
Abstract
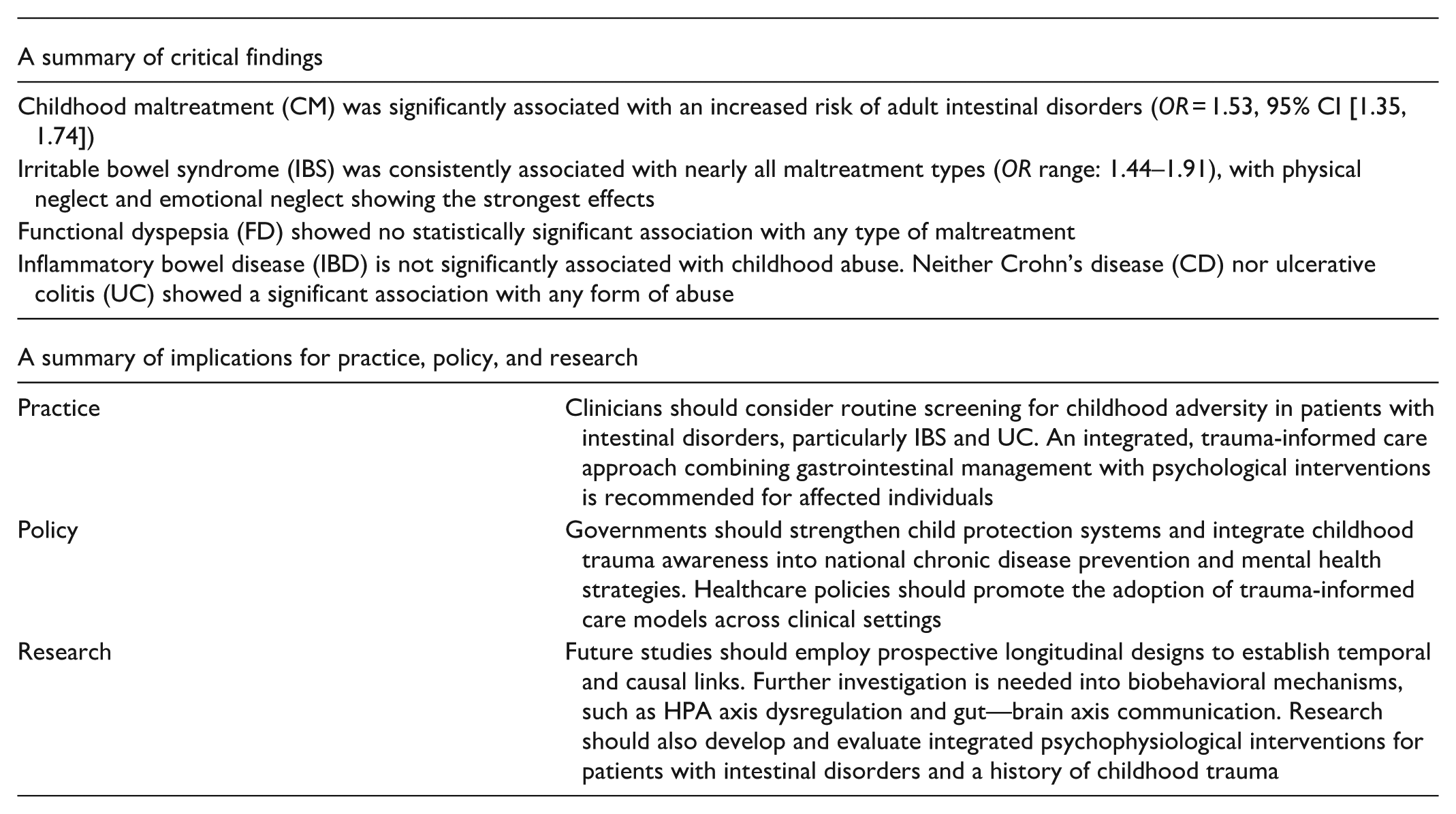
Over recent decades, research has steadily accumulated evidence on the relationship between childhood maltreatment (CM) and adult intestinal disorders, yet the findings remain inconsistent across studies. To address this, a three-level meta-analysis was conducted to quantitatively synthesize existing data, assessing both the overall association and its specificity across disease subtypes and maltreatment types. A comprehensive literature search identified 22 studies (comprising 498,709 participants and 75 effect sizes) from PubMed, Embase, Web of Science, Scopus, ScienceDirect, and PsycINFO databases up to April 2026. Pooled results revealed a significant positive association between CM and the risk of adult intestinal disorders (OR = 1.53, 95% CI [1.35, 1.74]). Notably, this association exhibited substantial specificity: irritable bowel syndrome was consistently linked with nearly all maltreatment types (OR range: 1.44–1.91), while functional dyspepsia showed no statistically significant association. Inflammatory bowel disease is not significantly associated with childhood abuse. Neither Crohn’s disease nor ulcerative colitis showed a significant association with any form of abuse. Sensitivity analyses affirmed the robustness of effect sizes, with no significant publication bias detected. This three-level meta-analysis highlights CM as a notable risk factor for specific adult intestinal disorders, highlighting the need to integrate early-life adversity into etiological models and trauma-informed clinical care for intestinal conditions.
Introduction
Childhood maltreatment (CM) is a widespread global public health concern with profound, long-lasting effects. According to a 2024 UNICEF report, one in five females and one in seven males have experienced sexual abuse during childhood (UNICEF, 2025). Worldwide, nearly 450 million children under the age of five endure psychological aggression or physical punishment at home (UNICEF, 2024). Simultaneously, not only do people pay attention to the long-term psychological problems caused by childhood abuse, but their concern about the physical health consequences is also increasing. The adverse experiences during childhood have been proven to have a definite impact on adult physical illnesses, yet these effects are rarely known among practitioners (Gordon, 2021; Hughes et al., 2017; Merrick et al., 2019). This has led to clinicians focusing solely on patients’ somatic symptoms for a long time. Among these, the link to chronic intestinal disorders has gained particular focus (Espinosa Dice et al., 2024). The etiology of adult intestinal disorders is multifactorial, with the biopsychosocial model offering a foundational framework for understanding the interaction between biological susceptibility, psychological stress, and social context (Drossman, 2006). Within this framework, CM is considered a powerful early-life stressor that can disrupt the brain–gut axis, leading to long-term dysregulation and heightened disease risk. Several studies have investigated the relationship between CM and the onset of adult intestinal disorders, examining mediating factors and proposing relevant theories (Fuller-Thomson et al., 2015). However, substantial variability exists across these findings, highlighting the need for a comprehensive synthesis of the evidence to better understand this association (Priego-Parra et al., 2024; Schubach et al., 2024). This inconsistency may arise from two main issues: first, treating CM or intestinal disorders as homogeneous constructs obscures potential subtype-specific pathways; second, a significant methodological limitation is that primary studies often report multiple, statistically dependent effect sizes, which traditional meta-analyses fail to address, leading to biased estimates. To overcome these limitations and synthesize the existing evidence with greater methodological rigor, the present study employs a three-level meta-analytic model. This approach is specifically designed to handle dependent effect sizes nested within studies, yielding more precise pooled estimates. Our objectives are threefold: (1) to quantify the overall CM-intestinal disorder association; (2) to examine specificity across maltreatment types and disease subtypes; and (3) to explore sources of heterogeneity. This review aims to resolve inconsistencies in previous findings and identify distinct risk patterns, with implications for etiology, clinical assessment, and public health.
