
Abstract
Public health training centers were established to enhance competencies in skills required to meet 21st-century public health challenges. In 2011, the Puerto Rico–Florida Public Health Training Center conducted surveys to assess the training needs of two populations of public health workers serving Hispanic communities: Florida Department of Health employees and workers at the regional and central offices of the Puerto Rico Department of Health. The two surveys were similar, but not identical in content and administration. A 52.6% response rate was achieved in the Commonwealth of Puerto Rico, where limited computer access necessitated use of a pen-and-paper survey. A 20.7% response rate was achieved in Florida, where an online survey was used and incomplete responses were problematic. Puerto Rico respondents (n = 1,414) were similar in age (Mdn age = 48 years) to Hispanic Florida respondents (n = 546, Mdn age =45 years). They also reported higher levels of academic achievement and more years of experience in public health. Nevertheless, self-assessed public health competency scores were in the low- to mid-range for Hispanic respondents in both locales. Although self-assessed training priorities differed, Hispanic employees in both jurisdictions preferred hands-on and face-to-face training to distance learning. Findings indicate a need for training based on adult learning theory, targeted to entry-level employees, and addressing the top five self-assessed training needs, especially health promotion and disease prevention and public health law and policy, which emerged as priority training areas in both survey populations.
Introduction
A well-trained and diverse workforce is needed to address persistent and emerging public health challenges in the 21st century (Cohen, Gabriel, & Terrell, 2002). For example, a skilled and culturally competent workforce can play an important role reducing health disparities (Dendoba, Bragdon, Epstein, Garthright, & Goldman, 1998). Research suggests that use of bilingual and bicultural facilitators may influence the success of health programs for Hispanics, such as interventions to promote nutrition and exercise (Mier, Ory, & Medina, 2010). Professional development is a way to both increase workforce competence and to enhance job performance to increase opportunities for advancement for employees of diverse racial and ethnic backgrounds. Effective professional development in turn, relies on training opportunities informed by an understanding of the training needs and preferences of targeted personnel (Betancourt, Green, Carrillo, & Ananeh-Firempong, 2003). The Council on Linkages (CoL) Between Academia and Public Health Practice (2010) has called for curricula to fill gaps in knowledge, skills, and professional abilities to respond to existing needs, priorities, and public health core competency requirements.
The Puerto Rico–Florida Public Health Training Center (PR-F PHTC) was established in August 2010 to identify training needs and improve the performance of Spanish- and English-speaking public health workers serving Hispanic and other underserved populations (Puerto Rico–Florida Public Health Training Center, 2011). As one of few public health training centers with a primary focus on Hispanic populations, the PR-F PHTC is also committed to enhancing career opportunities for public health professionals of Hispanic or Latino origin.
In Puerto Rico, 2,686 public health workers served a population of 3,706,690 residents in 2011. The vast majority of workers and residents were considered to be Hispanic and spoke Spanish fluently. In Florida, 17,837 workers were employed by the Department of Health on May 1, 2011, to serve a highly diverse population of approximately 19 million residents living in 67 counties (Hughes, 2011). Persons of Hispanic or Latino origin were estimated to comprise 22.9% of Florida’s population in 2011, an increase of 57.4% since 2000 (U.S. Bureau of the Census, 2012), and will almost certainly comprise a greater portion of the state population in coming years. The majority of Hispanic residents in Florida reside in three southeastern counties—Broward, Miami-Dade, and Palm Beach—where many residents communicate in Spanish.
In response to a national requirement of the Health Resources and Services Administration, the PR-F PHTC designed and conducted needs assessment surveys of department of health employees of the Commonwealth of Puerto Rico and the state of Florida. Survey findings will be used to prioritize training topics and activities for the public health workforces in Puerto Rico and Florida.
Background
Staff shortages due to retirements, resignations, layoffs, and hiring freezes have affected adversely the abilities of federal, state, territorial, and local health departments to carry out essential services and to respond to crises (Beck & Boulton, 2012). More than 20% of the estimated half million public health workers in the United States are now eligible for retirement. In some state health agencies, the number of employees eligible to retire represents over half the total workforce. Yet, while health agencies are losing their most experienced professionals, the need for public health services is rising: at least 250,000 additional public health workers will be needed by 2020 just to keep pace with population increases (Rosenstock et al., 2008).
