
Abstract
Social impairments are commonly reported by individuals with a history of child maltreatment (CM). However, a systematic review on the relationship between different types of CM and impairments across various domains of social functioning in adults with and without mental disorders that also addresses mediating and moderating factors is still missing. Therefore, we systematically searched the PsycINFO and Web of Science databases for peer-reviewed studies published from 2003 to February 2025 that examined the association between CM before the age of 18 and various clinically relevant impairments in social functioning in adulthood (≥18 years). A total of 281 articles were included and clustered in seven domains of social functioning. Most studies revealed negative associations between CM and social functioning, with small to moderate effect sizes. The strongest evidence was found for intimate partner violence, aggression, social connectedness, attachment, and early maladaptive schemas, while findings for other domains–such as sexuality, intimate partner relationships, and social-cognitive processes—were less consistent. Psychopathology, insecure attachment, and emotion regulation were the most frequently identified mediating or moderating factors. Taken together, CM and social dysfunctions need to be assessed and considered more systematically in psychotherapeutic treatment across disorders. Furthermore, longitudinal studies with standardized measures of social functioning are needed to identify transdiagnostic as well as disorder-specific targets for mechanism-based prevention and interventions for individuals with CM experiences.
Introduction
Social functioning is a central determinant of well-being across the general population. Impairments in social functioning can have debilitating effects on multiple domains of life and are common in many mental disorders. The significance of impaired social functioning is acknowledged in the ICD-11, where it is regarded as one of the two key domains in the assessment of the severity of personality disorders (World Health Organization, 2019). Similarly, impairments in social functioning are part of the diagnostic criteria of posttraumatic stress disorder (PTSD) and complex PTSD (American Psychiatric Association, 2013; World Health Organization, 2019), but also prominent in other mental disorders, such as affective, anxiety, or psychotic disorders (Keltner & Kring, 1998). Identifying risk factors, as well as potential mediators and moderators that may explain which social impairments are experienced in whom and why, is therefore of high clinical relevance.
Being the most significant single risk factor for mental disorders and physical illness later in life (Jaffee et al., 2017; Klinger-König et al., 2024), child maltreatment (CM) has also been proposed to contribute to impairments in social functioning. According to Bernstein et al. (2003), CM is defined as the experience of emotional, physical, or sexual abuse or emotional or physical neglect before the age of 18 (McLaughlin et al., 2020).
In fact, there is an expanding body of research indicating diverse social deficits in individuals with a history of CM, both in non-clinical (Pfaltz et al., 2022) and clinical populations, such as borderline personality (BPD), PTSD, affective or psychotic disorders (Aversa et al., 2014; Cotter et al., 2015; Fares-Otero, De Prisco, et al., 2023). These social impairments not only hinder the use or availability of social support, a key factor in resilience following trauma (Carr et al., 2020; McLaughlin et al., 2020), but also diminish the effectiveness of evidence-based psychological interventions contributing to reduced treatment success, prolonged treatment duration, and higher dropout rates (Dinger et al., 2013; Quilty et al., 2013; Tibi et al., 2019). The growing body of evidence highlighting social impairments associated with CM stands in stark contrast to the limited attention such dysfunctions have received in etiological models and psychotherapeutic approaches to CM-related disorders to date.
A central aim of our project is to improve the knowledge about the social functioning of individuals exposed to CM. Both CM and social functioning represent broad and multidimensional constructs, encompassing a wide range of experiences and processes. As a first step, we are therefore interested to identify which specific types of CM are linked with which specific social deficits, as well as to examine possible moderators and mediators of these associations in adulthood. Importantly, our focus spans the full spectrum of mental health functioning, including both clinical and non-clinical populations. Given the conceptual breadth of this topic and the heterogeneity of studies, a systematic review of the literature appeared the most promising way, allowing a balance between systematic synthesis and clinical knowledge in a broad and widespread field of research (Pfaltz et al., 2022). Following the ICD-11 definition of impairments in social functioning in personality disorders, we define social functioning as comprising: (a) the core skills needed to initiate and sustain mutually fulfilling interpersonal relationships, encompassing intimacy, empathy, and conflict resolution (World Health Organization, 2019) and (b) the ability to apply these skills to effectively fulfill one’s roles in various relationships, such as those in work, friendships, partnerships, and family (Weissman, 1975). This broad definition was deliberately adopted to map the existing literature across social functioning domains and to generate hypotheses and identify priorities for future research.
Three earlier reviews and meta-analyses have addressed partly overlapping topics (Carr et al., 2020; Fares-Otero, De Prisco, et al., 2023). However, all of them had a much narrower scope by focusing on specific age groups (adolescents), particular mental disorders (depression), or psychosocial adjustment defined very broadly without focusing on specific deficits. All three reviews suggest that CM is related to social impairments, highlighting the relevance of the topic addressed in the current article. However, our review extends these earlier works by (a) adopting a transdiagnostic perspective, (b) assessing subtypes of CM and (c) diverse clinically relevant social deficits as well as (d) focusing on mediating and moderating factors of the CM-social deficit-association. Therefore, in the current pre-registered systematic review, we addressed two key questions:
Which associations between CM and social functioning have been observed? We focused on social functioning in adult clinical and non-clinical samples and explored the relationship between different domains of social functioning and CM in general, as well as its subtypes.
Which general and specific factors moderate or mediate the association between CM and social functioning?
Methods
Search Strategy
We followed the guidelines set by the Preferred Reporting Items for Systematic Reviews and Meta- Analyses (PRISMA). A protocol for the review was preregistered on the International Prospective Register of Systematic Reviews (PROSPERO) on January 30, 2024, with the registration number CRD42024504187. The protocol is available at: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42024504187
On December 27, 2023, a systematic search was conducted in the databases PsycINFO and Web of Science for peer-reviewed studies published in English after 2003, which explored the relationship between CM before the age of 18 and impairments in social functioning in adulthood (≥18 years). A supplementary literature search was performed to ensure the inclusion of studies published up to February 10, 2025. The 2003 cut-off was selected based on the publication year of Bernstein et al.’s definition of CM that was also used in the current study. According to Bernstein et al. (2003), CM was defined as experiences of emotional, physical, or sexual abuse or of emotional or physical neglect before the age of 18 years. Social functioning was conceptualized according to multiple frameworks and perspectives, including the ICD-11 personality disorder framework (World Health Organization, 2019) of interpersonal dysfunction, which encompasses the desire for relatedness and perspective-taking, mutual relationship quality, and conflict management. This was further complemented by aspects of impaired social functioning emphasized in diverse clinical models (e.g., detachment, loneliness, mistrust, and rejection sensitivity), such as the Hierarchical Taxonomy of Psychopathology (HiTOP; Kotov et al., 2018), Schema Therapy (Young et al., 2003), and the Cognitive Behavioral Analysis System of Psychotherapy (CBASP; McCullough, 2006). In addition, the selection process was guided by clinical observations of impaired interpersonal symptoms linked to early trauma, as synthesized by independent clinical scientist-practitioners. Although search terms were intentionally broad, inclusion decisions were guided by whether outcome measures captured an explicit interpersonal component based on our definition in the introduction. The search strategy can be found in the supplemental material.
