research and Quality (AHRQ) scale, which comprises 11 items; total scores of 8–11 indicated high quality, 4–7 moderate quality, and 0–3 low quality (Rostom et al., 2004). The Grading of Recommendations, Assessment, Development and Evaluation (GRADE) framework was used to assess the certainty of the main pooled evidence. The framework rates the certainty of evidence as high, moderate, low, or very low, based on five downgrading domains and three upgrading factors (Foroutan et al., 2020; Schünemann et al., 2024).
Data Analysis
Data analyses were performed using Stata MP version 18. For studies reporting prevalence, we first extracted the raw event counts and corresponding total sample sizes to calculate each study’s prevalence rate. To stabilize the variances across studies, these proportions were transformed using the Freeman–Tukey double arcsine method. Subsequently, the transformed proportions were pooled using a random-effects model, with between-study heterogeneity (τ²) estimated via the Restricted Maximum Likelihood (REML) approach (Borenstein et al., 2009). The pooled result was then back-transformed to obtain the overall prevalence estimates, and the 95% confidence intervals were calculated using the Wilson method (Newcombe, 1998). Similarly, we used random‑effects models to calculate pooled AORs and 95% CIs comparing the risk of AOP in functionally dependent versus independent older adults. Meta-analyses were stratified by AOP subtypes and functional dependence types.
Heterogeneity across studies was assessed using the Q test and the I² statistic. To ensure the robustness of our findings, sensitivity analyses were conducted for each meta-analysis with ≥10 studies. Galbraith plots and funnel plots were generated to visually inspect publication bias, and both Egger’s and Begg’s tests were used to quantitatively evaluate the bias risk (with a p-value <.05 indicating significant publication bias). In instances where publication bias was detected, Duval and Tweedie’s Trim and Fill method was employed to further examine the funnel plot and assess the impact of the bias on the overall results (Duval & Tweedie, 2000).
Subgroup analyses were done to investigate sources of heterogeneity. Additionally, we conducted univariable meta-regressions with the Knapp-Hartung adjustment to reduce the risk of false-positive findings associated with heterogeneity and small sample sizes. We assessed the association of the following covariates with the pooled estimates: WHO region (Americas vs. rest of the world); country income classification (high-income vs. middle-income countries); data collection method (face-to-face vs. all others); sampling procedure (probability vs. non-probability sampling); study quality (high vs. moderate); sample size (N < 200 vs. N ≥200 for prevalence studies; N <1,000 vs. N ≥1,000 for risk studies); BADL measure (validated instruments vs. non-validated questions); and AOP measure (validated instruments vs. non-validated questions). Covariates that were statistically significant and relevant were subsequently entered into a multivariable meta-regression model. This study has been prospectively registered with the International Prospective Register of Systematic Reviews (PROSPERO) under the registration number CRD420250633309.
Results
A total of 14,124 records were retrieved through searches in 16 databases supplemented by additional methods. After deduplication, title and abstract screening, and full-text evaluation, 111 relevant articles were identified. Among these, three studies used the same datasets as other investigations, eight studies did not provide appropriate data, 60 studies either failed to specify a timeframe or provided data from varying periods (e.g., the past 1, 3, or 6 months, since age 60, or over a lifetime), 1 study focused on a special population, and 1 study did not specify the assessment tool for functional dependence. After excluding ineligible studies, 38 studies met the inclusion criteria, all employing a cross-sectional design. Among these, 33 provided prevalence data on abuse among functionally dependent older adults, and 22 studies reported AOR comparing abuse risk between functionally dependent and independent older adults (Supplemental Figure 1).
The 38 included studies encompassed data from 15 countries worldwide (Supplemental Table A). Geographically, the WHO Americas region was strongly represented with 17 studies; the Western Pacific region provided eight studies; the Southeast Asia region contributed six studies; the European region provided five studies; the Eastern Mediterranean region contributed two studies; and the African region provided one study. All studies were conducted in countries classified according to the World Bank income categories: 7 studies originated from lower-middle-income countries, 19 from upper-middle-income countries, and 11 from high-income countries, with one study based on combined data from high-income and lower-middle-income countries. In addition, 30 studies employed probability sampling methods, while the remaining 8 studies used non-probability sampling approaches. Data collection was predominantly carried out through face-to-face interviews (31 studies), with six studies employing telephone interviews and one study using a mail survey. In total of, 35 studies identified abuse through self-reports, while three relied on proxy reports. For measurement of functional dependence, 26 used validated instruments and 12 used non-validated questions. Most studies reported data for BADL-dependent older adults (n = 15,782), while IADL dependence (n = 3,756) and ADL dependence (n = 12,353) were less commonly reported. For AOP assessment, 23 studies used validated instruments and 15 used non-validated questions (Supplemental Table B). Among the 38 included studies, 34 were derived from community-based or nationally representative samples, 2 were conducted in hospital settings, 1 in a long-term care facility, and 1 encompassed both residential and institutional settings. According to Hoy’s tool, among the 33 prevalence studies, 2 achieved the maximum quality score, 25 were rated as low risk, and 8 were rated as moderate risk (Supplemental Table C). Additionally, using the AHRQ scale for the 22 risk studies, none reached the highest quality standard, 13 were rated as high quality, and 9 were rated as moderate quality (Supplemental Table D).
