
Abstract
Domestic and family violence (DFV) is a profound health concern, placing women at a disproportionate risk of injury or death. Research shows that women who experience DFV have higher rates of physical illness than women who do not, resulting in more frequent contact with healthcare providers, which creates an opportunity for intervention. Video-based interventions may provide a beneficial, accessible, and cost-effective method to increase awareness and help-seeking behaviours in women who may be experiencing DFV. This review evaluated the effectiveness of video interventions targeted at women within healthcare settings and assessed the characteristics of these videos to inform future developments. We conducted a systematic review of key databases (MEDLINE, Embase, CINAHL, PsycINFO, Scopus, Web of Science). Twelve articles describing seven trials underwent quality appraisal (QuADS) and were included in the review. Interventions were either standalone videos or embedded within DFV screening processes. Findings suggest that video interventions have the potential to improve help-seeking behaviours related to DFV; however, no effect was observed on quantitative measures of knowledge or quality of life. Although findings were mixed, feedback from women and healthcare staff was favourable. Video interventions appeared to be most effective when shown in private settings prior to appointments with healthcare providers, when videos could prompt further discussion with healthcare staff. Further research is recommended to identify the optimal format of delivery that aligns with women’s needs for discretion and safety.
Keywords
Introduction
Domestic and family violence (DFV) is a significant public health concern disproportionately impacting women, resulting in an estimated 51,500 deaths globally in 2023 alone (United Nations Office on Drugs and Crime, 2024; World Health Organisation, 2021). DFV is a leading cause of death and hospitalisation in women worldwide, and the primary cause of hospitalisation in women aged between 15 and 54 in Australia (Emergency Medicine Foundation, 2020). Women who experience DFV face a heightened risk of chronic health problems, an increased need for healthcare services, and are up to four times more likely to present to emergency departments (Baird et al., 2019; Kothari et al., 2015; Stubbs & Szoeke, 2022). Healthcare facilities are therefore ideal and opportune environments for women to disclose DFV and receive referrals to appropriate care (Evans & Feder, 2016).
Routine enquiry to enhance the identification and support of women experiencing DFV has been embedded within many healthcare facilities. However, many clinicians report being unsure of how to support or refer women appropriately (Fisher et al., 2020; Gillespie et al., 2023). Previous studies have identified several reasons for this, including a lack of skills, confidence, training, or time (Gillespie et al., 2023). Furthermore, women may choose not to disclose DFV due to feelings of guilt, shame, denial, fear of repercussions from the perpetrator, or fear of having children removed (Evans & Feder, 2016; Prosman et al., 2014). Despite the continued implementation of DFV screening policies, significant barriers continue to limit the identification, management, and referral of women experiencing DFV.
A potential strategy to improve DFV screening and disclosure is the implementation of video interventions. Video interventions are cost-effective, less resource-intensive, and easily administered across a range of settings and regions (Tuong et al., 2014). They also allow for engagement with individuals from culturally and linguistically diverse (CALD) backgrounds (Love et al., 2009). Videos may overcome potential discomfort between patients and healthcare providers by providing resources and information, while also enabling a dialogue between both parties (Humphreys et al., 2011). Videos can also utilise personal testimonials, which can be more persuasive in improving health behaviours, such as DFV help-seeking, rather than simply presenting data or information (Hinyard & Kreuter, 2007).
Past research has demonstrated improved health-related behaviours after video interventions, for example, in the promotion of breast self-examination, prostate cancer screening, sunscreen adherence, HIV testing, and treatment compliance (Tuong et al., 2014). An intimate partner violence (IPV) intervention incorporating video education effectively reduced IPV among married couples up to 1 year post-intervention (Braithwaite & Fincham, 2014). Another online module for survivors of interpersonal trauma that incorporated video elements showed significant improvements in post-traumatic stress disorder, depression, and anxiety (Fiorillo et al., 2017). To date, no systematic review of the literature has been conducted to examine video interventions explicitly designed for women experiencing, or at risk of experiencing, DFV.
This systematic review aims to identify and synthesise the evidence relating to the use of video interventions for women who may be experiencing DFV delivered in healthcare settings. The primary outcomes of interest are the characteristics of DFV video interventions, and any improvements in knowledge, awareness, or help-seeking behaviours. The systematic review will also report healthcare provider feedback to offer a more comprehensive understanding of DFV video interventions used in healthcare settings.
Research Questions
What literature exists on the creation, delivery, and evaluation of video interventions for women who may be experiencing DFV?
What are the characteristics of these interventions?
How do these studies evaluate the benefits or acceptability of these interventions?
What are the outcomes for women who have been exposed to video interventions?
What are the opinions and suggestions of healthcare providers regarding DFV video interventions for women who may be experiencing DFV?
Methods
Acknowledgement of Gender Diversity
The authors of this review recognise the pervasiveness of DFV and the severe danger applicable to many gender identities and expressions. This review focused specifically on DFV video interventions designed for women. The authors acknowledge that there are many expressions and identities of women and maintain that the use of gendered language in this review reflects that used in the original sources.
Study Design
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (Page et al., 2021). The study was registered on the PROSPERO international prospective register of systematic reviews (registration number CRD42023475338). A protocol paper for the review has also been published (Gillespie et al., 2024).
Eligibility Criteria
Peer-reviewed publications that included quantitative and qualitative primary data were included in the review. All study designs have been included (such as randomised controlled trials (RCTs), quasi-experimental trials, cross-sectional, case-control, interviews, and focus groups). There were no restrictions on time or location; however, only studies available in English were included. Two or more papers reporting on a single trial may have been included in the review when these articles presented distinct outcomes relevant to different aims of the research. Table 1 provides an overview of the eligibility criteria.
PICO Statement.
