
Abstract
There has been significant progress in studying gender-based violence (GBV) and precarious employment independently, yet there is a paucity of research on their intersection and the health impacts. The objective of this secondary analysis of a scoping review is to synthesize existing literature on this intersection and the associated health impacts among migrant women. Seven databases were searched for peer-reviewed articles in May 2024, with an updated search in May 2025. This secondary analysis was built on all the inclusion and exclusion criteria in the original scoping review, which focused on empirical studies including migrant women, aged 15 years and older, who self-report experiences of GBV and engagement in precarious employment. A total of 28 studies were included for analysis. Findings revealed the significant impact of the intersection of GBV and precarious employment on the health and well-being of migrant women. Unsafe working conditions and psychosocial stressors were found to be significantly associated with heightened risks of mental distress, physical injuries, musculoskeletal disorders, and barriers to accessing healthcare services. Community networks offered support but were often ineffective for women living with their employers. This review highlighted the urgent gaps in research, policy, and workplace protections that impact the health and well-being of migrant women. Addressing these issues to achieve health equity remains a priority.
Keywords
Introduction
Gender-based violence (GBV) is a widespread issue that significantly impacts the health and well-being of women, especially those from marginalized communities (Klugman, 2017; Sabri & Granger, 2018). Approximately one in three women worldwide has been subjected to GBV in her lifetime (Klugman, 2017). Research indicates that GBV not only causes immediate health problems but also contributes to long-term health issues, including non-communicable diseases (Sabri & Granger, 2018). In the context of migration, GBV is of concern to women, who face increased vulnerabilities stemming from intersecting structural and systemic inequalities, such as immigration status, education, gender, and race, which, in turn, may limit migrant women’s access to services, information, work, and education opportunities (Bellizzi & Molek, 2022; Tan & Kuschminder, 2022).
Employment is regarded as an important social determinant of health, considering that work influences many aspects of human life that affect health, including income, healthcare access, housing, financial security, and social status (H. Lai et al., 2022; World Health Organization, 2017). For migrant women, especially those going through the initial resettlement period, work is fundamental in establishing an economic foundation, providing economic independence, enhancing social integration, and fostering personal growth (H. Lai et al., 2022; Refugee Council of Australia, 2010). The type of work that migrant women have access to matters, as it influences the extent to which they can gain economic independence and integrate into their new environments. Previous studies have revealed that migrant women often face difficulties in entering the labor market due to various factors, which include discrimination, lack of local work experience and referees, limited knowledge of the local labor market, and language barriers (Al-Hamad et al., 2024; Bar-Haim & Birgier, 2024; Refugee Council of Australia, 2010; Shinam & Pandey, 2026). As a result, migrant women often encounter precarious employment opportunities during their settlement in host countries, characterized by job insecurity, unpredictable schedules, long working hours, excessive workloads, limited or no workplace protections, and low wages (International Labour Organization [ILO], 2012; Premji et al., 2014), which may increase their vulnerability to abuse and exploitation, resulting in poor health outcomes.
Both GBV and precarious employment, as standalone factors, exert significant detrimental effects on the health and well-being of migrant women (Bhattacharya & Ray, 2021; Perri et al., 2024; Tastsoglou, 2025; World Health Organization, 2017). Experiencing GBV while engaged in precarious employment creates a compounded vulnerability for migrant women, which can lead to poor health outcomes (Premji, 2018). Similarly, navigating unsafe work environments coupled with trauma of abuse can lead to mental and physical health problems (MacGregor et al., 2021). Furthermore, the unstable working environments with no workplace protections, benefits, and labor rights can often prevent women from seeking care and support from formal service providers (Premji, 2018; Premji et al., 2014).
Importantly, the intersection of GBV and precarious employment not only deepens social and economic marginalization but also reinforces health inequities. Globally, migration has become a central issue in public health discourse, and governments are being challenged to integrate the health needs of migrants into policies and intervention programs (Manji et al., 2023; World Health Organization, 2017). Approximately one in seven people globally identify as migrants (nearly 1 billion individuals), and women comprise about 48% of international migrants (McAuliffe & Oucho, 2024; World Health Organization, 2017). According to the International Organization for Migration, female international migrants constitute 135 million of the total population of international migrants (McAuliffe & Oucho, 2024). Although they may be more male international migrants than female globally (McAuliffe & Oucho, 2024), the International Labour Organization (ILO) report that many of international migrant women struggle to get high-skilled jobs, regardless of their education and work experience and often end up working in low-skilled jobs, predominantly in female dominated sectors such as health and social care (Rakotonarivo, 2020; World Health Organization, 2017). The heavy concentration of women in these occupations is rooted in patriarchal ideologies and is seen as a natural extension of women’s traditional gender roles, and this type of work is typically undervalued, undercompensated, and poses risks to abuse and exploitation (Rakotonarivo, 2020; Yilmaz & Ledwith, 2017).
As part of the United Nations (UN) Agenda, achieving good health, decent work, and gender equality for all requires addressing the structural and socio-cultural forces that perpetuate inequality and violence (Holliday et al., 2019). In the context of GBV and precarious employment among migrant women, Holliday et al. (2019) highlight the centrality of feminized precarious work, particularly domestic and care work, as a site of compounded vulnerability. They argue that meaningful progress toward the UN Sustainable Development Goals (SDGs) demands critical conversations that reveal the intersecting systems of gender, labor, and migration that sustain these inequalities. Without addressing the interconnections between gender equality, labor, migration, and sustainable development, the realization of Agenda 2030 remains uncertain (Holliday et al., 2019). Thus, given the vulnerabilities faced by migrant women, there remains a gap in understanding how the intersection of GBV and precarious employment impacts their health and well-being. Addressing this gap is crucial for informing equitable health interventions and policy responses that reflect the diverse needs and experiences of migrant women.
This secondary analysis builds upon a recent scoping review that examined the intersection of precarious employment and GBV among migrant women. In this secondary analysis, we delved into a distinct dimension of the data and focused specifically on synthesizing the evidence related to how the intersection of GBV and precarious employment influences health outcomes for migrant women. Our secondary analysis was guided by the research question: What are the health impacts described at the interconnections of GBV and precarious employment for migrant women? Examining the health impacts of this intersection contributes to global efforts to achieve the SDGs #3 (good health and well-being, #5 (gender equality), and #8 (decent work and economic growth) by generating evidence that can inform inclusive policies that advance migrant women’s health and well-being.
Methods
Our initial scoping review was conducted in accordance with Arksey and O’Malley (Arksey & O’Malley, 2005) scoping review methods and the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR; Tricco et al., 2018) and was registered on Figshare (Chadambuka et al., 2024). This secondary analysis was initiated following the completion of the initial scoping review (Chadambuka et al., 2025), which revealed that focusing solely on the intersection of GBV and precarious employment may not provide a comprehensive understanding of women’s experiences. This underscored the importance of examining health impacts associated with this intersection to enable a more holistic and nuanced account of the women’s lived realities.