AOP Prevalence Among Community-Dwelling Older Adults with Functional Dependence
Figure 1 presents the meta-analysis results for overall abuse prevalence in the past year among different functional dependence types. For BADL dependence (n = 14,109), the estimated overall abuse prevalence was 26.2% (95% CI [18.1, 35.2]), with significant heterogeneity (I2 = 98.99%, τ2 = 0.17); for IADL dependence (n = 3,336), it was 26.0% (95% CI [9.1, 47.8]; I2 = 99.35%, τ2 = 0.37); and for ADL dependence (n = 8,962), the estimate was 23.2% (95% CI [14.5, 33.2]; I2 = 99.03%, τ2 = 0.09).
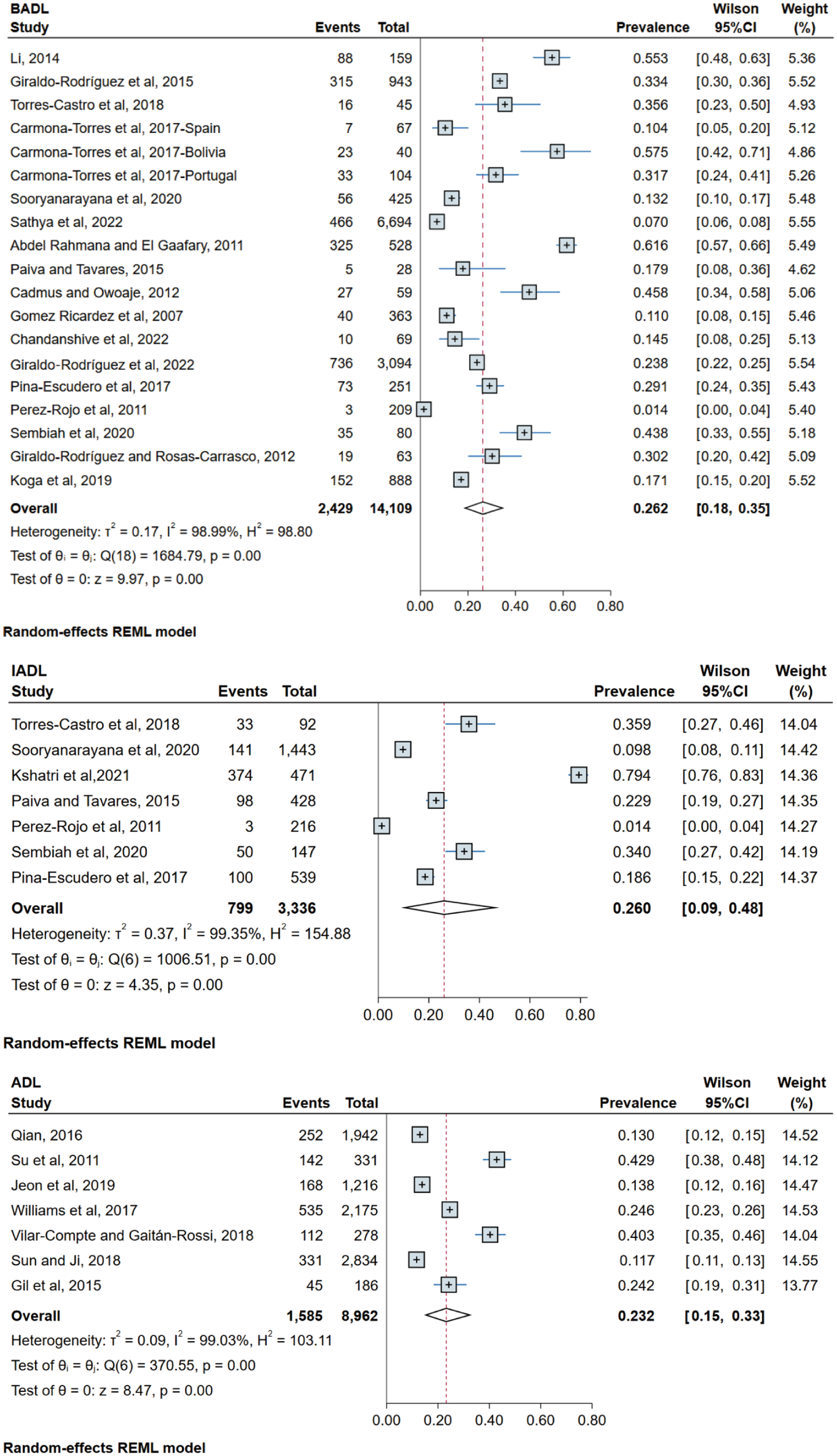
One-year prevalence of AOP among functionally dependent older adults.