Shrinking staffs are not the only concern for public health agencies. Only 20% of the nation’s currently employed public health professionals have the education and training required to do the jobs they hold (Hilliard & Boulton, 2012). Moreover, emerging public health challenges place a growing burden on the public health system (Association of Schools of Public Health, 2008). Not only current but also future public health professionals will require either basic grounding in core public health competencies, continuing education to keep abreast of evidence-based practices, or both (Gebbie & Turnock, 2006).
In 2011, 16.7% of the U.S. population was of Hispanic or Latino origin (U.S. Bureau of the Census, 2012). A 2008 survey of 2,794 local health departments showed that while 16% of health department employees were African American (or Black) and 15% were Hispanic, only 2% of top executives in local health agencies classified themselves as anything other than “White, non-Hispanic” (National Association of County and City Health Officials, 2010). In 2010, Hispanics were grossly underrepresented among public health graduates: 8% of graduates of the 46 U.S. schools of public health were of Hispanic origin, compared with 16% of the U.S. population (Association of Schools of Public Health, 2012). Available evidence suggests that while underrepresented minorities are being hired to fill public health vacancies, they are not prepared for highly technical jobs and thus tend to occupy lower level positions (Mitchell & Lassiter, 2006).
The Council on Linkages Between Academia and Public Health Practice (2010) has detailed core competencies for public health professionals at three levels or tiers: Tier 1 (entry level), Tier 2 (supervisors and managers) and Tier 3 (senior managers and executives). CoL competencies reflect the skills desirable for public health practice and are a starting point for assessing and meeting workforce training and development needs. The competencies include (1) analytical/assessment skills, (2) policy development and program planning skills, (3) communication skills, (4) cultural competency skills, (5) community dimensions of practice skills, (6) public health science, (7) financial planning and management, and (8) leadership and systems thinking (Council on Linkages Between Academia and Public Health Practice, 2010).
Method
This cross-sectional study employed a self-administered survey to collect data from employees of the Florida Department of Health and the regional and central offices of the Puerto Rico Department of Health. Although clerical staff were excluded from participation in Puerto Rico, all active state department of health employees, permanent and temporary, were eligible to participate in Florida.
Instruments and Procedures
Survey development was a collaborative effort involving investigators at Florida International University, the University of South Florida, and the Florida Department of Health, Office of Workforce Development. Survey items were taken from previous needs assessment surveys. The questionnaire was pretested in English and Spanish at the Florida Department of Health, Florida International University, and the University of South Florida, resulting in rewording of some questions. The final instrument inquired about demographic characteristics, training needs and preferences, and self-perceptions of public health competencies by career level (entry-level [Tier 1], mid-level [Tier 2], and supervisory-level [Tier 3]). The survey instrument distributed in Florida had six parts: (1) experience in public health, (2) perception of competence for public health professionals, (3) perception of competence related to public health preparedness and response, (4) capacity technology and business development, (5) demographic information, and (6) public health matters. Because the full battery of CoL competencies contains 72 items, a three-round Delphi process was conducted to pare the number of competencies to 32 to minimize respondent burden.
The instrument distributed in Puerto Rico was nearly identical to that used in Florida, the only differences being that the Puerto Rico instrument lacked Part III—Perception of Competence Related to Public Health Preparedness—and located demographic items in Part I, instead of Part V.
Surveys were administered differently in the two targeted jurisdictions because of differences in computer availability. In Puerto Rico, few public health employees had access to computers in the workplace (25.7%) or at home (17.3%), necessitating use of a pen-and-paper survey. Survey instruments were distributed at a meeting of all regional and central office directors, with each questionnaire enclosed in an envelope with a unique identification number. All surveys were anonymous. Participants were asked to return the completed questionnaire in the original envelope within a 2-week period to a specified location. The identification number was used to track the region or central office where the questionnaire was completed in order to assess survey coverage. Individuals who did not indicate whether or not they wished to participate in the study were sent reminder notices at the third and fifth weeks, using the same distribution system as the original survey. Data collection was terminated 8 weeks after initial survey distribution.
