
Abstract
This systematic review aims to synthesize what protective factors have been identified to promote resilience in adults who have experienced potentially traumatic events (PTEs). APA PsychInfo and PubMed were searched to identify literature published between 2014 and 2024 that studied resilience in trauma-exposed adults. Studies were included if: the PTEs experienced by participants met Criterion A for events preceding posttraumatic stress disorder as outlined in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition Text Revision (DSM-V TR); the study measured modifiable protective factors; and the study included a measure of resilience. Two independent reviewers used standardized data extraction forms and assessed risk of bias with the Mixed Methods Appraisal Tool. Of 991 unique references, 13 articles met inclusion after full-text review. A social–ecological framework guided the synthesis and categorization of factors bolstering resilience. At the interpersonal level, protective factors identified included social support and religious attendance. At the institutional or organizational level, employment, length of employment, and workplace belongingness were identified as promoting resilience. At the community level, access to social resources to help meet basic needs was found to strengthen resilience. Finally, at the public policy level, employee assistance supported resilience. This review identified critical gaps in current resilience literature. Future research should define the type, timing, and duration of PTEs exposure, as well as specify the time lapsed between data collection and the PTEs exposure. Resilience conceptualizations and interventions should focus on tracing resilience across time and on multisystemic resilience-oriented interventions that include the individual, interpersonal, institutional/organizational, community, and public policy levels.
Introduction
A global survey conducted by the World Health Organization of 68,894 participants found that 70.4% of respondents had experienced a lifetime traumatic event that met the exposure criteria required to be eligible for a diagnosis of posttraumatic stress disorder (PTSD) during their lifetime (Kessler et al., 2017). The high prevalence of potentially traumatic events (PTEs) in the general population underscores the importance of understanding the pathways to recovery following exposure to such an event. Previous studies have shown that the majority of people exposed to PTEs do not develop PTSD or other mental health difficulties (Fleming & Ledogar, 2008; Koenen et al., 2017). Exploring what is currently known about protective factors that promote resilience following PTE exposure, for whom, and in what contexts, is crucial to inform efforts to bolster resilience at the individual, community, and policy levels.
Resilience can be defined as the ability to positively adapt in the presence and wake of significant threats, challenges, or disruptions (Masten, 2018; Ungar, 2021). More than half a century of developmental resilience science has evolved to increasingly focus on environmental influences that promote positive engagement in adaptive processes (Horn et al., 2016; Masten, 2018, 2024; Ungar, 2013, 2018). The current conceptualization used in developmental resilience science is characterized by the integration of a multi-level, multisystemic perspective, which calls for a more comprehensive, ecological approach (Caiels et al., 2021; Masten, 2007; Mukherjee & Kuar, 2017; Panter-Brick & Leckman, 2013; Ungar, 2011; Ungar & Theron, 2020). This conceptualization recognizes that processes co-occur within individual, social, and community systems that promote positive functioning in the presence and wake of adversity (Caiels et al., 2021; Mukherjee & Kuar, 2017; Southwick et al., 2014; Van Breda, 2018), and argues for shifting the emphasis of resilience inquiry from individual-level to environmental factors (Ungar, 2011, 2013, Ungar & Theron, 2020).
As such, resilience-focused interventions must consider multiple environmental domains (Van Breda, 2018; Ungar, 2013). A multi-level systemic approach to resilience that incorporates individuals’ interactions with their environment, such as the social–ecological model (McLeroy et al., 1988), emphasizes equity by recognizing the environmental, structural, societal, economic, and political factors contributing to adversity and access to recovery (Hart et al., 2016). As a result, the social–ecological model shifts focus from the individual to the various environmental factors beyond an individual’s control, helping identify critical areas for policy intervention. A strength of the social–ecological model is the clear classification of an individual’s relationship with their environment at the intrapersonal, interpersonal, institutional, community, and public policy factors that influence behavior, which allows health interventions to be tailored at each environmental level (McLeroy et al., 1988).
As the shift toward a multi-systemic treatment and prevention agenda grows, attention has turned from studying individual correlates (a traits-focused approach) to studying the mechanisms and moderating processes through which one arrives at an outcome that could be considered better than expected given an individual’s risk exposure (Masten, 2018; Van Breda, 2018; Ungar, 2013). Identifying protective factors contrasts with prior deficit-focused approaches by orienting accountability at the social and societal level. This approach accounts for the resources available to individuals that promote the mobilization of resilience processes (Caiels et al., 2021) and argues that individuals’ abilities to employ protective factors are driven by their physical and social context.
Previous conceptualizations and studies of resilience have operationalized resilience in negative terms, defined as the absence of observed negative outcomes, and or have focused solely on individual characteristics/traits of those who appear to do better following adversity (Horn et al., 2016; Masten, 2018, 2024; Ungar, 2013). In this study, resilience is conceptualized as a process that promotes healthy functioning and well-being following adversity that is supported by mobilizing interactions between an individual and their social environment (Ungar, 2018). Utilizing the social–ecological model, this systematic review aims to explore the intrapersonal, interpersonal, institutional, community, and public policy factors that strengthen resilience in individuals, groups, or communities following PTEs. This study fills a critical gap in the resilience literature by examining environmental protective factors using multi-systemic frameworks of resilience and by applying rigorous criteria for traumatic events to ensure that findings are grounded in well-defined PTE exposure.
Methods
The systematic review was registered in Open Science (registration link: https://osf.io/ern7h).
