
Abstract
The aim of this study was to systematically evaluate the effectiveness of parenting interventions for improving parenting outcomes among general families with children under 3 years of age and without special conditions. Literature retrieval was carried out in six databases, including PubMed, Web of Science, Cochrane Library, Scopus, PsycINFO, and CINAHL. A total of 8,248 articles were screened against prespecified criteria. Findings of included studies were synthesized and if data were available, meta-analysis using random effects model was conducted. Subgroup analyses were conducted to test the effect of several moderators (intervention types, intervention duration, time lag between the end of intervention and first post-intervention measurement) in explaining the heterogeneity of the results. Twenty articles from 19 studies met the inclusion criteria for the systematic review, of which 14 studies provided sufficient data for meta-analysis. Compared to control groups, parenting interventions significantly reduced parenting stress (standardized mean difference [SMD] = −0.30, 95% confidence interval [CI] [−0.45, −0.15], p < .001, n = 9), and increased parenting self-efficacy (SMD = 0.61, 95% CI [0.12, 1.10], p = .02, n = 9). Only one study on child maltreatment outcome was retrieved and it reported that child maltreatment was reduced after intervention. No statistically significant differences in the pooled effect size across pre-specified moderators were observed. Among families without special conditions, parenting interventions showed effectiveness in reducing parenting stress and improving parenting self-efficacy, suggesting families at low risk can benefit from parenting interventions. Implications for future practice and research are discussed.
Introduction
Parenting perhaps represents the most enlightening, gratifying, and fulfilling social role in one’s life. The vast majority of parents are happily adjusting to parenthood in the first 3 years, in which challenges and difficulties are inevitable. If these challenges are not addressed properly, parents are likely to experience psychological problems and exhibit coercive parenting practices, which can not only affect parents themselves, but also directly or indirectly impact child development (Fuchs et al., 2022; Han et al., 2024; Khalsa et al., 2022; Mclean et al., 2022).
Parenting stress and parenting self-efficacy are among the most commonly used psychological indicators of adaptation to the parental role. A rich body of literature has documented that they can impact parental mental health (J. Brennan et al., 2024; Daundasekara et al., 2021), marital satisfaction (Dong et al., 2022), personal and family quality of life (Han et al., 2024; Vahedparast et al., 2022), and even children’s physical, mental, and social development (Klein & McDonald, 2024; Lean et al., 2018; Yaman et al., 2010). In addition, coercive parenting practices, especially child maltreatment, can result in adverse child development outcomes (Gnanamanickam et al., 2022; Han et al., 2024).
The first 3 years of life represent a pivotal period that shapes individuals’ future health. Evidence shows that early-life environmental exposures are closely associated with children’s neuro-development, metabolic health, and the formation of psychological resilience (Alley et al., 2025; McLean et al., 2024; Wang et al., 2022). In line with this, research indicates that investments in human capital during this window yield the highest returns, with the earlier the investment, the more significant the long-term returns (Heckman, 2006; Heckman & Masterov, 2007). Parents also acquire essential knowledge about infant and toddler care, develop parenting attitudes, skills and interaction patterns in the first 3 years of life. Parenting outcomes, such as parenting self-efficacy and parenting stress levels in this early stage of life can predict children’s subsequent social adaptability and the quality of parent-child relationships (Barroso et al., 2018; Jones & Prinz, 2005). Therefore, it is of great practical significance to focus on the first 3 years and invest in improving parents’ self-efficacy and reducing their stress during this period.
In order to help parents better adapt to their parental status during the first 3 years, many parenting interventions have been developed (Giallo et al., 2014; McFarlane et al., 2017; Paradis et al., 2011), especially for families with special conditions, such as families of children with Autism Spectrum Disorder (ASD) and other developmental disabilities (Dykens et al., 2014), parents with severe mental illness (Barnicot et al., 2024), or adolescent parents (Barlow et al., 2013; Firk et al., 2015). Findings from most of these randomized controlled trials have showed that these interventions are effective in one of the following outcomes: improving parenting self-efficacy, reducing parenting stress, or decreasing child maltreatment (Shorey et al., 2015; Williams et al., 2020); however, some studies failed to find statistically significant effects on one or more of the aforementioned outcomes (Ammerman et al., 2024; Hutchings et al., 2017).
Several reviews and meta-analyses have been conducted on the effects of interventions for families with special conditions, but the conclusions are inconsistent. For example, a systematic review by Schoemaker et al. (2020) showed that parenting interventions involving Parent-Child Interaction Therapy (PCIT) and Child-Parent Relationship Therapy were effective in reducing parenting stress in foster and adoptive families. Both Burgdorf et al. (2019) and Shorey and Ng (2021) evaluated the effectiveness of mindful parenting interventions for parents, most of whom had children and adolescents with ASD or Attention-Deficit/Hyperactivity Disorder (ADHD) diagnoses, on reducing parenting stress. Burgdorf et al. (2019) reported that parenting stress was alleviated following mindfulness interventions, whereas Shorey and Ng (2021) found no evidence of interventional effect on relief of parenting stress among parents with children up to age 24. Similarly, the systematic review by Coates et al. (2015) reported that overall parenting interventions did not yield significant effect for families with children diagnosed with ADHD, despite one study observed that the intervention could effectively reduce parenting stress (Anastopoulos et al., 1993).
Notably, relatively less research attention has been paid to families without special conditions. The universal tasks of child-rearing, such as fostering secure attachment, promoting self-regulation, and providing consistent nurture and discipline, are challenging for any parent. Epidemiological studies show that parents in the general population also experience high parenting stress, low self-efficacy, and reported high rates of child maltreatment during the first 3 years after childbirth (Hong et al., 2022; Monteiro et al., 2022). If left unaddressed, these issues can lead to the preventable onset of child behavioral and emotional problems (Ansar, 2024; Javier et al., 2016), thereby creating new demands on the selective and indicated service systems. To this end, a substantial number of parenting programs that targeted families without special conditions were developed and tested (Nam et al., 2016; Shorey et al., 2015; Williams et al., 2020), and their findings may be more profound for designing universal parenting programs for public health benefits.