Survey data were entered manually into SPSS Statistics, Version 17, reviewed for quality control purposes, and analyzed using the SPSS software. Quality control measures included tracking the number of questionnaires distributed, completed, and entered into computer files, as well as range-checking and related procedures.
In Florida, virtually all state department of health employees (98.7%) had access to an office computer, allowing for electronic survey administration using SurveyMonkey®. The department’s director of workforce development obtained approval to distribute a link to the survey instrument to all departmental employees through work e-mail accounts. The link was e-mailed to the 17,837 employees listed in the department’s electronic personnel files on May 1, 2011, along with a statement explaining the survey’s purpose. The survey—which was only accessible from department of health computers—was open from May 3 to May 20, 2011, and a reminder e-mail was sent to all personnel on May 13, 2011. Those who elected to participate completed the anonymous questionnaire online in either English or Spanish.
Responses to all six parts of the survey instrument used in Florida were downloaded from SurveyMonkey and analyzed using SPSS Statistics, Version 17.
Ethnicity and Competencies
All Puerto Rico respondents were considered to be Hispanic. Florida respondents were asked, “Do you consider yourself to be of Hispanic, Latino, or Spanish origin? If yes, is it Mexican, Mexican American, or Chicano; Puerto Rican, Cuban, or another (please specify).” Anyone answering “yes” was considered to be Hispanic.
Public health competencies were assessed using the 32 items taken from CoL public health competencies. These items encompassed eight domains: (1) analytical and assessment skills, (2) policy development and program planning, (3) communication, (4) cultural competency, (5) community dimensions of practice, (6) public health sciences, (7) managerial, financial planning and human resources skills, and (8) leadership and systems thinking (Council on Linkages Between Academia and Public Health Practice, 2010). Respondents were asked to score each item on a scale ranging from 0 (not applicable for my current position) to 4 (I have advanced knowledge or skills). The numeric values under each domain were summed, and mean domain scores and standard deviations computed across respondents.
Statistical Analysis