Inclusion and Exclusion Criteria
A population, intervention, comparison, and outcomes (PICO) framework (Schardt et al., 2017) was used to guide the research question, the literature search, and the inclusion and exclusion criteria. Articles were included if: (a) published in English (b); published between 2014 and 2024; (c) published in peer-reviewed journals; (d) based on a sample of adults that experienced PTEs meeting DSM-V TR Criterion A for PTSD defined as: exposure to actual or threatened death, serious injury, or sexual violence whether through direct experience, witnessing, learning about an event affecting a close relative or friend, or repeated indirect exposure to aversive content via work duties (American Psychiatric Association, 2020); (e) any empirical study (qualitative or quantitative) that measured short-term modifiable behavioral protective factors: defined as malleable conditions or attributes that help individuals cope with stressors or challenges; (f) only of adults ages 18+; and (g) included a measure of resilience. We limited inclusion to studies that used a resilience scale to ensure that resilience was operationalized and empirically measured.
Conversely, studies were excluded if the articles were not published in a peer-reviewed journal, the event experienced by participants did not meet Criterion A or the PTE sufficiency was unclear, the outcomes of interest were not measured with a resilience measure, the study did not measure modifiable protective factors, and or resilience was not included as a main outcome of interest. Posttraumatic growth (PTG) outcomes were excluded because PTG differs from resilience and is outside the scope of the present review. Resilience focuses on adapting to adversity, while PTG emphasizes positive growth following a traumatic event (Elam & Taku, 2022). Prior research supports the conclusion that these are separate constructs (Ersahin, 2022; Kangaslampi et al., 2022; Kheirallah et al., 2022; Simsir & Dilmac, 2021; Umer & Elliot, 2021). There was no exclusion criteria based on study design.
Search Strategy
Searches were conducted on MEDLINE on 2/14/2024 and PsychINFO via Pubmed on 03/31/2024. This timeframe from 2014 to 2024 reflects the most current understanding and developments in the field of resilience. Search terms and strategy focused on capturing traumatic events, psychological trauma, and adverse life events. Other terms of interest included terms related to resilience and protective factors. See Appendix A for the full search algorithm.
Selection Process
Two authors (CGH) and (WC) independently screened articles identified by the search strategy for inclusion. Initially, titles and abstracts were screened for eligibility. Two authors (CGH) and (WC) then screened the full text of all potentially eligible studies for final study inclusion. Search results were uploaded to PICO Portal, which uses machine learning to organize articles for screening (PICO Portal, 2024). PICO Portal was used for the title/abstract and full-text review phases. All articles were screened independently by two authors (CGH) and (WC). Standardized data extraction was conducted in Excel.
Data Collection Process and Data Extraction
Two authors (CGH) and (WC) independently extracted data using a standardized format to extract author name, study title, year, country/location, study design, population, sample size, trauma exposure type, time of event to data collection, resilience scale measure, protective factor, and resilience outcomes and study key findings in Microsoft Excel.
Quality Assessment
Two authors (CGH) and (WC) reviewed the risk of bias using the Mixed Methods Appraisal Tool (MMAT); the MMAT is an appropriate critical appraisal tool to assess qualitative, randomized controlled, nonrandomized, quantitative descriptive, or mixed methods studies (Hong et al., 2018).
Results
Figure 1 shows the flow of articles included at various phases. The final search identified 991 articles. Using PICO Portal, 45 duplicate records were removed, leaving 946 articles for title and abstract screening. The abstracts of these 946 articles were assessed for eligibility. During this phase, 791 records were excluded. Articles were excluded if studies included participants under the age of 18, if they did not specify the type of trauma exposure, if events failed to meet Criterion A, if the study did not measure modifiable protective factors, or if resilience was not measured as an outcome. The remaining 155 articles were sought for full-text retrieval and were successfully retrieved and assessed for eligibility. A total of 13 articles were included after full-text review.
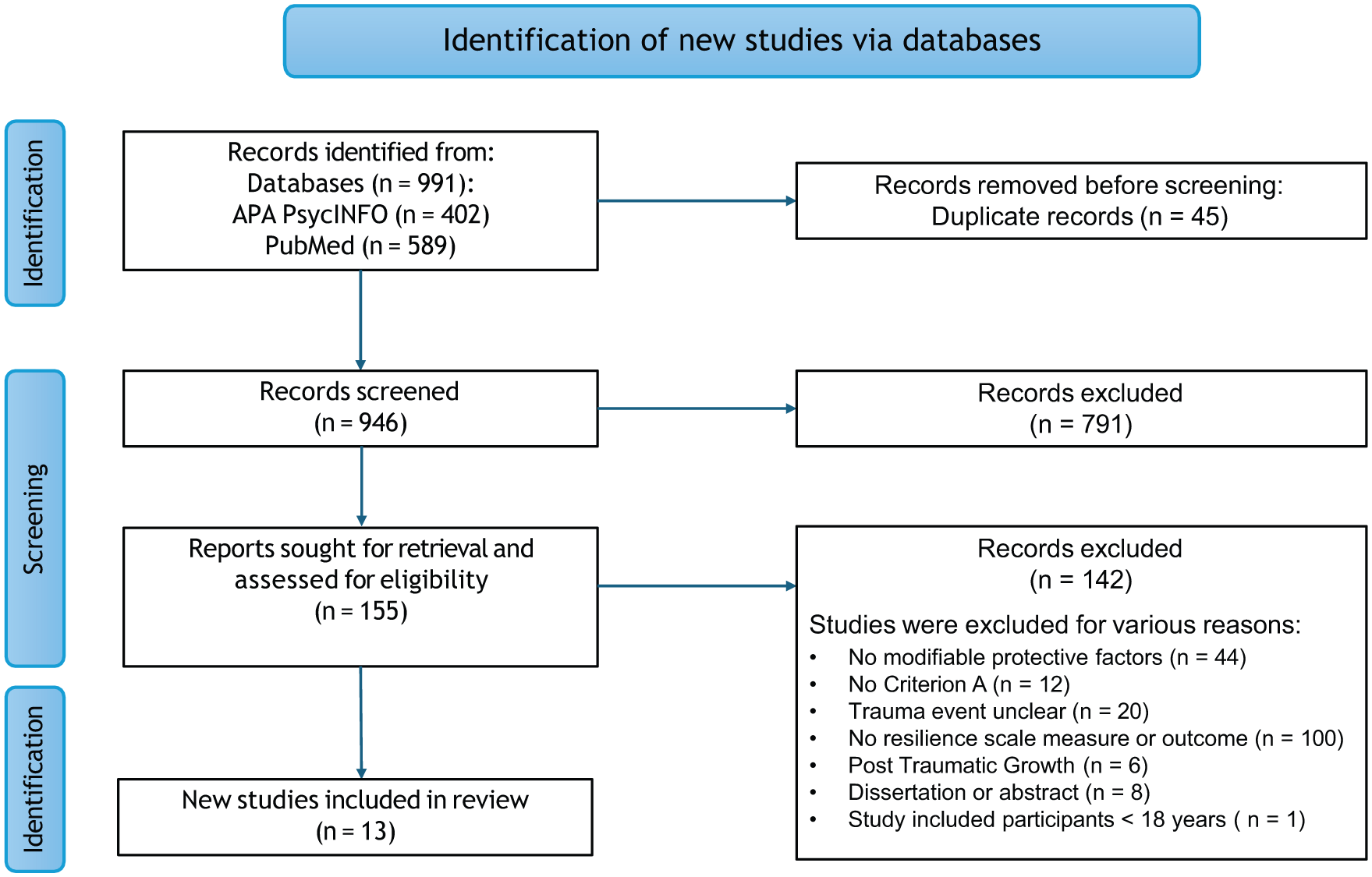
PRISMA flow diagram of literature search screening.