Eligibility Criteria
Studies were eligible for inclusion if they met the following criteria: (a) a quantitative analysis of longitudinal, experimental, cross-sectional, or clinical trial data; (b) inclusion of a validated psychometric measure of emotional abuse, emotional neglect, physical abuse, physical neglect, and/or sexual abuse; (c) inclusion of a validated psychometric measure of social impairment; (d) participation of individuals with and/or without mental disorders from both community and specialized settings; (e) participants aged 18 years or older at the time of the outcome measurement, with exposure to CM occurring before the age of 18 (including retrospective reports); (f) ethical approval and documentation of written informed consent as stated in the published article. Excluded were case reports, reviews, meta-analyses, animal studies, open trials, qualitative studies, gray literature, dissertations, and unpublished studies.
Data Extraction and Synthesis
As displayed in the flowchart (Figure 1), a total of 281 publications were included in the review. The web-based collaboration software platform Covidence (Veritas Health Innovation, 2024) was used for duplicate removal, title and abstract screening (conducted by KB, TB, TE, and IG), as well as full-text screening and data extraction (by all authors). Because of the extensive scope of the review, dual screening and data extraction by multiple reviewers were not feasible. The following information was extracted from the articles: authors, publication year, country, type of population, study aim, study design, descriptives (age, gender, diagnoses), validated measures of CM and social functioning, reported statistics (e.g., correlation/regression coefficients and odds ratios), and identified moderators or mediators. When studies reported effect sizes, this interpretation was extracted as presented. If no interpretation was provided and correlation coefficients were reported, effect sizes were classified using conventional thresholds by Cohen (1992) (r > .10 = small/weak; r > .30 = medium/moderate; r > .50 = large/strong) to allow for consistent reporting across studies. Given the heterogeneity of social functioning outcomes, we categorized them into seven domains, in line with previous reviews (Carr et al., 2020, 2023; Fares-Otero, De Prisco, et al., 2023; Haslam & Taylor, 2022): (a) Social connectedness and social-cognitive processes; (b) attachment and early maladaptive schemas (EMS); (c) sexuality; (d) aggression, violence, and offending; (e) intimate relationships; (f) intimate partner violence (IPV) and revictimization; and (g) parenting behavior. For each domain, the study findings were summarized in a narrative synthesis based on the statistical data.
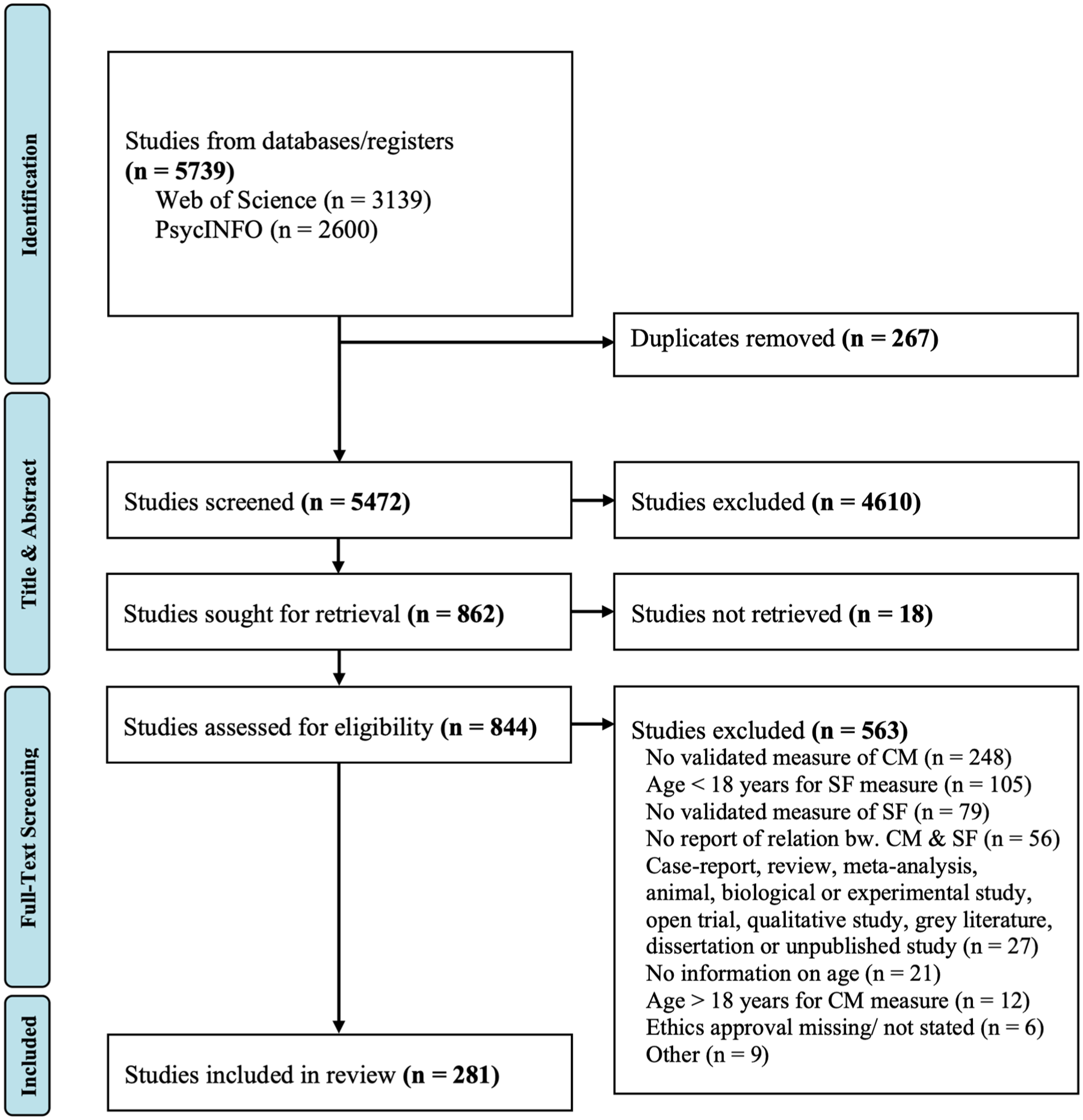
PRISMA flowchart of the systematic review procedure.
Study Characteristics
The 281 included publications presented data from a total of 263,016 participants. Sample sizes varied, ranging from 36 to 25,778 participants. However, it is important to note that the exact total sample size cannot be reliably determined, as data from the same cohorts (i.e., MIDUS, RYDS, and MTurk) or studies was likely used across 16 publications (Abajobir et al., 2017; Fitzgerald & Gallus, 2020; Fitzgerald & Morgan, 2022; Gallagher et al., 2023; Kisely et al., 2024; Lassri & Gewirtz-Meydan, 2025; Lassri et al., 2023; Smith et al., 2005, 2013; Widom, 2024; Widom et al., 2006, 2008, 2014; Wong et al., 2019; Zamir & Lavee, 2014, 2015). The studies were conducted across a diverse range of countries, which can be grouped by continent as follows: America (United States [n = 151], Canada [n = 14], Peru [n = 1]); Europe (Germany [n = 15], the United Kingdom [n = 7], Italy [n = 6], Spain [n = 6], Norway [n = 5], the Netherlands [n = 3], Portugal [n = 2], Switzerland [n = 2]; Finland [n = 1], Belgium [n = 1], Hungary [n = 1]), Middle East (Israel [n = 14], Iran [n = 4], Lebanon [n = 1]); Africa (South Africa [n = 1], Cameroon [n = 1], Kenya [n = 1], Ethiopia [n = 1], Botswana [n = 1], Uganda [n = 1]); Asia (China [n = 12], South Korea [n = 6], Turkey [n = 8], Taiwan [n = 2], the Philippines [n = 1], Japan [n = 1], Bangladesh [n = 1], Indonesia [n = 1]) and Oceania (Australia [n = 9]). The age of participants in these studies ranged from 18 to 89 years, with a weighted mean age of 28.90 years (SD = 9.62), based on the studies that reported age data. The studies included community populations (n = 128 studies), psychiatric patients (n = 44), healthy controls (n = 11), as well as forensic (n = 25) or other populations (n = 98). Across all studies, 57.04% of participants were female, 42.83% were male, and 0.13% identified as diverse.
