
Abstract
Childhood exposure to intimate partner violence (CEIPV) is a pervasive adverse childhood experience with wide-ranging mental health consequences, yet its associations with mental health problems remain inconsistent across studies. Existing meta-analyses are dated and have largely overlooked outcomes beyond childhood. This study employed a three-level meta-analysis to examine the magnitude of the association between CEIPV and mental health outcomes, as well as potential moderators. A systematic search yielded 36 eligible studies (78 effect sizes; N = 59,561). Based on variations in clinical specificity and outcome labels used across studies, outcomes were classified as internalising problems, depressive symptoms, and PTSD-related symptoms. Results revealed a significant moderate overall effect (r = 0.263). The association was significant across internalising problems (r = 0.252), depressive symptoms (r = 0.227), and PTSD-related symptoms (r = 0.319). Moderation analyses indicated that higher study quality and larger sample sizes were associated with smaller effect sizes, and these patterns also applied to the depressive symptoms and internalising problems subgroups, respectively. Studies using the Conflict Tactics Scale showed larger effect sizes compared to studies using other measures. In addition, older participant age was associated with slightly larger effect sizes in the PTSD-related symptoms subgroup. These findings indicate that CEIPV confers significant mental health risks, underscoring the need for trauma-informed prevention and intervention efforts.
Keywords
Introduction
Childhood exposure to intimate partner violence (CEIPV) encompasses a broad range of direct and indirect experiences, including witnessing or hearing parental violence, observing its aftermath, intervening in violent incidents, and living in a home characterised by ongoing threat, coercive control, and emotional insecurity (Carlson, 2000; Cater et al., 2015; MacMillan & Wathen, 2014). CEIPV has therefore increasingly been recognised as an adverse childhood experience associated with substantial mental health and developmental consequences (McTavish et al., 2016). A global data brief by the United Nations Children’s Fund (UNICEF) (2025) estimates that intimate partner violence (IPV) affects one in four children, around 610 million, who live with mothers experiencing such violence. A systematic review reported that approximately 29% of children in low- and lower-middle-income countries have experienced IPV exposure during their lifetime (Kieselbach et al., 2022). Similarly, in high-income contexts, evidence from a US national survey reports a comparable rate of 25.0% (Finkelhor et al., 2015), indicating that CEIPV is a significant social concern across contexts. A growing body of research indicates that CEIPV is associated with an increased risk of developing mental health problems, including internalising problems, depressive symptoms, and PTSD-related symptoms (Asiedu & Baliki, 2025; Gardner et al., 2019). However, previous meta-analyses have primarily synthesised studies conducted over two decades ago and focused exclusively on outcomes assessed in childhood, thereby omitting outcomes in adulthood (Evans et al., 2008; Wolfe et al., 2003). Recent meta-analyses have examined CEIPV as a subcategory of childhood maltreatment, rather than as a distinct construct with its own specific mechanisms of psychological effects (Gardner et al., 2019). Given the conflicting conclusions and the lack of an up-to-date, comprehensive meta-analysis, the present study aims to clarify the association between CEIPV and mental health problems using a three-level meta-analytic approach.
Mental Health Outcomes Associated with CEIPV
Internalising problems, depressive symptoms, and PTSD-related symptoms (e.g., PTSS and PTSD) are the most frequently reported mental health outcomes in the literature on CEIPV (Asiedu & Baliki, 2025; Lee et al., 2023). Although these variables reflect overlapping constructs, they differ in scope, which has led prior studies to adopt distinct terminological labels. Specifically, internalising problems typically reflect a broad spectrum of emotional distress, including anxiety, depressed mood, and withdrawal (McConaughy & Skiba, 1993). In contrast, depressive symptoms refer to the core clinical features of depression (e.g., worthlessness or guilt) (Paykel, 2008), while PTSD-related symptoms centre on trauma-specific reactions (e.g., avoidance or hyperarousal; Stein et al., 2014). Unlike internalising problems, the latter two constructs are more clinically specific and map more directly onto formal diagnostic criteria (Rossi et al., 2024). Analysing these three outcome types separately aligns with how these outcomes are labelled in the literature and helps reveal differences in their clinical specificity.
Some studies have examined internalising problems and found that, after controlling for co-occurring risk factors, early exposure to IPV significantly predicts children’s internalising problems (Lee et al., 2023). Longitudinal evidence has further substantiated the link between CEIPV and later internalising problems (Roopnarine et al., 2023; Skafida & Devaney, 2023; Yoo & Huang, 2013). Regarding depressive symptoms, research has shown that witnessing parental violence is associated with higher levels of depressive symptoms in children (Ponnamperuma & Kudagama, 2022). Early CEIPV directly predicts higher depression scores during adolescence (Huang et al., 2021) and in adulthood (Chan et al., 2018). In addition, the frequency of witnessed IPV is positively correlated with children’s PTSS (Levendosky et al., 2013). A significant relationship between the severity of IPV exposure and trauma symptoms has also been observed (Haj-Yahia et al., 2021). Overall, CEIPV is linked to multiple domains of mental health problems, exerting adverse effects not only on children’s psychological functioning but also on outcomes that persist into adulthood.