However, a systematic synthesis of the effectiveness of such programs on parenting outcomes during the early stage of parenthood is still lacking, except for the work by Jeong et al. (2021). This review showed that parenting interventions that targeted a population of children or parents without diagnosed illnesses or disabilities during the first 3 years of children’s lives could improve child outcomes, and benefit parenting knowledge, parenting practices, and parent-child interactions. However, it failed to include three important parenting outcomes, parenting stress, parenting self-efficacy, and child maltreatment that were the focuses of this study. Parenting stress and self-efficacy directly shape the care-giving environment, with stress undermining responsive care and self-efficacy promoting the nurturing interactions crucial for healthy child development. Child maltreatment, the most severe form of dysfunctional parenting, often emerges when high stress overwhelms a parent’s limited self-efficacy and coping resources. Therefore, the present systematic review aimed to systematically synthesize the evidence from published randomized controlled trials (RCTs) about the effectiveness of parenting interventions on parenting outcomes, including parenting stress, parenting self-efficacy, and child maltreatment in families with children of 3 years of age or younger and without special conditions. For studies with sufficient data, we performed a meta-analysis to quantitatively estimate the magnitude of the pooled effect size of the intervention effects. We also explored potential moderators of study heterogeneity. The finding of this study were expected to provide implications for designing universal parenting programs for public benefits.
Methods
Operationalization of Study Outcomes
The primary outcomes were parenting stress, parenting self-efficacy, and child maltreatment. Parenting stress is defined as the subjective feeling that results from incongruence between parental ability and demands. Parenting self-efficacy is defined as an extension of Bandura’s concept of self-efficacy to the parenting domain. It refers to the belief that parents have the ability to take care of their own children, that is, the degree of confidence in their own parenting ability. Child maltreatment is the abuse and neglect that occurs to children under 18 years of age (World Health Organization, 2024a, 2024b), and includes physical abuse, emotional abuse, sexual abuse, physical neglect, and emotional neglect. We adopted an inclusive approach and accepted any measurement method that the cited authors themselves specified and labeled as assessing child maltreatment, child abuse or child neglect. Parenting interventions refer to any strategies (e.g., professional guidance, skill training) to help parents optimize their parenting skills, attitudes, perceptions, confidence and other parenting-related factors, thereby directly or indirectly improving the quality of parent-child interaction and child development.
Search Methods and Selection Criteria
Six electronic databases including PubMed, Web of Science, Cochrane Library, Scopus, PsycINFO and CINAHL were searched. Searches were limited to publications of English language from January 2011 to January 2024. We inlcuded all types of interventions, and this review was not preregistered. The search strategy consisted of four blocks of terms related to parenting intervention, infant OR toddler, parenting efficacy OR parenting stress OR child maltreatment, and randomized controlled trial. Complete search terms and strategies for each database are provided in Supplemental Table S1. Four authors independently screened the title, abstract, and full text following the Cochrane guideline. Inconsistencies were resolved by discussion, or through consultation with the corresponding author. Reference lists of eligible studies and relevant reviews on the effectiveness of parenting interventions were hand-searched to locate additional relevant studies.
Randomized controlled trials were included if they: (1) targeted at parents with children aged under 3 years of age; (2) conducted parenting interventions that aimed to reduce parenting stress, improve parenting self-efficacy, or prevent child maltreatment. Studies on special families (i.e., families of children with ASD, ADHD, or other developmental disorders, families of premature children, adolescent parents, parents with diagnosed mental disorders or severe health conditions, and foster families) were excluded.
Data Extraction
Data about publication (first author, publication year, country), population (sex, age, number of participants in intervention and control group), parenting intervention (name, type, duration), outcomes, follow-up time, and the necessary data (means and standard deviations) for meta-analysis of all included studies were extracted by three researchers independently. Disagreements were resolved by discussions. Because five studies did not provide the necessary data (i.e., failure to report standard deviations, means, or to present data stratified by intervention and control groups) for the meta-analysis, and no responses were received after contacting the authors to request the necessary data, therefore they were only included in the systematic synthesis.
Quality and Risk of Bias Assessment
A researcher independently assessed the risk of bias in RCTs using the Cochrane Collaboration’s tool for assessing risk of bias (Higgins et al., 2011), including random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting bias (reporting bias), and other bias. Disagreements were resolved through discussions among the researchers, with input from the principal investigator as needed, until consensus was reached.
Data Synthesis and Analysis
Study findings were first synthesized systematically and described narratively. Then, available data were submitted to meta-analyses using the random effects model, which was a more conservative and recommended option than fixed-effect meta-analyses (Hunter & Schmidt, 2000), due to heterogeneity among research. When studies had multiple post-intervention assessments, we used the earliest available one for meta-analysis. Results were presented as standardized mean differences (SMD) and 95% CI. We conducted sensitivity analysis by removing each included study one by one, then evaluating whether the combined effect size is affected by a single study and changes significantly.
We used τ2 to assess heterogeneity among subgroup analyses instead of traditional I2 because I2 increases with the number of participants included in meta-analysis, even if the true heterogeneity between studies remains unchanged (Rücker et al., 2008). When heterogeneity was high, we identified potential moderators through subgroup analyses based on both prespecified factors and factors identified from the systematic synthesis. The prespecified factors included intervention types (educational vs. interactive vs. home visiting vs. composite vs. others), intervention duration (less than 1 month vs. 1–3 months vs. more than 3 months), and time lag between intervention endpoint and the first post-intervention measurement (immediately after intervention (< 1 week) vs. others (≥ 1 week or unclear)).
Funnel plots were used to test for publication bias and no significant publication bias was detected. All analyses were performed with Review Manager 5.4 and STATA 15 (StataCorp, College Station, Texas, USA).
Results
Study Selection
A total of 8,248 articles were identified from the six databases and relevant reviews, 1,903 of which were duplicates. After four independent reviewers strictly screened the titles and abstracts, the full-texts of 385 potentially eligible articles were obtained for further assessment. After full-text screening, 20 articles from 19 studies (n = 5,681) with two articles from the same study were retained for the systematic review. Among them, seven focused on only parenting stress, six only on parenting self-efficacy, five on both parenting stress and parenting self-efficacy, and one on both parenting stress and child maltreatment. From these 19 studies, 14 studies (n = 2,195) that provided necessary data were further included for the meta-analysis (Ammerman et al., 2024; Baziyants et al., 2023; Booth-LaForce et al., 2020; Cates et al., 2016; Fernandes et al., 2022; Giallo et al., 2014; Hutchings et al., 2017; Kohlhoff et al., 2021; Mannocci et al., 2022; Olofsdotter Lauri et al., 2023; Outhwaite, 2023; Shorey et al., 2015; Wigglesworth et al., 2023; Williams et al., 2020). The flow diagram (Figure 1) presents the study screening progress.