Study Characteristics of Included Studies
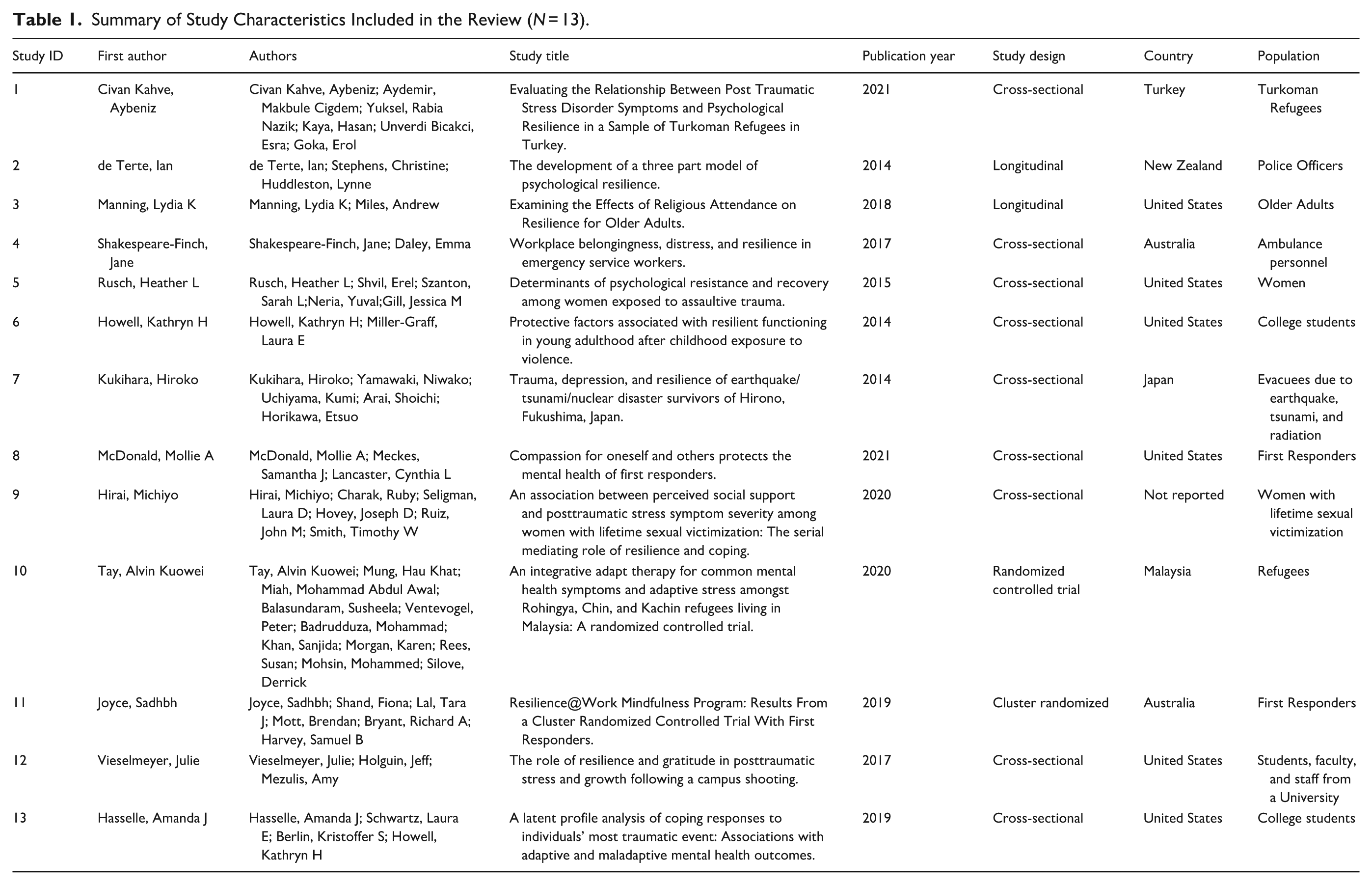
Table 1 depicts the study design, geographic location, population type, and traumatic event exposure in the final systematic review. Study designs included: cross-sectional, longitudinal, and randomized controlled trials. Studies included in the review collected data in the United States, Turkey, New Zealand, Australia, Japan, and Malaysia. Study populations in the final review included refugees, police officers, older adults, women, college students, first responders, and disaster evacuees. Traumatic event exposure events included: war, persecution, physical assault, sexual victimization, homicides, campus shootings, childhood violence, suicides, messy deaths, extreme injury or illness, disasters such as earthquakes, tsunamis, nuclear disasters, fires, and other major disasters.