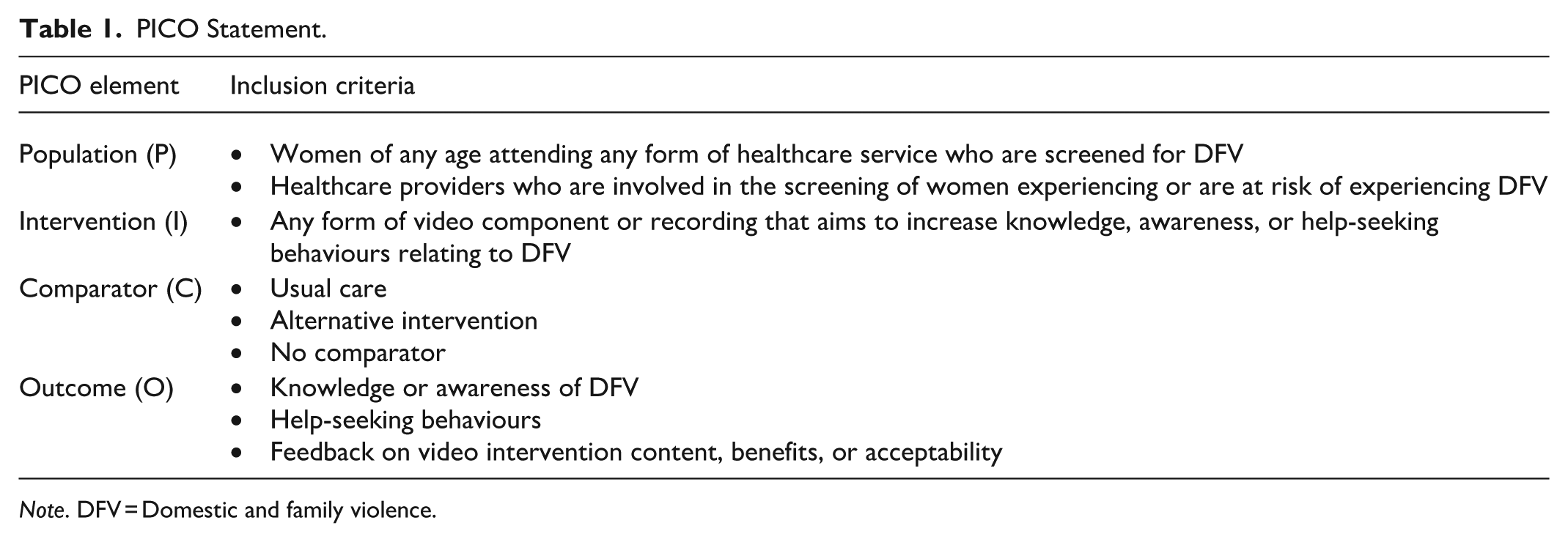
Note. DFV = Domestic and family violence.
Search Strategy
After running preliminary searches to identify an optimal search strategy, a systematic search of the literature was conducted in November 2023 using the online databases MEDLINE (Ovid), Embase (Elsevier), CINAHL (EBSCO), PsycINFO (EBSCO), Scopus (Elsevier), and Web of Science (Clarivate). Databases were systematically searched using the search string: [(videotape OR recording OR video* OR “video recording”) AND (“domestic violence” OR “intimate partner violence” OR “family violence” OR DFV)]. Medical Search Terms (MeSH) and Emtree terms associated with videotape and videorecording were also included. Hand searches were performed to identify articles that may have been missed in online database searches. Citation chaining was conducted on key articles identified in the database search, and articles found on Google Scholar and in the following academic journals: Journal of Interpersonal Violence, Violence Against Women, and Trauma, Violence and Abuse. Updated searches were completed in April 2025 to incorporate any recent publications.
Study Selection
Identified articles were imported into Covidence, a web-based systematic review management platform that supports study screening and data extraction (Veritas Health Innovation, 2025). Due to the high number of articles identified, abstract and title screening was conducted by four independent reviewers, with one reviewer screening all papers to maintain consistency. Conflicts were resolved by a fifth reviewer. Full text screening was conducted by two independent reviewers. Conflicts were resolved by a third reviewer or by consultation with all reviewers, if required.
Risk of Bias Assessment
Due to the inclusion of qualitative, quantitative, and mixed-methods studies, the Quality Assessment with Diverse Studies (QuADS) checklist was used to assess for bias in included papers (Harrison et al., 2021). The QuADS was chosen due to its versatility in assessing heterogeneous study designs with strong reliability. The QuADS includes 13 criteria covering study elements such as description and presentation, theoretical underpinning, study design and procedures, sampling, analysis, and stakeholder input. Each criterion is scored on a scale of 0 to 3 (no mention, limited, moderate, or explicit detail included). Scores were calculated as the mean of all items. No cut-off criteria or quality thresholds were established as per Harrison et al. (2021), who suggest reporting scores descriptively and comparatively. Weaknesses in specific criteria were considered in the context of the review to inform future research. Quality appraisal was performed independently by two researchers. Discrepancies were mediated by team discussion until a mutual resolution was reached.
Data Extraction and Synthesis
Data extraction of key parameters was performed using a pre-specified spreadsheet and was completed by two independent reviewers. Data synthesis for this review was informed by The Joanna Briggs Institute “aggregate mixed method synthesis guidelines,” which provides a framework for the integration of qualitative and quantitative findings from diverse study methods (Lizarondo et al., 2017). Quantitative findings were transformed into descriptive results that could be categorised for the content analysis, while qualitative findings were aggregated into thematic categories. These quantitative and qualitative findings were then juxtaposed and investigated to produce final conclusions. This approach ensured a simplified method of combining data without distorting the findings of the individual studies (Connellan et al., 2017).
Deviation from the Protocol
The protocol for this systematic review has been published (Gillespie et al., 2024). A minor deviation from this protocol was the addition of a research question. The systematic review included articles that described the opinions and recommendations of healthcare providers who were involved in the implementation or evaluation of video interventions. The current manuscript has therefore added research question five to reflect the broader scope of the search and outcomes that were included.
Results
Selected Studies
Based on the search terms and inclusion criteria, 3,299 articles were identified. Duplicates were removed using the Bond University online Systematic Review Accelerator, leaving 2,480 articles for title and abstract screening. Articles were uploaded to Covidence online systematic review management software for screening. Full text screening was conducted on 24 articles, which excluded further 14 articles. Citation searches identified additional two articles (see Figure 1).