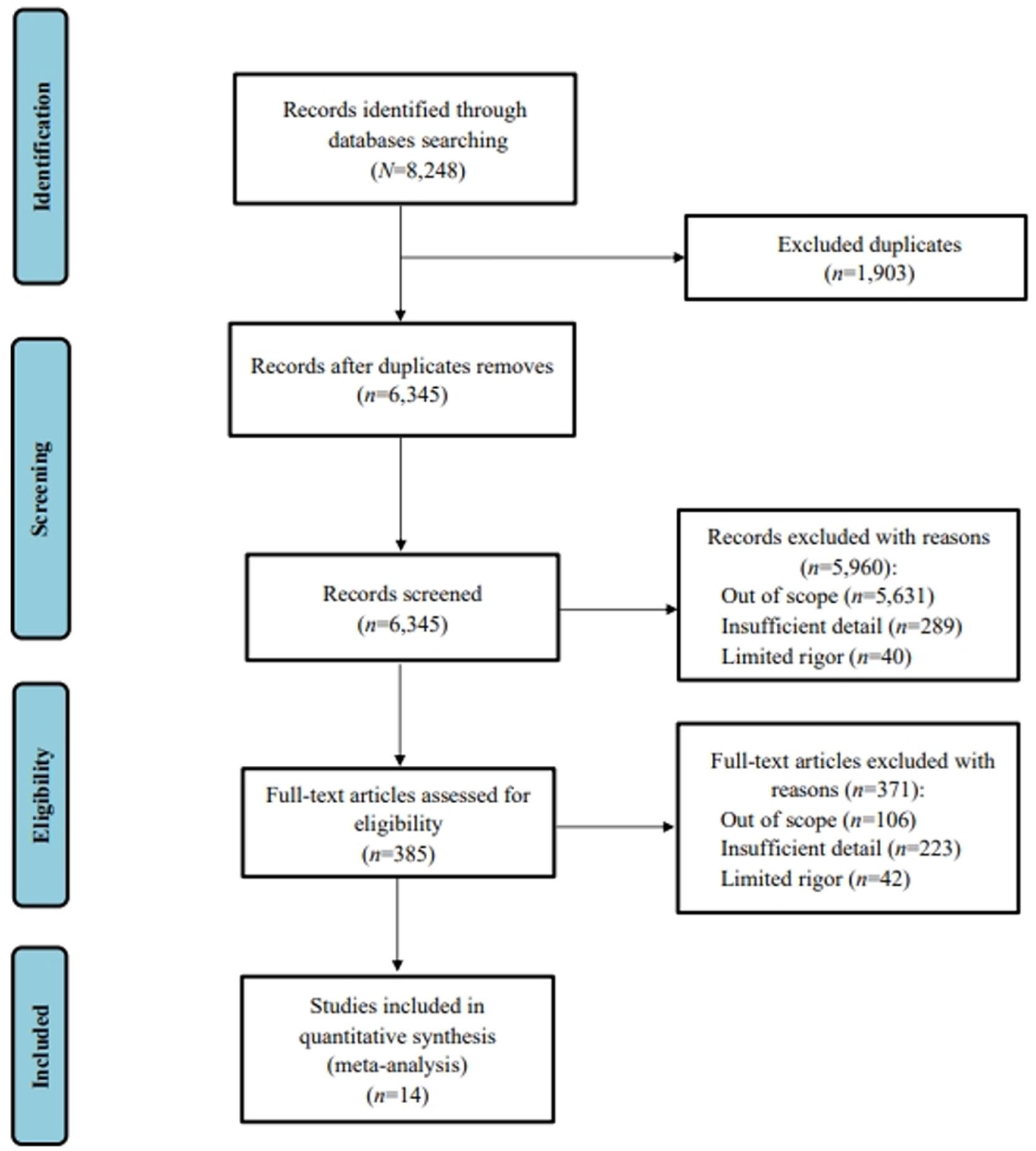
Preferred reporting items for systematic reviews and meta-analyses flow diagram of search results and included studies.
Study Characteristics
Table 1 describes the characteristics of the included 19 RCTs. These studies were conducted in 9 countries, including the United States (n = 8), the United Kingdom (n = 3), Australia (n = 2), China (n = 1), Denmark (n = 1), Italy (n = 1), Portugal (n = 1), Singapore (n = 1), and Sweden (n = 1).
Study Characteristics.
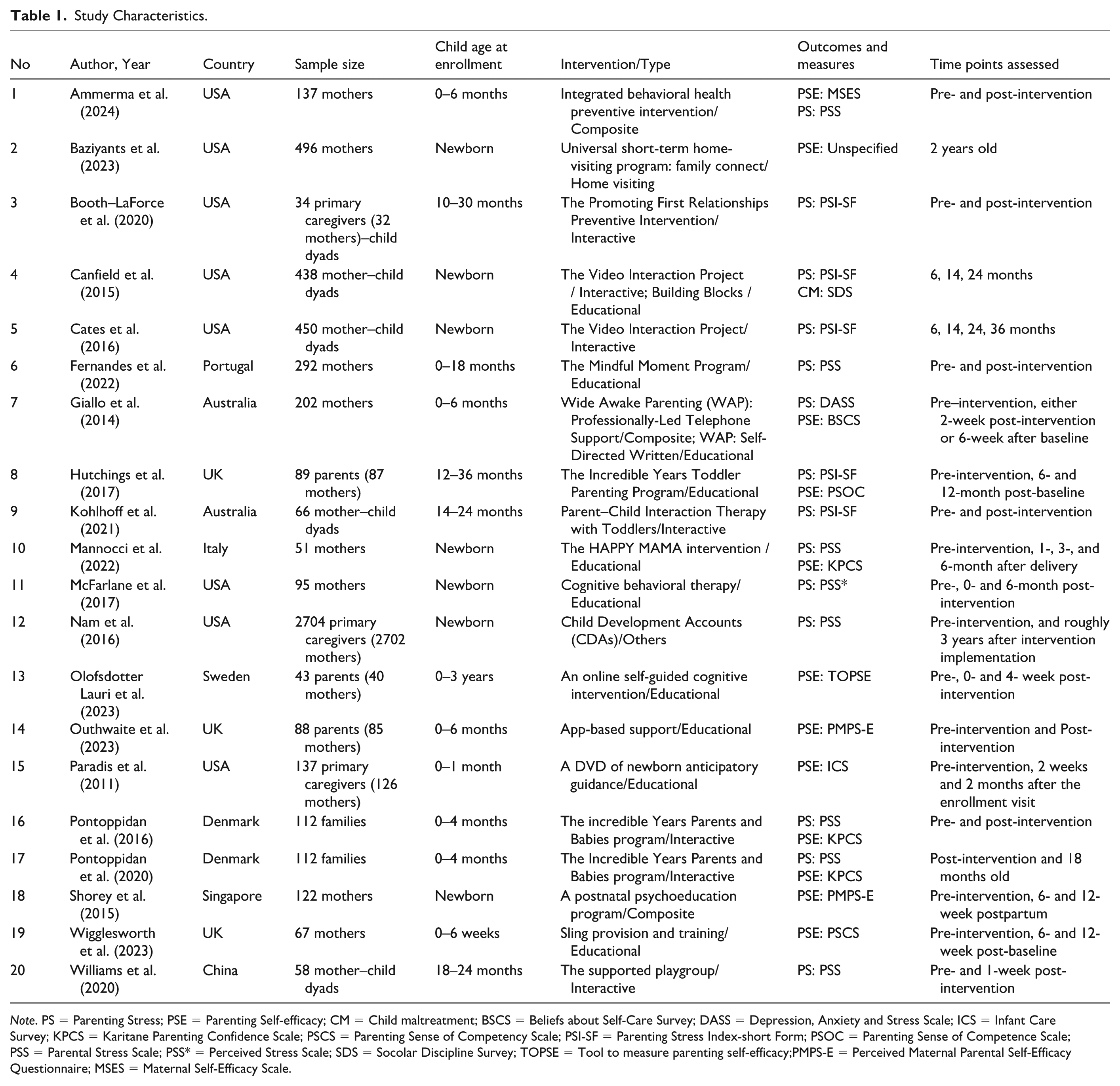
Note. PS = Parenting Stress; PSE = Parenting Self-efficacy; CM = Child maltreatment; BSCS = Beliefs about Self-Care Survey; DASS = Depression, Anxiety and Stress Scale; ICS = Infant Care Survey; KPCS = Karitane Parenting Confidence Scale; PSCS = Parenting Sense of Competency Scale; PSI-SF = Parenting Stress Index-short Form; PSOC = Parenting Sense of Competence Scale; PSS = Parental Stress Scale; PSS* = Perceived Stress Scale; SDS = Socolar Discipline Survey; TOPSE = Tool to measure parenting self-efficacy;PMPS-E = Perceived Maternal Parental Self-Efficacy Questionnaire; MSES = Maternal Self-Efficacy Scale.