Conceptualizations of Central Constructs
Childhood Maltreatment
CM is defined by the World Health Organization (WHO) as abuse and neglect occurring to individuals under the age of 18. This encompasses all forms of physical and/or emotional mistreatment, sexual abuse, neglect, negligence, and exploitation, resulting in actual or potential harm to a child’s health, survival, development, or dignity within a relationship of responsibility, trust, or power (WHO, 2025). Drawing from a comprehensive review of existing definitions, this study examines CM as both a composite construct and through its specific subtypes: any abuse, any neglect, physical abuse, physical neglect, emotional abuse, emotional neglect, and sexual abuse.
Intestinal Diseases
Intestinal diseases refer to pathological processes affecting any segment of the intestine, from the duodenum to the rectum (MeSH). Three clinical entities dominate the epidemiological burden: Irritable Bowel Syndrome (IBS), a functional disorder marked by chronic abdominal pain and altered bowel habits without structural abnormalities (Chey et al., 2015); Inflammatory Bowel Disease (IBD), an immune-mediated inflammation of the intestinal tract, including Crohn’s disease (CD) and ulcerative colitis (UC; Kaplan, 2015); and Functional Dyspepsia (FD), a functional upper intestinal disorder characterized by postprandial fullness, early satiety, or epigastric pain without organic causes (Ford et al., 2020). A thorough search included all MeSH-listed intestinal disease categories to ensure a comprehensive review.
The Relationship Between CM and Adult Intestinal Disorders
The association between CM and adult intestinal disorders is well conceptualized within the brain-gut axis framework, a key component of the biopsychosocial model (Chen et al., 2025; Qian et al., 2025). CM, as a severe early-life stressor, is hypothesized to induce long-term dysregulation across multiple interconnected physiological, psychological, and social pathways (Lee et al., 2025; Sheng et al., 2025).
Physiological pathways: CM can disrupt gut microbiota composition, reducing beneficial bacteria and increasing pro-inflammatory species, thus destabilizing the intestinal ecosystem (Karaboycheva et al., 2024). This dysbiosis, coupled with stress-induced inflammatory responses, can compromise intestinal barrier integrity (Xie et al., 2025). In addition, CM may lead to persistent sensitization of visceral afferent nerves, lowering pain thresholds, and contributing to the core symptoms of functional disorder (Tao et al., 2023; Tomoda et al., 2025).
Psychological pathways: Chronic stress resulting from maltreatment activates the hypothalamic-pituitary-adrenal (HPA) axis and autonomic nervous system, leading to elevated cortisol levels that disrupt gut motility and secretion (Blecker et al., 2025; Martins et al., 2024). Concurrent psychological conditions, such as anxiety and depression, can further alter gut microbiota, creating a vicious cycle via the gut-brain axis (Bai et al., 2024).
Social pathways: Maltreatment negatively impacts attachment and social relationships, acting as a persistent social stressor that affects physiological systems (He et al., 2024). Early social isolation has been linked to sustained high cortisol levels, which damage the gut barrier (Beaucage-Charron et al., 2023). Socioeconomic disadvantages associated with maltreatment may limit access to nutritious food and healthcare, further impairing intestinal health (Ming et al., 2025).
The Present Study
Despite accumulating evidence linking CM to adult intestinal disorders, significant gaps remain that hinder a more nuanced understanding and clinical application. A primary limitation in the existing literature is the tendency to treat both CM and intestinal disorders as homogeneous constructs. This broad approach obscures potential differential risk pathways: distinct forms of maltreatment may engage different neurobiological and psychological stress-response systems, while intestinal disorders with fundamentally diverse pathophysiologies may exhibit varying sensitivities to early-life adversity. This study aims to clarify precise, subtype-specific associations. It is hypothesized that the strength and significance of the CM-intestinal disorder link are not uniform, but rather moderated by the specific type of maltreatment experienced and the type of intestinal disease developed. Therefore, a central and novel objective of this three-level meta-analysis is to systematically test for interaction effects between maltreatment types (any abuse, any neglect, physical abuse, physical neglect, emotional abuse, emotional neglect, and sexual abuse) and intestinal disease subtypes (IBS, FD, IBD, UC, and CD). Methodologically, this study employs a three-level meta-analytic model, particularly suited to address this research question. Primary studies in this area often report multiple CM subtypes and multiple disease outcomes within the same sample, resulting in statistically dependent effect sizes. Our chosen model explicitly accounts for this dependency, providing more accurate and reliable estimates for the complex interaction analyses intended. In summary, this study will offer a comprehensive overview of existing research on the impact of CM on intestinal diseases in adulthood. This review will inform trauma-oriented clinical practice by identifying specific patient groups most likely to benefit from comprehensive psychological care and will ultimately guide future research toward exploring the underlying mechanisms behind these distinct associations.
Method
Literature Search and Study Selection
According to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, we conducted a comprehensive and systematic literature search (Moher et al., 2009; Page et al., 2021). The search strategy was designed using the Population, Exposure, Outcome framework to identify observational studies examining the relationship between CM and various intestinal disorders (Aromataris et al., 2024). Six major electronic databases—PubMed, Web of Science, Embase, Scopus, ScienceDirect, and PsycINFO—were searched from their inception until April 28, 2026. A thorough search strategy was developed combining subject headings (MeSH, Emtree) and free-text terms, structured around two core conceptual blocks linked with the Boolean operator “AND.” The exposure block included terms for “CM,” “adverse childhood experiences,” “child abuse,” “neglect,” and their specific subtypes. The outcome block utilized the broad Medical Subject Headings (MeSH) term “Intestinal Diseases” and encompassed key terms such as “IBDs,” “Colitis, Ulcerative,” “CD,” “IBS,” “FD,” and “Intestinal Neoplasms.” The complete, database-specific search syntax is available in Supplemental Material S1. In addition, relevant literature reviews and reference lists related to the topic were carefully examined to identify further eligible studies. The study selection process is summarized in a PRISMA flow diagram (Figure 1).