Theoretical Frameworks
Intersectionality
Like the initial scoping review, this secondary analysis was guided by the intersectionality theory to critically examine the health impacts of the intersection of GBV and precarious employment (Crenshaw, 1991; Shannon et al., 2022). As highlighted in previous studies, migrant women face structural barriers that not only increase their exposure to exploitation and GBV but also negatively impact their health and well-being and limit their ability to seek care and support (Ahmadzai et al., 2016; Fonteyne et al., 2024; Holtmann & Rickards, 2018). Through the adoption of an intersectional lens, we were able to explore how the interlocking systems of oppression, such as gender, immigration status, and class, shaped individual experiences of violence, work precarity, and exposure to health problems, including access to care. By accounting for these intersecting factors, our review moved beyond one-dimensional analyses to capture the vulnerability and health outcomes experienced by migrant women in precarious employment and at the risk of GBV.
World Health Organization Healthy Workplace Model
The World Health Organization (WHO) Healthy Workplace Model underscores the dynamic interaction between work environment and human factors, illustrating how a negative interaction between occupational conditions and human factors can pose risks to mental and physical health (World Health Organization, 2010; World Health Organization & Burton, 2010). This model consists of four overlapping elements in which actions toward achieving healthy workers and workplaces can be taken; (i) physical environment (affecting physical safety, health and mental well-being); (ii) psychosocial work environment (organization cultures including harassment, gender discrimination, racism, which affects mental health); (iii) personal health resources in workplaces (employment conditions making it difficult to maintain lifestyle); and (iv) enterprise community involvement (activities for health and well-being in communities; World Health Organization, 2010). Thus, as work is increasingly being recognized as either a place of safety or risk for women (Scott, 2023), this framework illuminates how precarious employment conditions and experiences of abuse intersect to shape migrant women’s health outcomes and their ability to access care and support systems.
Evidence on the use of the WHO Healthy Workplace Model in precarious employment contexts, particularly among migrant workers, is limited, with existing studies largely focused on formal employment settings (World Health Organization & Burton, 2010). However, the need to apply this kind of model in precarious employment studies is increasingly being recognized. For example, a systematic review focusing on examining initiatives to address precarious employment and its effects on workers’ health and well-being highlights the lack of structured frameworks in addressing the impacts of precarious work environments- underscoring a gap that the WHO Healthy Workplace model can fill (Gunn et al., 2021). The comprehensive nature of this model in addressing physical, psychosocial, and organizational determinants of workers’ health makes it suitable for this secondary analysis.
Information Sources and Search Strategies
In the initial scoping review, with the help of a professional health sciences librarian, an initial search strategy was developed in Medline, which was modified and adapted for other databases (See Appendix A in Supplemental Material). The search strategy included text words and subject headings related to GBV in its various forms, precarious employment in its various dimensions, and migrant women (both documented and undocumented). Searches for relevant literature were conducted in May 2024 and updated in May 2025 across seven electronic databases: Medline, Scopus, PsycInfo, Embase, Web of Science, Econlit, and CINAHL. For this secondary analysis, no new search strategy was developed, and no new literature search was conducted. We screened the full set of studies included in the updated 2025 review to identify those that reported health-related outcomes of the intersection of GBV and precarious employment.
Similar to the initial scoping review, we adopted the UN definition of GBV, as articulated by the Committee on the Elimination of Discrimination Against Women, which encompasses any behavior likely to cause physical, sexual, or psychological harm or suffering to women, such as threats, coercion, or deprivation of liberty in both public and private settings (United Nations, 1993). In this review, GBV encompassed both intimate partner and non-partner violence, including sexual and psychological abuse, occurring privately or publicly, including in the workplace by either employers, supervisors, or co-workers, or by non-employers, including intimate partners, where GBV risk and experiences intersect with precarious employment to shape health outcomes. In line with our adopted definition of GBV, our scope included workplace violence or harassment when these behaviors were framed by the authors as gendered and disproportionately affecting migrant women in precarious work. For studies that used a broad workplace construct, we considered elements that aligned with our adopted definition of GBV. Forms of workplace violence that were not gender related (e.g., incidents motivated by theft or other non-gendered acts) fell outside the scope of GBV as understood in this review.
Precarious employment, as broadly understood, is work characterized by uncertainty, insecurity, low and unstable pay, lack or limited control over working conditions, inadequate legal or workplace protection, and schedule unpredictability (ILO, 2012, 2017). Similar to the initial review, international migrants are defined as individuals who are resident, legally or illegally, in a country other than their country of birth (United Nations, Department of Economic and Social Affairs, Population Division, 2016). We focused on both racialized and non-racialized migrant women to capture the breadth of experiences across diverse geographical, cultural, and socio-economic contexts.
Eligibility Criteria
Our inclusion and exclusion criteria were based on the original criteria of the initial scoping review (Chadambuka et al., 2025) and were adopted to answer the secondary analysis research question as described below.
Studies focused on individuals who self-identify as migrant women (including transgender women) who are 15 years and above and self-report GBV experiences and engagement in precarious employment. The age limit of 15 years was selected considering that the ILO defines 15 years as the working age (ILO, n.d.). In addition, the age limit of 15 years was included to accommodate studies that would have been conducted in contexts where early marriages and intimate partner violence (IPV) are prevalent (Ellsberg & Heise, 2005). Studies that did not specify the age of the women but indicated that the sample included adult women were included in the study.
Studies that report on the health impacts on migrant women at the intersection of GBV and precarious employment. Studies that only focused on describing the intersection of GBV or precarious employment without a discussion on how this intersection impacts the health and well-being of migrant women were excluded from the secondary analysis.
Peer-reviewed primary studies with a quantitative, qualitative, or mixed methods design with full text available were included. We excluded book chapters, narrative reviews, systematic reviews, conference abstracts, and dissertations.
Screening/Study Selection Process
For the initial review, four reviewers independently conducted title/abstract and full-text screening, and any disagreements were resolved through discussion among the researchers. In this secondary analysis, an additional criterion was applied to identify the relevant studies that discussed any health impacts on migrant women. Three reviewers (CC, PKN and RR) independently reviewed the “Results” sections of 50 included studies from the initial scoping review and considered whether any of the studies reported on the health impacts of the intersection of GBV and precarious employment among migrant women. Disagreements were resolved transparently through consultation among the reviewers.