Summary of Study Characteristics Included in the Review (N = 13).
Risk of Bias
As shown in Table 2, most studies met the methodological quality criteria, as indicated by a “1” for “yes” when the criterion is met and a “0” for “no” when the criterion is not met. Studies were primarily scored a “0” if the study sample was not representative of the target population and/or had high dropout rates.
Risk of Bias Quality Assessment for the Included Studies.
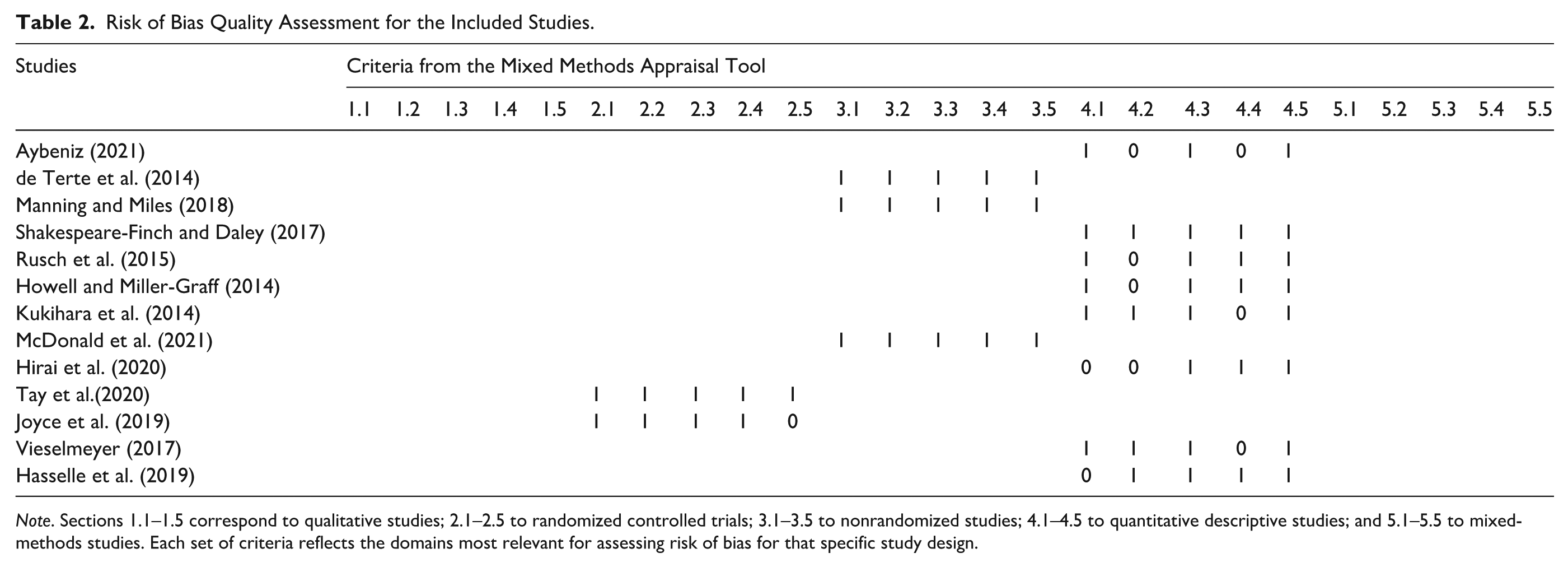
Note. Sections 1.1–1.5 correspond to qualitative studies; 2.1–2.5 to randomized controlled trials; 3.1–3.5 to nonrandomized studies; 4.1–4.5 to quantitative descriptive studies; and 5.1–5.5 to mixed-methods studies. Each set of criteria reflects the domains most relevant for assessing risk of bias for that specific study design.
Resilience Intervention Components
Table 3 highlights the identified protective factors that promoted resilience in the study sample, which included: self-compassion, integrative adapt therapy (IAT), mindfulness, gratitude, engagement coping, mastery (perception of control over life-altering forces), access to social resources to meet basic needs, perceptions of health, healthy lifestyle (eating breakfast, vegetables, eating in moderation, eating balanced meals, and exercise), religious attendance, spirituality, social support, employment, workplace belongingness, greater length of employment, and employee assistance.
Summary of Resilience Results Following PTEs.