Theoretical Mechanisms: From IPV Exposure to Mental Health Problems
Several theories provide insight into the association between CEIPV and mental health problems. Emotional security theory conceptualises children’s exposure to interparental violence as a threat to emotional security within the family system; in this framework, emotional insecurity serves as a risk factor for the development of dysfunctional traumatic stress reactions and increased vulnerability to psychological maladaptation (Davies et al., 2006; Meijer et al., 2019). Attachment theory suggests that CEIPV undermines caregiver-child attachment relationships and is associated with lower levels of secure attachment; this disruption subsequently hinders self-regulation and contributes to emotional and behavioural difficulties (Levendosky et al., 2012; Noonan & Pilkington, 2020). From a trauma-based perspective, these experiences are often chronic, repetitive, and relational; therefore, they may be classified as complex trauma (Kliethermes et al., 2014), leading to severe trauma-related consequences. Accordingly, traumatised children may experience emotional dysregulation and psychological problems, such as depression and anxiety (Voith et al., 2020). These theoretical perspectives suggest that CEIPV constitutes a traumatic experience that may disrupt key psychological mechanisms, thereby adversely affecting children’s mental health.
Inconsistent Findings and the Need for Moderator Analyses
Despite the general pattern, the relationship between CEIPV and mental health problems remains complex and inconclusive. Several studies have reported that the associations between IPV exposure and certain mental health outcomes are not significant (Capaldi et al., 2020; Cochran et al., 2022; Rea & Rossman, 2005; Renner & Boel-Studt, 2012). For instance, Renner and Boel-Studt (2012) found no direct or indirect associations between IPV exposure and internalising problems among adolescents. Another study found that the direct effect of IPV exposure on children’s PTSD symptoms was not statistically significant (Rea & Rossman, 2005). Similarly, Capaldi et al. (2020) found that the effect of IPV became nonsignificant after controlling for parent-child aggression. Differences in research design, sample composition, and the operationalisation of IPV across studies may substantially influence the observed associations between CEIPV and mental health outcomes. In addition, age may moderate this association. Evidence suggests that the timing of violence exposure is significantly related to child outcomes (Cater et al., 2015; Graham-Bermann & Perkins, 2010), with effect sizes potentially varying according to chronological age. Such variations may partly explain inconsistent effect sizes across studies, underscoring the need for an integrative meta-analytic approach and detailed moderator analyses.
The Current Study
Given the conflicting conclusions in the existing literature and the lack of a comprehensive and up-to-date meta-analysis, the present study aims to clarify the association between CEIPV and mental health problems using a three-level meta-analytic approach. This method addresses the multilevel and multivariate nature of the data, yielding more precise and reliable results than traditional meta-analyses. Specifically, this study examines: (a) the overall association between CEIPV and mental health problems; (b) the difference across three outcome types (internalising problems, depressive symptoms, and PTSD-related symptoms); and (c) potential moderators, including participant age, study quality, sample size, and IPV measurement tools. By synthesising available evidence, this study provides a robust empirical foundation to help social service professionals better understand the overall and specific mental health consequences of CEIPV, thereby facilitating evidence-based policies and targeted interventions.
Methodology
Search Strategy
This meta-analysis followed the PRISMA guidelines (Moher et al., 2010). The study protocol was registered in the PROSPERO database (Registration ID: CRD420251155830). Seven electronic bibliographic databases (i.e., PsycINFO, PubMed, Scopus, Web of Science, ProQuest Social Science Database, Social Services Abstracts and EBSCO) were searched for articles published up to October 2025; Google Scholar served as a supplementary source. The search also used snowball sampling to identify additional relevant literature.
The search strategy employed keywords related to children exposed to IPV (e.g., children exposed to IPV, childhood IPV exposure, CEIPV, exposure to family violence in childhood, indirect family violence victimisation, and witnessing IPV), psychological outcomes (e.g., psychological outcomes, mental health outcomes, psychological well-being, mental health, psychological health, mental health problems, mental illness, psychological disorders and psychological distress).
Inclusion and Exclusion Criteria
To be included in the meta-analysis, studies had to meet the following criteria: (a) be peer-reviewed quantitative studies; (b) investigate exposure to IPV before age 18; (c) examine the association between CEIPV and mental health outcomes; and (d) report a correlation coefficient or other effect sizes convertible to correlations for the relationship between CEIPV and mental health outcomes. Additionally, studies were excluded if they failed to meet the above inclusion criteria, were not written in English, or were unavailable in full text.
Screening and Data Extraction
Three reviewers imported the retrieved records into reference management software for deduplication and initial screening. The reviewers independently screened each study for inclusion by reviewing its title and abstract. Subsequently, full-text screening was conducted for the potentially eligible studies, and a total of 36 full-text articles were ultimately included. Any discrepancies were discussed and resolved by consensus.
The three reviewers then extracted relevant research findings from the full-text articles for coding and analysis. The team extracted the following data from each included article: (a) first author’s name and publication year; (b) sample characteristics (e.g., sample size, study region, age at CEIPV exposure, age at assessment of subsequent psychological outcomes, and proportion of female participants); (c) methodological characteristics (e.g., measurement tools for IPV exposure, reporters of children’s IPV exposure, and study design); and (d) correlation data between children’s IPV exposure and psychological outcomes.