The association between CM and social functioning was predominantly examined using correlational models, with 62 studies (22.06%) relying exclusively on correlations. Other statistical approaches included regression analyses (34.88%), t-tests, ANCOVAs, or MANCOVAs (12.10%), odds ratios (OR), risk ratios (RR), or hazard ratios (HR) (11.74%), chi-squared tests (3.56%), and multilevel modeling (MLM) (1.07%). Mediation or moderation analyses were conducted in 94 studies, predominantly based on cross-sectional data (84.04%), with only 15 studies utilizing longitudinal data. CM was most frequently assessed retrospectively using the Childhood Trauma Questionnaire (CTQ; Bernstein et al., 2003) in 47.26% of studies.
Results
As outlined above, we organized the results into seven categories, which align with classifications used in previous reviews and meta-analyses (Carr et al., 2020, 2023; Fares-Otero, De Prisco, et al., 2023). However, these categories remained broad, encompassing studies with conceptually diverse constructs and measures. We summarized the associations of CM with (a) social connectedness and social-cognitive processes, (b) attachment and EMS, (c) sexuality, (d) aggression, (e) intimate partner relationships, (f) IPV and revictimization, and (g) parenting behavior.
Comprehensive details of all included studies are available in Table S.1 on the Open Science Framework (OSF), accessible via the following link (under the ‘Files’ tab): https://osf.io/6qcun/?view_only=e753d74927c44cb09db231ee4747f480. Figure 2(A) shows the distribution of social functioning domains examined across studies, with IPV and revictimization being the most frequently studied domains of social functioning (n = 106), while sexuality emerged as the least explored domain (n = 14). Figure 2(B) visualizes the associations explored between different types of CM and various domains of social functioning in the included studies. Note that in most studies, CM was assessed as an overall measure that combined multiple types, meaning most associations do not correspond to specific forms of CM. Physical abuse (87.54%) and sexual abuse (83.63%) were the most commonly examined forms of CM, whereas emotional abuse (67.62%), emotional neglect (52.67%), and physical neglect (53.02%) were assessed less frequently.
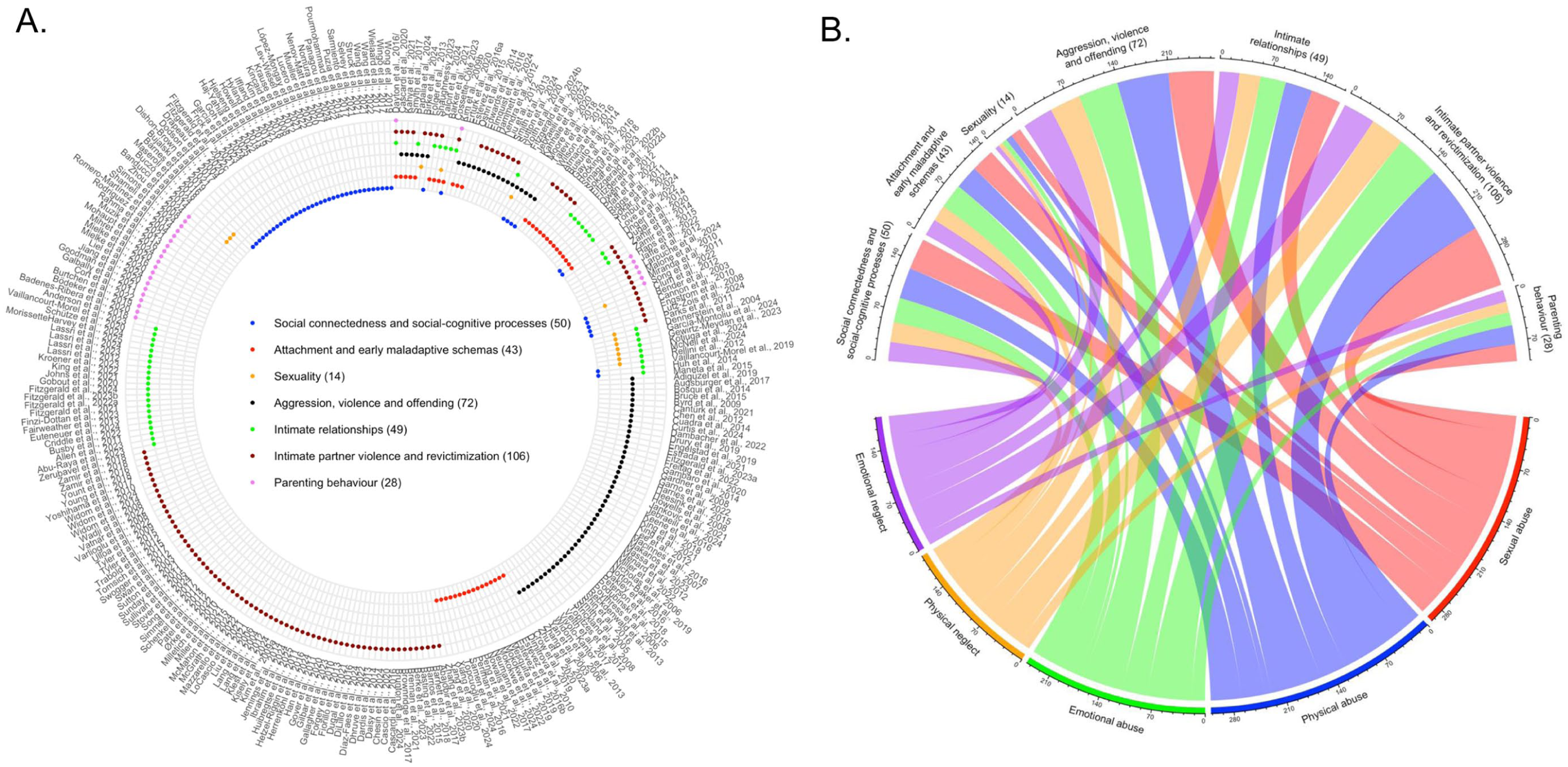
Domains of social functioning explored in each study (A), and explored associations between types of CM and domains of social functioning (B).
Social Connectedness and Social-Cognitive Processes
Fifty studies investigated the relationship between CM and social connectedness as well as social-cognitive processes.
Social Connectedness
Social connectedness refers to an individual’s sense of belonging within a social network, encompassing feelings of closeness, mutual support, and meaningful relationships (Lee & Robbins, 1995). It was most commonly measured using questionnaires that assess social support (e.g., Perceived Social Support Scale; Procidano & Heller, 1983), the size of social networks (e.g., Lubben Social Network Scale; Lubben, 1988), or loneliness (e.g., UCLA Loneliness Scale; Russell, 1996).