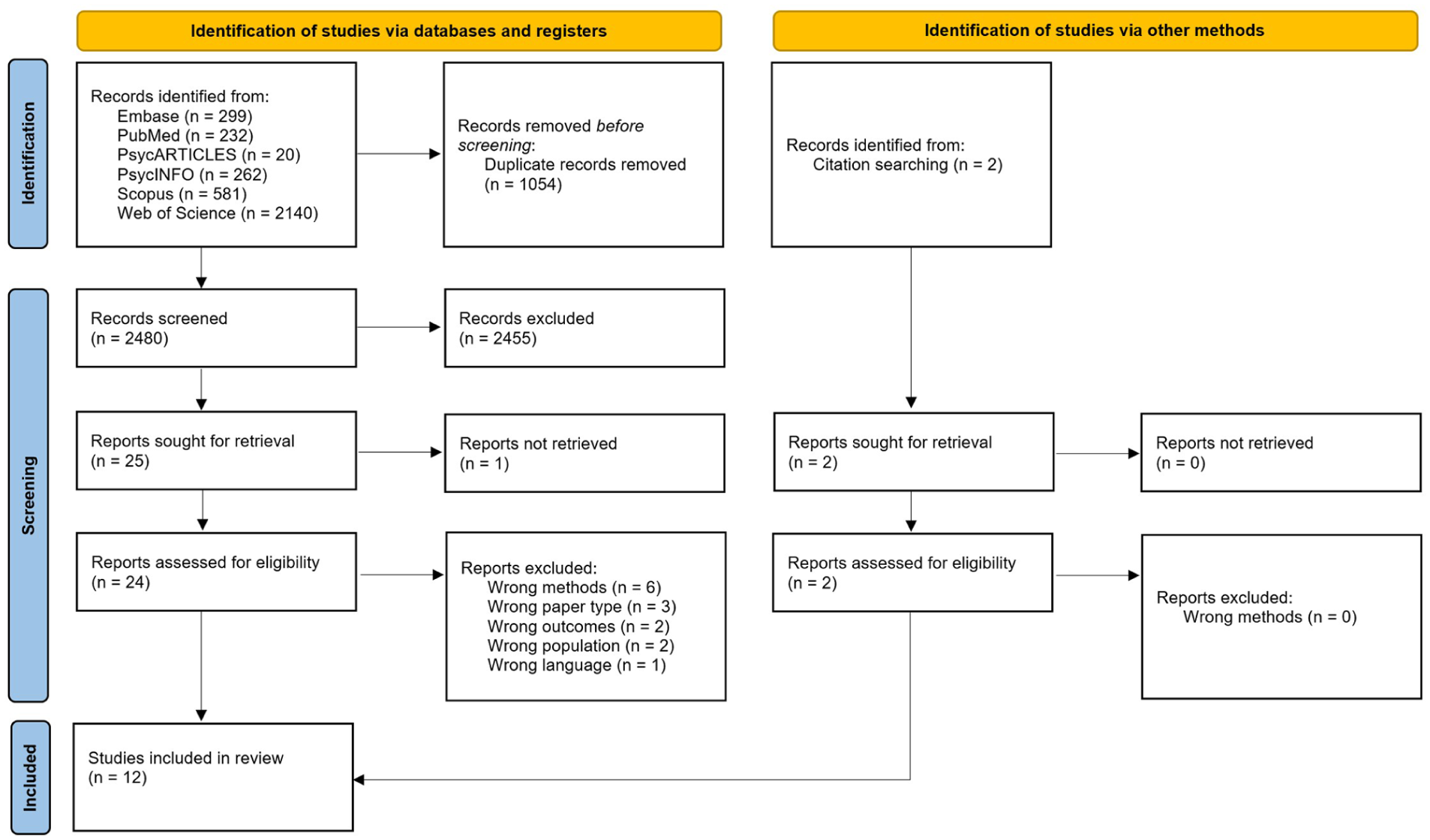
PRISMA flow chart.
Risk of Bias Results
QuADS scores for all studies ranged from 65.4% to 92.3% (See Supplemental Table 1). Five studies scored above 85% (Choo et al., 2016; Ernst et al., 2011; Flaathen et al., 2022; Klevens et al., 2015; Walter et al., 2021). Three of these studies were limited by having minimal stakeholder input in the design process (Ernst et al., 2011; Flaathen et al., 2022; Klevens et al., 2015). Studies with lower ratings tended to lack adequate recruitment methods, analysis transparency, and rationale for data collection tools, and stakeholder input (Klevens et al., 2012a; Tavrow et al., 2021). Furthermore, only three trials reported engaging stakeholders in a co-design process (Choo et al., 2016; Flaathen et al., 2020; Tavrow et al., 2021). Refer to Supplemental Table 1 for QuADS items scores and total ratings.
Participant and Study Characteristics
The review identified 12 studies (quantitative = 6, mixed methods = 2, qualitative = 4) from the USA (n = 8) and Norway (n = 4) (see Table 2 for study characteristics). The included articles described seven separate trials, which evaluated data from 3,178 participants, including 3,037 women, 115 men (Ernst et al., 2011), and 26 healthcare providers or research assistants (Choo et al., 2016; Garnweidner-Holme et al., 2020; Tavrow et al., 2021). One study also included medical record data from 54,887 visits of female clients aged older than 14 years (Tavrow et al., 2021). Studies varied in size, with quantitative studies involving 50 (Humphreys et al., 2001) to 2,364 participants (Klevens et al., 2012a), and qualitative studies involving groups of 9 (Garnweidner-Holme et al., 2020) to 60 (Tavrow et al., 2022). Two studies incorporating mixed methods included surveys and interviews with 25 (Tavrow et al., 2021) and 38 (Choo et al., 2016) individuals. Six studies conducted cross-sectional or immediate pre-post designs (completed on the same day) (Ernst et al., 2011; Flaathen et al., 2021; Garnweidner-Holme et al., 2020; Tavrow et al., 2021, 2022; Walter et al., 2021), while the remaining 6 incorporated longer follow-up surveys and interviews (Choo et al., 2016; Flaathen et al., 2022; Humphreys et al., 2011) of between 6 to 9 days post-intervention (Klevens et al., 2012b) up to 1 year (Klevins et al., 2012a, 2015).