Data Analytic Procedures
Compared to traditional meta-analysis, three-level meta-analysis addresses within-study dependency among effect sizes. In this study, a random-effects model was employed to simultaneously estimate the variances at the sampling variance level, study level, and effect size level. Since the sampling distribution of the correlation coefficient r is not normal across the included studies, the r values from different studies may exhibit heterogeneous variances. Following Cooper’s (1994) recommendation, the extracted r values from the original studies were transformed into Fisher’s Z scores, because the distribution of Z scores approximates normality and has stable variance, satisfying the assumptions required for the pooling of effect sizes. After completing the calculations, Fisher’s Z was back-transformed into r for interpretability. Based on the guidelines suggested by Wilson and Lipsey (2001), effect sizes of 0.10, 0.25 and 0.40 were interpreted as small, medium, and large, respectively.
Heterogeneity was examined using the Q and I² statistics, with a significant Q statistic indicating the presence of heterogeneity (Hedges & Olkin, 2014). The I² statistic was used to evaluate the degree of heterogeneity, with values interpreted as low (<25%), moderate (25%–50%), substantial (50%–75%) or high (≥75%) (Higgins et al., 2003). When significant heterogeneity was detected, subgroup analyses were performed.
In addition to common sample and study characteristics, such as age, gender and study design, studies were also categorised based on specific psychological outcomes. In the included studies, the labelling of outcome variables varied. Some studies directly used the term “internalising symptoms,” while others used a subdomain-related term, such as “anxious-depressed behaviour problems.” Some studies used “depression” or “depressive symptoms,” and others used “PTSD” or “PTSS.” Based on the operationalised content of the scales used, we consolidated these outcome variables into three categories. The first category was internalising symptoms (broadly defined), which included general internalising symptoms measured by the Child Behavior Checklist (CBCL) or its subdimensions. The second category was depressive symptoms, and the third was PTSD-related symptoms. The first category encompassed a broader spectrum of symptoms, whereas the latter two categories included only studies that used specific scales to measure the respective clinical symptoms.
Moreover, Egger’s regression test and funnel plots were employed to test for publication bias. Based on the nonsignificant p-value (p > .05) from Egger’s regression test and the observed symmetry of the funnel plot, the risk of publication bias was considered nonsignificant. Additionally, to validate the robustness of the results, a leave-one-out sensitivity analysis was performed by sequentially removing each effect size and rerunning the three-level meta-analysis. Subsequently, this procedure was repeated by removing each individual study to assess the stability of the findings. All data analysis procedures were conducted using R 4.4.3.
Methodological Quality Assessment
Study quality was assessed using the NIH Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. The maximum score for this assessment tool was 14, with three researchers rating each study. The three researchers resolved any scoring disagreements through discussion until they reached consensus. If an article met a criterion on the scale, it received 1 point; otherwise, it received 0 points. A higher score indicated better methodological quality. Supplemental Table S1 presents the specific scoring for each included study.
Results
Study Characteristics