We further examined pooled prevalence according to abuse subtypes for individuals with BADL, IADL, and ADL dependence (Table 1). For physical abuse, pooled prevalence among BADL-dependent individuals (n = 1,181) was 9.8% (95% CI [3.5, 18.5]), while for those with IADL dependence (n = 645), it was 7.8% (95% CI [5.6, 10.3]). For psychological abuse, pooled prevalence was 27.9% (95% CI [17.1, 40.1]) in the BADL group (n = 1,211) and 28.3% (95% CI [21.4, 35.8]) in the IADL group (n = 658). For financial abuse, pooled prevalence was 6.0% (95% CI [1.2, 13.8]) among BADL-dependent individuals (n = 1,127) and 21.5% (95% CI [0.0, 67.1]) among ADL-dependent individuals (n = 3,291). For neglect, pooled prevalence was 28.1% (95% CI [13.3, 45.6]) among BADL-dependent individuals (n = 270). In addition, we aggregated the overall abuse prevalence according to the severity of functional dependence (Supplemental Table E). The estimated overall abuse prevalence was 29.3% (95% CI [14.5, 46.6]) for individuals with moderate BADL dependence (n = 5,048) and 32.7% (95% CI [12.6, 56.2]) for severe BADL dependence (n = 2,684).
Pooled Prevalence Estimates of Abuse Subtypes Stratified by Functional Dependence Type.
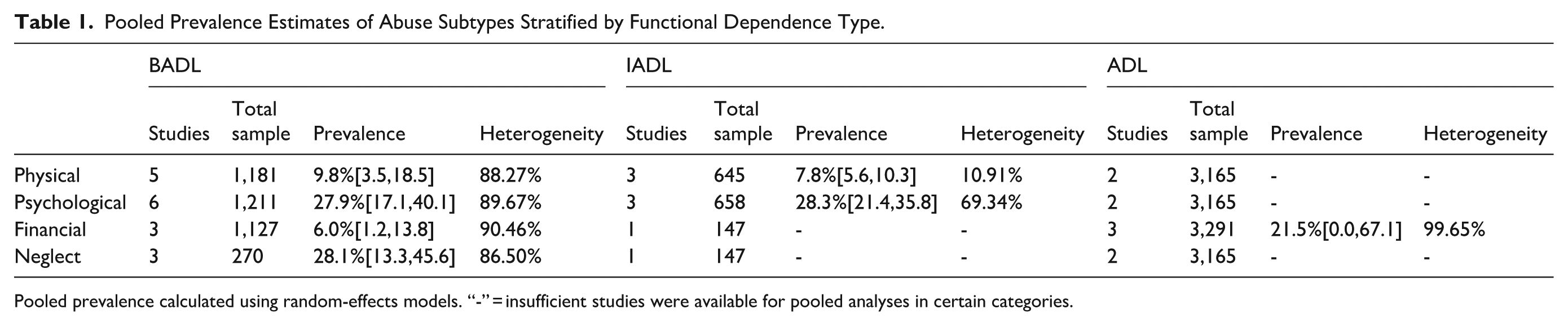
Pooled prevalence calculated using random-effects models. “-” = insufficient studies were available for pooled analyses in certain categories.
In the BADL-dependent group with >10 studies, Galbraith plots revealed no evidence of publication bias, and leave-one-out sensitivity analysis confirmed the robustness of the meta-analytic estimates (Supplemental Figures 2 and 3). Begg’s test (p = .944) indicated no significant publication bias, whereas Egger’s test (p = .049) detected potential bias (Supplemental Figures 4 and 5). Subsequent analyses using the trim and fill method showed that the estimates remained unchanged, confirming the stability of our findings (Supplemental Figure 6). To explore sources of heterogeneity, we conducted subgroup analyses (Supplemental Figure 7) and univariable meta-regressions for eight variables. Only the subgroup by data collection method showed a significant difference (Q[1] = 4.89, p = .03). Studies using face-to-face interviews reported higher AOP prevalence (26.8%) than other methods (17.1%). Given the limited number of studies, these findings should be interpreted cautiously. No covariates reached statistical significance in the meta-regressions, so we did not fit a multivariable meta-regression model. Nevertheless, subgroup analyses based on national income classification (Q[2] = 3.83, p = .147) showed prevalence estimates of 13% (95% CI [2.9, 28.6]) in high-income countries, 26.8% (95% CI [18.2, 36.3]) in upper-middle-income countries, and 36.1% (95% CI [17.5, 57.1]) in lower-middle-income countries (Supplemental Figure 8). Subgroup analysis by sampling procedure (Q[1] = 2.29, p = .13) revealed that studies employing probability sampling had a pooled prevalence of 22.4%, whereas those using non-probability sampling yielded a higher pooled prevalence of 38.3%. Additional subgroup analyses by sample size (Q[1] = 2.90, p = .09) revealed a pooled prevalence of 33.5% in studies with smaller samples (N < 200) compared to 19.6% in studies with larger samples (N ≥ 200).