Data Extraction
A data extraction tool developed in Covidence in the initial scoping review was used to capture the specific data and was piloted by two independent reviewers involved in the title/abstract and full-text screening, and adjusted as needed. Two independent reviewers (CC and RR) abstracted data on the health impacts reported in the studies, and this served as the primary data for analysis. All abstracted data were verified by another independent reviewer (PKN).
Data Analysis
We analyzed data with a focus on the health impacts at the intersection of GBV and precarious employment using a qualitative approach and guided by the intersectionality theory and the WHO Healthy Workplace Model. In our analysis, we treated the author-reported findings as the primary data. We extracted material from the “Results/Findings” section and conducted an interpretive analysis of the authors’ findings, in line with our research question. The analytic process included reviewing the extracted findings relevant to the health impacts of GBV and precarious employment; inductively grouping similar findings across studies into preliminary categories and refining these categories into thematic domains; and identifying cross-cutting patterns and divergences in the health impacts of GBV and precarious employment among migrant women.
An intersectional lens was used to better understand how precarious employment and GBV interact with socio-structural conditions to produce differential health impacts among migrant women. Adopting this intersectional lens allowed a more holistic understanding of how structural inequalities mediate the relationship between work, violence, and health.
The WHO Healthy Workplace Model guided the synthesis of findings across the included studies. This framework enabled a structured analysis of how the intersection of precarious employment and GBV is associated with health outcomes within the model’s four key domains: the physical work environment, the psychosocial work environment, personal health resources, and enterprise community involvement. By integrating an intersectionality lens, we further examined how these interrelated experiences-shaped by gender, migration status, race, and class-produced layered health impacts for migrant women. This combined approach allowed us to attend to both individual-level and structural drivers of harm, offering a more nuanced understanding of how precarious employment and GBV jointly shape health inequities.
Results
Characteristics of Included Studies
In total, 28 articles reporting on the health impacts of the intersection of precarious employment and GBV among migrant women were included in this review. For a summary of the article selection process, beginning with the initial scoping review, including the updated search, see Figure 1. Most of the studies were conducted using qualitative methods (75%), with a few using quantitative (21%) and mixed methods (4%). Although studies included in this secondary analysis covered a range of employment categories, the majority of studies exclusively discussed health impacts of domestic workers (46%), with a few also reporting on care workers (14%); and very few studies discussed domestic workers’ and care workers’ experiences collectively (7%). Few studies specifically reported on other employment categories, such as garment workers, farmworkers, and housekeepers (14%), while one study discussed the health impacts of domestic workers and janitorial workers together. A few studies (14%) either reported on informal work or did not specify the employment categories; however, the highlighted elements of the jobs aligned with our adopted definition of precarious employment. Most studies reported on both physical and mental health impacts (75%), with a few discussing the sexual and reproductive health impacts (17%) of GBV and precarious employment. Few studies discussed women’s experiences of accessing healthcare services (46%) as well as the contribution of informal support networks in the healing and recovery process (33%). Few of the included studies reported on the migration status of women (21%), while the majority of the studies (63%) vaguely described or did not report the documentation status of women. Very few studies included and explicitly described both documented and undocumented women (16%). See Appendix B in Supplemental Material.
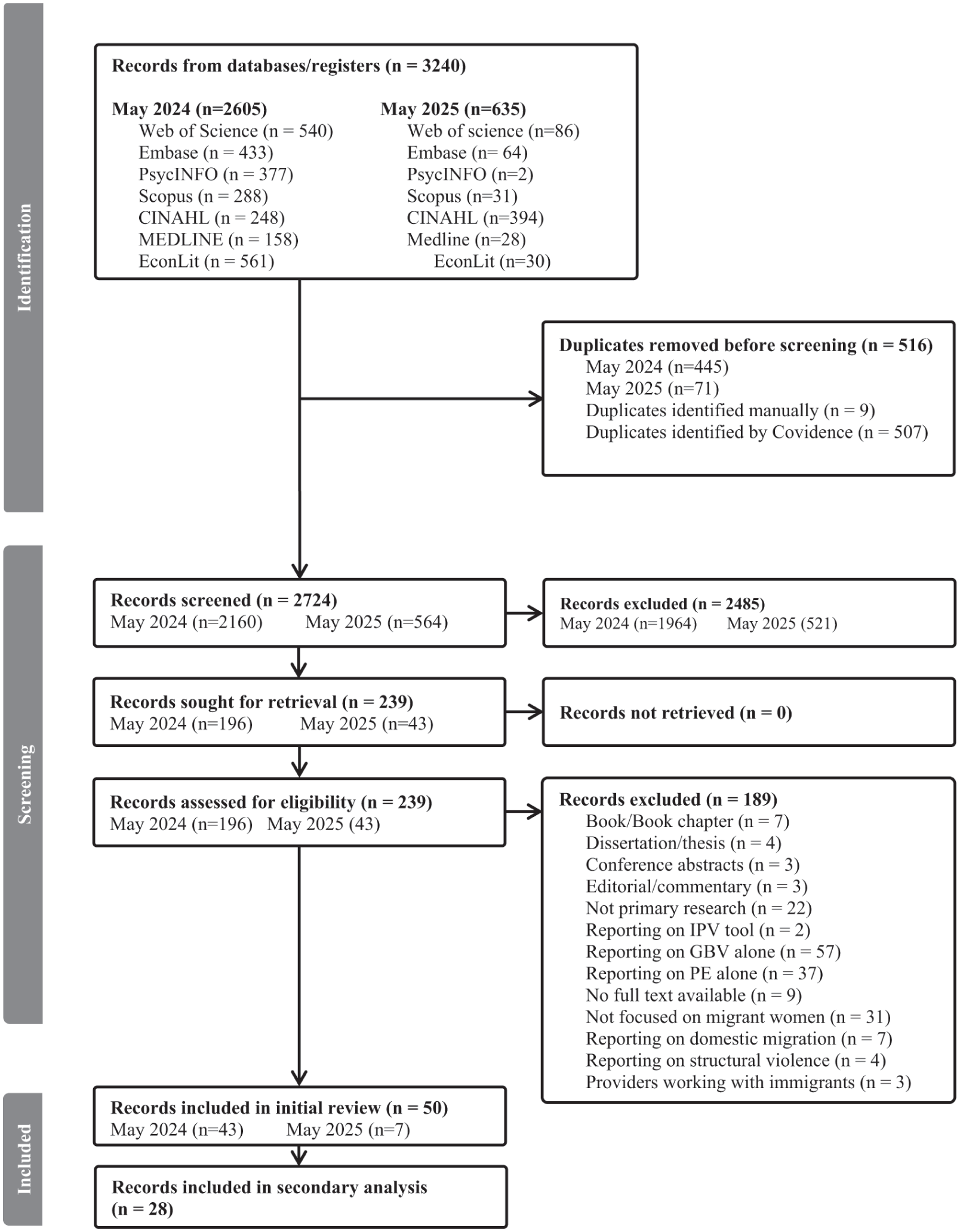
PRISMA flow diagram of the study selection process.