Statistical analyses of cleaned datasets were conducted to assess results (Rosner, 2011). Comparisons were made between Hispanics and non-Hispanics only for Florida respondents. For the analysis of public health competencies, internal consistency (reliability) was determined by computing the alpha coefficient (Cronbach’s alpha) separately for Florida and Puerto Rico respondents. Cronbach’s alpha for each domain ranged from .90 to .98, indicating a high degree of internal consistency.
Results
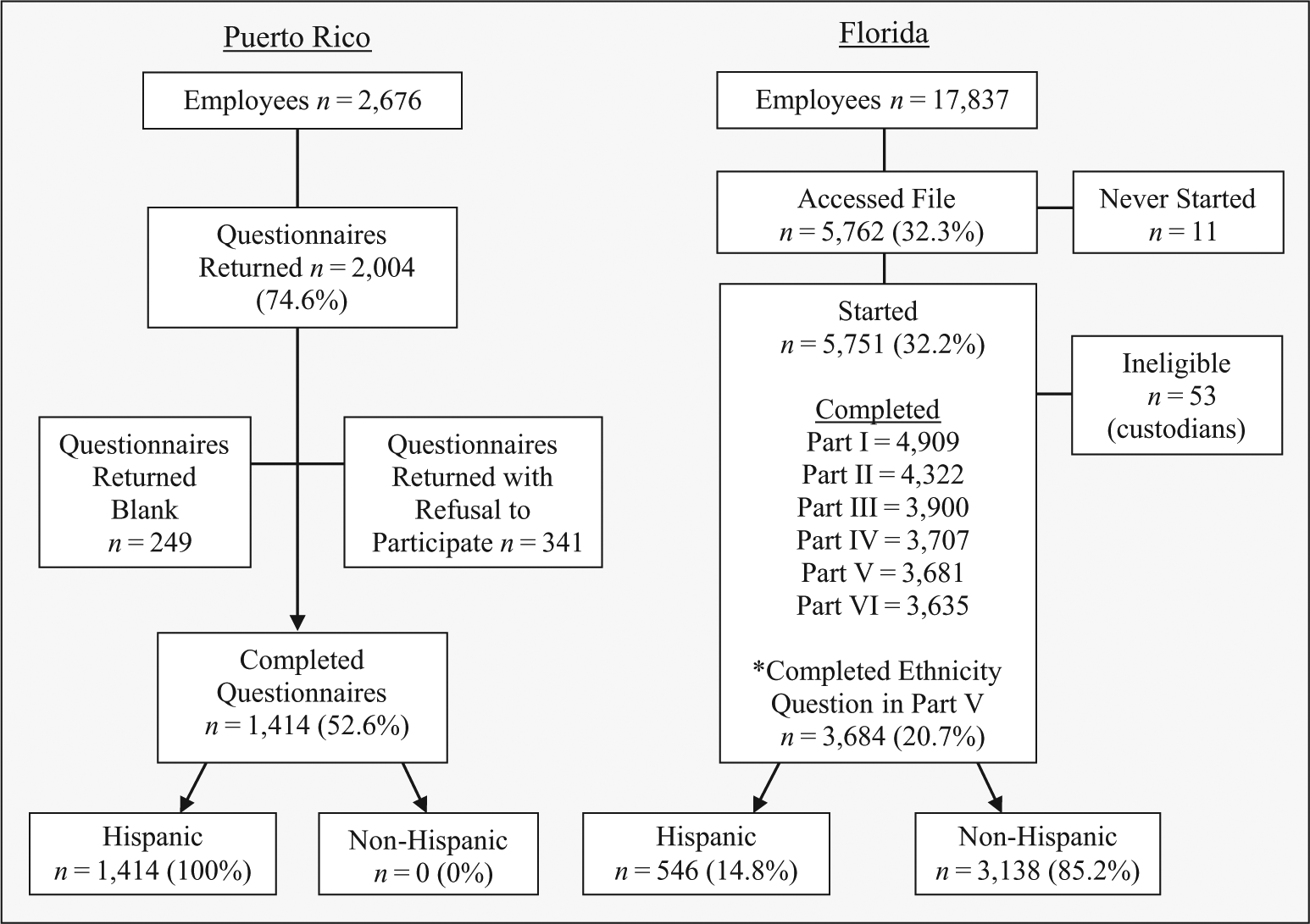
Survey instructions and questionnaires were delivered to 2,676 public health employees in Puerto Rico and sent via e-mail to 17,837 Florida Department of Health employees (see Figure 1). In Puerto Rico, 1,414 employees (52.8%) participated in the survey. In Florida, 5,762 employees (32.3%) accessed the survey. Of these, 123 (2.1%) opened the Spanish version. Most Florida participants started to fill in the questionnaire by answering at least one question, but about a third discontinued and never returned to finish the questions. Breakoffs were particularly prevalent near the beginning of the 32-item competency assessment. Among the incomplete questionnaires were 53 from individuals who reported being janitors or custodians and, thus, ineligible for public health training. These questionnaires were not included in our analysis.
Department of Health Employees in Puerto Rico and Florida
A total of 3,635 Florida respondents (20.4%) completed the entire questionnaire within the allowable 17-day period, taking an average of 28 minutes to complete the online questionnaire. A total of 3,684 respondents (20.7%) provided demographic information in Part V, including information on ethnicity. Survey analysis was based on these 3,684 questionnaires.
All Puerto Rico respondents were considered to be Hispanic; more than three quarters (78%) were female. The median age was 48 years. Just 4.8% were 29 years old or younger and 7.4% 60 years old or older. About three quarters (72.4%) were between the ages of 40 and 59 years. Almost half (48.1%) identified their highest academic credential as a bachelor’s degree, and 15.7% identified the highest credential as a master’s (10.9%) or doctoral (4.8%) degree. One third (34.3%) had been working in their current employment setting for more than 20 years. Two thirds (64.4%) had more than ten years of experience working in the Puerto Rico Department of Health. More than two thirds (69.8%) of respondents reported being in an entry-level position, and 30.3% reported being in a supervisory (28.0%) or senior-level (2.3%) position (see Table 1).