Comparison of AOP Risks Between Community-Dwelling Functionally Dependent Versus Independent Older Adults
Figure 2 displays the meta-analysis results of AORs for AOP in the past year, comparing older adults with different types of functional dependence to independent older adults. Compared to the independent counterparts, significantly higher odds of experiencing AOP were observed among 8,494 individuals with BADL dependence (pooled AOR = 1.53, 95% CI [1.26, 1.85], I2 = 60.43%, τ2 = 0.04), 2,615 individuals with IADL dependence (pooled AOR = 1.63, 95% CI [1.33, 1.98], I2 = 0.00%, τ2 = 0.00), or 6,456 individuals with ADL dependence (pooled AOR = 1.87, 95% CI [1.52, 2.30], I2 = 59.04%, τ2 = 0.03). Based on the pooled estimates of AOR according to abuse subtypes and dependence types, functionally dependent older adults faced elevated risks across multiple abuse categories (Supplemental Table F). For physical abuse, the pooled AOR was 2.05 (95% CI [1.10, 3.81]) in those with ADL dependence and 1.89 (95% CI [1.30, 2.76]) in the overall functionally dependent group (only including BADL- or ADL-dependent group). In the case of psychological abuse, BADL dependence yielded an AOR of 1.49 (95% CI [0.89, 2.50]), ADL dependence an AOR of 1.68 (95% CI [0.88, 3.19]), and overall functional dependence an AOR of 1.58 (95% CI [1.08, 2.30]). For financial abuse, the pooled AOR was 1.75 (95% CI [1.08, 2.83]) for BADL dependence, and 1.87 (95% CI 1.45–2.41) for overall functional dependence. Neglect was associated with a pooled AOR of 4.99 (95% CI [1.52, 16.39]) among functionally dependent older adults.
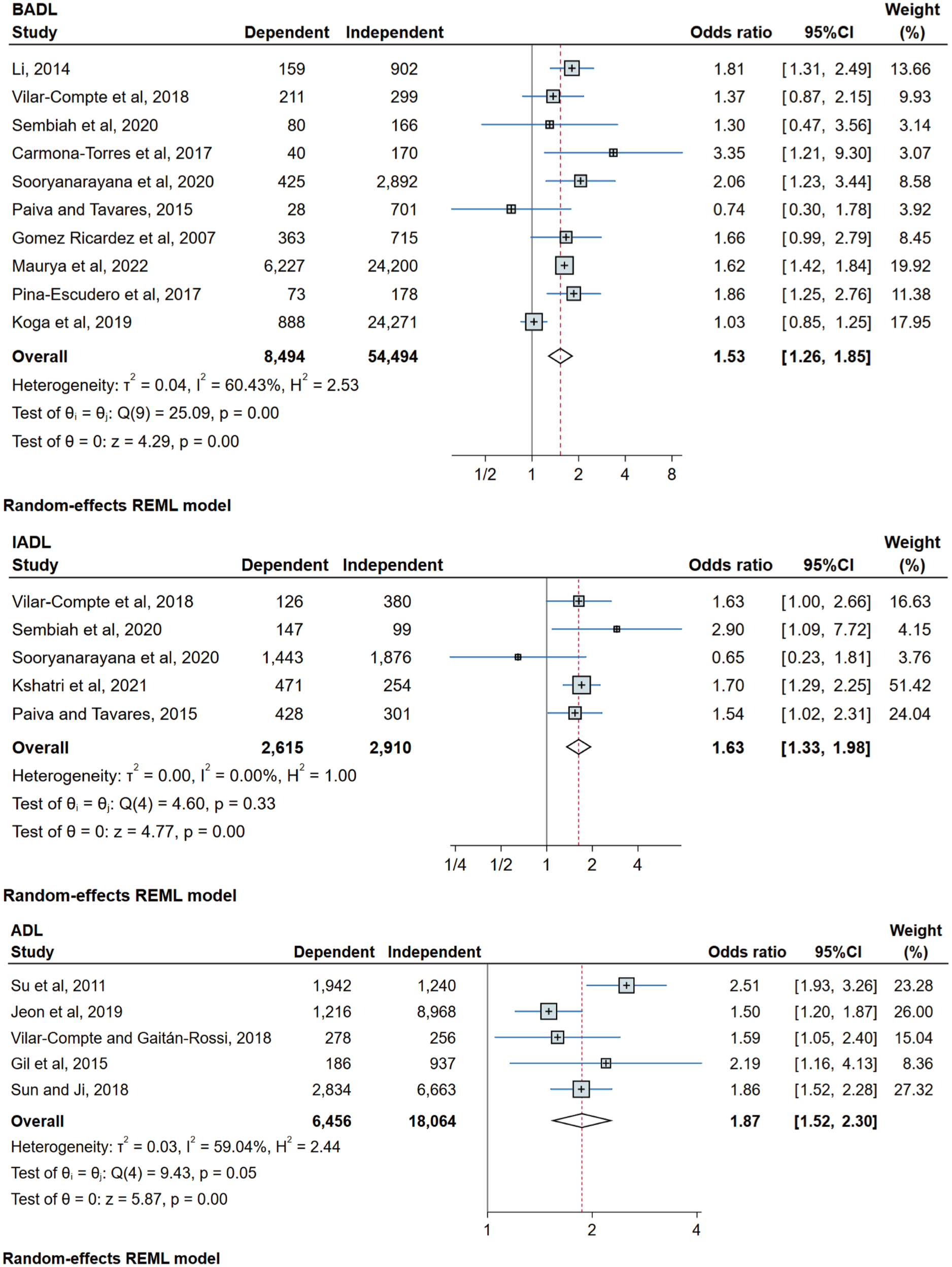
One-year risk of AOP among functionally dependent older adults.