This study synthesised evidence from 36 studies conducted across four continents (see Figure 1). Supplemental Table S1 displays the characteristics of the retained studies. The United States accounted for the largest number of studies (k = 22). Among Asian regions, studies were conducted in Israel (k = 2), China (k = 2), and Sri Lanka (k = 1). In Europe, studies were conducted in the United Kingdom (k = 3), France (k = 2), Portugal (k = 1), and Switzerland (k = 1). Additionally, one study originated from Brazil and one from Guyana in South America. A total of 59,561participants were included, with a mean age of approximately 13.79 years.
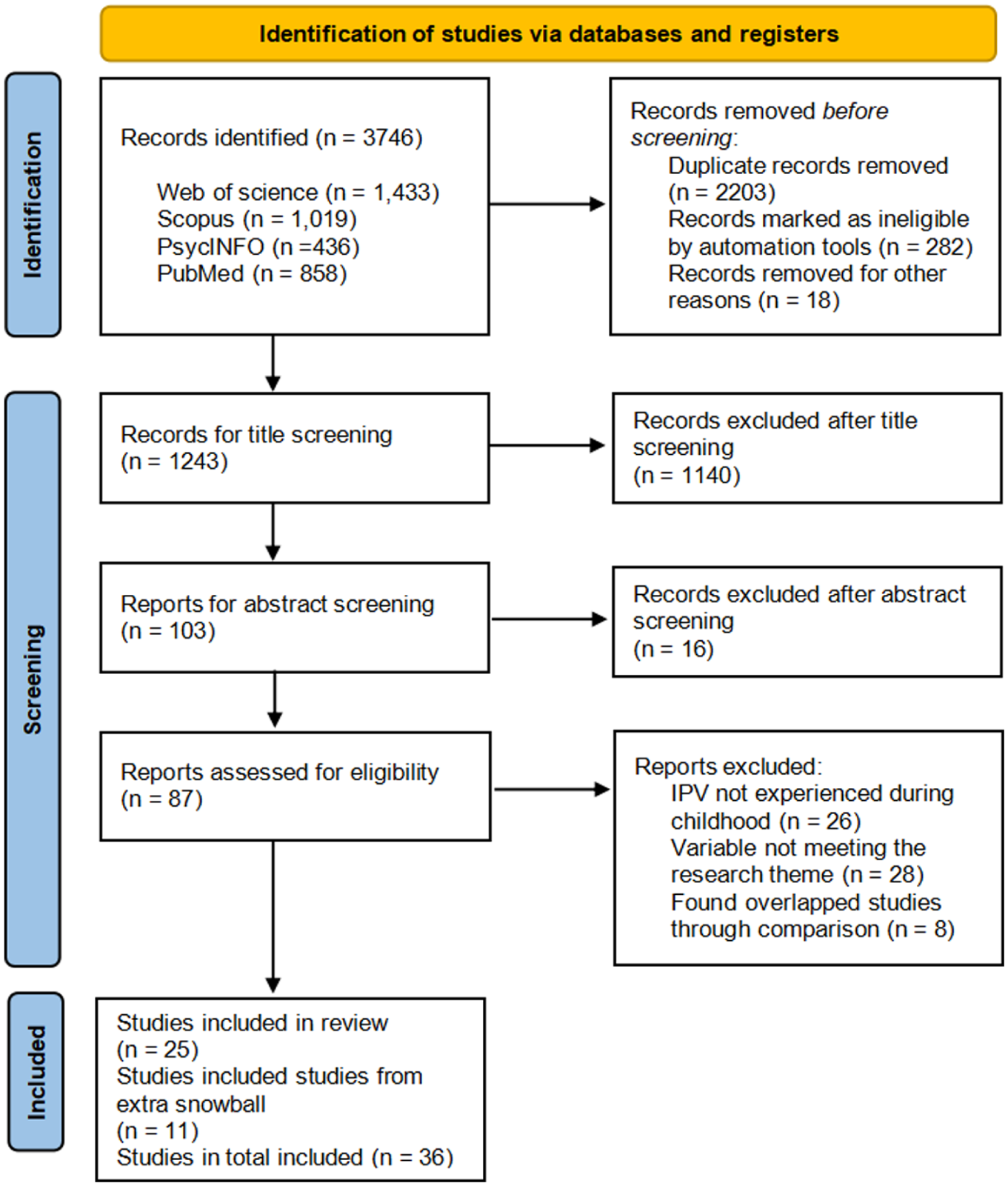
PRISMA flowchart.
Regarding study design, 19 studies used a cross-sectional design, whereas 17 employed a longitudinal design. To measure CEIPV, some studies used self-developed questionnaires or structured interviews to assess IPV exposure (n = 9), whereas others used validated scales (n = 27). The most frequently used scales were the (Revised) Conflict Tactics Scale (CTS, Straus, 1979; CTS2, Straus et al., 1996) (n = 20). Moreover, among the 24 studies relying on parental reports, 18 primarily involved mothers reporting their own IPV experiences, whereas the other six studies utilised joint reports from parents. Nine studies used child self-reports, and three studies used multiple perspectives, assessing both parental violence experiences and children’s exposure. Regarding study quality, the average NIH checklist score for the included studies was 10.39.
Among all included effect sizes (n = 78), most findings indicated an association between IPV exposure and mental health problems. These results highlight the adverse association between IPV exposure and the mental health of children and adolescents. However, eight effect sizes yielded nonsignificant findings, indicating that the associations between IPV and some mental health indicators were not significant.
Main Effects and Heterogeneity
The results showed a significant positive correlation between CEIPV and mental health outcomes (r = 0.263, 95% CI [0.209, 0.316], p < .001). This correlation corresponds to a medium effect size, as suggested by Wilson and Lipsey (2001). A total of 35 effect sizes reported the correlation between IPV exposure and internalising problems (r = 0.252, 95% CI [0.186, 0.316], p < .001). Twenty-one effect sizes showed the association between IPV exposure and depressive symptoms (r = 0.227, 95% CI [0.152, 0.299], p < .001), whereas 22 effect sizes revealed the association between IPV exposure and trauma-related symptoms (r = 0.319, 95% CI [0.247, 0.387], p < .001).
Significant variance existed at the within-study (Level 2; σ2 = .004, p < .001) and between-study (Level 3; σ2 = .023, p < .001) levels. Regarding the composition of the total variance, sampling error (Level 1) accounted for 19.99%, whereas within-study and between-study variance contributed 12.46% and 67.55%, respectively. The substantial between-study heterogeneity underscores the necessity of examining potential moderators in this three-level meta-analysis.
Publication Bias and Sensitivity Analysis
Egger’s test was nonsignificant (F[1, 76] = 3.520, p = .065; intercept = 0.330, 95% CI [0.244, 0.416]), and the funnel plot appeared roughly symmetric (see Figure 2). These results suggested an absence of substantial publication bias in the present meta-analysis. Sensitivity analyses were then performed to examine the reliability of the results by excluding each study and effect size sequentially. When each individual effect size was excluded, the aggregated effect sizes ranged from 0.260 to 0.266. A leave-one-study-out procedure further demonstrated that the effect size estimates remained stable, varying between 0.258 and 0.268. To conclude, the overall effect remained significant and stable throughout the sequential exclusion, supporting the robustness and reliability of the current meta-analytic results.