Characteristics of the Public Health Workforce in Puerto Rico (100% Hispanic) and Florida (14.8% Hispanic)
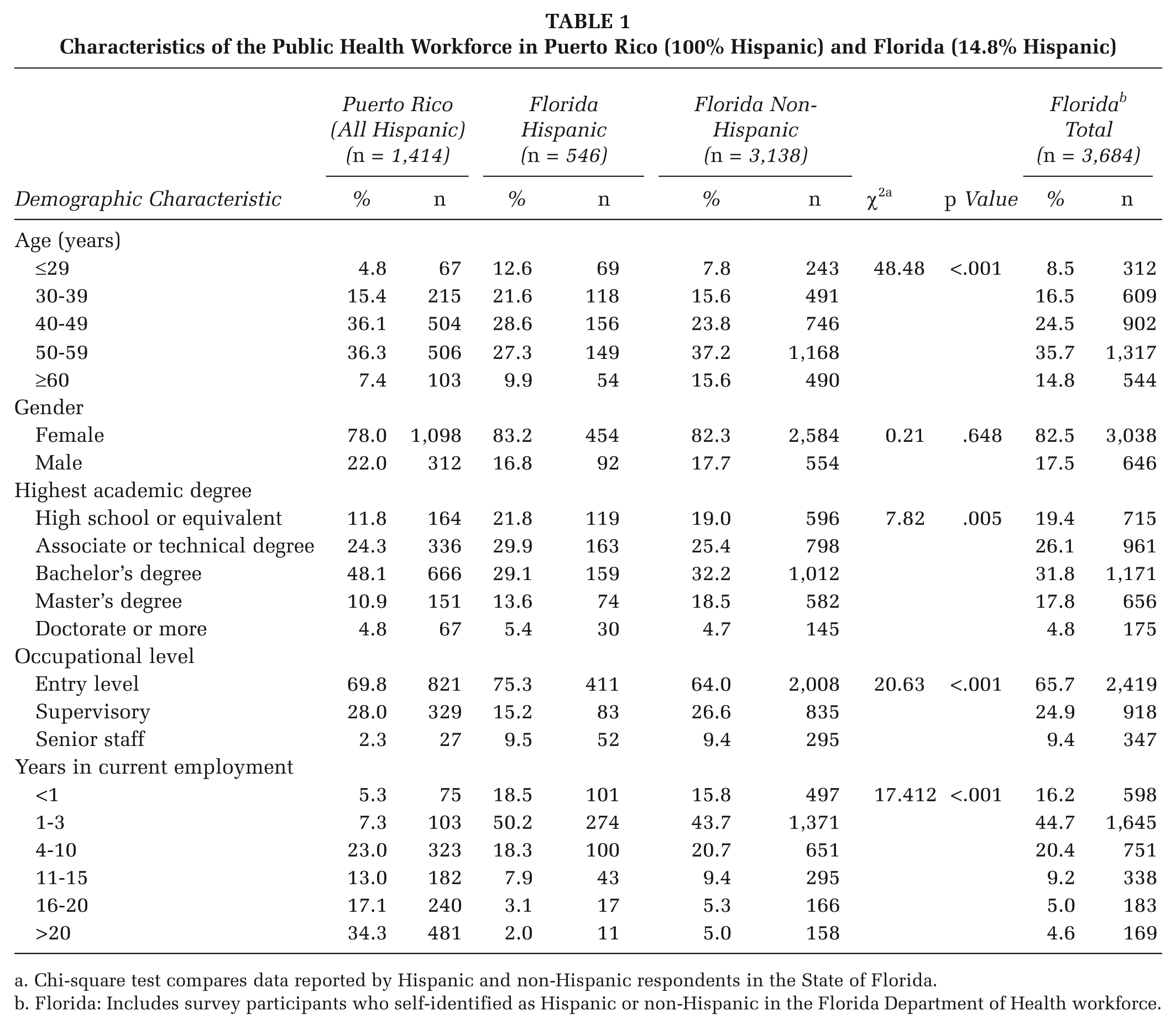
Chi-square test compares data reported by Hispanic and non-Hispanic respondents in the State of Florida.