The sample sizes ranged from 34 to 2,704 parents. All studies only or predominantly recruited mothers. Among them, three studies additionally invited mothers’ partners or significant others to participate (Pontoppidan et al., 2016, 2020; Shorey et al., 2015; Wigglesworth et al., 2023). Most of the children were newborn at enrollment. In terms of types of intervention strategies, 10 studies were educational, 6 studies were classified as interactive, one study was home visiting by nurses and community staff, 3 studies were composite with home visiting and educational strategies, and one study used Child Development Account intervention and was classified as others.
Risk of Bias Assessment
All articles mentioned randomization in the methods section, but seven articles did not describe the specific methods of randomization. Fifteen studies were deemed to have a high risk of performance bias because they did not clearly describe whether participants and personnel were blinded. See Figure 2.
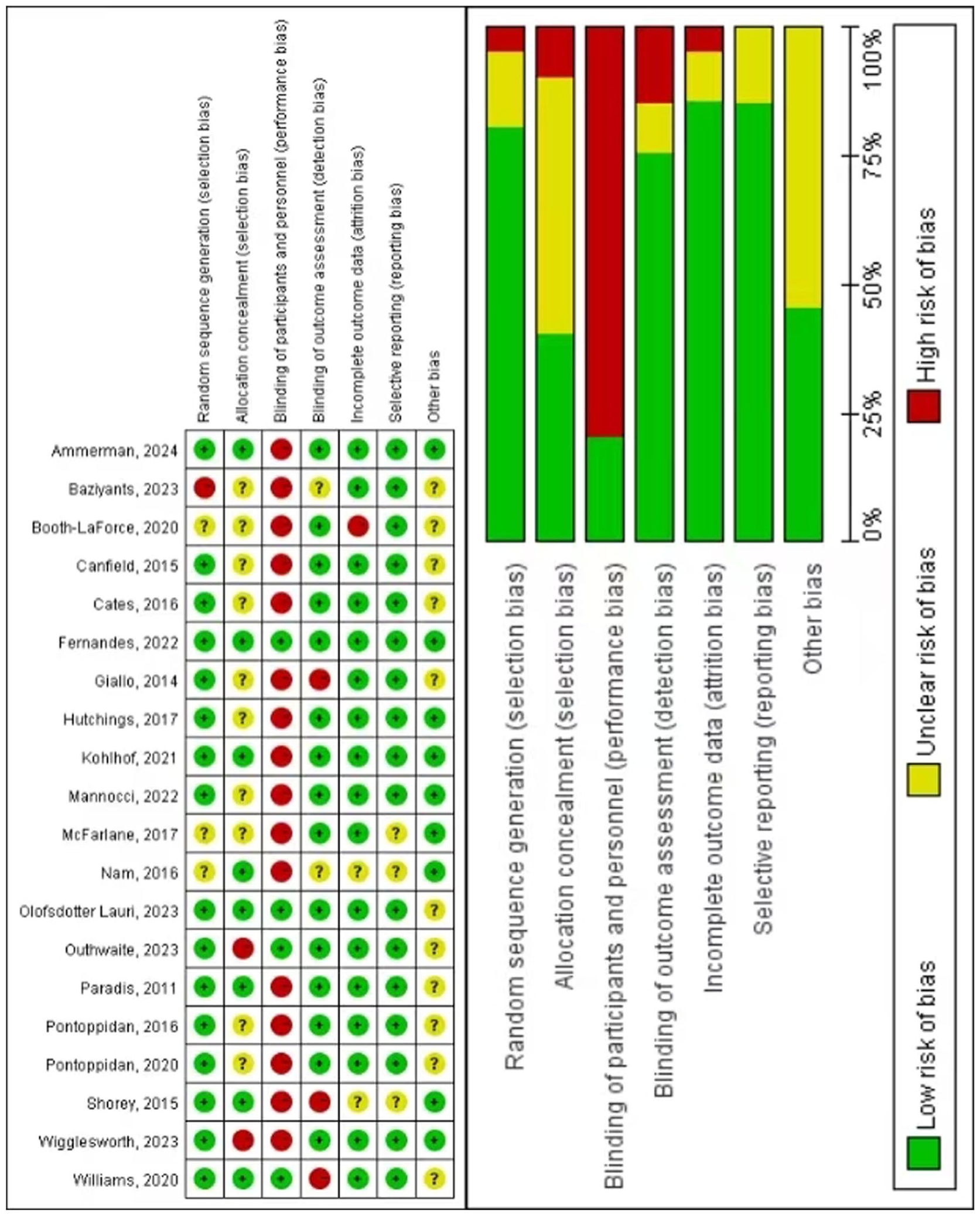
Risk of bias graph & risk of bias summary.