For the 10 studies comparing BADL-dependent older adults with independent ones, visual inspection of the Galbraith and funnel plots revealed no evidence of publication bias, and leave-one-out sensitivity analyses confirmed the robustness of the meta-analysis (Supplemental Figures 9, 10, and13). Begg’s test (p = .721) and Egger’s test (p = .749) both indicated no significant publication bias (Supplemental Figures 11 and 12). To explore heterogeneity, we conducted subgroup analyses (Supplemental Figure 14) and univariable meta-regressions for eight variables. In univariable meta-regressions, country income (β = .47, p = .003), data collection method (β = −.47, p = .003), and BADL measure (β = −.47, p = .003) were significantly associated with AOR of AOP. Subgroup analyses gave consistent results. Because of collinearity among covariates and the small number of studies, we did not fit a multivariable meta-regression model. Studies from middle-income countries, using face-to-face interviews, or using validated instruments showed higher estimates (AOR = 1.65) than studies from high-income countries, using non-face-to-face interviews, or using non-validated questions (AOR = 1.03). Subsequently, we conducted sensitivity analyses (Supplemental Figure 15). After excluding one study that used non-face-to-face interviews, was from a high-income country, and used non-validated BADL questions, the pooled AOR was 1.65 (95% CI [1.49, 1.83], I² = 0.0%). Heterogeneity fell to 0.0%, suggesting that data collection method, country income, or BADL measure may explain the heterogeneity. The sensitivity estimate lies within the 95% CI of the primary analysis (1.26–1.85), confirming the robustness of the result.
Additional Descriptive Findings (Studies Not Included in Meta-Analysis)
Six studies were excluded from the meta-analysis because they were conducted in hospital or institutional settings, used proxy reports, or reported polyvictimization data, but they provide valuable contextual information. Supplemental Table G summarizes their characteristics and key findings.
Certainty of Evidence (GRADE)
The GRADE summary is provided in Supplemental Table H. Due to substantial heterogeneity and wide confidence intervals, the certainty of evidence for prevalence estimates was rated low to very low, whereas the certainty for pooled AORs was rated high to moderate. Heterogeneity was the main factor limiting evidence certainty.