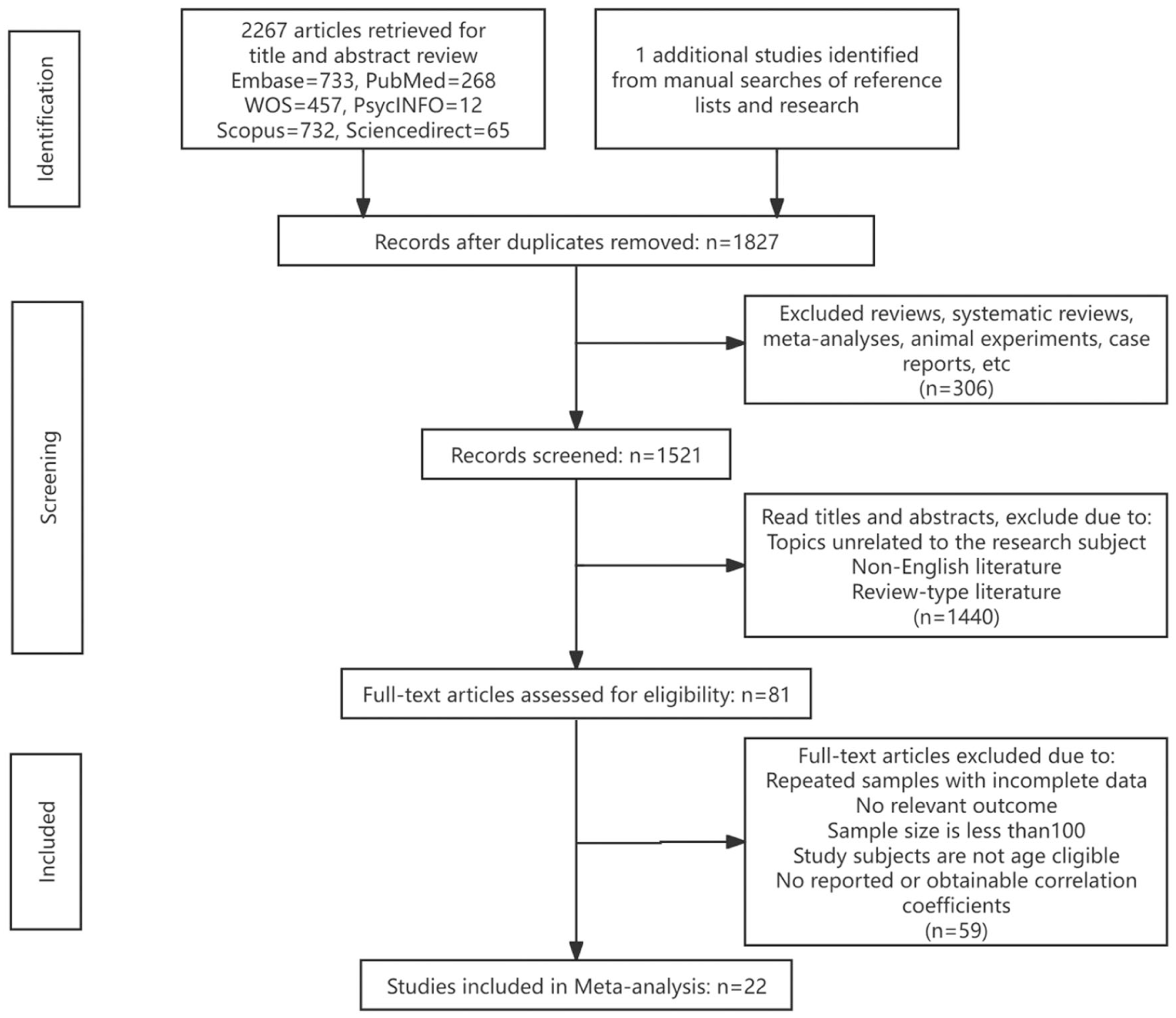
Flow chart for screening study (PRISMA).
The inclusion criteria for studies were as follows: (1) Published in English; (2) Cross-sectional, case-control, or cohort design; (3) Involving adults (18 years or older) who reported exposure to maltreatment before the age of 18; (4) Investigating the association between maltreatment (including any abuse, any neglect, physical abuse, sexual abuse, emotional abuse, physical neglect, and emotional neglect) before the age of 18 and intestinal diseases, and reporting odds ratios (ORs) or prevalence rates. Studies were excluded if they: (1) Were not quantitative research; (2) Were not written in English; (3) Used an overlapping sample; or (4) Did not present relevant statistical information required to calculate the OR between CM and intestinal diseases.
Data Set Preparation
The OR was selected as the primary measure of association to assess the relationship between CM and intestinal diseases. The OR is particularly well-suited for this purpose, as the available evidence largely stems from observational studies, where it serves as an effective estimator of association. In addition, the majority of the included studies reported their results as ORs with 95% confidence intervals (CIs). For studies that did not directly report these metrics, this study followed the conversion methods recommended in the Cochrane Handbook for Systematic Reviews of Interventions and the meta-analysis principles outlined by Borenstein et al. (2021) to calculate the OR and 95% CI from contingency tables or p-values (Higgins et al., 2024).
Effect Design Factors
The following data were extracted from all eligible studies:
(1) Method factors: These include the study design (e.g., cross-sectional or longitudinal), methods for measuring child trauma (e.g., Child Trauma Questionnaire, Child Trauma Questionnaire Short Form), and diagnostic methods for intestinal diseases (e.g., Rome III or Rome IV criteria); (2) Sample factors: These consist of total sample size, sample age, and the country from which the sample was drawn (e.g., United States and Canada); (3) Variable factors: These include dimensions of child trauma (i.e., any abuse, any neglect, physical abuse, physical neglect, emotional abuse, emotional neglect, and sexual abuse); (4) Types of diseases: These include various intestinal diseases, such as IBS, IBD (comprising CD and UC), and FD.
Effect Rigor
To evaluate the quality of cross-sectional studies, the JBI scale was applied (Porritt et al., 2020). This scale assesses multiple aspects, including sample representativeness, exposure measurement, disease diagnostic methods, identification and handling of confounders, outcome measurement, and statistical analysis methods. Each question is answered with “Yes,” “No,” or “Unclear.” The quality of cohort and case-control studies was assessed using the Newcastle-Ottawa Scale (Wells et al., 1996). This scale uses a star rating system (up to 9 stars) and evaluates case-control studies based on three key areas: the source and definition of cases and controls, the comparability between groups and control of key confounding factors, and the accuracy of exposure measurement. For cohort studies, the scale evaluates the representation of exposed and unexposed cohorts, the comparability between groups, the control of confounding factors, and the objective assessment and completeness of outcome events and follow-up. This comprehensive approach ensures that the methodological rigor and potential bias risk of different types of observational studies are thoroughly evaluated (Supplemental Material S2).