Social Network and Social Support
Thirteen cross-sectional studies and four longitudinal studies consistently demonstrated a small to moderate negative correlation between CM and social support, as well as smaller social networks. The majority of these studies were conducted among North American college students, although similar findings were also reported in clinical and non-clinical populations and forensic samples. Individuals with CM reported lower perceived support from both family and friends. Whereas different types of CM were not systematically compared, emotional neglect, emotional abuse, and physical neglect showed higher correlations with low social support than sexual or physical abuse. Among these, emotional neglect demonstrated a particularly strong negative association with social connectedness to family members.
Loneliness and Lack of Belongingness
Moderate positive associations have been identified between loneliness, as well as a lack of belongingness, and CM in six cross-sectional and one longitudinal study. These links were observed in both community samples and clinical populations, including individuals with persistent depressive disorder (PDD) or BPD. Among all CM types, emotional abuse and neglect demonstrated the strongest associations with loneliness and thwarted belongingness in both clinical and non-clinical samples. Physical abuse showed a small positive association with thwarted belongingness, while sexual abuse was not significantly related in a healthy sample. Survivors of childhood sexual abuse reported less mattering to parents but showed no difference in their sense of mattering to friends than participants without the experience of abuse.
Social-Cognitive Processes
This paragraph includes studies on various social competencies and social-cognitive and -emotional processes, such as empathy and theory of mind, which were assessed using a range of different methods.
Social Competences
Overall, the findings of 11 cross-sectional and one longitudinal study revealed a significant association between CM and reduced social competencies, which encompassed aspects such as decreased social adjustment and prosocial activities, as well as increased withdrawal, emotional sensitivity, need for approval, a lack of sociability, and more domineering and intrusive behaviors. This association was observed across diverse populations, including university students, adults with and without low birth weight, and patients with schizophrenia, schizoaffective disorder, bipolar disorder, personality, mood, and anxiety disorders, but not in healthy controls and veterans with PTSD and/or depression.
Empathy and Theory of Mind
Physical abuse was associated with cognitive, but not affective, empathy deficits in both community and forensic samples. However, a study with a mixed sample (i.e., clinical and non-clinical) reported the opposite effect, while no significant correlation between CM and empathy was found in a community sample. In adult patients with PDD compared to those with episodic depression or healthy controls, general CM was associated with heightened empathic distress and interpersonal problems, with medium to large effect sizes. In sum, the nine cross-sectional studies exploring the relationship between CM and empathic concern or perspective-taking (Theory of Mind) have yielded highly inconsistent results.
Social Expectations and Interactions
Evidence from five cross-sectional and two longitudinal studies suggests that individuals with experiences of CM may carry negative expectations and mistrust into social interactions, which can shape both their perceptions of others and the way they interact with them. For instance, individuals with CM history may have a heightened desire to feel comfortable in social settings, yet simultaneously expect to receive less social support. They may also experience more social embarrassment and social anxiety. However, one study found no link between CM and fear of evaluation. In social interactions, individuals with CM may encounter more critical reactions from others and face higher levels of social rejection from peers.
Attachment and EMS
Anxious and Avoidant Attachment
According to attachment theory, a secure attachment with an attachment figure (e.g., caregiver/partner) is marked by comfort with emotional closeness and intimacy. In contrast, insecure attachment styles manifest as either (a) anxiety, with fear of abandonment and preoccupation with intimacy, or (b) avoidance, marked by emotional distance and a discomfort with closeness (Bowlby, 1982). A total of 33 cross-sectional studies and two longitudinal studies examined the relationship between CM and attachment, with the Experiences in Close Relationships Scale (ECR; Wei et al., 2007) being the most commonly used measure.
The studies revealed significant positive associations, ranging from weak to strong, between CM and both anxious and avoidant attachment styles. Notably, the associations were generally stronger with emotional abuse than with physical or sexual abuse, especially in the case of anxious attachment. The strength of these associations appears to be influenced by factors such as the abused individual’s gender, with one study noting a slightly stronger relationship between emotional abuse and attachment in women than in men. Moreover, stronger associations were found between CM and attachment to caregivers or romantic partners compared to friends. No significant correlations were found between CM and secure attachment or close and dependent attachment.
EMS
According to Schema therapy (Young et al., 2003), EMS are pervasive patterns of thoughts, emotions, and behaviors that develop in early childhood as a result of unmet core emotional needs. The schemas can be characterized into the five domains: Disconnection/Rejection, Impaired Autonomy, Impaired Limits, Other-Directedness, Overvigilance, and Inhibition. In total, nine cross-sectional studies investigated the relationship between CM and EMS, with Young Schema Questionnaire (Young & Brown, 1990) being the most commonly used assessment tool. These studies consistently found significant associations, with the most pronounced associations observed for emotional abuse/neglect. The “Disconnection/Rejection” schema domain, encompassing EMS such as social isolation, emotional deprivation, abuse, and defectiveness, showed one of the strongest links to CM. In addition, schemas related to failure and vulnerability to harm, both part of the “Impaired Autonomy” domain, also displayed notably strong associations with CM. In contrast, evidence concerning other domains, such as “Other-Directedness,” was less conclusive.
Sexuality
Fourteen studies explored the relationship between CM and sexuality, with the majority focusing exclusively on female participants. Each study employed a different measurement approach, and six of these studies specifically examined the relationship between sexual and/or physical abuse and sexual outcomes.
Sexual Functioning and Well-being
The nine cross-sectional and two longitudinal studies examining the relationship between CM and adult sexual functioning found weak associations. Women with a history of CM reported lower levels of sex drive, sexual activities, sexual motivation, and sexual communication, as well as reduced arousal, fewer orgasms, and higher levels of sexual shame and sexual problems. Sexual satisfaction was negatively associated with CM in three studies, with weak effect sizes observed in both women and men.
Sexual Risk-Taking
In three cross-sectional and one longitudinal study, all forms of CM, with the exception of emotional neglect, were significantly associated with risky sexual behavior, such as unprotected sex with casual partners, compulsive sexual behavior (hypersexuality), partner concurrency, exchanging sex for drugs, and behaviors linked to HIV risk. The associations ranged from weak to moderate in strength, with the strongest effect sizes observed for sexual abuse.
Aggression, Violence, and Offending
A total of 72 studies were identified, most of which utilized the Buss-Perry Aggression Questionnaire (Buss & Perry, 1992) to measure aggression and the Conflict Tactics Scale (CTS; Straus, 1979) to assess violence, or relied on data from official police records.
Aggression
The 40 cross-sectional and five longitudinal studies, primarily involving community, psychiatric, or forensic samples, reported a positive association of weak to moderate strength between CM and general aggression. Although types of CM were not statistically compared in these studies, associations appeared strongest for emotional and physical neglect and abuse. Furthermore, the gender of both the abusive and abused individuals seemed to influence the strength of the association. For example, emotional or sexual abuse by the father was linked to higher aggression in women, while less maternal but higher paternal physical abuse was associated with increased aggression in men. Stronger correlations were found in populations exposed to additional stressors, such as veterans, refugees, and psychiatric patients, compared to community samples.