Trial and Intervention Characteristics.
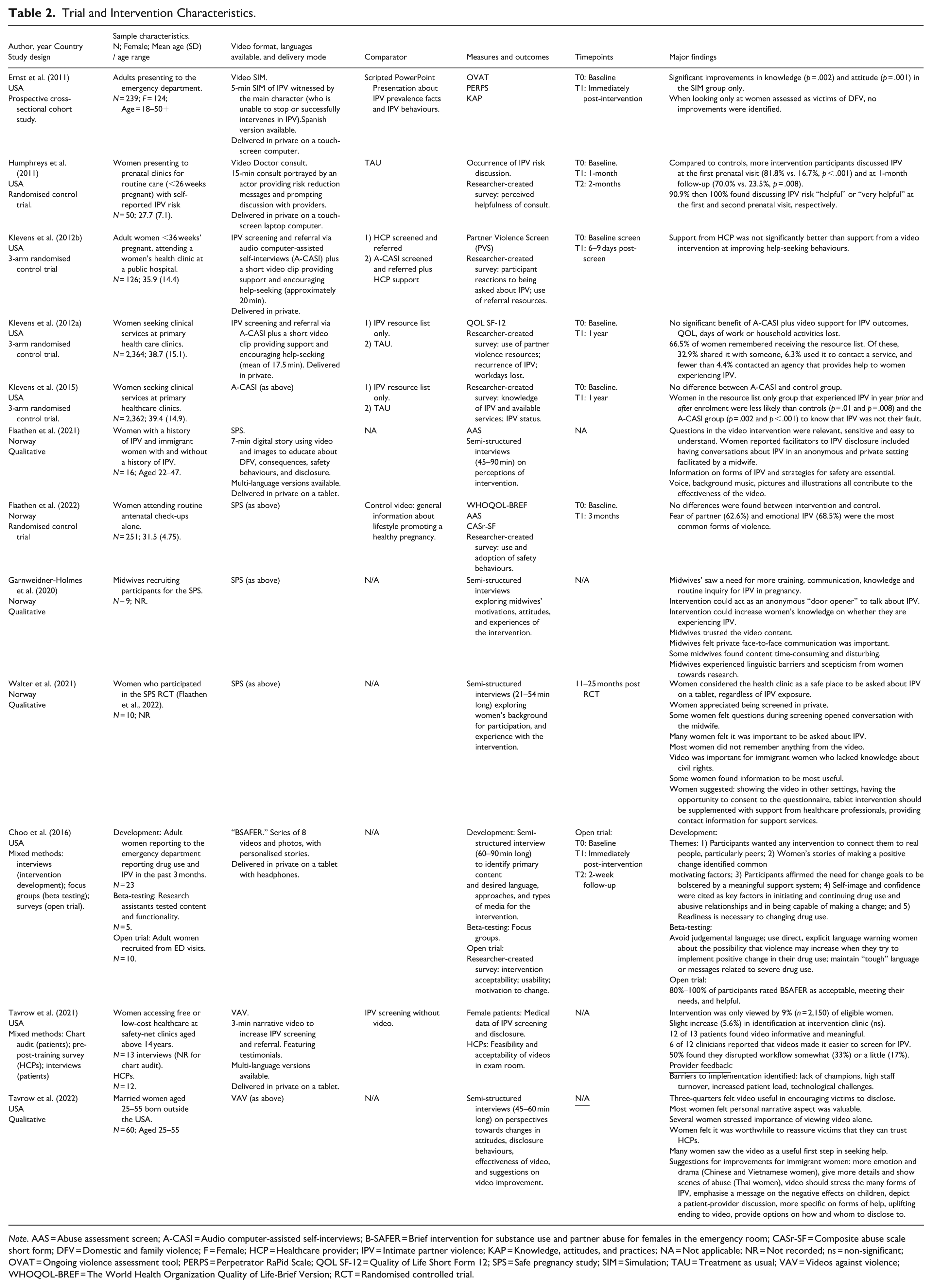
Note. AAS = Abuse assessment screen; A-CASI = Audio computer-assisted self-interviews; B-SAFER = Brief intervention for substance use and partner abuse for females in the emergency room; CASr-SF = Composite abuse scale short form; DFV = Domestic and family violence; F = Female; HCP = Healthcare provider; IPV = Intimate partner violence; KAP = Knowledge, attitudes, and practices; NA = Not applicable; NR = Not recorded; ns = non-significant; OVAT = Ongoing violence assessment tool; PERPS = Perpetrator RaPid Scale; QOL SF-12 = Quality of Life Short Form 12; SPS = Safe pregnancy study; SIM = Simulation; TAU = Treatment as usual; VAV = Videos against violence; WHOQOL-BREF = The World Health Organization Quality of Life-Brief Version; RCT = Randomised controlled trial.
Four articles were part of the Safe Pregnancy Study (SPS) from Norway. The SPS papers included a qualitative user-involvement study to obtain participant feedback on the intervention design to inform the larger trial (Flaathen et al., 2020). Three articles provided the outcomes of different research aims from the same trial of the SPS: an RCT investigating the impacts of the SPS on quality of life (QoL) and DFV outcomes (Flaathen et al., 2022), qualitative interviews to explore participant experiences (Walter et al., 2021) and interviews with midwives to obtain clinician perceptions and feedback (Garnweidner-Holme et al., 2020).
Klevens et al. (2012a, 2015) reported on different outcomes from the same IPV video screening intervention in a 3-arm RCT. Klevens et al. (2012b) used the same intervention with a different sample. Two articles described outcomes of the Videos Against Violence (VAV) project. Tavrow et al. (2021) used a pre-post-intervention survey and chart audit to determine the impacts of VAV on disclosure rates, as well as patient and provider perceptions of feasibility and acceptability. A second study evaluated participant perceptions and feedback of the translated versions of the VAV designed for immigrant Asian women (Tavrow et al., 2022).