This review revealed the multifaceted health consequences arising from the intersection of GBV and precarious employment. The terminology that is used for our emergent issues (Table 1) reflects the language and key issues that are emphasized in the literature, and this allowed us to capture migrant women’s lived experiences as described in the included studies. Furthermore, the included studies varied in design and terminology, yet collectively documented how GBV intersected with precarious employment to shape health outcomes across intimate and workplace contexts. Anchored in an intersectional lens, our analysis highlights how the interplay of key identity markers, particularly immigration or legal status, gender, and ethnicity, shapes migrant women’s vulnerability and their access to support services. The following section summarizes the central issues that emerged from this secondary analysis.
Overview of Health Impacts Linked to the Intersection of GBV and Precarious Employment.
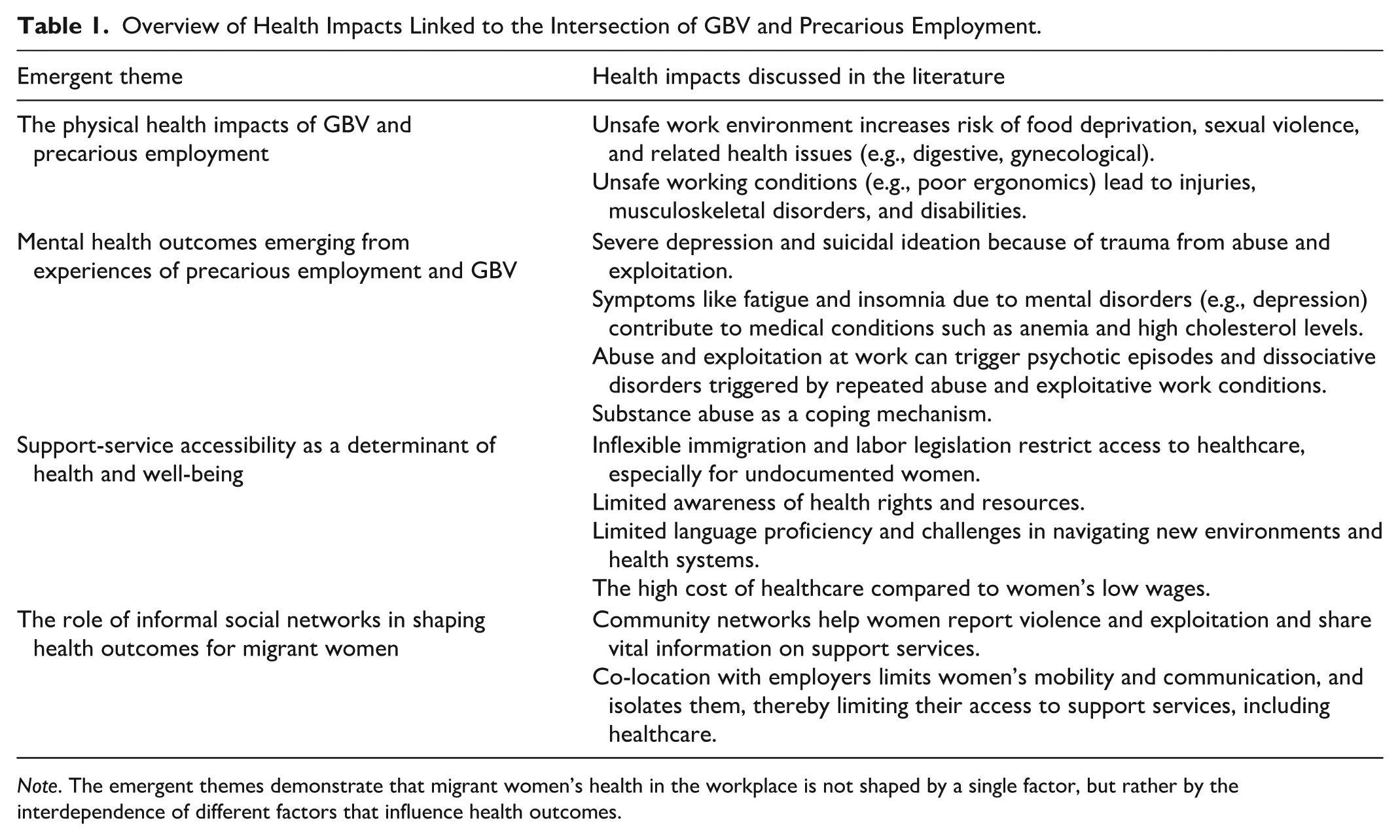
Note. The emergent themes demonstrate that migrant women’s health in the workplace is not shaped by a single factor, but rather by the interdependence of different factors that influence health outcomes.
Narrative Synthesis of Key Findings
The Physical Health Impacts of GBV and Precarious Employment
Several studies linked health risks at the intersection of GBV and precarious employment among migrant women to unsafe physical work environments, thereby contributing to a range of physical health issues, including diagnosed illnesses, injuries, and musculoskeletal disorders (Ayalon & Ayalon, 2012; Bevilacqua et al., 2023; Chung & Mak, 2020; Covington-Ward, 2021; Mahdavi, 2013; Reda, 2015; Rocha et al., 2022; Serrano & Martin, 2022; Vasil, 2023). The health risks are severe for women who are co-located with their employers in the same work environment (e.g., domestic workers and care workers), with such boundaries leaving the boundary between personal life and work blurred, leading to abuse and exploitation (Diab et al., 2022; Ladegaard, 2025; Y. Lai & Fong, 2020; Wickramage et al., 2017).
Across several studies conducted with care and domestic workers, heavy lifting, exhaustion due to long working hours, and repeated abuse led to severe work-related injuries and attempts to escape the exploitative and abusive work environment, with some women jumping out of windows from top-floor rooms, sometimes resulting in permanent disability or death (Anbesse et al., 2009; Ayalon & Ayalon, 2009; Mahdavi, 2013; Rocha et al., 2022; Wickramage et al., 2017). In a study conducted in the United States, care workers experienced fatigue, physical exhaustion, and back injuries due to long working hours (150 or more hours every 2 weeks) and heavy workloads, which involved attending to more than a dozen patients during each shift and included heavy lifting of patients (Covington-Ward, 2021). Similarly, women working in garment factories who experienced repeated physical violence sustained injuries commonly located on the upper limbs, head, and neck (Wickramage et al., 2017). For some women, partner financial sabotage and abuse due to gender role shifts often forced them to take on even more precarious jobs with long working hours and schedule unpredictability to meet living costs, leading to severe back and neck pains (Vasil, 2023).