When examining distinct dimensions of aggression–such as physical aggression, verbal aggression, anger, and hostility–associations with CM appear to be most pronounced between physical abuse and physical aggression, and the links tend to be stronger for anger and hostility than for verbal aggression. Furthermore, positive associations were observed across a wide range of outcome measures, including trait hostility, hostile cognitions, hostile attribution bias, hostile-dominant interpersonal style/problems, hostility following military deployment, trait anger, outward anger-related behaviors, trait physical and verbal aggression, appetitive and reactive aggression, impulsive/premeditated aggression, psychological aggression, and even sexual aggression.
Violence and Offending
The association between CM and violent behavior, including violent sexual offending, has been addressed in 20 cross-sectional and seven longitudinal studies. Significant positive correlations of weak to moderate strength have been reported between CM and various outcomes, including a lifetime propensity for violence, a history of violent (assaultive) behavior, violence risk or tendency, criminal thinking, the frequency of violent behavior and violent arrests, child-to-parent violence, elder abuse, sexual violence perpetration, and stalking. The heightened risk for violence after CM was corroborated by six large longitudinal studies.
Certain aspects of the abuse, such as its type, the cumulative number of adversities, or the re-experience of violence during adulthood, have been found to increase the risk for subsequent violence. Specifically, stronger associations with violence were found for physical, emotional, or sexual abuse compared to physical and emotional neglect. Violence and CM were particularly correlated in individuals with mental disorders, such as schizophrenia, within forensic populations. The only six studies, however, in which no significant association between CM and aggression or violence was found, were carried out in forensic or psychiatric settings, suggesting the influence of additional risk factors for aggression and violence in these populations. The results regarding gender effects remain inconclusive, though a pattern has emerged linking the type of CM to the type of offending. Physical abuse showed a comparatively higher correlation with non-sexual violence, while correlations were higher between sexual abuse and sexual violence.
Intimate Relationships
A total of 49 studies were identified. The majority of the studies (31 cross-sectional and 6 longitudinal) explored the relationship between CM and the quality or satisfaction with adult intimate relationships, typically using the Couple Satisfaction Index (Funk & Rogge, 2007) or the Dyadic Adjustment Scale (Sabourin et al., 2005). Overall, most of the studies were cross-sectional (n = 42) and included community samples (n = 29).
Relationship Satisfaction and Quality
Overall, 26 studies, mostly cross-sectional, found a negative correlation between CM and relationship satisfaction in adulthood. However, the effects were generally weak when considering general CM experiences. The strongest negative correlations were observed for emotional abuse, while results remained inconclusive for other forms of CM, such as physical abuse and sexual abuse, with two studies finding no significant correlation. In addition, the results suggest a stronger association between CM and relationship satisfaction in women compared to men. The results of twelve studies indicate a negative association between experiences of CM and relationship quality (including subdimensions such as affection and love) in adulthood. Emotional abuse emerged as a predominant subtype of CM, while findings for other subtypes remained inconclusive or under-researched.
Problematic Behaviors in Intimate Relationships
Eleven cross-sectional and two longitudinal studies, involving community, undergraduate, forensic, and other samples, reported weak to moderate associations between CM and various types of problematic behaviors in intimate partnerships. CM was linked to increased levels of openly expressed anger and aggression within the family, marital strain, directiveness, conflicts, and hostility, as well as verbal aggression toward partners. In addition, CM was related to a tendency to conceal distressing or negative information about oneself. CM was associated with reduced responsiveness, more negative communication patterns, lower commitment, lower marital support, and more detachment, and at the same time, it was linked with higher dependency and rejection sensitivity in intimate relationships. Three studies also provided preliminary evidence suggesting that CM shows a weak to moderate association with perceiving one’s partner more negatively and making negative attributions about their behavior.
IPV and Revictimization
IPV
Ninety-seven studies (75 cross-sectional and 22 longitudinal) investigated the association between CM and IPV. Approximately three-quarters of these studies used the CTS to assess IPV with a primary focus on various domains of violence, such as physical, sexual, and emotional or psychological violence. In 23 studies, IPV was examined bidirectionally, while 48 studies focused on IPV victimization (violence from partner toward the study participant) and 26 studies on IPV perpetration (violence from study participant toward the partner). Thirty-nine studies focused exclusively on female participants while primarily examining IPV victimization, and eleven studies focused solely on male participants, mostly investigating IPV perpetration.
With the exception of four studies, all studies consistently reported at least a weak to moderate association between some form of CM and IPV. CM was found to be related to both IPV victimization and perpetration in women and men. Notably, 10 out of 11 prospective studies that followed children and adolescents with CM experiences into adulthood reported elevated rates of physical and/or psychological IPV victimization and/or perpetration. An epidemiological study examining specific effects of different types of CM on IPV in a nationally representative sample of over 25,000 U.S. adults confirmed that CM is related to more reciprocal intimate violence. So far, there is limited evidence for specific associations between CM types and the types of adult IPV (sexual, emotional, or physical) across studies. However, childhood sexual abuse appears to have an additional specific link with general IPV victimization in both women and men. There is some evidence that the associations between CM and IPV vary between men and women, depending on the type of CM. Childhood sexual abuse and physical neglect appear to be more consistently associated with both victimization and perpetration in women, whereas emotional abuse may be a more relevant factor in men. The association between CM and IPV appears to be particularly high in populations exposed to multiple cumulative risks, such as veterans, parental mental and substance use problems, inter-parental violence, family conflicts, poverty, and socially disadvantaged neighborhoods.
Revictimization
Seven cross-sectional and three longitudinal studies consistently reported a significant positive association between CM and revictimization in adulthood. The findings were similar for male and female participants and appeared to be stronger in specific groups facing additional stressors, such as individuals who were deaf or hard of hearing or those living in communities with higher poverty rates. Some evidence suggests that childhood sexual abuse may be a stronger predictor of sexual and physical violence in adulthood compared to physical abuse. Certain characteristics of childhood sexual abuse, such as use of physical force or the age at which the abuse began, emerged as significant predictors of sexual revictimization. However, exposure to any form of CM may have a stronger association with revictimization than the specific type of CM experienced.
Parenting Behavior
A total of 28 studies examined the relationship between parental experiences of CM and subsequent parenting behavior. Most of the studies focused on one or two specific types of CM and utilized a variety of measures to assess parenting behavior, such as the Emotional Availability Scales (Pipp-Siegel & Biringen, 1998). Notably, only eight studies also included male participants (fathers).
Parental Sensitivity and Parental-Child-Bonding
Eleven cross-sectional and four longitudinal studies investigated the following links. The association between CM and parental sensitivity/competence and/or parental-child-bonding was investigated in 10 studies, parental reflective functioning in 2 studies, and parental self-efficacy and maternal representation of the child were each investigated in 1 study. Results regarding CM and paternal sensitivity were inconsistent. Three studies reported no significant association, while four studies found a weak negative association between CM and maternal sensitivity, although this was not observed for emotional availability. Furthermore, CM was negatively related to parental reflective functioning/ meta-parenting and parenting self-efficacy. CM was also negatively associated with mother-infant bonding and child-mother relationship quality. In addition, pregnant women with experiences of physical neglect were more likely to exhibit distorted prenatal representations of the child, characterized by inconsistency and unrealistic expectations. The studies did not compare different types of CM.