Most studies recruited women attending healthcare settings (Ernst et al., 2011; Flaathen et al., 2022; Humphreys et al., 2011; Klevens et al., 2012a, 2012b, 2015; Tavrow et al., 2021, 2022; Walter et al., 2021). Two studies included women recruited from the community, and two included only women who screened positive of, or at risk of, DFV (Choo et al., 2016; Humphreys et al., 2011). Another two studies recruited healthcare providers to give their feedback and discuss barriers to implementation (Garnweidner-Holme et al., 2020; Tavrow et al., 2021). Videos were presented in a range of healthcare settings, such as the emergency department (ED) (Choo et al., 2016; Ernst et al., 2011), antenatal clinics (Flaathen et al., 2020, 2022; Garnweidner-Holme et al., 2020; Humphreys et al., 2011; Walter et al., 2021), primary health clinics (Klevens et al., 2012a, 2015), safety-net clinics (Tavrow et al., 2021, 2022), or public hospitals (Klevens et al., 2012b).
Intervention Characteristics
DFV intervention videos ranged in format but commonly featured narrative (Ernst et al., 2011; Flaathen et al., 2022), testimonial (Choo et al., 2016; Klevens et al., 2012a, 2015; Tavrow et al., 2021), and informational (Flaathen et al., 2022; Humphreys et al., 2011; Klevens et al., 2012a, 2012b, 2015; Tavrow et al., 2021) elements. Narrative elements typically portray a DFV situation followed by advice on appropriate help-seeking behaviours. Other videos utilised DFV survivors and advocates educating on types of DFV, safety planning, and help-seeking behaviours. Interventions were either presented as videos and images focused on education (Ernst et al., 2011; Flaathen et al., 2020, 2022; Garnweidner-Holme et al., 2020; Tavrow et al., 2021, 2022; Walter et al., 2021), or as part of a full screening process involving a video doctor consultation (Humphreys et al., 2011), computer-assisted self-interview (Klevens et al., 2012a, 2012b, 2015), or motivational interviewing (Choo et al., 2016).
Video-only interventions ranged from 3 to 7 min. Screening and interviewing interventions with embedded videos ranged in length from approximately 15 to 30 min. All videos were viewed in private, on tablets or computers. The Video Simulation (Ernst et al., 2011), the VAV project (Tavrow et al., 2021, 2022), and the SPS (Flaathen et al., 2020, 2022; Garnweidner-Holme et al., 2020; Walter et al., 2021) provided adaptations for CALD women. Three trials adapted their DFV video interventions for CALD populations (Ernst et al., 2011; Flaathen et al., 2022; Tavrow et al., 2021). Language variations also had slightly different content to address culturally specific fears, such as deportation, stigma, and trafficking.
Knowledge and Awareness
Two trials reported on women’s changes in DFV knowledge or awareness (Ernst et al., 2011; Klevens et al., 2015). A 3-arm RCT incorporating 2,362 women found no improvements in DFV awareness and knowledge after screening, video viewing, and receiving printed resources, compared to those receiving only a resource list (Klevens et al., 2015). The smaller, but moderately sized simulation study screened a video depicting the perpetration of IPV and a PowerPoint providing statistics relating to IPV (Ernst et al., 2011). This study also found no improvements in knowledge, attitudes, and practices relating to IPV in the intervention group compared to the control group, who received the PowerPoint only. Both studies utilised a bespoke, researcher-designed survey.
Help-Seeking, Safety Behaviours, and Disclosure
Of the four trials that examined safety, help-seeking behaviours, and disclosure rates, only one identified improvement (Humphreys et al., 2011). This was a relatively small study (n = 50) that embedded videos within an interactive “Video Doctor,” delivered risk-reduction messages, and simulated a discussion with a prenatal healthcare provider. Humphreys et al. (2011) found that at 1-month follow-up, significantly more women in the intervention group reported having a discussion about IPV risk with their prenatal providers than women receiving usual care (81.8% vs. 16.7%). Three studies that incorporated between 13 and 251 participants found no impact of videos (Flaathen et al., 2022; Klevens et al., 2012b; Tavrow et al., 2021) on women’s help-seeking, disclosure, or safety behaviours. Three of these studies employed researcher-designed surveys to measure outcomes, whereas Klevens et al. (2012b) analysed medical record data from 54,887 female client visits to examine changes in disclosure rates. Although the large sample size and use of routinely collected medical data employed by Klevens et al. (2012b) may enhance the reliability of findings, the study was subject to a number of limitations. These included lack of organisational support, time constraints, and substantial imbalances in sample size between intervention and control clinics. Collectively, these factors may have compromised the interpretability and generalisability of the findings.
Quality of Life
Two articles representing the two largest studies (n = 251 and N = 2,364) reported on QoL outcomes (Flaathen et al., 2022; Klevens et al., 2012a). Both studies used validated QoL measures to assess outcomes. Klevens et al. (2012a) used the SF-12 to measure QoL alongside days of work and household activities lost and found no significant differences between baseline and 1-year follow-up. The study SPS (using the WHOQoL-BREF) found no significant differences between groups at 3-month post-intervention (Flaathen et al., 2022).
Participant Satisfaction and Feedback
The seven trials assessing acceptability and satisfaction were predominantly qualitative or mixed methods and included smaller sample sizes (N = 9 to N = 60). These studies all found high acceptability of DFV video interventions among women (Choo et al., 2016; Flaathen et al., 2020; Humphreys et al., 2011; Tavrow et al., 2021, 2022; Walter et al., 2021) and healthcare providers (Garnweidner-Holme et al., 2020). Women saw DFV video interventions as informative and meaningful, particularly regarding the inclusion of personal testimonials (Tavrow et al., 2021, 2022). Findings suggested that video interventions were useful if followed by patient-provider discussions and stressed the importance of discretion and trust during disclosure (Tavrow et al., 2021, 2022). Women interviewed by Walter et al. (2021) reported that the video increased their awareness of different types of DFV. One woman felt that videos could be important for women who lacked knowledge of their civil rights and needed information about where to seek help. Qualitative feedback from the VAV project and SPS recommended improvements, such as greater specificity about support services (listing available services with contact details), clearer demonstrations and examples of DFV, providing additional avenues for disclosure (such as a hotline number in the patients’ native language) and showing how a woman’s life may improve after disclosure of DFV.