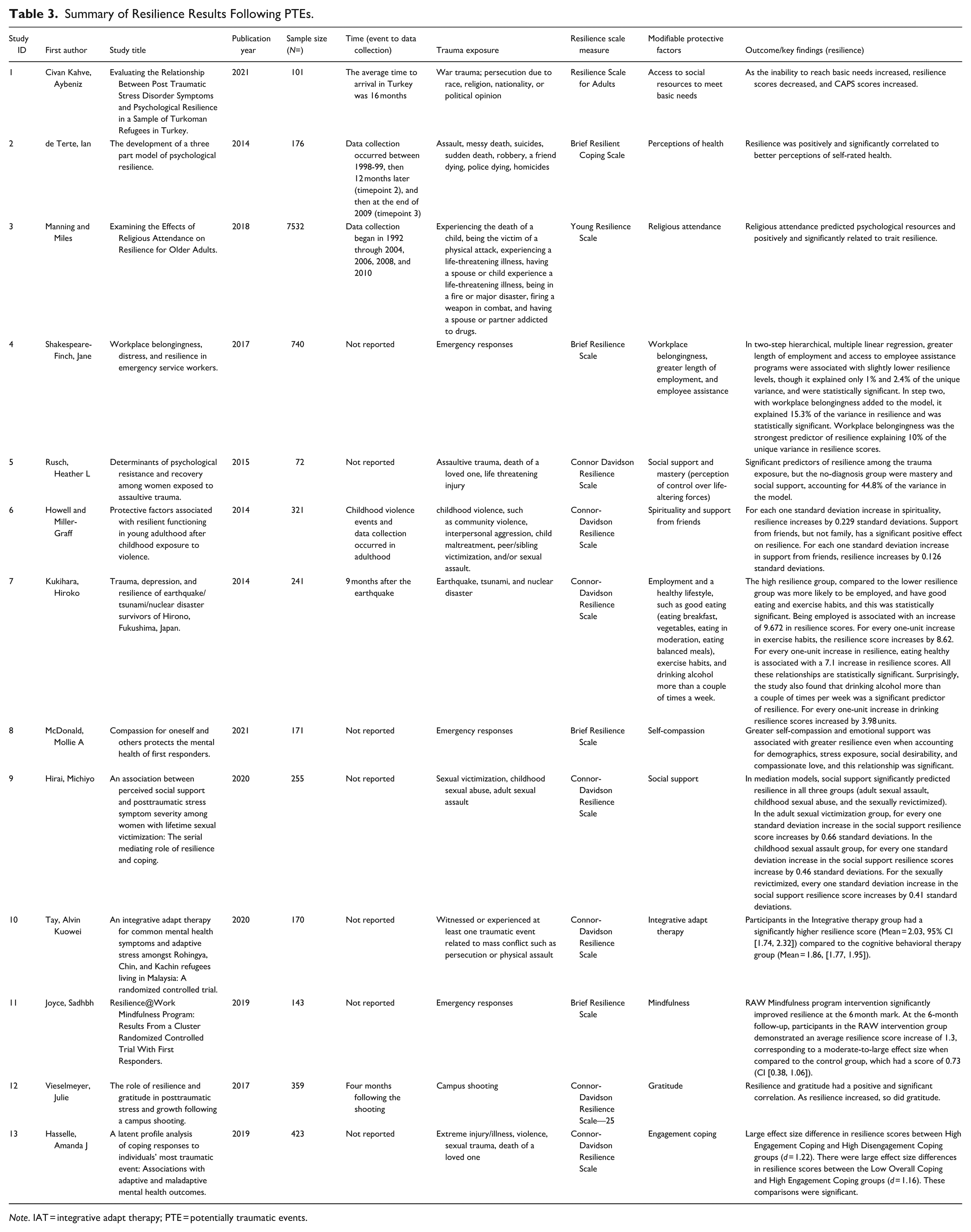
Note. IAT = integrative adapt therapy; PTE = potentially traumatic events.
Figure 2 illustrates the various protective factors across different studies categorized by levels of the social–ecological framework: intrapersonal, interpersonal, institutional/organizational, community, and public policy levels that promote resilience in adult individuals, groups, or communities. The intrapersonal level encompasses traits or characteristics attributed to perceptions, beliefs, and attitudes. The interpersonal level includes primary groups such as friends or family that provide role identity, social support, and interactions to support an individual. The institutional and organizational level focuses on the organizational behavior of organizations such as businesses, schools, and churches. The community level encompasses norms and standards amongst communities, organizations, and institutions within defined boundaries. Finally, public policy refers to policies and or laws that affect health (McLeroy et al., 1988).
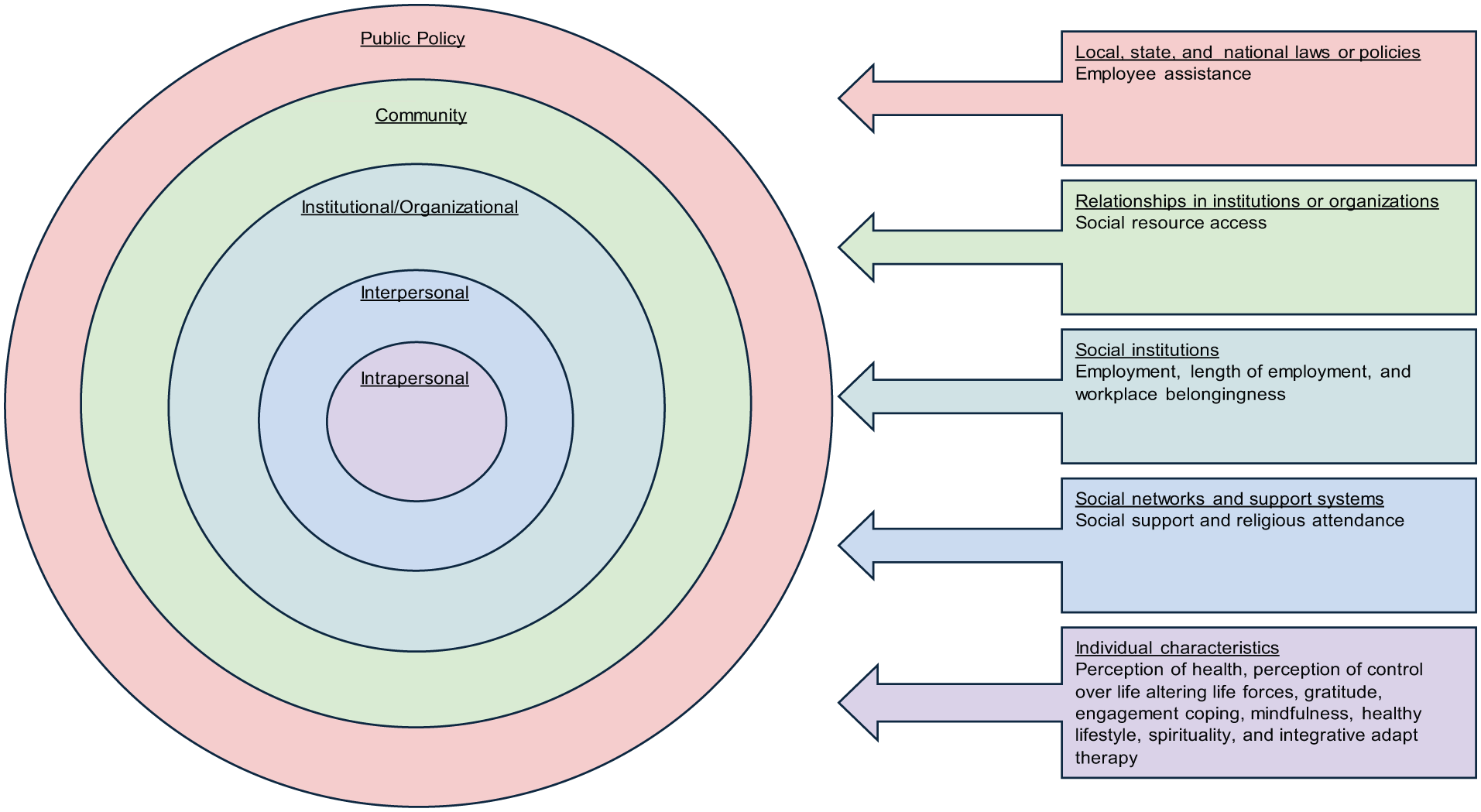
Social–ecological model resilience protective factors following PTEs.