Statistical Analyses
Meta-Analysis Method
Given the various types of CM and intestinal diseases examined in the included studies, multiple effect sizes were extracted from individual studies. To account for the statistical dependency among effect sizes derived from the same study, as well as heterogeneity across studies, a three-level meta-analysis was conducted. Compared with traditional meta-analytic approaches, this method allows inclusion of all eligible effect sizes by modeling three variance components: sampling variance of the observed effect sizes (level 1), within-study variance between effect sizes extracted from the same study (level 2), and between-study variance (level 3; Van den Noortgate et al., 2013). We first constructed a three-level random-effects model to estimate the overall association between child maltreatment and intestinal diseases. ORs were log-transformed to obtain log odds ratios (logORs) as the effect size metric. Variances were calculated from the reported 95% CI. All logORs were weighted by the inverse of their variance, and the pooled estimate was then back-transformed to OR for interpretation. Analyses were performed using the “metafor” package in R 4.3.3, with restricted maximum likelihood estimation. Heterogeneity was quantified using variance components (τ2) at both within-study (level 2) and between-study (level 3) levels (Cheung, 2014). In addition, I2 statistics were calculated to describe the proportion of total variability attributable to heterogeneity at each level beyond sampling error. To further examine associations between specific types of CM and subtypes of intestinal diseases, we fitted a three-level meta-regression model using a categorical moderator representing each maltreatment type—disease-subtype combination. The model was specified without an intercept so that each coefficient represented the pooled effect for one observed combination. Effect sizes were analyzed on the log(OR) scale and exponentiated to obtain pooled ORs and 95% CI. To account for the non-independence of multiple effect sizes contributed by the same study, we used a multilevel random-effects structure. This approach enabled heterogeneity to be estimated from the full dataset rather than separately within each combination, thereby improving the stability of variance estimation for combinations with relatively sparse data.
Publication Bias Assessment
Publication bias was assessed using both the funnel plot and Egger’s regression test. A symmetrical funnel plot suggests that publication bias may be negligible. In contrast, for Egger’s regression test, publication bias is considered absent if the linear regression results are nonsignificant (p > .05). In cases where publication bias was detected, the trim-and-fill method was applied to adjust the asymmetrical funnel plot.
Sensitivity Analysis
Given that the multilevel random-effects model may not fully capture the complexity of the data dependency structure, extreme values were identified and excluded from the analysis. Specifically, effect sizes with OR values greater than 10 or less than 0.1 were considered extreme and excluded. The model was then re-estimated to assess the robustness of the results. In addition, the differences in effect sizes between the original and adjusted models were compared to evaluate the impact of extreme values on the overall findings.
Results
Characteristics of Studies
Table 1 summarizes the characteristics of the studies included in this meta-analysis. A total of 22 studies contributed 75 independent effect sizes, involving 4498,709 participants. The study designs were predominantly cross-sectional (K = 14), followed by case-control (K = 5) and cohort (K = 3) studies. Participants were from nine different countries. The disease types primarily consisted of IBS (K = 15), with other intestinal diseases (K = 2), FD (K = 2), IBD (K = 2), UC (K = 2), and CD (K = 2). The types of abuse included emotional abuse (K = 11), physical abuse (K = 16), sexual abuse (K = 15), emotional neglect (K = 5), physical neglect (K = 4), any neglect (K = 2), and any abuse (K = 11). Most studies used standardized scales, such as the Childhood Trauma Questionnaire and the Childhood Experiences of Violence Questionnaire, to assess childhood abuse. Eleven studies used the Rome criteria to diagnose intestinal diseases in participants.
Characteristics of Included Studies.
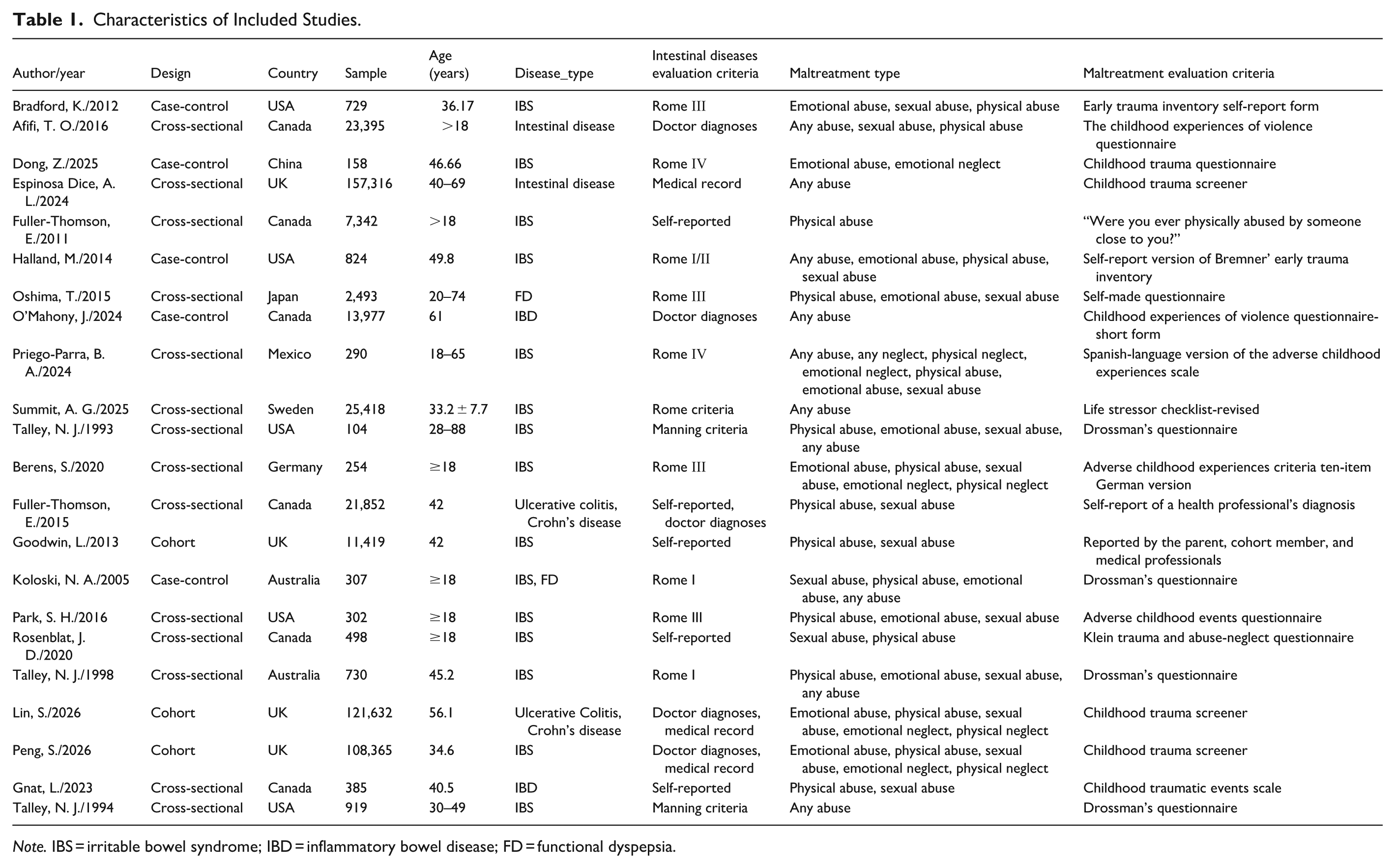
Note. IBS = irritable bowel syndrome; IBD = inflammatory bowel disease; FD = functional dyspepsia.