Among several studies, poor ergonomic conditions (e.g., prolonged standing, heavy lifting, repetitive muscle strains), particularly in domestic, care, and hospitality work settings, resulted in women frequently experiencing back and joint pain, musculoskeletal injuries, and strains (Chung & Mak, 2020; Rocha et al., 2022). For instance, a study conducted in the United States revealed that women working as hotel housekeepers experience high rates of musculoskeletal disorders and occupational injuries among hotel employees (Hsieh et al., 2017). These health problems are directly linked to abusive work environments and unsafe work conditions characterized by weak workplace protections, rooted in gender power imbalances in these high-risk work sectors, that do not prioritize occupational health and safety measures, which expose women to physical and psychosocial hazards leading to poor physical health outcomes (Hsieh et al., 2017).
While physical hazards in precarious employment are frequently emphasized in the literature as primary determinants of physical health outcomes, it is equally critical to consider how these risks intersect with psychosocial stressors such as discrimination, harassment, and abuse, which can exacerbate physical health impact. These nonphysical hazards can lead to distractions, poor coordination, and errors in judgment, ultimately resulting in severe injuries and strain. For instance, in a study conducted in Hong Kong with domestic workers, repeated verbal abuse and harassment from employers and their family members led to fatigue and exhaustion, which made it difficult to concentrate and resulted in physical health problems, including neck and shoulder pains (Chung & Mak, 2020; Ladegaard, 2025). This overlap of the physical and psychosocial environment intensifies the burden on women’s health and well-being.
In addition, food insecurity emerged as both a consequence of exploitative labor conditions and a key contributor to poor physical health outcomes with mistreatment by employers and low wages making it hard for women, to access sufficient and nutritious food, which undermined their physical health (Bhuyan et al., 2018; Chan & Trahms, 2023; Fuentes-Pumarola et al., 2025; Kodoth, 2016; Y. Lai & Fong, 2020; Pan & Yang, 2012; Serrano & Martin, 2022; Trần, 2023; Wickramage et al., 2017; Zahreddine et al., 2014). Across several studies, migrant live-in domestic and care workers reported receiving inadequate and unsuitable food, noting that employers deliberately limited their access to food, sometimes as a form of punishment, forcing some to resort to eating from wastebaskets (Anbesse et al., 2009; Ayalon & Ayalon, 2009; Pan & Yang, 2012; Wickramage et al., 2017). In another study, migrant domestic workers in Saudi Arabia, women were deprived of food after working more than 15 hours, and ended up eating stale and rotten food (Trần, 2023). These instances of food deprivation resulted in migrant domestic workers being underweight and malnourished, with some women suffering from gastrointestinal problems and digestive illnesses (Serrano & Martin, 2022; Trần, 2023; Wickramage et al., 2017; Zahreddine et al., 2014).
A few studies also highlight that the intersection of sexual and reproductive health outcomes is shaped by the interplay of the physical and the psychosocial work environment. Workplace factors such as gender-based discrimination, power imbalances, and the absence of workplace protections, particularly in settings where women live with their employers, increase vulnerability to sexual violence, leading to gynecological problems, including sexually transmitted infections (Ayalon & Ayalon, 2009; Diab et al., 2022; Serrano & Martin, 2022). For instance, a study involving live-in migrant domestic workers in Hong Kong found that unsafe working conditions, combined with psychosocial stressors such as fear of job loss and deportation, limited women’s ability to exercise bodily autonomy and created environments where some women experienced severe violations of their rights, including rape by their employers (Ladegaard, 2025). In a study conducted with service providers working with live-in care workers in Israel, women would complain that they had been raped by family members of the care recipient and become pregnant (Ayalon & Ayalon, 2009). However, these women were subsequently threatened with termination of employment and deportation if they did not abort the baby, forcing them into unsafe abortions (Ayalon & Ayalon, 2009). In another study conducted with domestic workers in Lebanon who were sexually abused by their employers, or relatives and friends, irregular menstruation, sexually transmitted infections, and bruises, cuts, and tears to their vaginal area were reported as the common sexual and reproductive health problems experienced due to sexual abuse (Diab et al., 2022).
Mental Health Outcomes Emerging From Experiences of Precarious Employment and GBV
The mental health impacts (emotional and psychological consequences that disrupt emotional well-being and functioning) of the interconnectedness of precarious employment and GBV among migrant women were discussed in several studies (Ayalon & Ayalon, 2012; Chung & Mak, 2020; Kim et al., 2016; Reda, 2015; Rocha et al., 2022; Serrano & Martin, 2022; Zahreddine et al., 2014). These mental health impacts are largely linked to unsupportive psychosocial work environments characterized by limited support, work-life imbalance, mostly due to long working hours, schedule unpredictability, and workplace harassment and discrimination.
Notably, there is a complex interplay between mental health conditions and somatic symptoms, which often co-occur in the context of GBV and precarious employment. Across several studies, mental health issues such as depression, anxiety, and chronic stress were found to contribute to physical symptoms, including insomnia, persistent fatigue, and migraines (Anbesse et al., 2009; Ayalon & Ayalon, 2009; Chan & Trahms, 2023; Chung & Mak, 2020; Diab et al., 2022). These, in turn, were associated with medical conditions such as anemia and elevated cholesterol levels, illustrating the cumulative and interconnected nature of psychosocial and physiological health outcomes at the intersection of precarious employment and GBV.
Among domestic and care workers, exposure to unsafe working environments and the trauma of verbal, sexual, and physical abuse led to severe forms of depression, which led to suicidal ideations (Ladegaard, 2025; Rocha et al., 2022; Wickramage et al., 2017). A study conducted in Israel among live-in care workers revealed that the trauma of abuse and hazardous working conditions led to severe emotional distress, with some women experiencing deep hopelessness and engaging in suicidal thoughts and behaviors (Ayalon & Ayalon, 2012). Likewise, in a study with live-in domestic workers in China, the trauma experienced as a result of sexual violence led to suicide attempts among women (Ladegaard, 2025). Furthermore, work-life imbalance also emerged as a contributing factor to mental health challenges, particularly when women were unable to maintain a clear boundary between their professional responsibilities and personal lives (Kim et al., 2016; Y. Lai & Fong, 2020). For instance, a study conducted in the United States with Mexican female migrant farmworkers highlighted how the struggle to balance work and caregiving responsibilities led to chronic stress, post-harassment trauma, and depression (Kim et al., 2016).