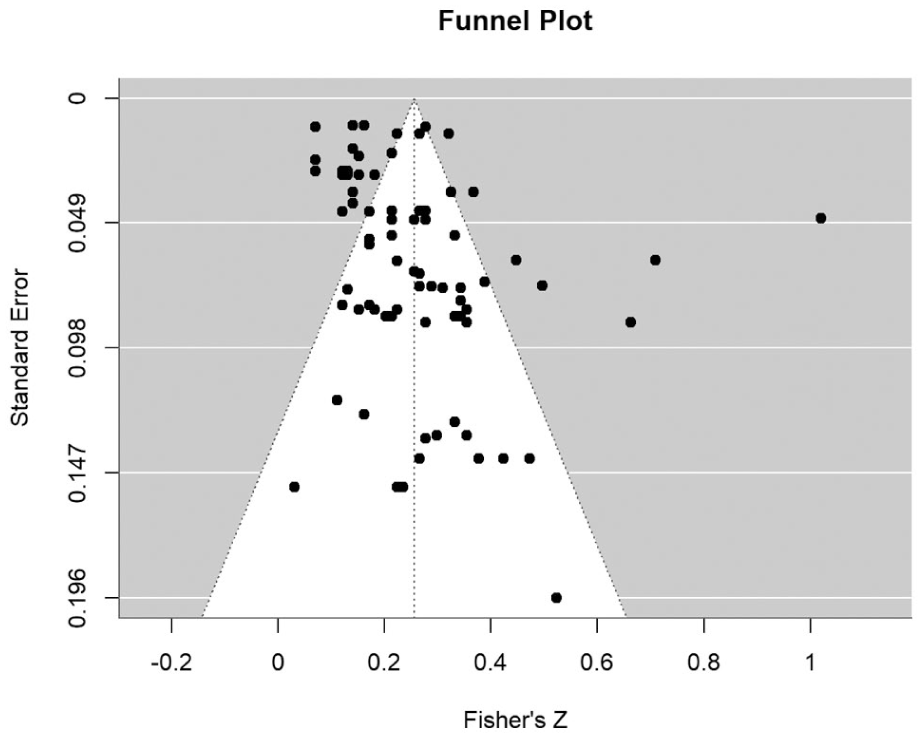
Funnel plot for publication bias.
Moderating Effect
Analysis of several variables revealed significant moderating effects (see Table 1). First, the type of mental health outcome significantly moderated the effect size. Specifically, studies assessing PTSD-related symptoms (r = 0.319, SE = 0.040, 95% CI [0.247, 0.387], p < .001) yielded significantly larger effect sizes than those assessing internalising problems (r = 0.252, SE = 0.035, 95% CI [0.186, 0.316], p < .001) or depressive symptoms (r = 0.227, SE = 0.040, 95% CI [0.152, 0.299], p < .001).
Moderator Analyses of Overall Mental Health Problems and Outcome Subgroups.
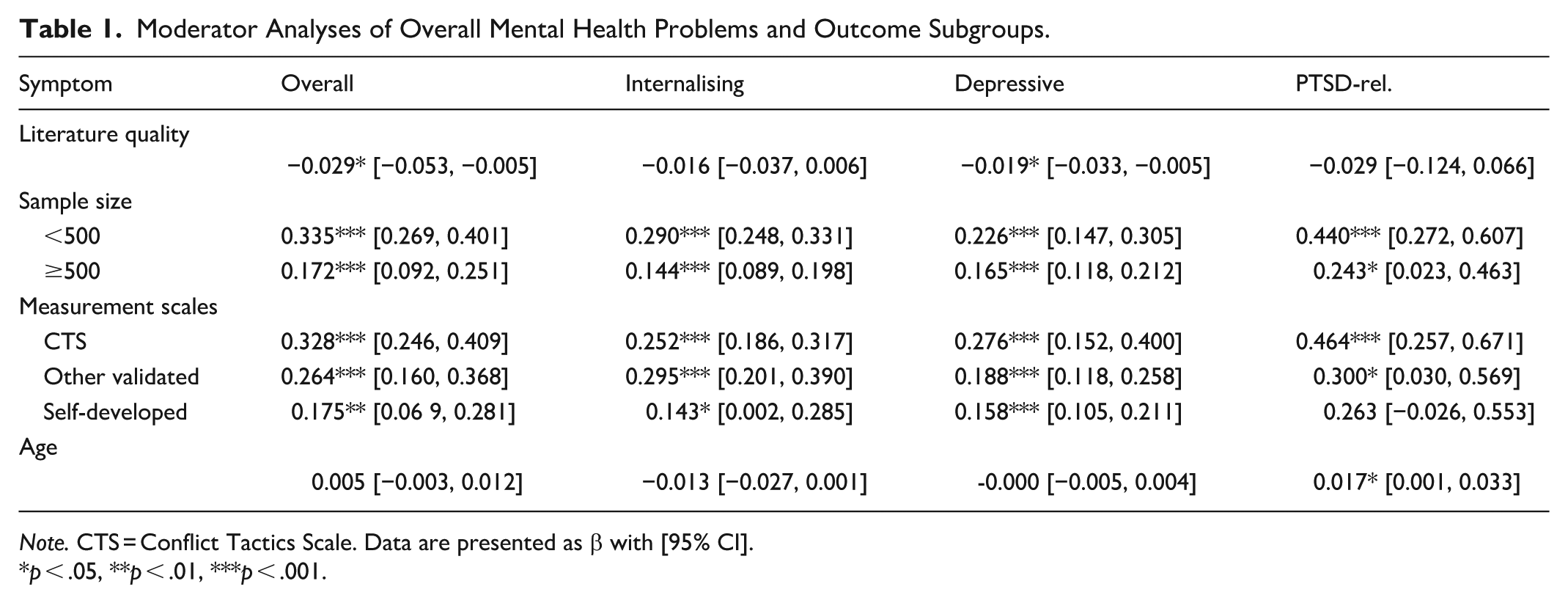
Note. CTS = Conflict Tactics Scale. Data are presented as β with [95% CI].
p < .05, **p < .01, ***p < .001.