Risk for Child Maltreatment
The risk for CM has been examined in 12 cross-sectional studies and 1 longitudinal study. Despite variations in measurements and methodology, all but one study revealed a significant association between parental experiences of CM and an expected heightened risk of maltreatment in their offspring and maladaptive parenting practices and attitudes. Five studies found weak to moderate correlations between childhood sexual abuse and parental maltreatment behavior. Moreover, parents who had experienced physical abuse and/or emotional victimization were more likely to report positive attitudes toward physical discipline and an increased child abuse potential. Finally, in a forensic sample, individuals convicted of child sexual offending were more likely to have experienced sexual abuse during childhood.
Summary of Main Findings
Overall, the majority of studies suggest a predominantly positive association between CM and impairments in multiple domains of social functioning. Using a harvest plot, Figure 3 displays the distribution of findings and direction of associations across the domains and study designs. The associations were generally of small to moderate strength and varied depending on both the type of CM and the social functioning outcome. As displayed in Figure 3, the strongest body of evidence emerged for the domains of IPV, aggression, social connectedness, attachment, EMS, and risk of CM. In contrast, the domains of sexuality, intimate partner relationships, parental sensitivity, and social-cognitive processes (i.e., empathy and theory of mind) have been less extensively studied and show less consistent findings.

Harvest plot of associations between child maltreatment and social functioning outcomes across study designs.
Mediators and Moderators of the Link Between CM and Social Functioning
In the following, we will summarize mediators and moderators of the relationship between CM and specific domains of social functioning identified in research to date. Table 1 provides a structured overview of all identified mediators and moderators, clustered into three overarching categories: psychological processes, interpersonal patterns, and contextual factors. Moreover, we report the number of cross-sectional and longitudinal studies for each SF domain, given the limitations of cross-sectional data for mediation and moderation modeling. The most frequently identified mechanisms are presented in Figure 4. Further details regarding all mediators and moderators are provided on the OSF in Table S.1.
Mediators and Moderators Linking Child Maltreatment and Social Functioning Domains.
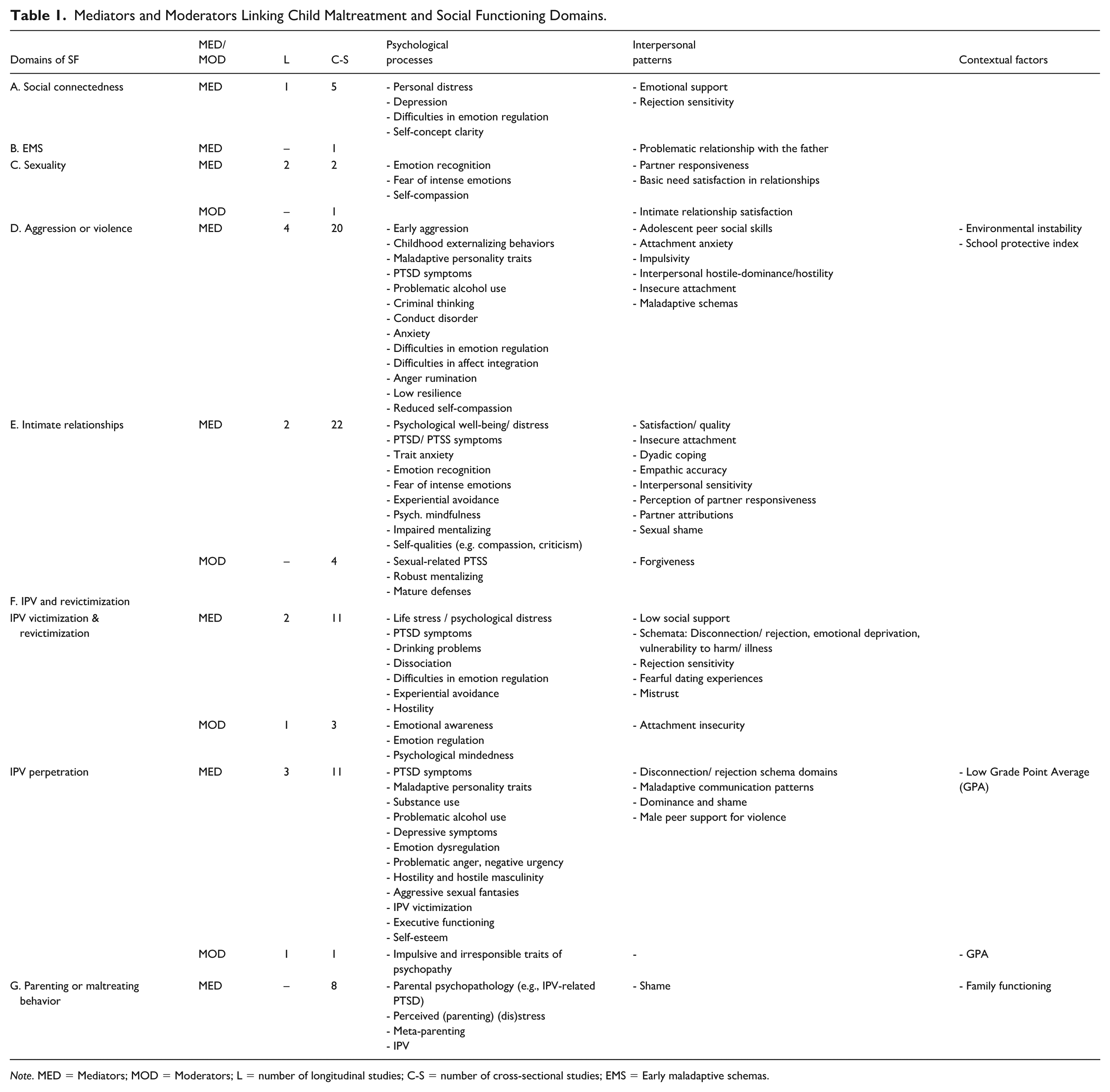
Note. MED = Mediators; MOD = Moderators; L = number of longitudinal studies; C-S = number of cross-sectional studies; EMS = Early maladaptive schemas.