For domestic workers, the exposure to poor living conditions in the homes they worked, the long working hours, and excessive workloads, along with the abuse, led to psychotic episodes, histrionic personality, dissociative disorders and tragic incidents of suicide by hanging or jumping from top floors (Ayalon & Ayalon, 2012; Trần, 2023; Wickramage et al., 2017; Zahreddine et al., 2014). In a study conducted with domestic workers in Hong Kong and Chile, unsatisfactory, poor living and working conditions, such as sleeping on the floor in corridors and kitchens, negatively impacted their mental well-being (Chan & Trahms, 2023; Cheung et al., 2019). For some women, the disconnect between their cultural beliefs and certain job responsibilities led to significant emotional strain, contributing to stress and, in some cases, depression. For example, a study involving domestic workers in Chile revealed that certain job tasks, such as removing a male employer’s jacket upon his arrival, were perceived as culturally intimate acts traditionally reserved for a spouse (Chan & Trahms, 2023). When combined with experiences of emotional and sexual abuse, these tasks contributed to significant psychological distress among the women, manifesting as fatigue and migraines (Chan & Trahms, 2023). In some instances, the accumulation of mental health challenges forced women to adopt harmful coping mechanisms, particularly when efforts to escape abusive and exploitative conditions proved unsuccessful. For example, to deal with the stress and depression that came with the abuse and exploitation, some domestic workers in Lebanon and Hong Kong resorted to substance abuse and excessive alcohol consumption (Diab et al., 2022; Ladegaard, 2025).
Access to Support Services as a Determinant of Health and Well-Being
Limited access to support services emerged across the reviewed literature as a key factor that exacerbates the health impacts associated with the intersection of GBV and precarious employment. Several studies discussed women’s access to support services, particularly healthcare and social services, often linked to the absence of workplace protections, benefits, and immigration policies (Anbesse et al., 2009; Bevilacqua et al., 2023; Diab et al., 2022; Mahdavi, 2013; Robillard et al., 2018; Serrano & Martin, 2022). A study involving migrant platform cleaners in Germany highlighted significant barriers to accessing basic health care, primarily due to the high costs relative to their low wages (Mondon-Navazo & Murgia, 2025). Limited access to health insurance further compounded these challenges, and, in some cases, women were compelled to take on additional precarious jobs that provided public health insurance, enabling them to seek medical care (Mondon-Navazo & Murgia, 2025).
In a study conducted in Taiwan, access to healthcare services for live-in migrant domestic workers was challenging, mostly due to inflexible legislation that limits access to essential healthcare services to migrant women, especially those with tenuous immigration status (Pan & Yang, 2012). In a U.S. study, migrant women farmworkers reported being unable to file complaints or seek support due to threats that disclosing abuse and exploitation would be futile, given the farm’s financial power and access to skilled lawyers, consequently making it hard to seek care and support without risking their jobs (Kim et al., 2016). Notably, some women lacked the resources that allow them to learn about health rights and resources, particularly concerning support services, which consequently made it difficult for them not only to access care and support but also to extricate themselves from the abusive and exploitative situations (Serrano & Martin, 2022). Furthermore, language barriers and challenges in navigating new environments and healthcare systems limited migrant women’s ability to seek care and support, particularly for women working and living in the same environment as their employers (Chan & Trahms, 2023; Mahdavi, 2013; Robillard et al., 2018; Serrano & Martin, 2022).
The disregard of women’s health by employers was also highlighted as a barrier to accessing healthcare services. A study conducted with live-in domestic workers and care workers revealed that women were not allowed to visit doctors for medical care, and instead, they were expected to continue working (Fuentes-Pumarola et al., 2025). Another study conducted in Brazil with migrant women working in a home-based sewing workshop, women suffering from stomach pains linked to severe stress were not allowed by their employers to seek medical care during the week as they were needed at work (Serrano & Martin, 2022).
Notably, the fear of abuse at work or home being discovered or reported, and the fear of losing jobs and income, also posed difficulties in seeking healthcare services for women. In the United States, women feared the potential impacts of seeking healthcare and reporting violence within intimate relationships and workplaces on their employment status, stating that reporting violence and exploitation “was a luxury they did not consider” (Bevilacqua et al., 2023, p. 6).
Social workers working with Filipino live-in migrant care workers in Israel reported that even when migrant women were approached by service providers, communication difficulties and lack of trust (on both sides) hampered their ability to benefit from the services (Ayalon & Ayalon, 2009). Service providers and decision-makers working with caregivers in Canada also highlighted that debt bondage, cultural beliefs around discussing sexual assault, and family pressures (back home) to safeguard the contract by remaining silent were identified as common barriers to accessing care and support (Robillard et al., 2018). However, in the same study, some service providers and decision-makers highlighted the unique barriers faced by service providers in reaching and supporting migrant women. These challenges primarily stem from inefficiencies within the judiciary system, systemic structures that hinder adequate support, particularly when filing complaints, and significant gaps in human and financial resources, with many organizations relying on volunteers and students who lack sufficient training to provide the necessary support to migrant women (Robillard et al., 2018).
The Role of Informal Social Networks in Shaping Health Outcomes for Migrant Women
In a few studies, informal social networks (including community groups, peer connections, and local support structures) emerged as essential mechanisms that promote health and well-being among migrant women navigating the intersecting challenges of GBV and precarious employment. Their presence was shown to foster connection, resource-sharing, and collective resilience, while their absence or disruption heightened vulnerability and compromised both mental and physical health.
Community networks, including friends and religious groups, were essential in providing care and support for women in precarious employment and at the risk of GBV (Anbesse et al., 2009; Bevilacqua et al., 2023; Bhuyan et al., 2018; Chung & Mak, 2020; Kouta et al., 2021). In some studies, social networks were reported to foster a sense of community among workers, enabling them to share experiences, access resources related to their health and well-being (Chung & Mak, 2020). Peer community organizations, friends, and neighbors were reported to facilitate reporting of violence, share information on how to access health and social services, and dispel any misconceptions around reporting any abuse and exploitation (Bevilacqua et al., 2023). In a study conducted with Filipino caregivers in Canada, social media groups, for example, on Facebook, friends and fellow Filipino migrants were reported to be useful to caregivers in dealing with challenges and conflicts, which would have resulted in mental health issues (Bhuyan et al., 2018).
Notably, for some women, restrictions around their mobility and communication isolated them from their social networks and increased their vulnerability to mental health disorders. A study conducted with Ethiopian domestic workers in Middle Eastern countries highlighted how women were disconnected from their Ethiopian ties and communities and were locked inside the compound, which led to depression, loneliness, and chronic stress, and hampered their ability to seek healthcare services (Anbesse et al., 2009). Likewise, in a study conducted with domestic workers from Sri Lanka and the Philippines working in the Republic of Cyprus, women who had not formed any social links with their communities faced significant challenges in dealing with the consequences of sexual abuse (Kouta et al., 2021). In this same study, some of the Filipino migrant women, after being raped, waited outside their employers’ houses in case other Filipino women would pass by and help them with material and informational support on how to access care and support (Kouta et al., 2021). These restrictions limited women’s access to vital social support systems and advocacy networks, which are essential for promoting their health and well-being and linking them with relevant resources.