Second, study quality (β = −.029, 95% CI [−0.053, −0.005], p = .018) emerged as a significant overall moderator. Higher-quality studies were associated with significantly smaller effect sizes. This moderating effect was also significant within the subset of studies measuring depressive symptoms (β = −.019, 95% CI [−0.033, −0.005], p = .013).
Third, the sample size showed different effects across outcome groups. Studies with fewer than 500 participants (β = .335, 95% CI [0.269, 0.401], p < .001) demonstrated significantly larger effect sizes than those with more than 500 participants (β = .172, 95% CI [0.092, 0.251], p < .001) (difference between groups: Δβ = .163, 95% CI [0.063, 0.263], p = .003). This pattern remained significant among studies measuring internalising problems (for studies with <500 participants: β = .290, 95% CI [0.248, 0.331], p < .001; for studies with >500 participants: β = .144, 95% CI [0.089, 0.198], p < .001; difference between groups: Δβ = .146, 95% CI [0.082, 0.210], p < .001).
Fourth, the type of IPV measurement tool significantly moderated the results. Studies using the CTS (β = .328, 95% CI [0.246, 0.409], p < .001) reported significantly larger effect sizes than those using self-developed questionnaires (β = .175, 95% CI [0.069, 0.281], p = .002), with a significant pairwise difference (Δ β = .153, 95% CI [0.024, 0.281], p = .026). Other validated scales yielded moderate effect sizes (β = .264, 95% CI [0.160, 0.368], p < .001) and did not differ significantly from either the CTS (Δβ = .063, p = .338) or self-developed questionnaires (Δβ = .090, p = .227).
Finally, participant age significantly moderated the association between CEIPV and PTSD‑related symptoms, such that the positive association was stronger among older individuals (β = .017, 95% CI [0.001, 0.033], p = .049).
Discussion
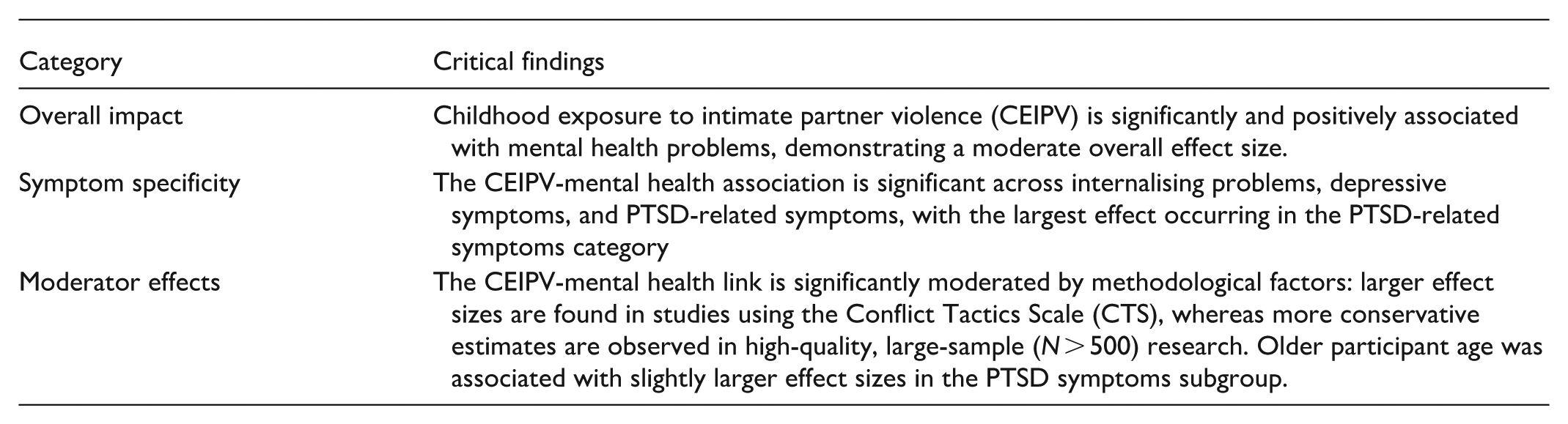
The three-level meta-analysis revealed associations between CEIPV and mental health problems across the included studies. Overall, CEIPV showed a significant positive correlation with mental health problems, yielding a moderate effect size. This result indicates that higher levels of CEIPV are associated with increased mental health problems. This positive association was significant across internalising problems, depressive symptoms, and PTSD-related symptoms, with the largest effect occurring in the PTSD-related symptoms category. Regarding the moderating effects, study quality scores significantly moderated the association between CEIPV and mental health problems; the effect size decreased as study quality increased, and this pattern was also observed in the depressive symptoms subgroup. In addition, larger sample sizes (>500) were associated with significantly smaller effect sizes than smaller samples (<500), and this pattern was also significant in the internalising problems subgroup. Studies utilising the CTS reported larger effect sizes than those using self-developed questionnaires. Finally, age positively moderated the association, suggesting that older participant age was associated with a stronger relationship between IPV exposure and PTSD-related symptoms.