Discussion
Compared to other systematic reviews, this review contributes to the current resilience literature by adopting a clear definition of PTEs that aligns with Criterion A (Bonanno et al., 2024; Chmitorz et al., 2018; Ferreira et al., 2021; Johnson et al., 2017; Schäfer et al., 2024). Ensuring participants’ PTEs meet Criterion A is an important distinction from previous systematic reviews, as resilience can only be identified in the presence or wake of adversity (Masten, 2001). For example, out of 43 articles examining interventions that promote resilience in Chmitorz et al.’s (2018) systematic review, only two studies included reported the type or amount of individual stressor exposure participants experienced. Further, this systematic review only included studies that measured resilience with one of the following established resilience scales: Resilience Scale for Adults, Brief Resilient Coping Scale, Young Resilience Scale, and the Connor Davidson Resilience Scale. In contrast, other empirical studies have included and compared articles that attempt to capture resilience in a variety of ways, some of which mix conceptualizations of resilience within the same review (i.e., negative conceptualizations denoted through lower-than-expected self-reported symptom inventories). For example, a systematic review by Macedo et al. (2014) examining resilience interventions found that, of the seven randomized controlled trials, only three used a validated resilience measure. Additionally, among the five non-randomized trials, only one used a validated measure of resilience (Macedo et al., 2014). In comparison to prior research, adopting more stringent criteria, particularly of PTEs exposure and resilience measures, helps ensure sufficient conceptual and definitional similarities among the studies included in this review, and thus the clarity of currently available findings.
A total of 13 studies met the inclusion criteria. Final identified modifiable protective factors promoting resilience for adults who have experienced a Criterion A event at the intrapersonal level focused on psychological resources, coping, and health-promoting behaviors. More specifically, these included perception of health, mastery (perception of control over life-altering forces), gratitude, engagement coping, mindfulness, healthy lifestyle, such as good eating (eating breakfast, vegetables, eating in moderation, eating balanced meals, and exercise), spirituality, and IAT. Joyce et al.’s (2019) meta-analysis evaluated the efficacy of mindfulness- and cognitive-based interventions and found that combined mindfulness and cognitive approaches produced the greatest effects, with a moderate effect size promoting resilience. Findings from our systematic review also suggest that health-promoting behaviors may support resilience; however, the healthy lifestyle behavior measure used in Kukihara et al.’s (2014) study, one of the included studies in this review, may lack sufficient specificity to draw firm conclusions on what behaviors promote resilience. Similarly, Chmitorz et al. (2018) suggest that future resilience research incorporates more comprehensive baseline assessments of physical health and medical history, which may provide greater insight into the physical health–promoting activities that support resilience. At the interpersonal level, protective factors centered on social connections, including social support and religious attendance. Prior systematic reviews have identified the central role that social support networks and social connections from significant others, family, and community play in supporting resilience (Ungar & Theron, 2020; Raghavan & Sandanapitchai, 2024). A meta-analysis by Schwalm et al. (2022) found a moderate association between religiosity/spirituality and resilience. This association may be partly explained by the social support provided through religious communities, as well as the role of faith/spirituality in fostering meaning-making and encouraging a positive or optimistic outlook; however, the meta-analysis did not restrict its sample to adults who had experienced PTEs (Schwalm et al., 2022). At the institutional or organizational level, protective factors associated with resilience were employment status, workplace stability, and workplace inclusion/belongingness. A meta-analysis by Vanhove et al. (2016) found that organizational resilience-building interventions—including stress management, coping skills, social, leadership, and management interventions—had small but statistically significant effects on well-being, workforce performance, and psychological distress; however, the analysis did not restrict the sample to individuals who had experienced PTEs. At the community level, access to supportive resources to meet basic needs (food, water, clothing, shelter, warming, and access to medical care) was found to support resilience. The public policy level included access to employee assistance sponsored services (such as counseling services, referrals, and or wellness programming). These factors were identified in diverse traumatic contexts, including war, assault, shootings, natural disasters, and life-threatening accidents. Despite variations in study design (longitudinal, cross-sectional, and randomized controlled trials) and population (refugees, police officers, older adults, ambulance personnel, women, college students, first responders, and evacuees due to earthquake, tsunami, and radiation), the findings underscore the critical role of coping behaviors and accessible supports at the individual, community, and societal levels that mitigate the adverse effects of PTEs.
Our systematic review identified three meaningful points of clarity for future scholarship exploring traumatic stress and resilience. A total of seven included studies did not specify the timing of the event exposure or the time lapsed prior to data collection. Moving forward, studies should report more precise timing on when data collection occurs in relation to participants’ PTE exposure. This will help clarify what is known about the dynamics of resilience trajectories that can occur at various timepoints after PTEs. For instance, in one study from this review by Joyce et al. (2019), resilience scores were not significant at 6 weeks, but were at the 6-month follow-up. The ability of resilience measures to predict future resilience has been questioned (Bonanno et al., 2024), and findings are limited to the timepoint at which data were collected. Therefore, specifying when the PTE occurred in relation to data collection allows for continued examination of resilience across timepoints.