Intervention Effects on Parenting Stress
Description of Study Characteristics and Findings Synthesis
A total of 13 studies examined the effectiveness of parenting interventions on parenting stress. Of these studies, the Parenting Stress Index Short Form (PSI-SF) and the Parental Stress Scale (PSS) were the most commonly used measures of parenting stress. Two studies had two intervention groups and one control group (Canfield et al., 2015; Giallo et al., 2014). Among the remaining 11 studies, 5 conducted interactive interventions (Booth-LaForce et al., 2020; Cates et al., 2016; Kohlhoff et al., 2021; Pontoppidan et al., 2016, 2020; Williams et al., 2020), 4 used educational interventions (Fernandes et al., 2022; Hutchings et al., 2017; Mannocci et al., 2022; McFarlane et al., 2017), one applied Child Development Account intervention (Nam et al., 2016), and one carried out composite interventions (Ammerman et al., 2024).
Nine out of 13 studies reported statistically significant small to medium intervention effects on reducing parenting stress, whereas the other 4 studies did not find evidence of significant intervention effects.
Meta-Analysis
A total of nine out of 13 studies were included in the meta-analysis and the estimated pooled effect size SMD was −0.30 (95% CI [−0.45, −0.15], p < .001; Figure 3A), indicating a small benefit from intervention in parenting stress reduction. Sensitivity analysis showed that the magnitude of the changes of the confidence intervals was less than 0.1. See Figure S1A. The funnel plot (Figure 4A) was symmetric.
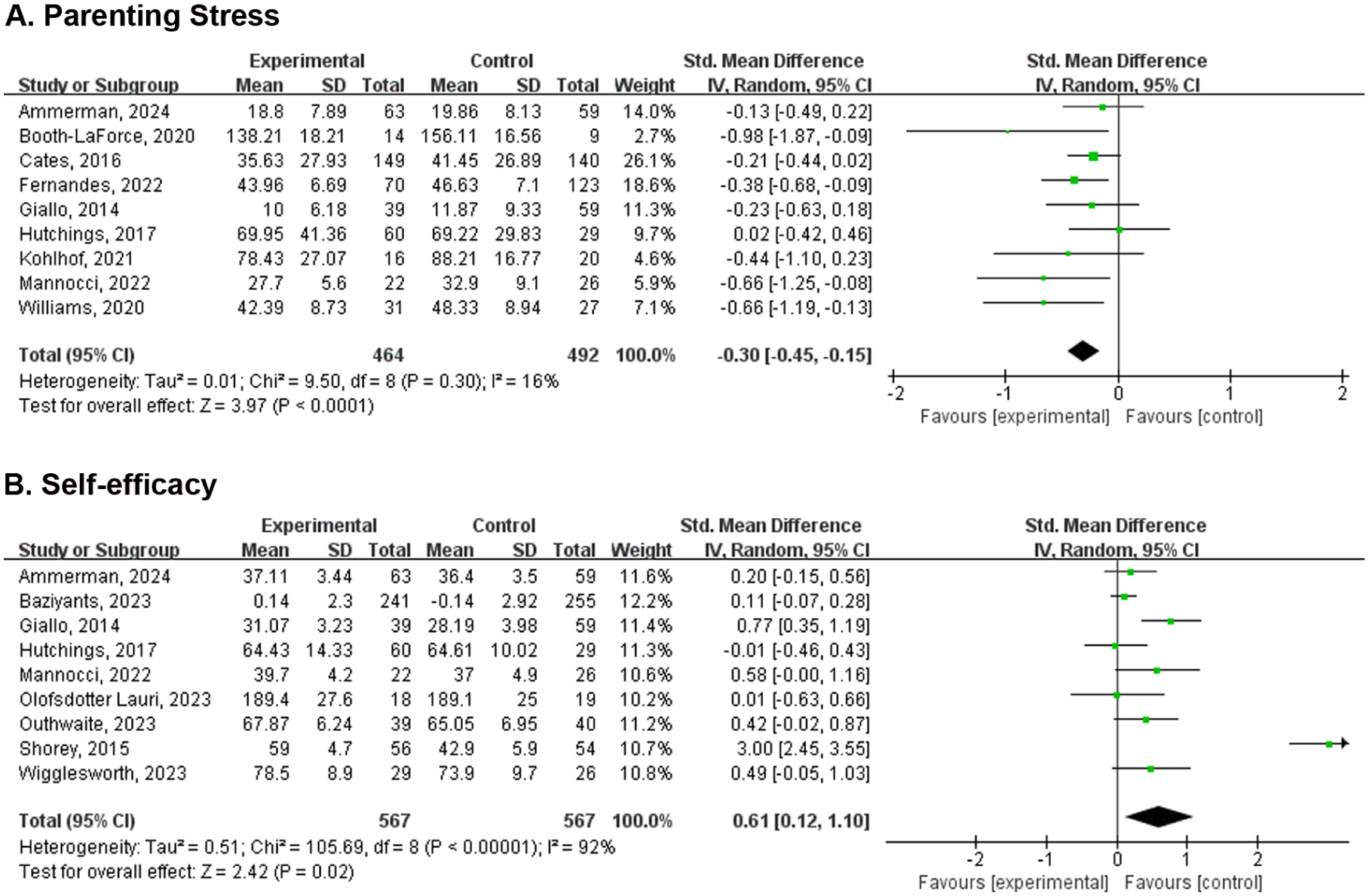
Forest plot for the effect of parenting interventions on parenting stress (A.) and self-efficacy (B.).