These findings align with the mechanisms proposed in previous studies (Asiedu & Baliki, 2025; Vu et al., 2016) and provide empirical support for these theoretical explanations. The results also support theories suggesting that CEIPV may contribute to subsequent mental health problems, including depressive symptoms, internalising problems, and PTSD-related symptoms. Trauma-related theories propose that individuals who experience highly distressing events, including exposure to domestic violence, may develop psychological problems. Additionally, the cognitive-contextual framework and emotional security theory examine the association between IPV on children’s adjustment through the lens of children’s responses to parental conflict (Hungerford et al., 2012). These theories emphasise that exposure to adverse events in early life constitutes toxic stress, which can lead to psychological changes (Bucci et al., 2016). Although internalising problems, depressive symptoms, and PTSD-related symptoms are closely interconnected, they represent distinct psychological conditions with unique characteristics. Consequently, the association between IPV exposure and each outcome may differ, underscoring the need for more granular research on the mental health outcomes of IPV exposure.
Higher methodological quality scores were linked to lower effect sizes. Methodological quality is often closely related to study design and other methodological factors, with high-scoring studies typically employing a longitudinal design. By contrast, cross-sectional studies collect exposure and outcome data at a single time point, making it impossible to determine the temporal sequence of variables. This limitation makes such studies more susceptible to confounding factors, reverse causality, and selection bias, which may lead to an overestimation of the true effect.
Consistent with this pattern, smaller sample sizes (<500) were associated with larger effect sizes. Small studies are more vulnerable to biases, including publication bias and random error, as well as methodological constraints, all of which may contribute to overestimated effects. In addition, larger samples tend to be more representative of the general population and are therefore more likely to include individuals who, despite exposure to CEIPV, maintain good mental health due to higher levels of resilience. Prior research further suggests that psychological outcomes among individuals exposed to CEIPV are heterogeneous, with not all individuals experiencing adverse effects to the same extent. Protective factors, including adaptive coping strategies and social support, can buffer the negative impact of CEIPV (Tajima et al., 2011). Consequently, in more representative large samples, a relatively higher proportion of resilient individuals may be captured, which can attenuate the overall observed effect size.
In addition, studies using the CTS reported larger effect sizes than those using self-developed questionnaires. The CTS is a widely used instrument designed to assess conflict tactics within intimate relationships. Its items use concrete behavioural indicators, such as being kicked, bitten or punched by a partner, which may help minimise recall bias and facilitate more reliable reporting of overt violent behaviours. This may partly explain why studies employing the CTS often report larger effect sizes for mental health outcomes. However, IPV involves complex dynamics, and the CTS may not adequately capture certain subtle but dangerous forms of IPV, such as coercive control and harassment. In recent years, the Composite Abuse Scale (CAS) has gained increasing recognition for its ability to assess these covert forms of abuse more comprehensively (Hegarty et al., 1999). Moreover, the measurement of emerging critical dimensions like economic abuse remains underdeveloped in existing scales, highlighting the need for future research to address this gap.
The present study also showed that older age was associated with a larger association between IPV exposure and PTSD-related symptoms. This finding may arise from several underlying mechanisms. Unlike internalising problems or other psychological distress, which are more susceptible to recent emotional states, PTSD is more closely tied to neural circuits involved in memory and fear. This neurobiological basis may enhance the stability of CEIPV’s impact on PTSD, making its effects more persistent. Ogle et al. (2013) found that childhood trauma exposure had the strongest effect on PTSD symptoms in older adulthood compared to trauma in other periods. Beyond these neurodevelopmental pathways, individuals exposed to IPV often grow up in disadvantaged circumstances characterised by limited social support, and the accumulation of additional adversities over time may further exacerbate their mental health problems. Some research suggested a delayed effect of trauma, whereby the effects of early IPV exposure may be reactivated or amplified as individuals transition into adulthood and encounter more complex social roles (Cater et al., 2015). However, the participants in the included studies were predominantly young, so the results should be interpreted with caution.
Limitations and Implications
Several limitations of this meta-analysis should be noted. First, the moderator analyses focused primarily on study characteristics, whereas individual-level developmental factors (e.g., coping strategies, attachment style) were not examined because of insufficient reporting in primary studies. Future research should incorporate these individual-level variables to better understand the heterogeneity in mental health outcomes following CEIPV. Second, most included studies were conducted in Western countries, particularly the United States and European nations. Consequently, these findings may be more applicable to Western populations than to Asian or other non-Western contexts. Cross-cultural research on CEIPV is therefore needed. Third, given the methodological heterogeneity across samples and studies, the overall effect size should be interpreted with caution.