Discussion
To date, limited research has examined the health impacts arising from the intersection of precarious employment and GBV, particularly among migrant women, regardless of its criticality in achieving SDGs #3 and #8. This study sought to address this critical gap by exploring how the convergence of these two structural conditions shapes health among migrant women. While both precarious employment and GBV independently contribute to poor health among migrant women, we found that the interconnectedness of these conditions intensifies vulnerabilities and increases harm. Furthermore, access to services, although vital, remains largely inaccessible to women, and this further entrenches their vulnerability and hinders opportunities to recovery and healing. Although our data synthesis was guided by the four elements of the WHO Healthy Workplace Model, our findings reinforce the argument made by Burton and colleagues (World Health Organization & Burton, 2010) that the division between these domains is conceptually artificial. In practice, these elements are deeply interrelated, and their influence on health is cumulative and overlapping rather than discrete, particularly in the context of precarious employment and GBV, which is marked by structural vulnerability and exploitation. This highlights the intrinsic interconnectedness of psychological and physical health in the context of GBV and precarious employment, emphasizing that mental health disorders are not isolated from the body but are deeply embodied, with tangible physiological consequences.
Our findings also resonate with previous studies (Jaydarifard et al., 2023), highlighting how the experience of working in unsafe environments and being economically dependent on abusive employers and partners, without legal or institutional protection, leaves women powerless and vulnerable to abuse and exploitation, which contributes to poor health. Our review further revealed how the intersection of precarious employment and GBV contributes to mental and physical health problems, including permanent disabilities due to severe injuries, stress, depression, fatigue, physical health disorders due to food deprivation, muscle strains, suicidal ideations, and, in extreme cases, death. Importantly, there is evidence of manifestations of long-term, repeated exposure to trauma, resulting from the violence and exploitative labor practices, which lead to mental health disorders.
While previous studies (Blindow et al., 2024; Matteo & Scaramuzzino, 2022) have shown that GBV and precarious employment each independently contribute to poor sexual and reproductive health outcomes, their combined impact was seldom addressed in our review. This relative scarcity of evidence may, in part, reflect cultural norms surrounding the disclosure of sexual violence, the impact of trauma on women, as well as coercive control and threats from perpetrators, which can limit both reporting and scholarly inquiry into these experiences.
The intersection of GBV and precarious employment demonstrably creates significant barriers to accessing healthcare services for women experiencing compromised health. Based on our findings, the experiences of migrant women are layered and largely compounded by a lack of knowledge on their rights, and tenuous immigration status, fear of employer retaliation, and deportation, and the weak workplace regulations that provide women with limited to no time to seek medical help when needed. While these barriers are evident in situations involving GBV (Asseervatham et al., 2023; Muuo et al., 2020), the intersection of the two reinforces a silencing effect that places migrant women in a double bind and can exacerbate poorer health outcomes. In some instances, health systems are sites of further exclusion, as this review highlighted how women struggled with navigation and communication when seeking care.
Notably, social isolation and disconnection emerged as a significant determinant of health, compounding the vulnerabilities experienced by women and their health consequences. Our findings revealed that the effects of social isolation and disconnection from their communities are more pronounced among domestic workers and care workers, sectors that are highly feminized and characterized by gendered discrimination and abuse. The absence of supportive social ties not only exacerbates mental distress but also limits personal autonomy and community support, which may be essential in the provision of informal care, information, and pathways to crucial health and social services.
Although existing evidence demonstrates that various identity markers can heighten the vulnerability of precariously employed migrant women and shape their health experiences (Sisic et al., 2024; Yalcinoz-Ucan et al., 2025), the literature offers limited analytic attention to how these markers influence health consequences or access to services. When these identity markers are not adequately integrated, the health impacts of GBV and precarious employment can appear uniform among migrant women, obscuring how converging social identities and social variables such as documentation status, racialization, language, age, socio-economic status, and education can amplify health risks for migrant women at risk of GBV and precariously employed. In addition, domestic and care work feature prominently in our analysis, not because these sectors experience uniquely extreme health impacts, but because the evidence base is disproportionately focused on them while other sectors remain understudied. The limited attention to other sectors obscures how different employment contexts may produce distinct GBV risks, exposure, and health consequences for migrant women. A more sector-sensitive lens is therefore essential for understanding the full range of health impacts associated with the intersection of GBV and precarious employment and for informing policy and practice that responds to this diversity.
Implications for Policy and Practice
A summary of the implications of this review is displayed in Table 2. Taken together, our findings affirm the need to move beyond siloed approaches to GBV and precarious employment. These findings underscore the need for intersectional policy responses, provisions, and interventions that address the systemic links between labor precarity and GBV. Acknowledging precarious employment and GBV as social determinants of the health and well-being of women is critical in the design and implementation of strong labor protections and employee-centered economic policies and regulations that safeguard the rights and safety of migrant women. When policies and interventions fail to address the intersection of labor precarity and GBV, they risk overlooking the diverse experiences of migrant women and may inadvertently reinforce the system that sustains their marginalization and abuse.
Summary of the Implications for Policy, Practice, and Research.