Florida: Includes survey participants who self-identified as Hispanic or non-Hispanic in the Florida Department of Health workforce.
Florida respondents were overwhelmingly female (83.2%). Just 8.5% were 29 years old or younger and 14.8% were 60 years or older. In all, 60.2% were between the ages of 40 and 59 years. More than half (54.4%) had at least one college degree; 31.8% held a bachelor’s degree, 17.8% held a master’s degree and 4.8% held a doctorate. About two thirds (67.2%) classified themselves as entry-level staff, about a quarter (23.0%) as “supervisory or management,” and one tenth (9.0%) as “senior level.” The majority (65.1%) had between one and ten years of experience in their current employment setting; just 4.6% had more than 20 years experience and 16.2% had less than 1 year experience.
Of the 3,684 Florida Department of Health employees whose survey data were analyzed, 546 (14.8%) self-identified as Hispanic, Latino, or of Spanish origin. This Hispanic subset represents many nationalities and combinations of nationalities. The nationalities most frequently reported were Puerto Rican, Cuban, and Mexican. Hispanic employees tended to be younger (Mdn age = 45 years) than non-Hispanic employees (Mdn age = 53 years; p < .001).
Hispanic Florida respondents were slightly less likely to hold a bachelor’s or master’s degree than non-Hispanic respondents (p = .005). Overall, 29.9% of Hispanic respondents identified their highest degree as an associate or technical degree, and 29.1% identified their highest degree as a bachelor’s degree; the corresponding figures for non-Hispanic respondents are 25.4% (associate or technical degree) and 32.2% (bachelor’s degree). Just more than 20% of Hispanic employees had only a high school or high school equivalency degree, compared with 19.0% of non-Hispanic respondents. Three quarters of Hispanic respondents (75.3%) and almost two thirds of non-Hispanic respondents (64.0%) were in entry-level positions (p < .001). More than half of the Hispanic employees had 1 to 3 years of experience in their current employment setting, compared with 43.7% of non-Hispanic respondents. Fewer than 15% of Hispanic employees had more than 10 years of experience in their current place of employment, compared with almost 20% of non-Hispanics (p < .001).