Discussion
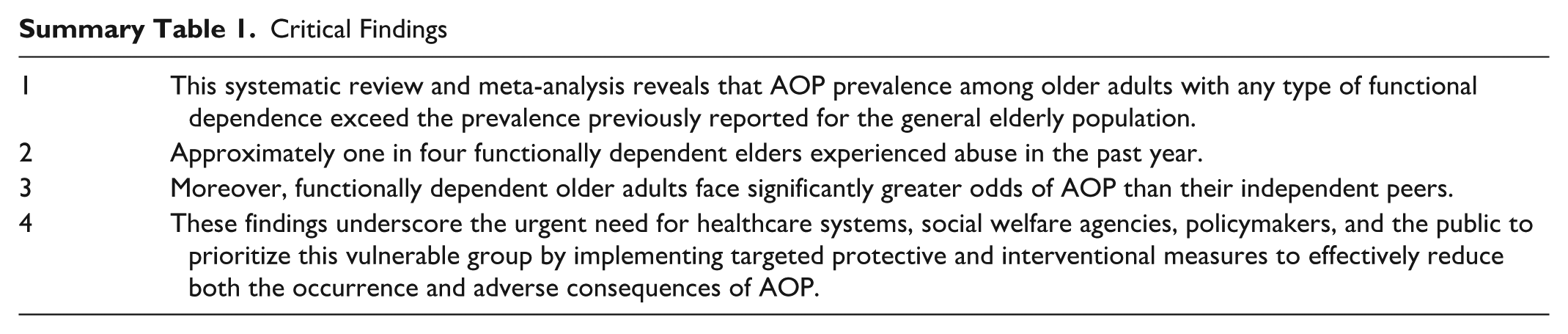
Although substantial evidence from multiple studies has identified functional dependence as a significant risk factor for AOP, no meta-analysis has yet been conducted to estimate the global prevalence and risk specifically for this vulnerable population (X. Q. Dong, 2015). As we know, this meta‑analysis offers the most comprehensive synthesis to date of AOP among functionally dependent older adults. First, the pooled prevalence of abuse in the past year was 26.2% for those with BADL dependence, 26.0% for IADL dependence, and 23.2% for ADL dependence, affecting approximately one-quarter of functionally dependent older adults. Second, compared with independent peers, functionally dependent older adults faced significantly higher odds of abuse, with pooled AORs of 1.53 for BADL dependence, 1.63 for IADL dependence and 1.87 for ADL dependence. However, the CIs are wide, especially for IADL, and overlap across groups. This may reflect imprecise estimates, limited sample sizes, or a lack of statistically significant differences. Although stratified meta-analyses by dependence type (BADL, IADL, ADL) yielded similar pooled prevalence and AOR estimates, these findings should be interpreted cautiously. According to the WHO’s Decade of Healthy Ageing: Baseline Report, as of 2020 at least 142 million older people (14% of all people aged 60 years and over globally) were dependent on ADL (WHO, 2020). This corresponds to approximately 33 million functionally dependent older adults experiencing abuse each year.
This study focused on functionally dependent older adults and found that the pooled prevalence of overall abuse for each of the three functional dependence categories exceeded the 15.7% (95% CI [12.8, 19.3]) reported by Yon and colleagues among general community-dwelling older adults. In Yon’s meta-analysis, psychological abuse was most common (11.6%), followed by financial abuse (6.8%), neglect (4.2%) and physical abuse (2.6%) (Yon et al., 2017). In our study, the meta-analysis of the most prevalent BADL-dependent group found that neglect likewise had the highest pooled prevalence (28.1%), followed by psychological abuse (27.9%), physical abuse (9.8%), and financial abuse (6.0%). This discrepancy may stem from the inherent characteristics of functionally dependent older adults. Functional dependence serves both as a marker of increased care needs and a potential driver of abuse: loss of independence undermines social engagement and autonomy, intensifies isolation and creates conditions conducive to mistreatment.
The association between functional dependence and AOP risk can be explained through multiple interrelated pathways. Functional limitations can reduce older adults’ sense of self-worth, undermining their ability to manage and resolve conflicts with family members (Gratão et al., 2013). Elderly individuals with functional disabilities have greater needs for assistance with self-care and more complex daily activities, which may in turn elevate caregiver burden and stress, thereby increasing the risk of mistreatment (Gratão et al., 2013; Sathya & Premkumar, 2020). Moreover, functional dependence often coexists with cognitive impairment, frailty or chronic illness (Kshatri et al., 2021; Piña-Escudero et al., 2021), compounding vulnerability by diminishing self-protection and self-advocacy capacities. It also may restrict older adults’ mobility, use transportation or seek support, leading to reduced social participation and further limiting their opportunities to report or escape abuse (Curcio et al., 2019). These factors collectively escalate the risk of AOP. Concurrently, functional dependence intensifies caregiver burden, especially under prolonged co-residential, high-intensity caregiving (Queiroz et al., 2010). Caregivers commonly experience physical and emotional exhaustion, emotional burnout, social isolation and diminished self-worth, and without professional training or external support, these factors can ultimately precipitate abusive behaviors. Functional dependence may also grant caregivers substantial control over elders’ mobility, finances, and daily routines, providing potential perpetrators with greater opportunities for AOP.
Social exchange theory proposes that social interactions tend toward balanced exchanges that satisfy both parties, with benefits and costs in equilibrium (Blau, 1964). When one partner has limited resources but rising needs, they become dependent on the other, and the other partner gains greater power in the relationship (Fundinho et al., 2021). That power can be exercised in many ways, including withholding necessary care, financial exploitation, or physical and psychological abuse, sometimes framed as a way to restore a perceived balance. BADL dependence involves intimate, sustained personal care and worsens need asymmetry because older adults cannot reciprocate equally. Self-care dependence increases close physical contact and gives caregivers direct control over daily activities. Loss of privacy and dignity may make older adults feel ashamed and less willing to seek help or report abuse. In practice, most BADL-dependent older adults also have IADL needs. IADL dependence gives caregivers or proxies control over instrumental resources and information, such as shopping, transport, and finances, and this control concretizes power into economic domination and decision-making authority, undermining the older person’s autonomy. Social exchange theory posits that AOP occurs in imbalanced relationships. Victims with low self-worth are unable to defend themselves, while perpetrators gain greater power through their caregiving role and can manipulate exchanges (Kong & Jeon, 2018). When power is imbalanced and social support is lacking, victims may become isolated or dependent on the more powerful party, perpetuating AOP.