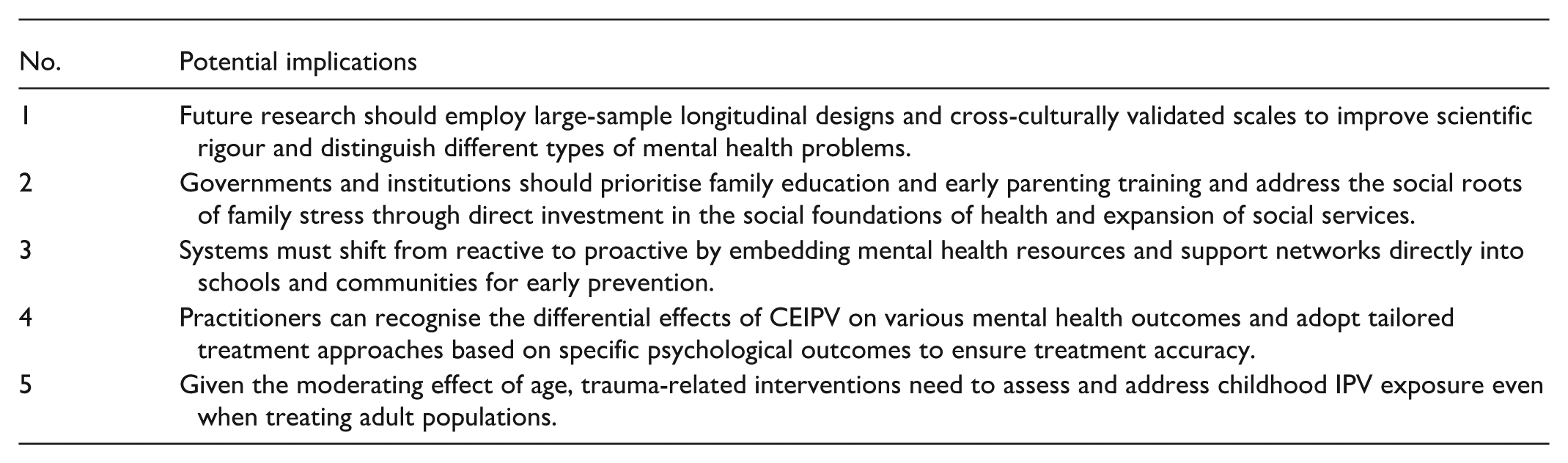
This meta-analysis also offers several practical insights. The findings suggest that future research should employ large-sample longitudinal designs and cross-culturally validated scales to improve scientific rigour. Moreover, treating mental health as a single composite variable is insufficient to explain children’s psychological development; instead, the findings highlight the differential associations between CEIPV and various mental health outcomes. From a practical perspective, governments and institutions should prioritise family education and early parenting training to reduce CEIPV. However, individual and family education may not be sufficient to eliminate violence without broader structural support. New policies are needed to tackle the social roots of family stress and abuse. Economic aid is a proven method to reduce financial burdens and prevent family conflict, including more affordable childcare and higher subsidies for low-income households (Matjasko et al., 2012). In addition, social systems must become proactive rather than reactive. Governments need to invest early by placing mental health resources and support networks directly into schools and communities. This study also suggests the importance of adopting targeted treatment approaches for different psychological outcomes. For example, attachment- and emotion-focused parenting interventions may be particularly suitable for addressing CEIPV and internalising problems. Such interventions help parents understand and respond to their child’s potential attachment and emotional needs, thereby improving family relationships and reducing internalising symptoms (Jugovac et al., 2022). Preventive cognitive behavioural therapy has also been shown to be effective in addressing depressive symptoms (Arena et al., 2023). In addition, trauma-focused cognitive behavioural therapy and school-based trauma interventions may improve children’s adjustment following potentially traumatic events (Lange et al., 2022).
To ensure children’s positive development, governments and social workers should commit to reducing CEIPV. Given the significant moderating effect of age, interventions targeting trauma-related symptoms should address the impact of childhood IPV and other adverse childhood experiences, even among adult populations. Institutional policies should avoid placing the responsibility for child well-being solely on families. Parents cannot address structural problems without support from society. Therefore, governments must lead efforts in poverty reduction and social welfare. This requires direct investment in the social foundations of health. For instance, authorities can raise the minimum wage and promote stable housing. Expanding social services is also necessary. These concrete actions may remove the environmental stressors that limit parents’ ability to care for their children. In sum, structural support is essential for promoting healthy child development.
Critical Findings of This Review
Potential Implications for Research, Practice, and Policy
Supplemental Material
sj-docx-1-tva-10.1177_15248380261462866 – Supplemental material for Childhood Exposure to Intimate Partner Violence: A Three-Level Meta-Analysis to Examine the Impact on Mental Health
Supplemental material, sj-docx-1-tva-10.1177_15248380261462866 for Childhood Exposure to Intimate Partner Violence: A Three-Level Meta-Analysis to Examine the Impact on Mental Health by Shuo Xu, Zhe Xie, Mingyan Li, Jianing Zhao and Manya Li in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
The authors would like to thank the anonymous reviewers for their insightful comments on earlier versions of this manuscript. We also express our gratitude to the primary researchers whose work made this meta-analysis possible.
Ethical Considerations
This study is a meta-analysis based on previously published data and does not involve direct contact with human participants or animals. According to institutional guidelines, ethical approval and informed consent were not required for this type of study. The research was conducted in accordance with the ethical standards of the 1964 Helsinki Declaration and its later amendments.
Author Contributions
Shuo Xu: Conceived of the study, performed the statistical analysis, drafted the Results section, and wrote the initial manuscript. Zhe Xie: Participated in the study design, performed data cleaning, and drafted the Discussion, Implications, and Limitations sections. Mingyan Li: Contributed to the study conception, conducted the literature review, drafted the Introduction, and coordinated the submission process as the corresponding author. Jianing Zhao: Designed and formatted the tables and figures, and performed critical language editing and proofreading of the manuscript. Manya Li: Contributed to the conceptual discussion, and performed critical language editing of the manuscript. All authors contributed to the literature search and screening, data extraction, and final revision of the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analysed during the current study are available from the corresponding author on reasonable request.*
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.