Healthcare Provider Feedback
Two articles interviewed 9 and 12 healthcare providers to obtain their opinions and recommendations and to identify perceived barriers to implementation. Providers involved in the VAV trial reported that the video made it somewhat or definitely easier for them to screen for IPV (Tavrow et al., 2021). However, 50% felt that the videos disrupted workflow a little or somewhat, and 66% felt that the clinic should continue showing the videos. Midwives recruiting for the SPS believed that the video could supplement face-to-face care and promote safety behaviours, though it was still important to build trust and rapport with women before questioning them about DFV. When investigating enablers and challenges to implementation, upper management support and encouragement were identified as crucial factors for engaging staff. Staff turnover and technical issues were also barriers to successful implementation. Staff feedback also suggested that there was a general lack of knowledge and training relating to DFV screening (Garnweidner-Holme et al., 2020; Tavrow et al., 2021).
Evaluation
The eight studies that included quantitative measures of knowledge, awareness, or help-seeking used purpose-specific research-created surveys. Only the two studies that evaluated changes in QoL included validated surveys: the WHOQoL-BREF (Flaathen et al., 2022) and the SF-12 (Klevens et al., 2012a).
Discussion
Video-based interventions have been used in healthcare settings to increase knowledge, awareness, and help-seeking behaviours in women who have experienced, or are at risk of experiencing, DFV. To the author’s knowledge, there have been no previous systematic reviews examining the evidence regarding video interventions in this context. This review aimed to synthesise the evidence of these interventions to better understand their characteristics and impacts on knowledge, awareness, help-seeking behaviours, and disclosure. It also synthesised satisfaction, acceptability, and feedback from patients, women, and healthcare providers.
Overall, out of the seven trials, three utilised videos within broader screening processes and four were standalone interventions. Mixed evidence was observed across outcomes: knowledge and awareness findings were not significant in quantitative trials, but qualitative studies reported that participants found the videos acceptable, informative, and helpful. Help-seeking and disclosure outcomes were inconsistent, and QoL outcomes did not show significant quantitative improvement in the largest studies. These mixed findings likely reflect heterogeneity in intervention duration, setting, and study design. The use of non-validated, researcher-created surveys hinders comparability between these studies and limits generalisability to other populations. Despite limited quantitative evidence, feedback from women and healthcare providers indicated that it was a useful first step in seeking support.
Five trials measured disclosure and help-seeking behaviours. However, only one moderately-sized quantitative study found significant improvements in terms of discussion rates (i.e. how many women reported having a conversation with their healthcare provider about IPV) (Humphreys et al., 2011). Qualitative evidence suggested that videos may still support disclosure, particularly if screening occurred privately, with provider follow-up recommended. Healthcare providers found them useful as a primer to initiate discussions. These findings highlight that participant satisfaction and behavioural patterns (such as readiness and intention to change or long-term behaviour change) may not be adequately captured by short-term quantitative measures. Findings suggest that videos could be flexibly integrated into healthcare workflows. Humphreys et al. (2011) used a “video doctor” recording played by an actor to prompt discussion points with women experiencing DFV. They found that women in the intervention group were more likely to continue the discussion with a healthcare provider.
Standalone video interventions may provide additional cost-effective advantages. If they are relatively short in duration, they could be administered to more women at a smaller cost to healthcare resources. Longer screening measures, on the other hand, may utilise unnecessary time and resources from healthcare. The trials that used videos embedded in screening interventions took longer to complete and still required follow-ups from healthcare staff. A short video shown before a healthcare appointment, however, may be less time-intensive and integrated more efficiently into healthcare workflows while also improving knowledge, attitudes, and awareness of DFV (Ernst et al., 2011). Although a short video may be far from a one-size-fits-all solution, its cost-effectiveness suggests it could be beneficial as a “first step” or “door opener” to further awareness and help-seeking.
While there was some evidence of benefit from video interventions, findings were often mixed or non-significant. This is unsurprising, given that DFV is a complex situation in which disclosing and improving it are not always options due to family, financial, and systemic nuances (Coumarelos, 2019). Women impacted by DFV often carry pervasive and lifelong trauma symptoms that could impact their health and functioning (Lynch et al., 2022). While it is important to deliver DFV interventions that improve women’s knowledge and awareness, avoidance of re-traumatisation must be considered when retelling and reliving traumatic experiences to women who have experienced DFV (Lynch et al., 2022). Triggering maladaptive states of arousal in women can impact their ability to take in information, which may explain these mixed findings (Courtois, 2004). As such, interventions delivered in a setting where women feel safe and supported are essential. The format and content of the videos may also have negatively influenced outcomes. Simulations of violent encounters and DFV-related events, such as the simulation intervention in Ernst et al. (2011), may re-traumatise women or cause viewers to disengage with the content.
Women in this review reiterated the need for privacy when viewing video interventions and disclosing DFV. All trials in this review delivered video interventions in private settings on tablets or laptops; however, there were some logistical barriers for healthcare providers. Findings from Tavrow et al. (2021) showed that increased patient load impacted staff’s ability to privately deliver the video intervention to eligible women in examination rooms. The importance of privacy was evident as women were more likely to disclose DFV, or at least more willing to disclose DFV, when shown the intervention in private. Qualitative feedback from women further stressed the importance of viewing video interventions in private settings. Furthermore, there are substantial cultural, systemic, and logistical barriers towards women feeling safe to disclose DFV. Women might hold concerns around disclosing DFV victimisation to healthcare providers, due to a lack of trust in providers, a belief they will be unable to help, safety concerns, fear of child removal, and other consequences of disclosing (Heron & Eisma, 2021; Rathnayake et al., 2023). Disclosure is an increasingly complex issue for CALD women who may feel stigmatised, face language barriers, and fear deportation (Tavrow et al., 2022). Providers frequently report a reluctance to instigate conversations around DFV due to concerns around heavy workloads, insufficient training, high patient load, discomfort, or fear of offending women (Garnweidner-Holme et al., 2020; Tavrow et al., 2021). Video interventions that address these barriers could ideally prime further conversations around DFV.