Previous meta-analyses of AOP in the general population found that larger sample sizes, random sampling, and high-income country settings were associated with lower prevalence estimates (Yon et al., 2017). Although these factors were not independently significant in our analyses, we observed similar trends. Probability samples yielded a lower pooled prevalence (22.4%) than non-probability samples (38.3%). Large samples produced lower estimates (19.6%) than small samples (33.5%). Studies from high-income countries reported lower estimates (13%) than those from middle-income countries (30.3%). The pooled AOR was lower in probability samples (1.49) than in non-probability samples (3.35). Because most included studies used probability sampling, the pooled estimates restricted to probability samples fell within the 95% CI of the main analysis and were close to the overall estimates, providing some reassurance about robustness.
Strengths, Limitations, and Future Research Directions
This study has several notable strengths. We conducted a comprehensive literature search across 16 databases without language restrictions and incorporated eight non-English publications (Spanish and Chinese) into the analysis. In the risk meta-analysis, we included only studies reporting AORs to control for confounding and isolate the independent effect of functional dependence. We applied rigorous methods to synthesize data, validate the robustness of our findings, and explore potential sources of heterogeneity. In addition to pooling community-based data in the meta-analysis, we provided supplementary descriptive summaries of studies conducted in institutional settings or based on proxy reports.
However, several limitations warrant consideration when interpreting our findings and planning future research. The number of studies addressing particular AOP subtypes and IADL or ADL dependence remains limited. For studies that did not specify the abuse timeframe or the dependence assessment tool, we contacted the corresponding authors and other reachable authors by email several times to request clarification. Studies without responses were excluded from the analysis. Restricting the timeframe to the past-year may have produced conservative prevalence estimates. Considering stigma, fear of retaliation, or dependence on perpetrators, our estimates are limited by underreporting, so the actual prevalence of AOP may be higher. Because cross-sectional designs cannot establish causality, pooled prevalence estimates and AORs may be biased by residual confounding and reverse causality. Multilevel potential confounders, such as caregiver burden, cognitive impairment, and social isolation, may influence both dependence and abuse. For example, heavily burdened caregivers are more likely to care for highly dependent older adults, and caregiver stress is a strong risk factor for AOP ((Lu et al., 2016; WHO, 2024c). Reverse causality is also possible because abuse may accelerate declines in physical or cognitive function (Wong & Waite, 2017b). In addition, our analysis did not fully encompass all methodological characteristics and contextual variables. Unmeasured or inconsistently measured confounders may partly explain the high heterogeneity observed across studies. Variations in prevalence across countries may stem from differences in cultural norms and family structures, the availability of social welfare and support services, the strength of legal protections and enforcement for functionally dependent older adults, and prevailing public attitudes and stigma. Future research could explore the influence of these social normative variables. Although tests by instrument type were not statistically significant, pooled estimates from validated instruments were higher, suggesting that non-validated questions may under-detect abuse. Therefore, measurement heterogeneity remains an important limitation. Additionally, analysis of prospective, population-based data from the Canadian Longitudinal Study on Aging (CLSA) (Burnes et al., 2022) found that functional impairment was associated with higher odds of past-year AOP whether modeled as a baseline continuous measure, AOR = 1.16 (95% CI [1.08, 1.24]), or as a categorical indicator of decline over follow-up, AOR = 1.46 (95% CI [1.27, 1.66]). Excluding studies that used continuous measures of dependence limited our ability to assess finer distinctions.
Although studies indicate a high prevalence of AOP in institutional settings among the general older population (Yon et al., 2019), the scarcity of research on abuse rates in functionally dependent elders residing in nursing homes or long-term care facilities precluded meta-analysis for these environments. Future studies should prioritize investigations in institutional contexts to fill this gap. Furthermore, most included studies were conducted in high- and upper-middle-income countries or within the Americas. Although subgroup differences were not statistically significant, pooled prevalence estimates increased from 13% in high-income settings to 26.8% in upper-middle-income and 36.1% in lower-middle-income countries. Future research should prioritize low-income countries and regions such as Eastern Mediterranean and Africa, harmonize methods and timeframes, and employ standardized instruments of functional dependence and abuse to enhance comparability and enable robust synthesis. Moreover, future research should expand quantitative investigations of AOP prevalence and risk among other vulnerable populations, such as left-behind rural elders, migrant elders, individuals with multimorbidity, and those with poor psychological well-being. These data are essential for informing tailored prevention and intervention strategies.