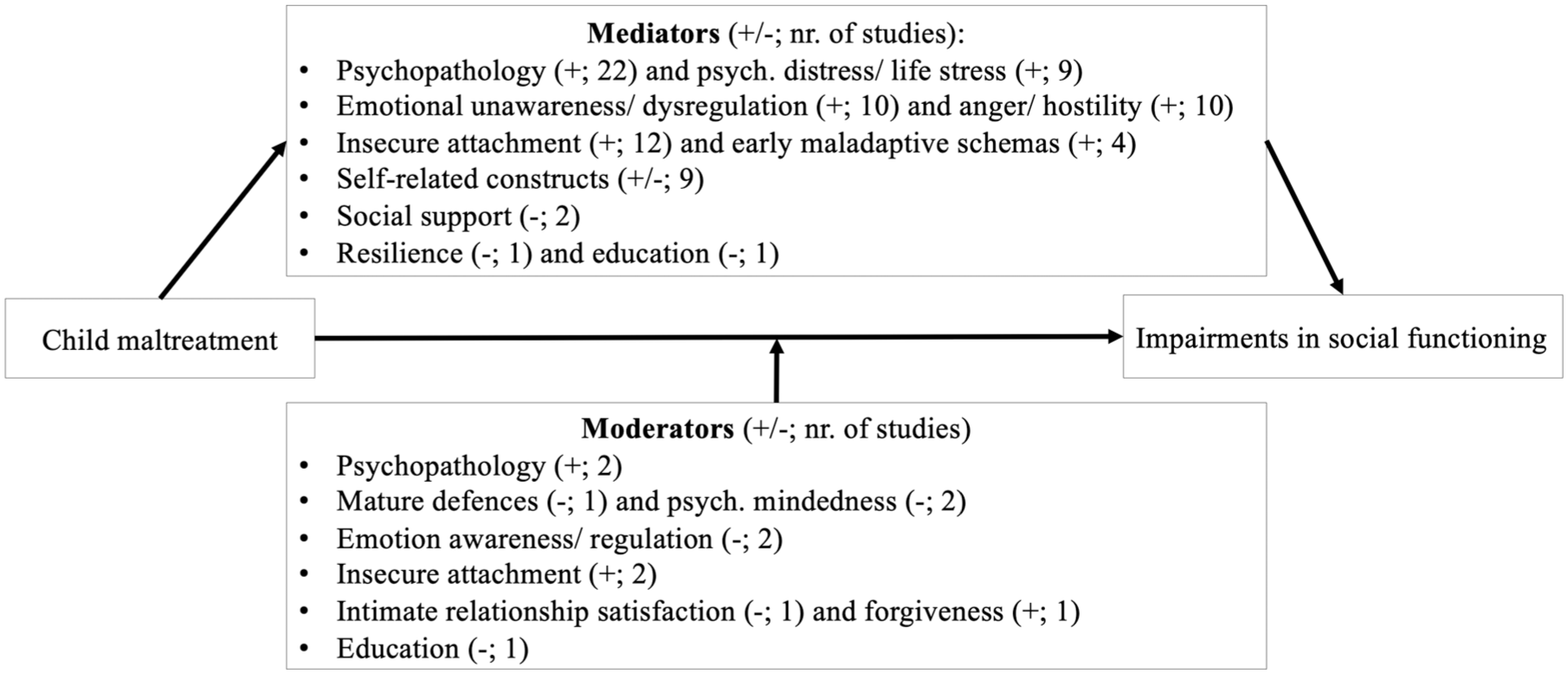
Mediators and moderators between child maltreatment and impairments in social functioning.
Discussion
Impairments in social functioning might be associated with CM experiences across the population and are prominent in many mental disorders. Following our goal to develop interventions for improving social functioning in individuals with CM, we were interested in which social deficits are related to which types of CM and which mediators and moderators need to be considered. Differentiating between domains of social functioning and linking social dysfunction to CM as a potential correlate or risk factor can support the development of transdiagnostic models of social dysfunctions and mechanism-based interventions (Goerigk et al., 2023).
Relationship Between CM and Social Functioning
We found an association between CM and fundamental social competencies and their application in specific domains of social functioning, confirming previous reports (Carr et al., 2020; Haslam et al., 2020). Interestingly, the strength of the associations ranged from small to moderate and varied based on the type of CM and the specific social function. The strongest evidence emerged for IPV, aggression, social connectedness, attachment, and EMS, whereas findings for other domains, including sexuality, intimate partner relationships, and social-cognitive processes, were more inconsistent. The negative association between CM and social connectedness was reflected in lower social support, increased loneliness, interpersonal difficulties, diminished relationship satisfaction, and negative social expectations, while findings on empathic concern and perspective-taking were mixed. Weak to strong associations emerged between CM, particularly emotional abuse, and insecure attachment, as well as EMS. In terms of sexual health, studies found weak associations between CM, particularly sexual abuse, and reduced sexual functioning, satisfaction, and increased risky sexual behaviors. CM also correlated weakly to moderately with physical and verbal aggression, hostility, anger, violence, and offending, with stronger associations for physical, emotional, or sexual abuse. Most studies consistently revealed at least weak to moderate associations between some form of CM and IPV, both as victimization and perpetration, as well as to revictimization. Research has documented associations often described in the context of intergenerational patterns of CM, with parental CM history being correlated with child maltreatment (CM) risk and maladaptive parenting, though findings on parental sensitivity were inconsistent.
Potential Mechanisms in the Link Between CM and Social Functioning
A secondary objective was to identify potential mechanisms in the sense of mediating and moderating factors within the association between CM and impaired social functioning. Across studies and domains, the most frequently observed factors included psychopathology, insecure attachment, and emotion dysregulation, which is consistent to previous reports (Fares-Otero, Alameda, et al., 2023; McNeil & Rehman, 2024; Shahab et al., 2021).
First, the most commonly identified mediators and moderators were psychopathology and psychological distress, including a range of conditions, such as PTSD symptoms, personality traits (including antisocial, borderline, and narcissistic tendencies), maladaptive personality features, traits of psychopathy, depression, social anxiety, dissociation, problematic substance use, and conduct disorder. This pattern may suggest that impaired social functioning co-occurs with or follows CM-related psychopathology. However, cross-sectional designs limit inferences regarding temporal causality. It remains unclear whether the strength of the CM-social functioning association differs between adults with and without psychopathology, and a deeper understanding of the complex interactions among the types of CM, psychopathology, and social functioning is needed.
Second, attachment insecurity appeared not only as an outcome but was also investigated and reported as a significant mediator and moderator in the relationship between CM and other domains of social functioning, such as IPV victimization and revictimization, antisocial behavior and criminal thinking, as well as various relationship characteristics, including quality, satisfaction, respect, attributions, and dyadic adjustment. This aligns with models proposing that attachment security–alongside early schemas, and sociocognitive competencies, for example, social perception, sharing, and mentalizing–are fundamental elements that develop continuously from a very young age (Flechsenhar et al., 2022). These elements are theorized to be influenced by early experiences, including CM, and are thought to underlie more complex social processes and domains of social functioning. These include the ability to build and maintain satisfying interpersonal relationships, resolve conflicts, navigate aversive social situations, and care for children. In line with this, Pfaltz et al., 2022 suggested that it is crucial to identify attachment-related changes that contribute to broader social functioning difficulties, such as a lack of perceived social support.
Lastly, emotional regulation and awareness were the third most often reported mediating or moderating factor in seven studies investigating the association between CM and the availability of social support, trait anger, IPV perpetration, and victimization. McNeil and Rehman (2024) emphasize the importance of recognizing internal factors, such as emotional awareness and regulation, which can enhance communication skills and, in turn, improve external factors like the social network size.
Implications for Clinical Practice and Future Research
This systematic review offers valuable insights into the relationship between different types of CM and various domains of social dysfunction. Firstly, one of the most important findings is the non-specificity of CM sequelae in the sense of a rather widespread association of different types of CM with very different domains of social functioning, ranging from fundamental social competencies (e.g., empathy) to specific domains (e.g., sexuality). Therefore, clinicians and researchers across clinical, community, and preventive contexts should assess CM types and domains of social functioning comprehensively in individuals with CM experiences. Interestingly, emotional abuse and neglect showed the strongest and broadest associations across multiple domains of social functioning such as social connectedness, attachment, EMS, aggression, as well as relationship satisfaction and quality (Fares-Otero, De Prisco, et al., 2023; Haslam & Taylor, 2022). Yet these forms of CM were among the least studied in existing literature and are often underrecognized in clinical settings and therefore require more attention. In contrast, childhood sexual abuse appeared to be more consistently associated with outcomes related to sexuality and interpersonal victimization, whereas childhood physical abuse might be more specifically linked to aggressive outcomes. However, a key limitation of the present review is that effect sizes were not systematically comparable across CM subtypes or social functioning outcomes, precluding formal comparisons. Future research should therefore conduct focused, domain-specific, and subtype-specific meta-analyses to quantify and compare the relative strength of associations across different forms of CM.