Overall Effect Sizes
This study employed a three-level meta-analysis model to evaluate the association between adverse childhood experiences and intestinal diseases. Figure 2 presents the overall average effect of the 22 studies, incorporating all 75 effect sizes, and includes the OR and 95% CI of the combined overall effect. The results revealed a significant positive correlation between childhood adverse experiences and the risk of intestinal diseases (combined OR = 1.53, 95% CI [1.35, 1.74]). This indicates that individuals with a history of childhood abuse face a 1.53 times higher risk of developing intestinal diseases compared to those without such experiences. The heterogeneity test revealed substantial variability among the studies (Q = 494.13, df = 74, p < .001, I2 = 93.95%). The variance component estimation showed that the variance between studies (τ2_between = .0693, I2 = 91.69%) was greater than the variance within studies (τ2_within = .0017, I2 = 2.26%). This suggests that, aside from sampling errors, differences in study design, publication year, and publication country also contribute to the observed variability in effect sizes.
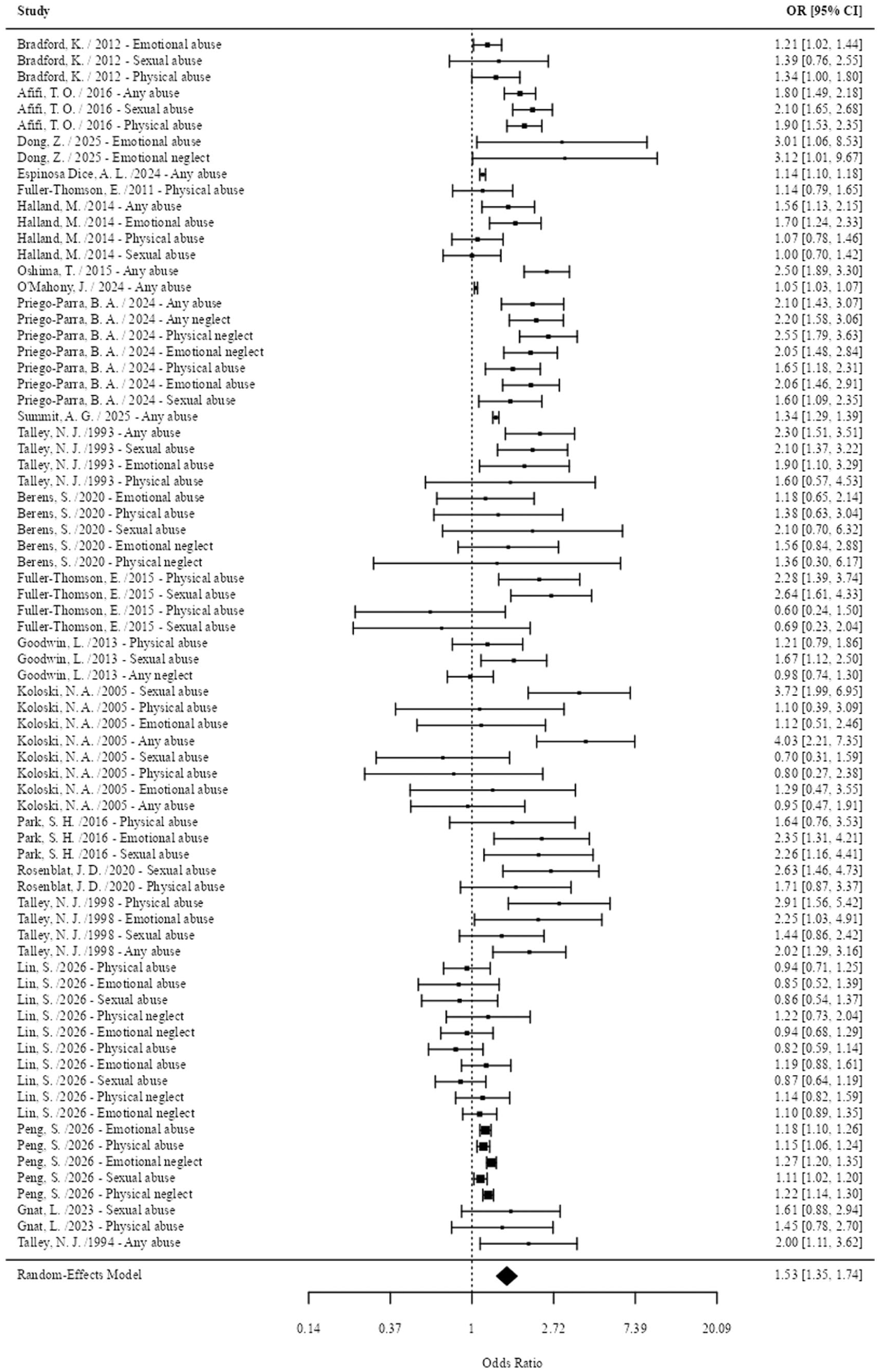
Forest plot of the association between childhood abuse and intestinal disease.
Subtype Analyses
Based on the core hypothesis of this study, we conducted specific analyses according to different forms of childhood abuse and subtypes of intestinal diseases, and only included subgroups with two or more effect values. The analysis revealed a significant interaction between CM and intestinal diseases (Q = 62.14, df = 27, p < .001). Specifically, a detailed breakdown showed that the association patterns exhibited distinct disease-subtype specificity and varied by type of maltreatment (Table 2). IBS demonstrated significant and stable positive associations with all types of maltreatment (any abuse: OR = 1.91, 95% CI [1.50, 2.43]). Regarding specific types of abuse, emotional neglect (OR = 1.77, 95% CI [1.34, 2.32]) and physical neglect (OR = 1.79, 95% CI [1.34, 2.40]) showed the largest ORs for IBS. The association between any neglect and IBS was marginally significant (OR = 1.44, 95% CI [1.01, 2.05]). For other intestinal disease subtypes, the number of available effect sizes was very limited. No statistically significant associations were found for abuse and CD (physical abuse: OR = 1.06, 95% CI [.62, 1.80]; sexual abuse: OR = .97, 95% CI [.52, 1.80], UC (physical abuse: OR = 1.27, 95% CI [.77, 2.11]; sexual abuse: OR = 1.38, 95% CI [0.84, 2.27]), FD (any abuse: OR = 1.55, 95% CI [.93, 2.57]), or intestinal disease (any abuse: OR = 1.42, 95% CI [.93, 2.16]). For subgroups with effect sizes less than two, the results are presented in Supplemental Material S3.
Subgroup Analysis Based on the Type of CM and the Subtype of Intestinal Diseases (K ≥ 2).