While many quantitative disclosure or help-seeking outcomes did not significantly improve, qualitative findings suggested that women still found video interventions useful. These disparate findings could be explained by the Stages of Change theory (Prochaska & DiClemente, 1984). This theory suggests that people move back and forth through steps toward change; from Precontemplation, Contemplation, Preparation, Action, and hopefully to Maintenance of behaviour change. Women may be moving from precontemplation toward contemplation or preparation, which would represent a significant positive shift, but may not be reflected in quantitative measures of help-seeking and disclosure. Measures of QoL were also not significantly impacted by any intervention. Even when victims had an increased awareness of DFV not being their fault, their QoL did not meaningfully improve (Klevens et al., 2015). This may indicate that QoL measures are more closely tied to material changes in the environment or lifestyle than to alterations in knowledge, attitudes, or disclosure. If so, these measures may not reflect appreciable improvements until many years of post-intervention.
Strengths and Limitations
A strength of the current study is the inclusion of qualitative, quantitative, and mixed-methods research. Including qualitative data allows the authors of this review to examine women’s attitudes towards, and acceptance of, DFV video interventions in-depth. This permits further investigation into related topics that may not have otherwise been considered by researchers, such as what was considered important content to include for women in the video interventions. All studies that conducted follow-up assessments adequately described attrition, which was minimal for all studies.
This systematic review contains a number of limitations to consider. First, the number of included studies was small, particularly those that incorporate robust, quantitative methodologies using validated tools. Sample sizes were also limited for the majority of studies; however, four of these achieved adequate numbers for the qualitative methods they employed. Considerable heterogeneity was observed across studies in terms of design, intervention content and format, and participant characteristics. In addition, studies screening for DFV provided little detail regarding the criteria for recent DFV used. A formal grey literature search was not conducted, which may have identified additional DFV video interventions and intervention characteristics. However, the current review focused on interventions that included sufficient methodological detail and evaluation of outcomes, such as participant satisfaction, knowledge, disclosure, or help-seeking. Many publicly available or unpublished DFV-related videos lack this level of reporting or evaluation, limiting their suitability for systematic appraisal and synthesis.
A further limitation of the study is that the included papers involved broader populations or study participants beyond the core target population (such as men and perpetrators). The inclusion of broad populations may provide greater contextual insight but increases heterogeneity and reduces generalisability to the intended population. Lack of ethnic inclusion, description, or subgroup analyses in these papers also limited the ability to determine culture-specific acceptability and feedback. Another limitation is the exclusion of foreign language studies due to a lack of translation services. We acknowledge that this may have led to the exclusion of some important international studies in this area. Furthermore, while most studies incorporated validated tools, there are no validated assessments of participants’ knowledge and understanding of DFV. Therefore, the studies relied on independently created, researcher-designed surveys, which introduced additional heterogeneity and complexity to the interpretation.
Critical Findings
Few studies have examined the impact and acceptability of DFV video interventions on knowledge and help-seeking, and existing studies vary widely in format, population, evaluation, and follow-up duration.
Video interventions were not seen to improve quantitative measures of knowledge, awareness, or QoL.
Impacts on help-seeking and safety behaviours were mixed, with only one of four papers identifying improvements.
According to qualitative findings with women and healthcare providers, videos were acceptable and useful in providing essential information and education around DFV and may work as a “first step” for provider conversations.
Clinical Implications
This review highlights the clinical implications of using DFV video interventions for women accessing health services. See Table 3 for a summary of the implications. Videos appear to be a practical strategy to raise awareness of DFV. Video as a method of delivery offers several advantages, including increased confidentiality, reduced costs, a lighter time burden for clinicians, and expanded access to underserved patients. These advantages mitigate several barriers that women experiencing DFV may face in receiving care. Perpetrators of DFV are known to instigate coercion and harassment through technology, which creates privacy concerns for victims (Rogers et al., 2023). The capacity to show videos in healthcare settings with complete privacy, such as on tablets or via QR codes in toilet cubicles/examination rooms, could increase confidentiality and victim safety.
Implications for Practice, Policy, and Research.
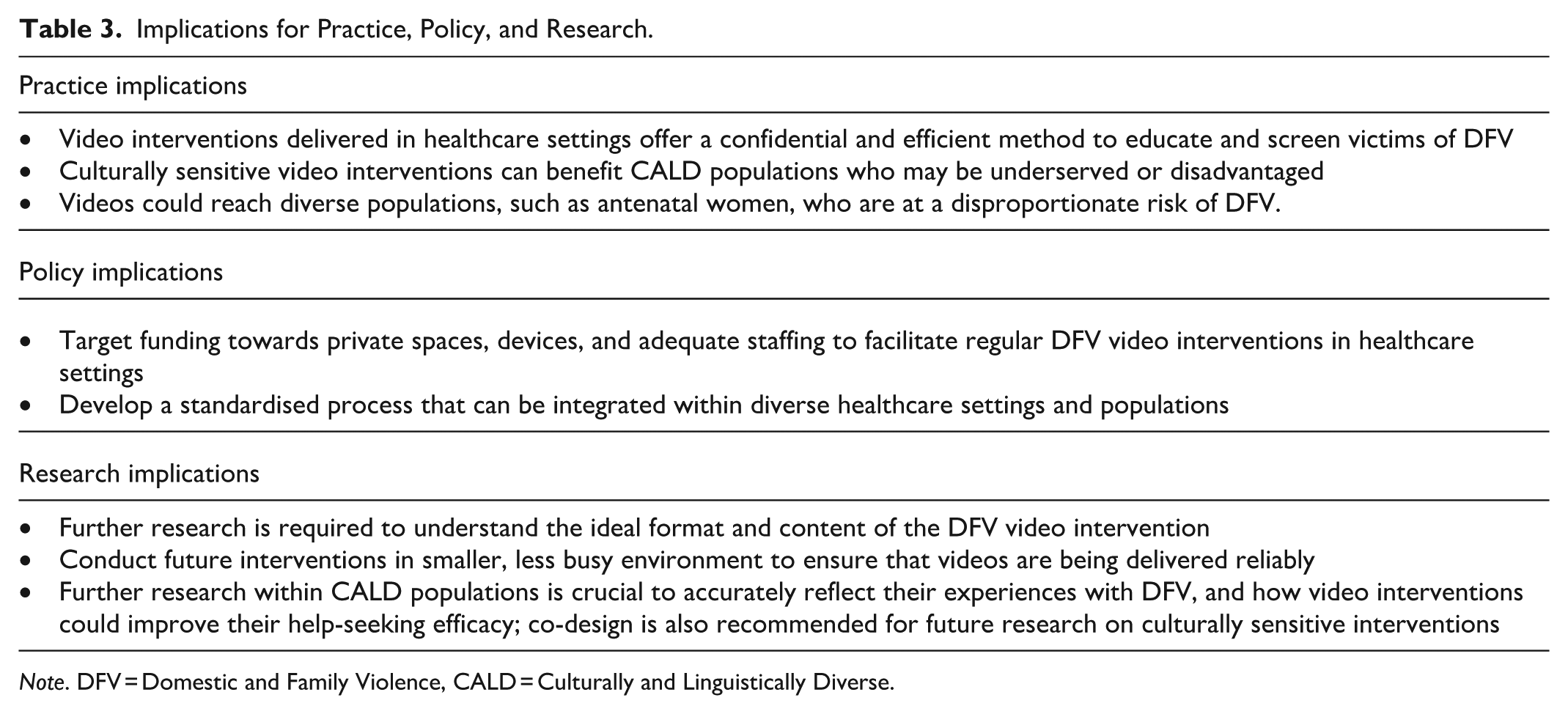
Note. DFV = Domestic and Family Violence, CALD = Culturally and Linguistically Diverse.