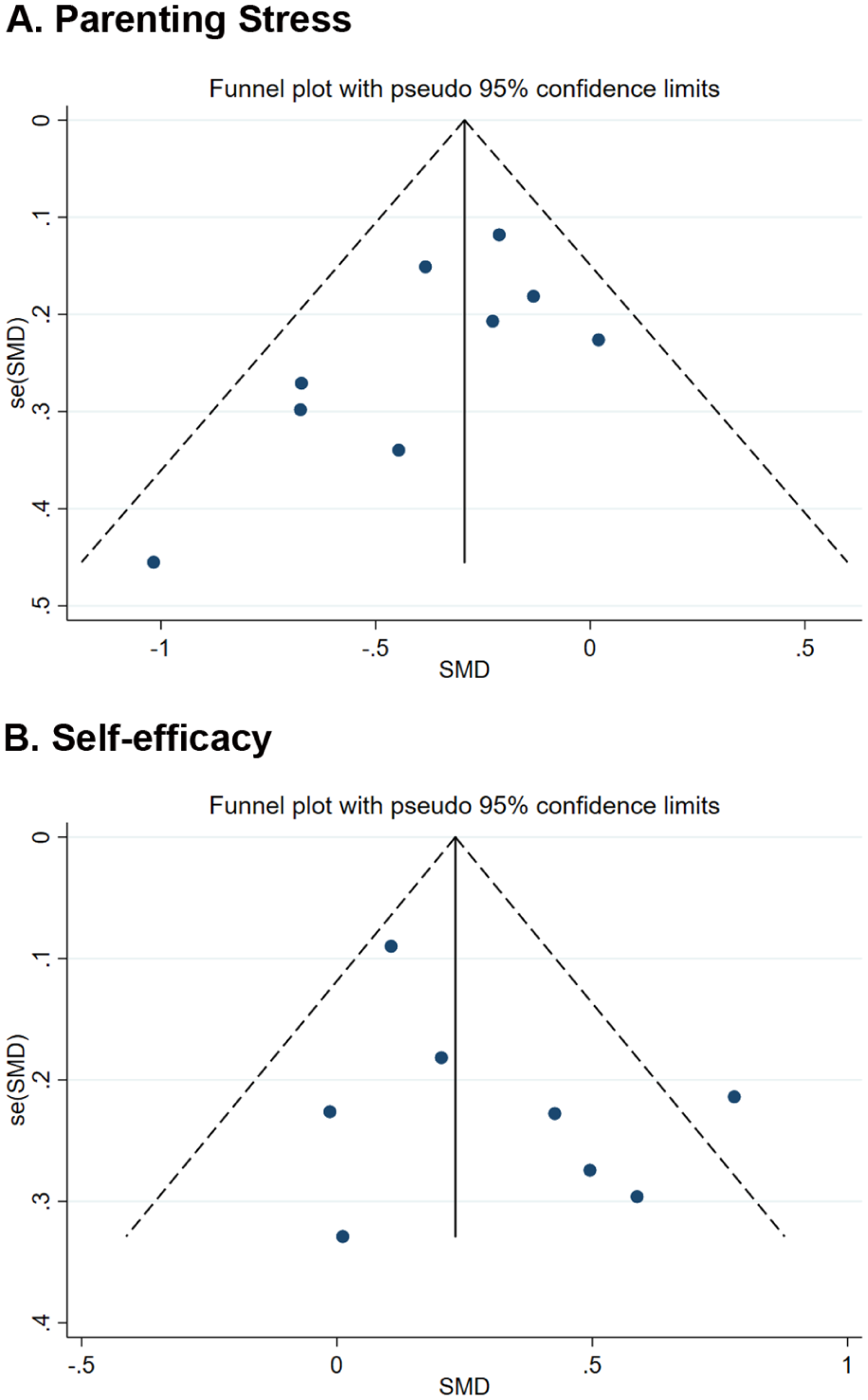
Funnel plot of studies on parenting stress (A.) and self-efficacy (B.).
Inter-study heterogeneity was small (τ2 = .01). Although subgroup analyses showed no significance by pre-specified factors, intervention effect was relatively higher for studies with interactive intervention (SMD = −0.43, 95% CI [−0.75, −0.12], p = .007) than those with educational (SMD = −0.32 [−0.65, 0.02], p = .06) and composite interventions (SMD = -0.17 [-0.44, 0.10], p=0.21; Figure S2A), and higher for those with intervention lasting 1 to 3 months (SMD = −0.32 [−0.51, −0.12], p = .002) than those over 3 months (SMD = -0.25 [−0.52, 0.02], p = .07; Figure S2B), and lower for those with the first post-intervention measurement carried out immediately upon completion (SMD = −0.28 [−0.44, -0.12], p < .001) than others (SMD = −0.36 [−0.67, −0.05], p = .02; Figure S2C).
Intervention Effects on Parenting Self-efficacy
Study Characteristics and Finding Synthesis
Eleven studies reported intervention effects on parenting self-efficacy. These studies were conducted in seven different countries, including the United Kingdom (n = 3), the United States (n = 3), Australia (n = 1), Denmark (n = 1), Italy (n = 1), Singapore (n = 1), and Sweden (n = 1). In terms of intervention type, 7 of them carried out educational interventions (Giallo et al., 2014; Hutchings et al., 2017; Mannocci et al., 2022; Olofsdotter Lauri et al., 2023; Outhwaite, 2023; Paradis et al., 2011; Wigglesworth et al., 2023), one study carried out interactive interventions (Pontoppidan et al., 2016, 2020), 3 studies applied composite interventions (Ammerman et al., 2024; Giallo et al., 2014; Shorey et al., 2015), and one study applied home-visiting intervention (Baziyants et al., 2023). The Parenting Sense of Competence Scale (PSOC) and the Karitane Parenting Confidence Scale (KPCS) were the two most frequent measurement tools of assessing parenting self-efficacy.
Nine out of 11 studies reported that the interventions were effective in improving parenting self-efficacy, while the other 2 did not find significant intervention effects.
Meta-analysis
Nine out of 11 studies were included in the meta-analysis and the pooled effect was significant in favor of the intervention groups (SMD = 0.61, 95% CI [0.12, 1.10], p = .02; Figure 3B). Sensitivity analysis identified that the study by Shorey et al. (2015) was influential, as its exclusion decreased the pooled effect size to 0.30 [0.10, 0.49]. See Figure S1B. The funnel plot was symmetric after excluding this influential study (Figure 4B).
The study heterogeneity was moderate (τ2 = .51). Although the results of subgroup analyses were not significant, the intervention effect was higher in studies where the first post-intervention measurement was carried out immediately after intervention (SMD = 0.78, 95% CI [−0.04, 1.61], p = .06) than others (SMD = 0.27 [-0.15, 0.69], p = .20; Figure S3C).
Child Maltreatment
We only identified one study concerning child maltreatment. Canfield et al. (2015) randomized 438 mothers into three groups (Video Interaction Project [VIP] group, Building Blocks [BB] group, and a standard pediatric care group). They measured physical punishment using the Socolar Discipline Survey when their children were 14 and 24 months, which was 8 to 18 months after intervention. When the children were 14 months old, fewer parents (61.7%) in the VIP group reported using any physical punishment in the previous 3 months, compared to the control (70.0%) and the BB (69.2%) groups. Such a difference was enlarged when the children were 24 months old.