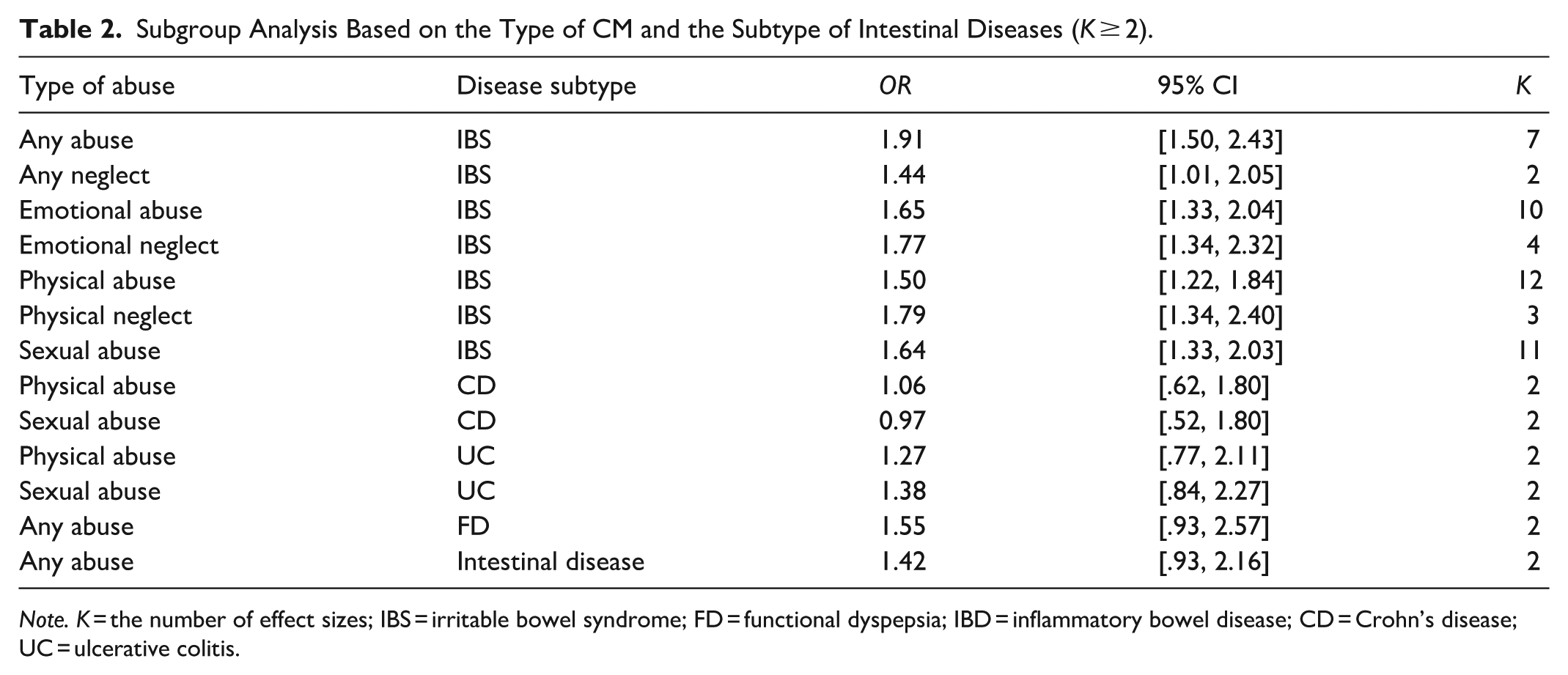
Note. K = the number of effect sizes; IBS = irritable bowel syndrome; FD = functional dyspepsia; IBD = inflammatory bowel disease; CD = Crohn’s disease; UC = ulcerative colitis.
In summary, the findings suggest that the association between CM and adult intestinal diseases is highly specific. The risk of IBS shows a broad, nonspecific increase; other types of intestinal diseases do not have such a correlation. These results indicate that adverse childhood experiences are an important predictor of the risk of intestinal diseases, and abuse is of significant importance in the risk of certain types of intestinal diseases.
Sources of Heterogeneity
To further explore sources of heterogeneity, multilevel meta-regression was employed to investigate between-study heterogeneity. Study design accounted for approximately 48% of the between-study heterogeneity (R2 = 47.9%, p = .0036), indicating that differences in study design contributed substantially to variation in effect sizes. Publication year explained only about 21.8% of the between-study heterogeneity (R2 = 21.8%, p = .0655), suggesting no apparent temporal trend in the results. The country of publication could explain 33.2% of the heterogeneity (R2 = 33.2%, p = .0372). Collectively, the three variables accounted for the majority of the between-study heterogeneity (R2 = 57.4%), and this combined effect was statistically significant (p = 0.0087). Notably, the total variance explained by the full model exceeds the sum of the individual R2 values from univariable models, which is consistent with the overlapping explanatory variance among covariates in a multivariable meta-regression framework.
Publication Bias and Sensitivity Analysis
To assess potential publication bias, multiple testing methods were employed. First, a funnel plot was generated for the overall effect size (Figure 3). Visual inspection suggested a roughly symmetrical distribution, indicating a low likelihood of publication bias. To quantify this, Egger’s regression test was performed, incorporating the standard error as a covariate in a multilevel meta-regression model. The result showed a coefficient of .214 (p = .562), indicating no significant publication bias. To estimate the impact of missing studies on the overall effect size, an imputation method was used. The original analysis included 22 studies, and the imputation analysis estimated that five virtual studies would be needed to restore symmetry to the funnel plot (Figure 4). After filling, the adjusted combined OR was 1.34, which was not significantly different from the original combined OR of 1.46. This suggests that the influence of publication bias was minimal. These results indicate that publication bias is unlikely to significantly affect the findings of this study, although it cannot be entirely ruled out. However, it is unlikely to alter the main conclusion of the meta-analysis.
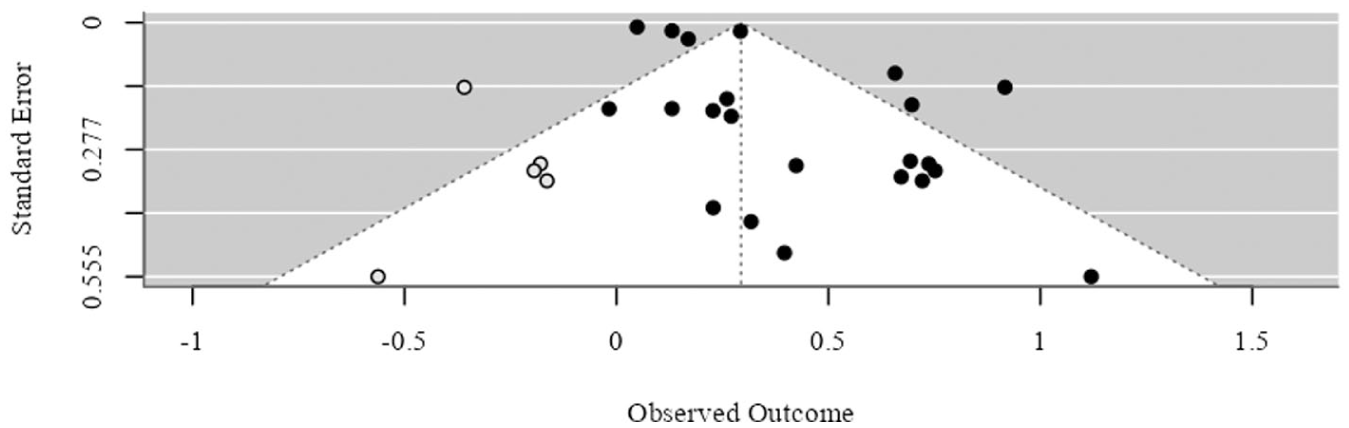
Funnel plot of the main overall effect size.