DFV video interventions could further benefit underserved consumers and disadvantaged minority populations if delivered in a discreet and culturally sensitive manner. When tailored to serve historically underrepresented communities, culturally congruent digital DFV interventions have been shown to be effective in raising awareness and screening of DFV (Koziol-McLain et al., 2018). This has clinical implications for at-risk populations such as CALD women who require culturally sensitive videos translated into their native language to address stigma, language barriers, legal and health literacy, and deportation fears (Tavrow et al., 2021; Walter et al., 2021). This highlights the necessity of tailored and culturally sensitive interventions rather than a one-size-fits-all approach.
Furthermore, some trials focused on DFV interventions for antenatal women. While antenatal women are particularly vulnerable to DFV (Hailu et al., 2023; Lockington et al., 2023), their increased contact with healthcare services offers an opportune time to screen for DFV and provide support (Heron & Eisma, 2021; O’Reilly et al., 2010). The findings of this review suggest that video interventions implemented for women receiving obstetric care may be effective in improving DFV help-seeking behaviours.
Although videos should be tailored to suit diverse populations, a common theme among DFV video interventions was that they shared an element of encouragement and positive reinforcement around DFV disclosure. Tuong et al. (2014) found that “gain-framed” videos, videos that focus on gaining favourable outcomes (Bunge et al., 2010), may be effective in promoting positive health behaviours. While they did not focus on DFV behaviours, it was consistently reiterated by women in the review that video interventions should incorporate an element of hope at the end. If videos incorporate “gain framing,” there may be opportunities for the versatile design of video interventions.
Recommendations For Further Research
Our findings add to existing knowledge of what works to educate and support women regarding DFV. Considering these findings, the authors suggest several recommendations for future research. Based on the reviewed evidence, DFV video interventions may be a useful tool when preceding further screening and support from healthcare providers, rather than being used alone. However, this becomes difficult when considering cost-effectiveness and resource barriers. Findings in this review highlight that healthcare providers had difficulties in implementing video interventions when patient loads were high. This indicates that future studies may first need to be trialed in smaller, less busy environments to ensure that study protocols can be adhered to without compromising patient care. This would additionally facilitate the opportunity to trial more in-depth quantitative psychometric measures to fully elucidate the impact of using video interventions for DFV.
Additional in-depth studies are required to determine ideal formats of delivery for these video interventions (e.g. screening vs. standalone, narrative, informational). Another useful method of video style could be animation. No trials in the current review explicitly mentioned utilising animated videos. Animated videos have the advantages of being less resource-intensive to produce and have also been found to improve short-term outcomes in healthcare settings (Dahodwala et al., 2018). Future research is recommended on video formats, including animation, to improve reach and cost-effectiveness.
Only two trials engaged stakeholders in co-designing video interventions. Given the in-depth qualitative feedback on acceptability and satisfaction, it is recommended that future interventions engage diverse populations with experiences of DFV and healthcare providers to co-design video interventions. Suggestions from women in the current review included extra details of abuse, help-seeking, implications of disclosure, and role-playing scenarios. It is recommended that future research focus on engaging women to aid in the development of different types of video interventions. It is also recommended that future interventions focus on engaging broader populations, such as CALD populations and male victims of DFV. The findings from Ernst et al. (2011) indicate there may be gender differences in terms of the impacts of these interventions.
Conclusion
This review aimed to evaluate how video interventions in healthcare settings could improve knowledge, awareness, and help-seeking behaviours in women experiencing, or at risk of experiencing, DFV. Some studies provided evidence of their efficacy; however, results were mixed. Privacy concerns, healthcare resources, stigma, and cultural barriers may have contributed to these mixed findings. Regardless, qualitative feedback suggests that women and healthcare providers find DFV video interventions important and valuable. Future research should prioritise the co-design of interventions and trial alternate formats, such as animation, that streamline integration with healthcare processes. Furthermore, future trials should focus on methodological rigour and utilisation of validated measures to observe short- and long-term outcomes.
Supplemental Material
sj-docx-1-tva-10.1177_15248380261455772 – Supplemental material for Domestic and Family Violence Video Interventions Designed for Women in Healthcare Settings: A Systematic Review
Supplemental material, sj-docx-1-tva-10.1177_15248380261455772 for Domestic and Family Violence Video Interventions Designed for Women in Healthcare Settings: A Systematic Review by Matthew Porter, Kerri Marie Gillespie, Sam Adhikary, Megan McClenaghan and Grace Branjerdporn in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
The authors acknowledge the support of Mater Foundation and Mater Research Institute-University of Queensland, as well as Hayley Kimball and Reaksmey Pirotta for their assistance.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is publicly available as this review synthesises previously published literature.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.