Discussion
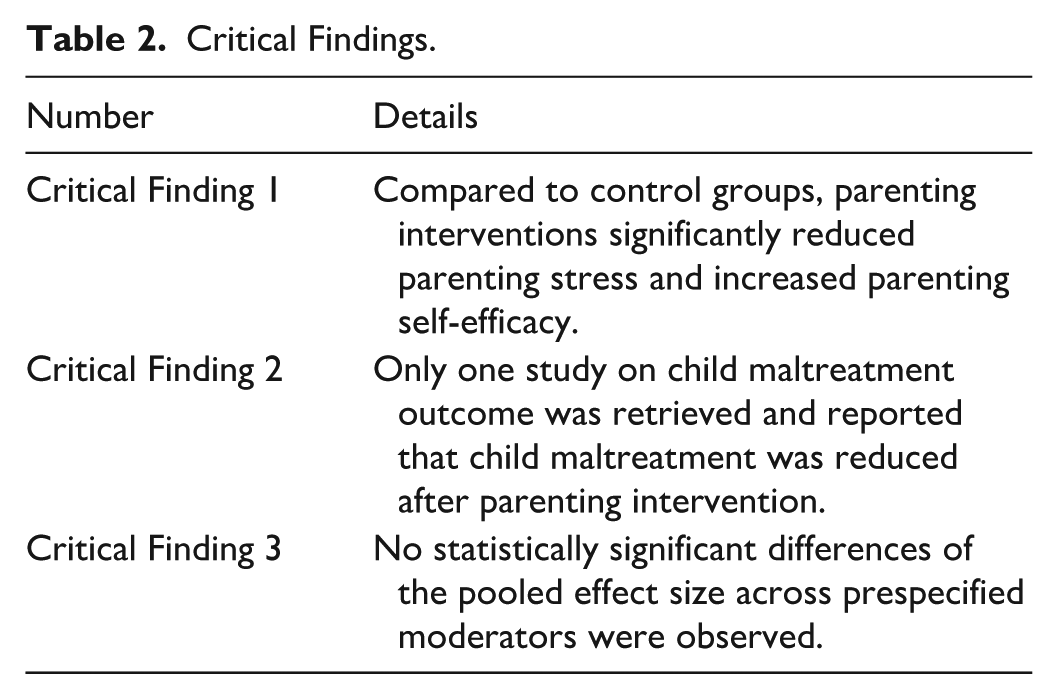
In this systematic review of 19 published RCTs of interventions delivered during the first 3 years of life to improve parenting outcomes among families without special conditions, we found evidence that parenting interventions moderately reduced parenting stress and improved parenting self-efficacy. However, the effects of parenting interventions on child maltreatment were inconclusive because only one study was identified (Table 2). The effect sizes were relatively higher for interactive interventions, interventions lasting 1 to 3 months, and when outcomes measured after a period of intervention completion.
Critical Findings.
Parenting Stress
We found a significant pooled effect size with a small magnitude of parenting interventions on reducing parenting stress. This finding is consistent with existing systematic reviews in the broad field of parenting practice. For instance, a systematic review evaluating the effectiveness of mindfulness interventions among parents of youths reported a small magnitude of post-intervention reduction in parenting stress, which grew to a moderate reduction at two-month follow-up (Burgdorf et al., 2019). Similarly, another systematic review (Bourke-Taylor et al., 2021) reported significant reduction of parenting stress after cognitive-behavioral interventions among mothers of children with disabilities. Furthermore, Ling et al. (2021) conducted a meta-analysis and found that stress management interventions yielded a small reduction in stress among socioeconomically disadvantaged parents.
The intervention strategies applied in the included studies were classified into five categories: educational, interactive, home visiting, composite, and others. The educational interventions involved coaching parents about child care, child development, and self-care such as mangaing fatigue, enhancing problem-solving skills and promoting mental health through ways such as paper materials, face-to-face sessions, or telephone consulting by health care providers. The interactive interventions had characteristics of parent-child participation, which demanded parents actively interact with children through activities, such as playing games. Interactive interventions also refer to those in which parent-child interaction was videotaped and professionals reviewed the tapes and provided feedback. Three studies adopted composite interventions including home-visiting and education. Although subgroup analyses showed that interactive interventions might produce a relatively higher effect size than educational interventions, this difference was not statistically significant. The similar effectiveness of the different intervention strategies indicates that regardless of focus and delivery mode, parenting interventions are effective in reducing parenting stress for families without special conditions, at least for mothers, as they were the primary informant.
Subgroup analysis also suggested that interventions lasting 1 to 3 months produced greater reductions in parenting stress compared to those lasting over 3 months. This is possible because long interventions can be burdensome and lead to decrease in parental engagement. For example, Fernandes et al. (2022) noted that postnatal mothers’ time constraints (balancing newborn care, family, and work) and issues related to program design and attractiveness reduced adherence. Robinson et al. (2022) reported that sending multiple weekly text messages to parents as an intervention strategy reduced their engagement in beneficial parenting behaviors (e.g., limiting screen time, encouraging sleep, checking homework). Similarly, the sustained pressure of the long-term intervention was identified as a core reason for dropout and low adherence in a family-based cognitive-behavioral intervention program for adolescent overweight and obesity (L. Brennan et al., 2012). In addition, we observed that the effect sizes were lower when post-intervention measure was carried out immediately after intervention completion for both parenting stress and self-efficacy than that of the measurement not carried immediately after the intervention. This may be because these interventions have yielded delayed effect, that is parenting self-efficacy increased when parents were given time to practice the skills they learned from the interventions, which was also observed in other studies (Cirlak & Kilicarslan, 2024; Zheng & Gao, 2023).
Parenting Self-Efficacy
Nine included studies reported that the interventions were effective on improving parenting self-efficacy, two studies did not find such significant effect, and the pooled effect size was statistically significant. This is consistent with the finding from two existing systematic reviews of studies among families with special conditions. A review of 25 RCTs among parents of children under 10 with neurodevelopmental disabilities reported that parent training programs significantly improved parenting self-efficacy (Hohlfeld et al., 2018). Similarly, a systematic review and meta-analysis examining the effectiveness of Stepping Stones Triple P (SSTP) in parents of children with disabilities showed a significant improvement in parenting self-efficacy (Ruane & Carr, 2019). Notably, the effect size dropped from 0.61 (95% CI [0.12, 1.10]) to 0.30 [0.10, 0.49] after removing an influential study by Shorey et al. (2015), and the confidence interval became more precise.