Conclusion–Critical Findings
Critical Findings
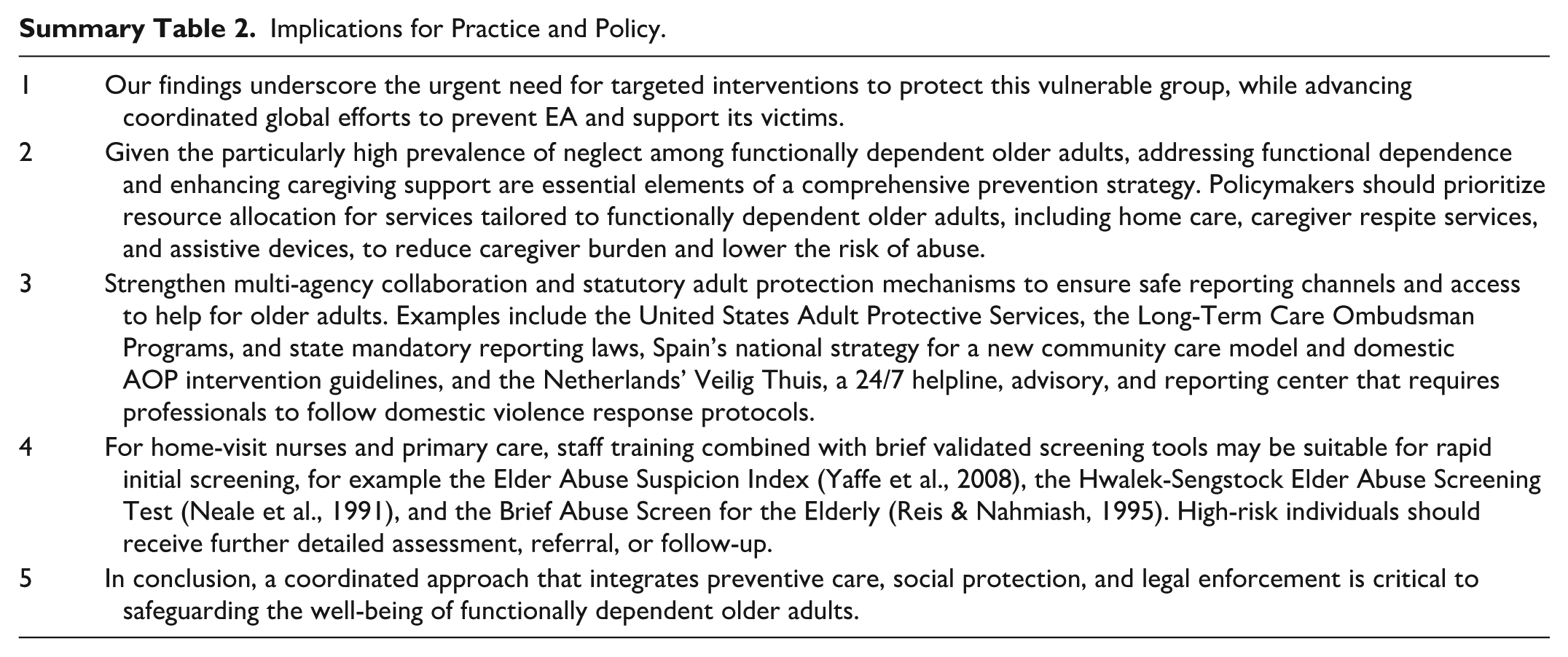
Implications for Practice and Policy
Implications for Practice and Policy.
Supplemental Material
sj-doc-1-tva-10.1177_15248380261426600 – Supplemental material for Prevalence and Risk of Abuse among Community-Dwelling Older People with Functional Dependence: A Systematic Review and Meta-Analysis
Supplemental material, sj-doc-1-tva-10.1177_15248380261426600 for Prevalence and Risk of Abuse among Community-Dwelling Older People with Functional Dependence: A Systematic Review and Meta-Analysis by Manjie Yu, Yajing Chen, Kangli Wang, Qingqing Li and Yeqin Yang in Trauma, Violence, & Abuse
Footnotes
Author Contributions
MJY and YQY conceived and designed the study. All authors supervised its implementation. MJY, YQY, and QQL developed the search strategy and conducted the literature search. MJY, YQY, YJC, and KLW coordinated data screening, extraction, and quality assessment. MJY and YJC performed data analysis. MJY drafted the initial manuscript. All authors critically revised the draft. All authors read and approved the final version of the manuscript. All authors had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Social Science Fund of China (Grant No. 21BRK032).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Relevant data have been presented in the manuscript and the Appendix.
Supplemental Material
Supplemental material for this article is available online.
Anonymized Information
This study has been prospectively registered with the International Prospective Register of Systematic Reviews (PROSPERO) under the registration number CRD420250633309.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.