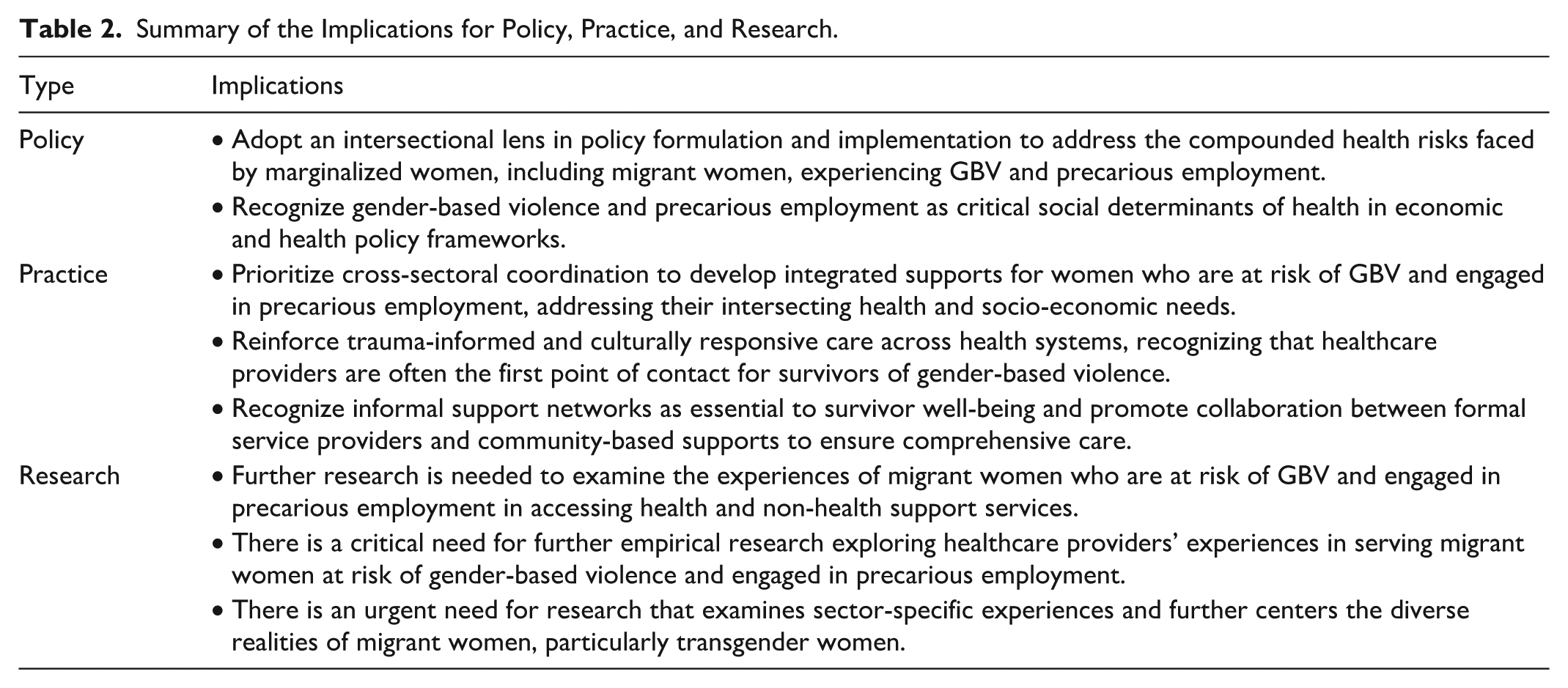
As highlighted in our findings, structural and sociocultural inequalities significantly shape women’s exposure to GBV and precarious employment, reinforcing their marginalization and limiting access to essential care and support services. Access to care is crucial, there is a need to prioritize access to support services, including health and social services. Consistent with previous studies (Aljomaie et al., 2022; Montesanti et al., 2025), health services are an access point for most women who experience violence, and as such, health systems play a critical role in the front-line response to migrant women’s abuse and exploitation, and in addressing their diverse needs. Thus, health responses should go beyond basic clinical care to include trauma-informed, culturally responsive care, recognizing the socio-cultural and structural factors that shape women’s exposure to violence and exploitation. Importantly, this also highlights the need for coordinated effort between health systems and other sectors such as labor, immigration, social services, and justice to develop integrated responses to the various health problems experienced by women in precarious employment and at risk of GBV.
Our findings highlight the importance of social networks and community groups in providing informational and material support to women in precarious employment and at risk of GBV. As such, intervention plans may also extend beyond formal services to include support for community-based programs that seek to empower community groups on how to address the challenges arising from the intersection of GBV and precarious employment. This may include providing funding programs that foster peer support and community building, as well as supporting grassroots organizations that provide advocacy, material and information resources, as well as safe spaces to women.
Although our study highlights key insights on the health impacts of the intersection of GBV and precarious employment among migrant women, several areas warrant further investigation. Few studies in this review examined the health impacts of migrant women and their experiences of accessing essential support services, which are often not readily available and accessible, highlighting a significant research gap. Further empirical research, from both survivors’ and service providers’ perspectives, would be beneficial to provide more certain evidence on the extent to which the intersection of GBV and precarious employment negatively affects the health and well-being of migrant women. In addition, there would be value in the prioritization of culturally responsive, trauma-informed, and rights-based approaches that center the lived realities of migrant women in precarious work in these further studies. Furthermore, the absence of analytic focus on how various identity markers, including age and race, mediate the health impacts of GBV for migrant women who are precariously employed highlights a significant gap in the literature on the intersection of GBV and precarious employment. As such, further intersectional-driven research is needed to examine the diverse pathways through which the interconnection of these various social identities compromises the health and well-being of migrant women who are precariously employed and at risk of GBV, to generate evidence relevant for policy and practice. Importantly, a key research gap is the limited attention given to migrant transgender women whose distinct experiences of marginalization, violence, and exclusion remain largely underexplored in migrant and GBV literature. Therefore, future research should explicitly examine the experiences of migrant transwomen. Addressing this gap is crucial in capturing the full diversity of migrant women and informing more inclusive policies and interventions that respond to their unique needs.
Limitations of the Review
Our scoping review has some limitations. First, our initial review primarily focused on understanding the interconnectedness of GBV and precarious employment, and we extracted data on health impacts from the studies included in this initial review. Given that we did not search gray literature, we may have missed relevant studies that discussed the health impacts of the intersection of GBV and precarious employment. In addition, our search terms were developed in English, which means we might have missed relevant studies published in non-English journals. Despite including only a few studies from the initial scoping review, we were able to distill the health impacts of GBV and precarious employment from the global literature, thereby laying the groundwork for future empirical studies seeking to explore the influence of this interconnectedness on poor health outcomes.
Conclusion
Our review explored the health impacts at the intersection of GBV and migrant women’s experiences, highlighting a critical health issue aligned with the SDGs. It sheds light on the detrimental effects of GBV and precarious employment on the health and well-being of migrant women, emphasizing the importance of adopting an intersectional lens in policy and program design. Such an approach is essential not only for supporting women’s healing and recovery but also for fostering their economic empowerment in new environments. The scientific literature on this topic remains scarce, underscoring the urgent need for further qualitative and quantitative research to deepen understanding of this complex phenomenon.
Supplemental Material
sj-docx-1-tva-10.1177_15248380261460447 – Supplemental material for Health Impacts at the Intersection of Precarious Employment and Gender-Based Violence Among Migrant Women: Insights From a Secondary Analysis of a Global Scoping Review
Supplemental material, sj-docx-1-tva-10.1177_15248380261460447 for Health Impacts at the Intersection of Precarious Employment and Gender-Based Violence Among Migrant Women: Insights From a Secondary Analysis of a Global Scoping Review by Cyndirela Chadambuka, Prossy Kiddu Namyalo, Rhea Raghunauth and Beverley M. Essue in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
We are grateful to the librarian who helped us with developing the search strategies for this study, and we would also like to thank Navya Arora, our research assistant, for her contribution to the screening process in the initial review.
Ethical Considerations
This secondary analysis of a scoping review did not require ethics approval as it did not involve the collection of data from human subjects.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institute of Health Research (Grant number 190733).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data relevant to the study have been shared in the manuscript and supplementary material.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.