Child Maltreatment
We only found one study that measured child maltreatment as the outcome, which showed that the interactive intervention reduced the occurrence of child maltreatment compared to regular pediatric care. It is surprising that there are such a small number of parenting interventions on the prevention of child maltreatment during the first 3 years, especially given the high rate of abuse and neglect in infancy and toddler-hood (Putnam-Hornstein et al., 2022), and the fact that many preventive and curative interventions have been conducted and showed effectiveness to mitigate occurrence/recurrence of child maltreatment and potential for child maltreatment among parents of children and adolescents (Branco et al., 2022; Mattheß et al., 2021). Prior to this review, we were aware of some successful child maltreatment-targeted programs, such as the Positive Parenting Program (Triple-P) and Incredible Years. However, none of these programs’ studies on child maltreatment were included. It may be because intervention studies concerning child maltreatment were usually conducted among at-risk families that were excluded from this study. For example, we excluded studies of Baby Triple P because this program targeted on parents with preterm children. It is also possible that we strictly restricted the age range of the targeted children to be under 3 years. This resulted in the exclusion of studies involving parents of children across a wider age range. For example, studies of PCIT and Play Nicely interventions, two well-known parenting programs, were excluded (Abrahamse et al., 2021; Richardson & Damashek, 2022; Thomas & Zimmer-Gembeck, 2012) because these programs targeted children aged 2 to 7 years or 1 to 5 years.
Study Strengths and Limitations
This review rigorously evaluated the effects of multiple parenting interventions on three parenting outcomes by including only RCT studies. Then we confirmed the effectiveness through quantitative analysis. Findings could fill gaps in existing reviews on parenting interventions for families with very young children and without special conditions.
Meanwhile, limitations should be noted. First, limiting the inclusion to studies published in English may have excluded some studies of interest. Second, there was considerable unexplained heterogeneity in the pooled effects with respect to parenting self-efficacy. Future research can explore other moderators that may explain the study heterogeneity in treatment effects. Third, the number of included studies on child maltreatment was limited, which made it impossible to derive meaningful pooled estimates. We did not include search terms related to harsh parenting and corporal punishment, and strictly excluded studies in which children’s age out of 0-to-3-year range. This may have resulted in omission of studies on child maltreatment and excluded studies from successful parenting programs, such as PCIT and Play Nicely. Fourth, we only focused on three of the most common parenting outcomes, and did not include other important outcomes, such as mental health and quality of life of parents and child development outcomes. Finally, in this study, all the included studies relied on self-reported data and mothers were the primary informants, and therefore, results are subject to report bias and may not be generalized to fathers.
Implications for Future Practice and Research
This systematic review highlights the critical role of parenting interventions in reducing parenting stress, improving parenting self-efficacy, and potentially mitigating child maltreatment among families without special conditions during the first 3 years of parenthood. These findings highlight the public health importance of making evidence-based parenting programs universally accessible—not only for families with specific challenges but for all families. Incorporating universal parenting interventions in existing public health infrastructures, such as maternal and child health services can serve as a preventive measure to reduce parenting stress and enhance parenting self-efficacy. This has the potential to further improve parental mental health, promote parent-child interactions, and foster positive child development (Fang et al., 2024; Williams et al., 2020). Interactive formats of interventions with reasonable periods may be favored although educational intervention, home visiting and composite formats can also be beneficial.
It should be noted that although six studies were conducted in low-income families, the majority of the included studies were conducted in developed or upper-middle-income countries. Future studies can make more efforts to evaluate the effectiveness of parenting interventions in low-income countries where parents may face more parenting challenges. Furthermore, more studies focused on reducing child maltreatment in the first 3 years after birth are needed. Finally, future research should further investigate long-term effects and optimal intervention designs to strengthen these findings and guide the development of scalable, cost-effective parenting support initiatives.
Diversity
The discussion of diversity in the reviewed studies reflects a meaningful effort to include a range of contexts and populations, contributing to a broader understanding of parenting interventions. The 19 studies included were conducted across 9 countries in Asia, Europe, Oceania, and North America, providing diverse geographical representation. This variety in settings allows for insights into how parenting interventions might function across different cultural and national contexts, even if the majority of studies were conducted in developed or upper-middle-income countries. Additionally, some studies specifically targeted low-income families, offering valuable perspectives on how socioeconomic factors may influence parenting outcomes. While most studies focused on mothers, the inclusion of several studies that involved both fathers and mothers is a positive step toward recognizing the role of diverse caregivers in parenting. The use of various intervention types, such as educational, interactive, and home visiting, also reflects an awareness of the need for adaptable strategies that can be tailored to different family needs and contexts. We recognize the limitation of the existing study that research from low- and middle-income countries is scarce, as is research focusing specifically on child maltreatment in the first 3 years of life. More studies are needed to further enhance the relevance and generalizability of these interventions. The current findings demonstrate the potential for parenting programs to benefit families without special conditions, and future research can continue to expand this understanding by exploring how these interventions can be adapted to form universal parenting programs.
Conclusions
This systematic review and meta-analysis examined the effectiveness of parenting interventions on three important parenting outcomes, namely parenting stress, parenting self-efficacy and child maltreatment among parents of families without special conditions during the first 3 years after child birth. Based on the synthesis and meta-analysis of the results of the published RCTs, parenting interventions were found to be effective in reducing self-reported parenting stress and improving parenting self-efficacy. These findings highlight the important role of parenting programs in promoting positive parental adaptation during the early and often challenging stages of parenthood. However, due to the limited number of included studies, no conclusive findings could be drawn regarding the effect of parenting interventions on child maltreatment in the targeted population. Future studies are recommended to expand the child age range and search terms to facilitate a more comprehensive investigation.
Supplemental Material
sj-docx-1-tva-10.1177_15248380261451785 – Supplemental material for Effectiveness of Interventions on Parenting Outcomes in Families With Children Under 3 Years of Age: A Systematic Review and Meta-Analysis of Published Randomized Controlled Trials
Supplemental material, sj-docx-1-tva-10.1177_15248380261451785 for Effectiveness of Interventions on Parenting Outcomes in Families With Children Under 3 Years of Age: A Systematic Review and Meta-Analysis of Published Randomized Controlled Trials by Xiaoyan Liu, Yinjun Hao, Yujing Zhang, Xunqi Zhang, Wenjie Zhang and Naixue Cui in Trauma, Violence, & Abuse
Footnotes
Ethical Considerations
This is a systematic review of published studies. Ethical approval is not required.
Consent to Participate
This is a systematic review of published studies without the involvement of individual participants. Informed consent is not required.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Social Science Fund of China (18CSH061 [to N.C.]) and the National Natural Science Foundation of China (32100877 to [N.C.]).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data are from published studies and are available from these studies.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.