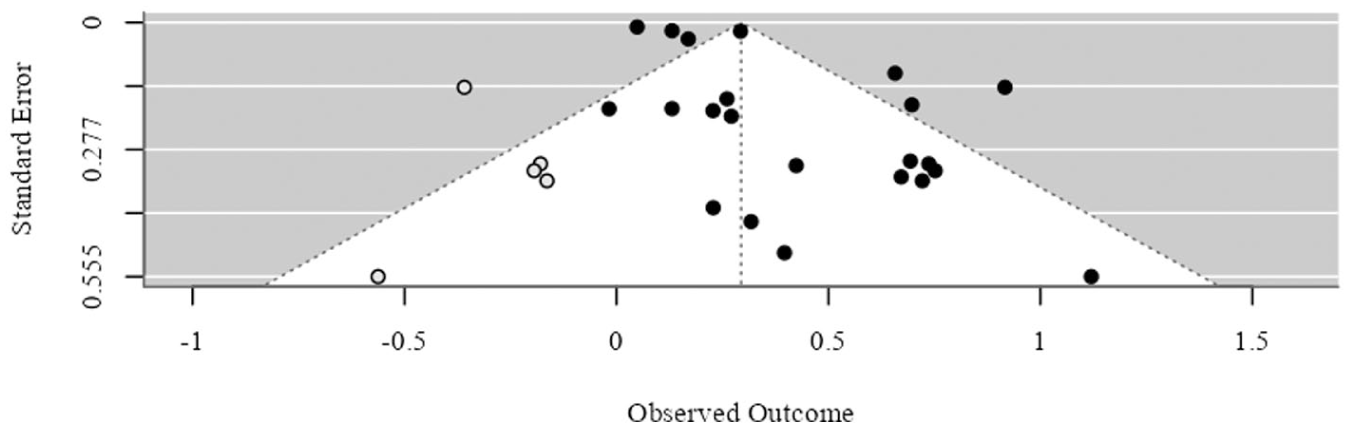
Funnel plot of the trim-and-fill method.
To evaluate the robustness of the results, a systematic sensitivity analysis was conducted. The one-by-one exclusion method showed that, when each study was excluded individually, the recalculated combined OR values fluctuated between 1.493 and 1.568, with only a small variation. More importantly, the lower limits of all recalculated 95% CIs were above 1, indicating that the main conclusion was not dependent on any single study, and the results were highly robust.
Discussion
This three-level meta-analysis, incorporating data from 22 studies with 498,709 participants, systematically examined the association between childhood abuse and the risk of intestinal diseases in adulthood. The key findings are as follows: (1) a moderately significant positive correlation between childhood adverse experiences and the overall risk of adult intestinal diseases (combined OR = 1.53); (2) a notable specificity in the association across disease subtypes and abuse types; (3) a low dependence on individual studies, with no significant publication bias detected. These findings provide valuable quantitative evidence for understanding the complex link between childhood psychosocial trauma and adult intestinal diseases.
The study confirms that childhood abuse is a significant risk factor for the development of intestinal diseases in adulthood. The observed overall association aligns with previous meta-analytic findings on the relationship between childhood abuse and intestinal diseases. The underlying biological mechanism likely involves long-term disruption of the “brain–gut axis.” Chronic or severe stress during childhood can lead to abnormal glucocorticoid secretion, immune-inflammatory dysregulation (such as elevated pro-inflammatory cytokines), increased intestinal permeability, and alterations in the gut microbiome through persistent activation of the HPA axis (Goltser-Dubner et al., 2025). These physiological changes collectively form the pathophysiological basis for various functional and IBDs (Bretto et al., 2025).
A key discovery in this study is the specific pattern of association. For IBS, significant positive associations were observed across nearly all types of CM, including emotional, physical, and sexual abuse as well as neglect. Among these, physical and emotional neglect showed relatively large point estimates (OR = 1.79 and 1.77, respectively). Current studies have established a significant association between childhood adversity and the increased risk of nonspecific IBS. As a classic brain-gut interaction disorder, IBS is characterized by visceral hypersensitivity, abnormal intestinal motility, and dysregulation of central pain processing (Raskov et al., 2016). These features may arise from long-term remodeling of early trauma via the HPA axis and limbic system, resulting in persistent functional changes in the stress-response system and central emotional regulation pathways (Powell et al., 2017). In contrast, the association between FD and childhood adversity did not reach statistical significance. This discrepancy suggests that, while IBS and FD are both functional intestinal disorders, their sensitivity to early-life stressors differs in terms of underlying pathological mechanisms. The onset of FD may be more closely linked to changes in vagal nerve tone and the local inflammatory microenvironment of the duodenum (Ali & Chen, 2023), whereas the central sensitization mechanism in IBS is more heavily influenced by HPA axis programming. In addition, the timing of stress exposure during critical developmental periods may induce specific phenotypes through differential epigenetic regulation (Dinan et al., 2010). However, given the limited number of studies on FD (i = 2), these differences warrant further investigation.
For IBD subtypes, the available evidence was very limited, with only two effect sizes available for each comparison (K = 2). No statistically significant associations were observed between childhood abuse and CD (physical abuse: OR = 1.06, 95% CI [.62, 1.80]; sexual abuse: OR = .97, 95% CI [.52, 1.80]) or UC (physical abuse: OR = 1.27, 95% CI [.77, 2.11]; sexual abuse: OR = 1.38, 95% CI [.84, 2.27]). Given the small number of effect sizes and the wide confidence intervals, these null findings should be interpreted with caution. Although UC and CD show significant differences in clinical manifestations, lesion distribution, and histological features, they share a series of similar underlying pathological bases. Studies have shown that both have genetic susceptibility and exhibit characteristics such as intestinal flora imbalance (Kaser et al., 2010; Pittayanon et al., 2020; Wang et al., 2024).
Through a comprehensive literature search and appropriate handling of independent effect sizes using a three-level model, this study provided more accurate estimates. The results confirming the extensive association between IBS and various types of abuse support and extend the model proposed by Drossman (2006). However, the findings regarding the differences in IBD subtypes diverge from some individual studies. This could be attributed to the enhanced statistical power achieved through meta-analysis, which accounted for the dependence of multiple effect sizes within each study, thereby revealing more clearly the potential patterns of differences. The lack of a significant association with FD suggests that future research should carefully define the FD phenotype and consider other potential confounding factors. This study also detected a high degree of heterogeneity, which is common in meta-analyses of observational studies involving diverse research designs, populations, and measurement tools for exposure and outcomes. Variance component estimation showed that inter-study variation was greater than intra-study variation, primarily because of differences in population characteristics, abuse assessment tools, and diagnostic criteria for intestinal diseases across studies, as well as factors such as self-reports versus medical records. Although an exploratory analysis of all potential sources of heterogeneity was not conducted, the investigation of heterogeneity by research methods, publication years, and countries explained 57.4% of the variance. The predefined moderation analysis was statistically significant, confirming that the heterogeneity of diseases and abuse types is a key factor in explaining the variation in overall effects and highlighting the need for detailed analyses in future studies.