Additionally, at full-text review, 20 articles could not be included in this review due to a lack of clarity about the focal events related to participants’ PTEs exposure. Without a minimum degree of specificity about participants’ traumatic prior experiences, it is not possible to assert sufficient similarities in the exposures of the individuals compared within a single study. This limitation compounds when attempting to compare findings across studies and significantly limits how findings can be contextualized within available scholarship. Improving clarity about events reported as “traumatic” would meaningfully increase the utility of these important empirical explorations and the knowledge gleaned from them. For example, future standardized data collection on the type and severity of PTEs, as well as the recurrence of the PTEs, would facilitate comparisons of resilience outcomes and trajectories (Galatzer-Levy et al., 2018). Subsequently, it is imperative that studies measuring or reporting resilience include an operationalized definition of their conceptualization of resilience. Numerous articles were excluded for appearing to use the absence of posttraumatic stress indicators as a proxy for resilience. It is well established that resilience and vulnerability coexist and that resilience indicators can increase over time even in the presence of ongoing traumatic stress symptoms (Sleijpen et al., 2017; Zuilkowski et al., 2016).
Finally, the emphasis on protective factors at the intrapersonal and interpersonal level is likely because some of the resilience measures used in the included studies only ask about individual-level items (e.g., “I tend to bounce back quickly after hard times,” “I usually get through hard times with little trouble,” “I am able to adapt to change,” “I have a sense of purpose in life”), participants’ evaluations of whether their environments provide adequate resources to meet their needs are missing from these resilience measures and studies. In a review of resilience scales, Windle et al. (2011) found that the majority of available resilience scales (9 out of 15) focused on identifying resilience at the level of individual characteristics and occasionally included social resources at the individual level. The review found a notable absence of multi-level considerations in the resilience scales that would be required to better align with the current conceptualization of resilience (Windle et al., 2011). Similarly, another systematic review identified limited reporting of protective factors at the societal or community-oriented level and found that (72%) of studies included in the review found protective factors at the individual level, (86%) at the social level, and only (26%) at the societal level (Schäfer et al., 2024).
This systematic review does not come without limitations. First, even though a rigorous literature review and search strategy occurred in collaboration with a librarian, we cannot rule out the possibility that some qualifying or relevant publications from other databases not searched were not identified and included. Second, all included articles were from peer-reviewed journals; therefore, the exclusion of unpublished studies and or grey literature may have introduced publication bias. However, contacting authors to request unpublished data could also introduce bias by selectively favoring non-peer-reviewed studies or authors who were reachable or responsive. Third, studies with traumatic exposure that did not meet Criterion A, such as generational or historical trauma, daily stressors, social marginalization, and or endemic stressors, were excluded. The exclusion of larger historical context that influences community capacities, goals, and resources may artificially contextualize traumatic exposures as more acute and individualized than would result from a more inclusive, historically sensitive alternative (Atallah, 2016). The findings of this systematic review should be interpreted with caution, given the cross-sectional study design conducted in high-resource settings of the included studies.
Summary of Implications for Research, Practice, and Policy
This review focused on modifiable factors that individuals, communities, and policymakers can target to enhance resilience. However, it is important to recognize that the modification of some of these factors occurs outside of a single individual’s locus of control. Disparities in resource availability and accessibility, such as social infrastructure (community spaces) can vary significantly across different geographic regions (Latham & Leyton, 2019). Access to social resources to meet basic needs, shared religious attendance, employment opportunities, social support, a sense of mastery, and access to health-enhancing factors or healthcare (e.g. therapy) all depend on the availability of the requisite environmental assets to be successfully mobilized by individuals. That is, individuals can only access employment in areas where jobs are available, medical services in regions where providers are accessible, and social support in areas where they are safe to move and communicate freely. This further emphasizes the central role that access to resources and opportunities plays in enabling individuals to navigate the psychological, social, cultural, and physical resources in their environment to promote resilience (Ungar & Theron, 2020). The social–ecological model illustrates how protective factors and resources within an individual’s environment work in unison. For example, this study identified the importance of social networks, employment, and a sense of belonging in the workplace. Strengthening positive workplace cultures that foster meaningful relationships can enhance social networks and support systems. In turn, improving access to one protective factor may positively influence others, creating opportunities for a diverse range of coping strategies (Ungar & Theron, 2020).
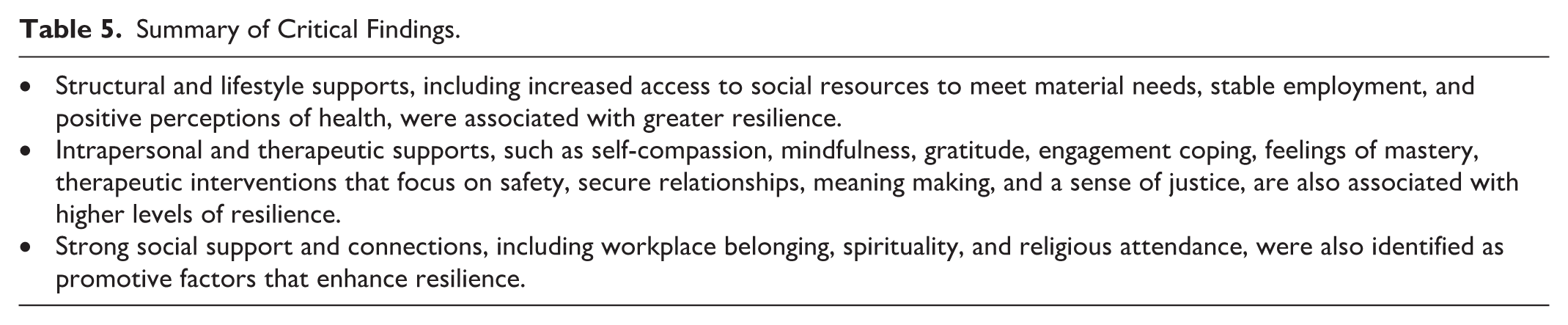
Organizations, companies, communities, governments, and clinicians also play a role in supporting factors that sustain or create opportunities for healthy living to bolster resilience. For example, organizations and companies can provide a positive workplace environment, strong benefits, appropriate accommodations, and wellness programs to promote workplace stability and a sense of belonging. Local governments can also invest in community resources/assets—such as parks, libraries, trails, schools, and grocery stores to foster healthy living. The findings of this review emphasize the importance of multi-level, resilience-oriented strategies that not only focus on the individual but also on the modifiable social and structural systems influencing resilience following PTEs. A summary of the research, practice, and policy implications is provided in Table 4. The critical findings are summarized in Table 5.