Secondly, the role of psychopathology as the most frequent mediator suggests that social dysfunction may be associated with other psychopathological symptoms and could improve through targeting them. An alternative hypothesis, however, would be that both may reinforce each other in a bidirectional cycle of chronicity. Consequently, social dysfunction should be considered as a therapeutic target in clinical practice, with future research directly examining its impact on other psychopathological symptoms to help break these possible reinforcing cycles. Thirdly, insecure attachment, maladaptive schemas, and emotion dysregulation are key processes linking CM to social dysfunction. Therapeutic approaches that address these underlying mechanisms (e.g., DBT, MBT, and CBASP) may improve interpersonal outcomes across diagnostic categories.
Finally, although many of the reported associations were characterized by weak to moderate statistical effect sizes, the lack of established clinical benchmarks for most social functioning outcomes limits direct inferences regarding clinical significance. Consequently, the review emphasizes the need for a more consistent definition of social functioning and a more comprehensive, nuanced assessment of its various domains and establishment of clinically meaningful thresholds. Future research would benefit from more high-quality mixed-method designs with real-life longitudinal assessments of social functioning to better understand causal relationships and temporal dynamics, particularly in underexplored domains (e.g., sexuality and parenting behavior). This would help improve comparisons across studies. Prospective longitudinal studies are also necessary to more closely study the relationship between social dysfunction and other symptoms of psychopathology in CM survivors. In addition, a deeper exploration of underlying mechanisms is essential for developing personalized transdiagnostic treatments that address specific social impairments in individuals with CM. The review suggests that insecure attachment, EMS, and deficits in emotion regulation may be more general outcomes of CM. However, it remains unclear whether specific types of CM are linked to distinct patterns within these domains and whether these patterns, in turn, contribute to more complex social dysfunctions, such as challenges with social connectedness, parenting, or aggression.
Strengths and Limitations
While the current review boasts several strengths, including a thorough examination of the association of CM with various domains of social dysfunction and a focused synthesis of key trends and gaps in the literature, it is important to acknowledge some notable limitations. First, we did not calculate general effect sizes or meta-analytic relationships across studies, limiting our ability to provide quantitative summaries or pooled estimates of the outcomes. Although the number of included studies might suggest the feasibility of a meta-analysis, the considerable heterogeneity across studies in terms of conceptualization, measurement, and reporting of social functioning as well as populations, exposure types, and analytic strategies, precluded meaningful quantitative synthesis. Conducting a meta-analysis would have risked producing misleading or non-generalizable conclusions. Instead, our goal was to provide a comprehensive synthesis to map the domains of social functioning affected by childhood trauma, identify gaps in the literature, and inform future research directions and clinical practice.
Second, an important limitation of this review is the absence of double screening and double data extraction. Given the large volume of articles screened (n = 5,739) and included (n = 281), titles, abstracts, or full-text screening were conducted by a single reviewer, and data extraction was not independently verified by a second reviewer. This approach deviates from best practice for systematic reviews and may increase the risk of selection bias, missed studies, and extraction errors. To mitigate these risks, we followed predefined eligibility criteria, piloted the screening and extraction forms, and documented all decisions. However, these steps cannot fully replace independent verification and this limitation should be considered when interpreting the findings. Third, we did not distinguish between different methods of CM assessment. In most studies, CM was assessed through retrospective recall and self-report, with the CTQ being one of the most commonly used instruments.
In addition, the studies included in this systematic review present several important limitations that should be considered when interpreting the findings. First, the majority relied on cross-sectional data (83.3%), limiting causal inference. Second, the evidence base is dominated by WEIRD (White, Educated, Industrialized, Rich, Democratic) samples, which constrain the cultural validity of the findings and likely reflect culturally specific norms regarding social relationships. Consequently, the relevance of these results for non-WEIRD populations remains uncertain. Importantly, culture may interact with gender, as both CM and SF are shaped by sociocultural context. A gender bias might have confounded the literature, as 57% of the participants across studies were female, and research of several SF domains, particularly IPV, sexuality, and paternal behavior, focused predominantly on one gender and specific types of CM (e.g., the impact of sexual abuse on sexual revictimization in women). Such gender-specific approaches often align with prevailing stereotypes and potentially obscure gender-specific mechanisms. This focus limits the generalizability of findings across gender-diverse perspectives and all forms of CM. As such, future research should prioritize culturally diverse samples, adopt gender-inclusive designs, and systematically explore the effects of various types of CM and their outcomes (e.g., victimization and perpetration) across diverse populations, ensuring balanced representation and consideration of all relevant factors.
Conclusion
CM, both in its general form and across distinct subtypes, appears to be linked with dysfunction in various domains of social and interpersonal functioning, with mostly small to moderate associations. These findings highlight the importance of comprehensively assessing CM and its effects on social functioning in both clinical practice and research. This includes evaluating general abilities (such as empathy and attachment), specific domains (like sexuality), and a range of relationships (including work, friendships, partnerships, and family). Such an approach can help facilitate the early identification of trauma histories and contribute to the development of more targeted and effective interventions for interpersonal dysfunctions. Potential mechanisms mediating the relationship between CM and social dysfunction, such as psychopathological symptoms, insecure attachment, and emotion dysregulation, have already been identified and may serve as transdiagnostic targets for interventions. However, most evidence to date is correlational and based on cross-sectional designs. Future longitudinal research is crucial for further clarifying the pathophysiological pathways linking CM to psychosocial functioning and for refining diagnostic and therapeutic models that address interpersonal dysfunctions.
Critical Findings of the Review.
Implications for Research, Practice and Policy.
Supplemental Material
sj-docx-1-tva-10.1177_15248380261439146 – Supplemental material for Old Scars Don’t Hurt? A Systematic Review on the Association Between Child Maltreatment and Adult Social Functioning
Supplemental material, sj-docx-1-tva-10.1177_15248380261439146 for Old Scars Don’t Hurt? A Systematic Review on the Association Between Child Maltreatment and Adult Social Functioning by Isabelle Göhre, Lea Vogel, Tanja Brückl, Kerstin Hupe, Janina Wollinger, Larissa Wolkenstein, Milena Aleksic, Alma-Sophia Merscher, Anamaria Semm, Nathalie Claus, Stephan Goerigk, Johannes Kopf-Beck, Elisabeth Binder, Frank Padberg, Matthias A. Reinhard, Thomas Ehring and Katja Bertsch in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
None.
ORCID iDs
Author Contributions
F.P., T.E., and K.B. developed the overall research question and review design. Title- and abstract screening was performed by KB, TB, TE, and IG. Full-Text screening, data extraction, and a narrative synthesis were performed by all authors. I.G. and K.B. drafted the manuscript. All authors provided critical revisions and approved the final version of the manuscript for submission.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: I.G., L.V., T.E., L.W, J.K, K.H., J.W., S.G., M.R., F.P, E.B., T.B, and K.B. are supported by the German Center for Mental Health (DZPG) funded by the Federal Ministry of Education and Research (Bundesministerium für Bildung und Forschung [BMBF]) and the Ministry of Bavaria (01EE2303A) and the current review was part of the DZPG project MUC-1 Early Trauma.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The extracted data supporting this review’s findings are available on request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.