In previous studies, childhood experiences may have been excluded from the mainstream of adult disease research because of concerns about retrospective memory bias, difficulties in causal inference, and other reasons. In clinical practice, for a long time, mainstream medicine has reduced all disease phenomena to the physical level for research and treatment, while neglecting the psychological conditions of patients. The findings of this study highlight the importance of inquiring about CM history during clinical assessments and the management of intestinal diseases, particularly in patients with IBS. This result helps to eliminate the residual derogatory attitude of doctors toward IBS patients as “hysterical” patients. It may also inform the development of comprehensive intervention strategies that integrate psychotherapy with conventional treatments for intestinal diseases, ultimately improving clinical outcomes. From a public health perspective, preventing and intervening in childhood abuse should be viewed as a long-term, essential strategy for reducing the burden of intestinal diseases in the population.
This study has several limitations. First, most of the included studies were cross-sectional or case-control designs, which do not establish causal relationships between childhood abuse and intestinal diseases. Although plausible biological mechanisms exist, reverse causality or common genetic or environmental factors may partially account for the observed associations. Second, abuse experiences were primarily based on retrospective self-reports in adulthood, which may be influenced by memory biases, current psychological states, or feelings of shame. Third, the occurrence of childhood abuse during different growth and development stages may have different effects. Moreover, previous studies have shown that the more times of abuse experienced during childhood have a greater impact on physical health in adulthood. In this study, the period and frequency of childhood abuse were not considered. Fourth, despite conducting subgroup analyses, some subgroups had relatively small sample sizes, potentially affecting the stability of the estimates. Finally, a detailed analysis of potential moderating variables (such as gender, age at the time of abuse, and abuse severity) was not performed, although these factors could modify the observed associations.
Implications for Research, Practice, and Policy
The implications of this review are significant for future research, clinical practice, and public policy. First, future studies should aim to elucidate the biobehavioral mechanisms underlying the association between CM and intestinal diseases, particularly focusing on the mediating or moderating roles of lifestyle factors, HPA axis dysregulation, elevated systemic inflammation, and alterations in gut microbiome–brain axis communication. Second, prospective longitudinal studies with adequate follow-up durations are necessary to establish temporal precedence and clarify potential causal pathways linking specific types of CM to distinct intestinal disorders (e.g., IBS, IBD, and FD). Third, researchers should systematically explore whether different forms of maltreatment (e.g., emotional neglect, physical abuse, and sexual abuse) have differential associations with various intestinal disease subtypes and investigate the distinct pathophysiological mechanisms that may underlie these associations. Fourth, future research could investigate protective factors, such as social support, psychological resilience, and early interventions, which may mitigate the long-term negative effects of CM on intestinal health. Fifth, future research should more fully consider the developmental stage at which CM occurs and further explore its differential adverse effects across stages. Finally, studies should aim to include more diverse and representative samples, encompassing clinical populations, socioeconomically disadvantaged groups, and individuals from different cultural backgrounds, to enhance the generalizability and translational value of the findings.
The findings of this study highlight several important considerations for clinical practice. Healthcare professionals managing patients with recurrent or refractory intestinal symptoms should consider routinely screening for a history of childhood adversity as a significant psychosocial factor. For patients with intestinal disorders and a history of maltreatment, an integrated care approach is recommended, combining standard intestinal treatments with trauma-informed care principles and appropriate psychological interventions (e.g., trauma-focused cognitive behavioral therapy and emotion regulation training). Pediatricians, primary care providers, and mental health professionals should enhance their capacity to identify and intervene early in cases of child maltreatment, mitigating its long-term physical and psychological impacts through multidisciplinary collaboration. Ongoing education for healthcare providers is essential to raise awareness of the link between childhood trauma and psychosomatic disorders and to promote trauma-sensitive clinical protocols, which can foster patient trust and improve treatment adherence.
From a public health and social policy standpoint, this review supports several recommendations. Governments should strengthen child protection and family support systems, improving mechanisms for preventing, monitoring, reporting, and intervening in child maltreatment to reduce its prevalence at the source. Childhood trauma should be recognized as a major social determinant of health and integrated into national chronic disease prevention strategies and mental health promotion initiatives, advocating for evidence-based primary prevention. Healthcare systems should encourage the adoption of trauma-informed care models, supported by policies and adequate resource allocation. Finally, establishing cross-sectoral collaborative networks is critical for integrating resources from healthcare, mental health, social services, education, and justice systems. This collaboration would provide continuous and comprehensive support services for individuals affected by maltreatment, ultimately reducing the long-term health burden.
Conclusion
In conclusion, this meta-analysis highlights that childhood abuse is generally associated with an increased risk of intestinal diseases in adulthood, with the association being specific to both disease subtypes and types of abuse. All types of abuse are generally associated with an increased risk of IBS, while FD and IBD do not show a significant association with specific types of abuse. These findings support incorporating early-life stress into the biopsychosocial model of intestinal diseases. Future research should focus on prospective cohort studies to establish causal relationships, employ more objective or multisource trauma assessment methods, and explore the biological mediating mechanisms involved. Clinically, IBS patients should be considered for routine screening for any adverse childhood experiences. For patients with intestinal diseases and a history of abuse, a comprehensive treatment approach should be recommended, combining conventional intestinal therapy with trauma-informed care principles and appropriate psychological intervention. In addition, developing and evaluating integrated psychophysiological interventions for patients with intestinal diseases and a history of childhood trauma will be a valuable direction for future research, with substantial clinical implications.
Supplemental Material
sj-docx-1-tva-10.1177_15248380261460029 – Supplemental material for The Association Between Childhood Maltreatment and Adult Intestinal Disorders: A Three-Level Meta-Analysis
Supplemental material, sj-docx-1-tva-10.1177_15248380261460029 for The Association Between Childhood Maltreatment and Adult Intestinal Disorders: A Three-Level Meta-Analysis by Han Ding, Shuying Chen, Faliang Xie, Chen Cao, Weizhen Sheng, Lincheng Guo, Gengfu Wang and Puyu Su in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-2-tva-10.1177_15248380261460029 – Supplemental material for The Association Between Childhood Maltreatment and Adult Intestinal Disorders: A Three-Level Meta-Analysis
Supplemental material, sj-docx-2-tva-10.1177_15248380261460029 for The Association Between Childhood Maltreatment and Adult Intestinal Disorders: A Three-Level Meta-Analysis by Han Ding, Shuying Chen, Faliang Xie, Chen Cao, Weizhen Sheng, Lincheng Guo, Gengfu Wang and Puyu Su in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-3-tva-10.1177_15248380261460029 – Supplemental material for The Association Between Childhood Maltreatment and Adult Intestinal Disorders: A Three-Level Meta-Analysis
Supplemental material, sj-docx-3-tva-10.1177_15248380261460029 for The Association Between Childhood Maltreatment and Adult Intestinal Disorders: A Three-Level Meta-Analysis by Han Ding, Shuying Chen, Faliang Xie, Chen Cao, Weizhen Sheng, Lincheng Guo, Gengfu Wang and Puyu Su in Trauma, Violence, & Abuse
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the National Natural Science Foundation of China (Nos. 82473655, 82204071).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.