Summary and Implications of the Review for Research, Practice, and Policy.
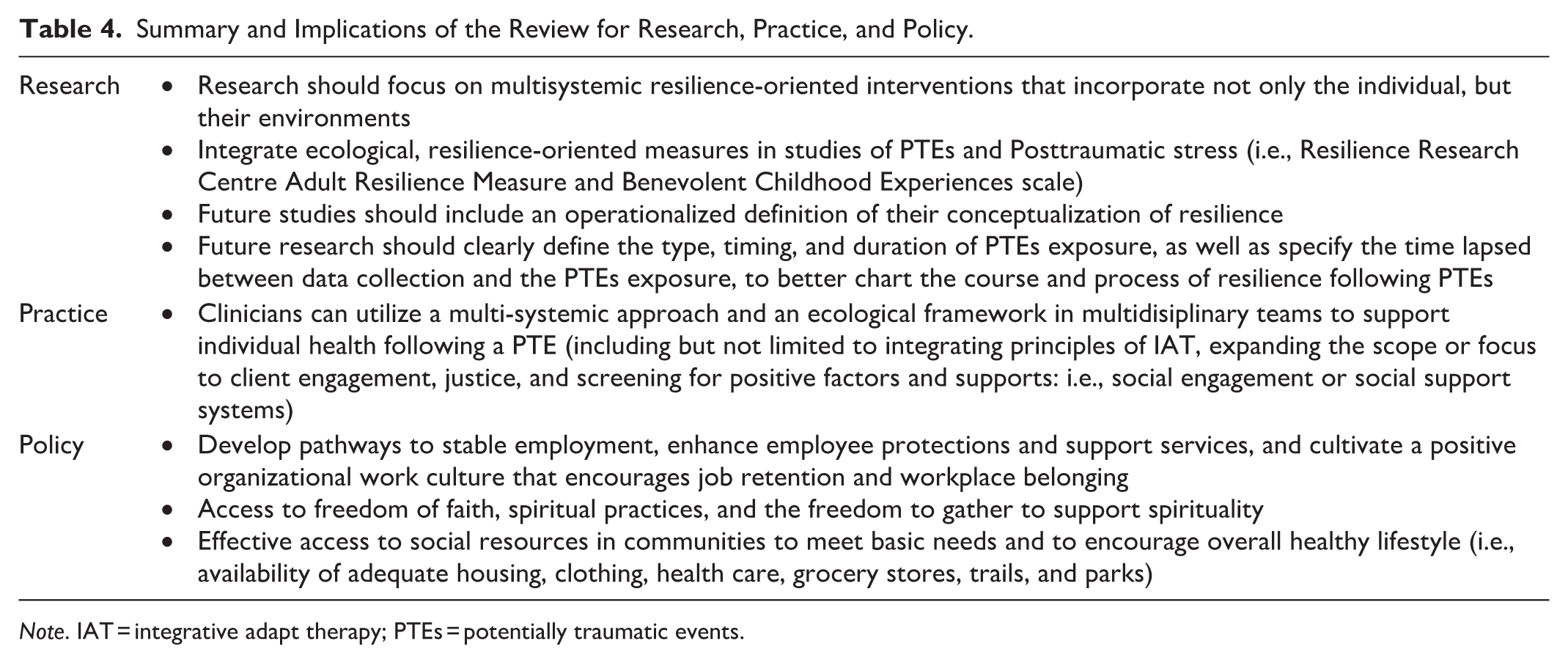
Note. IAT = integrative adapt therapy; PTEs = potentially traumatic events.
Summary of Critical Findings.
Conclusion
It is important to recognize the multifaceted nature of resilience factors that affect individuals at the individual, community, and public policy levels. Strengthening social support, opportunities for spirituality, meaningful employment/belonging, mindfulness, gratitude practices, coping skills, and access to basic resources that enable healthy living may be key factors in promoting resilience in individuals and communities. Although current scholarship has identified several broad mechanisms for promoting resilience in the wake of PTEs exposure, exactly how, how much, and when these processes occur remain important foci for future inquiry. The continued study of these nuances can enhance the availability of inclusive and effective supports for fostering resilience across diverse populations, life exposures, and post-exposure contexts. Future research should clearly define the type, timing, and duration of PTEs exposure, as well as specify the time lapsed between data collection and the PTEs exposure. Additionally, scholarship should focus on multisystemic resilience-oriented interventions that include the individual, community, and policy levels.
Footnotes
Appendix
Search strategy terms for MEDLINE and PsychINFO.

| Search Terms |
|---|
| ((“trauma” OR “traumatic experience” OR “adverse life events” OR “traumatic event”) AND (“protective factors” OR “resilience” OR “mitigating factors”)) AND ((“2014”[Date—MeSH]: “3000”[Date—MeSH]) AND adult) |
Acknowledgements
The authors would like to thank University of Minnesota librarian Amy Claussen who assisted with the search.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.