Competency domain scores for Puerto Rico public health employees ranged from means of 2.01 to 2.31, low- to mid-range on a scale of 1 to 5 (see Table 2). Competency domain scores for Hispanics in Florida ranged from 2.38 to 2.88, higher than the Puerto Rican respondents, but lower than non-Hispanic Florida Department of Health employees. Among Florida participants, non-Hispanics reported greater competency in policy development/program planning, financial planning and management skills, and leadership and systems thinking skills; Hispanics reported greater skills in cultural competencies (see Table 2). However, differences in mean self-assessed competency scores were slight (generally <0.5)
Competency Domain Mean Scores and Standard Deviations for Public Health Employees in Puerto Rico and Florida
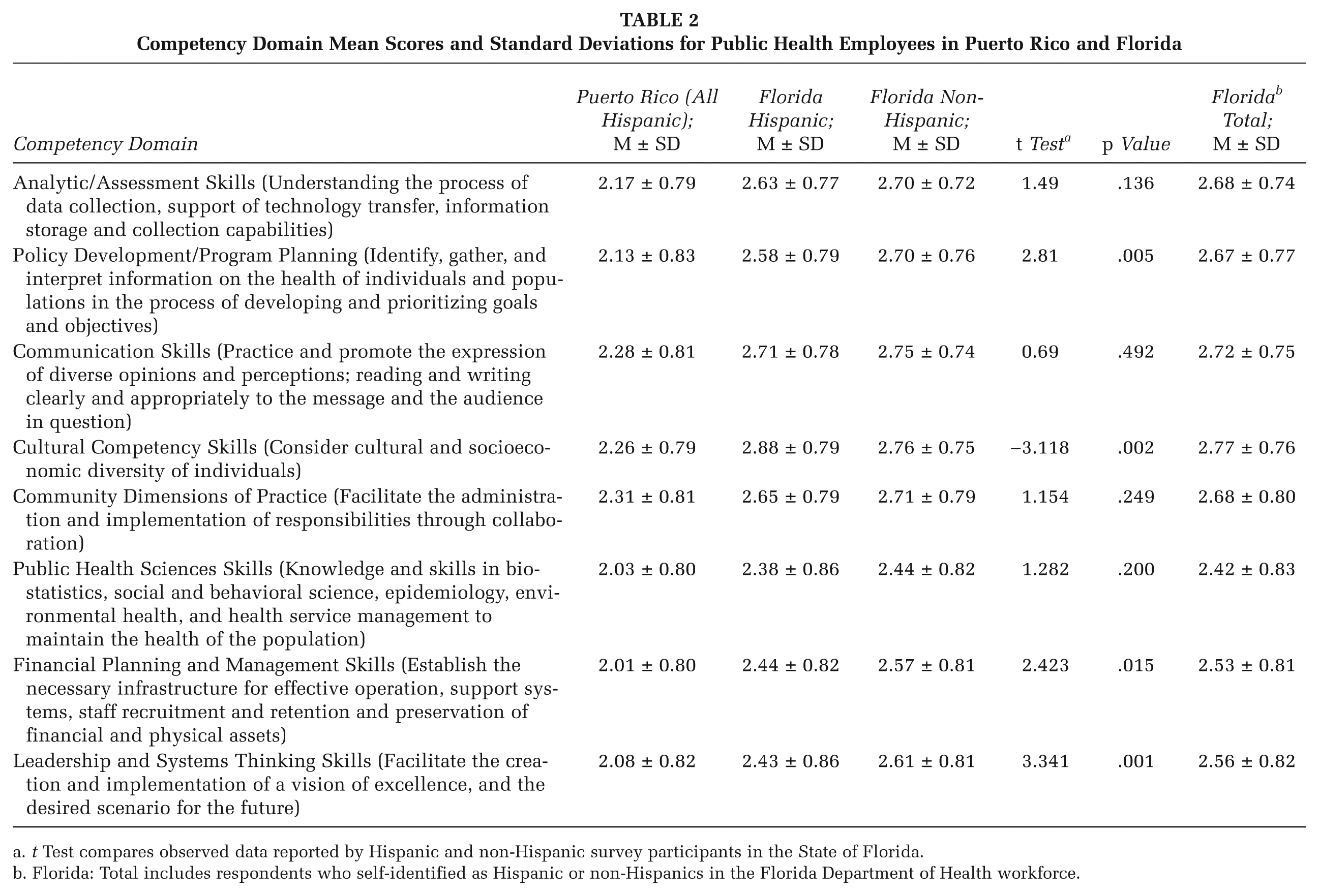
t Test compares observed data reported by Hispanic and non-Hispanic survey participants in the State of Florida.
Florida: Total includes respondents who self-identified as Hispanic or non-Hispanics in the Florida Department of Health workforce.
The primary source of public health training in Puerto Rico (42.2%) was work experience (see Table 3). The major barrier to participation in professional development activities was lack of time. Slightly more than half of the respondents (53.0%) reported having practical knowledge in the public health field. Identified areas of training need in Puerto Rico included (1) epidemic and outbreak investigations, (2) effects on the health system, (3) health promotion and disease prevention programs, (4) mental health, (5) global health, and (6) laws and policy in public health. Entry-level employees reported that their greatest weaknesses were in the public health sciences and management/financial planning. In the immediate future, the top priority was for training in COL competency areas. Face-to-face methods were by far the greatest preference in Puerto Rico (42%), which may reflect employees’ limited computer access.
Needs Assessment for Training the Puerto Rico and Florida Public Health Workforces
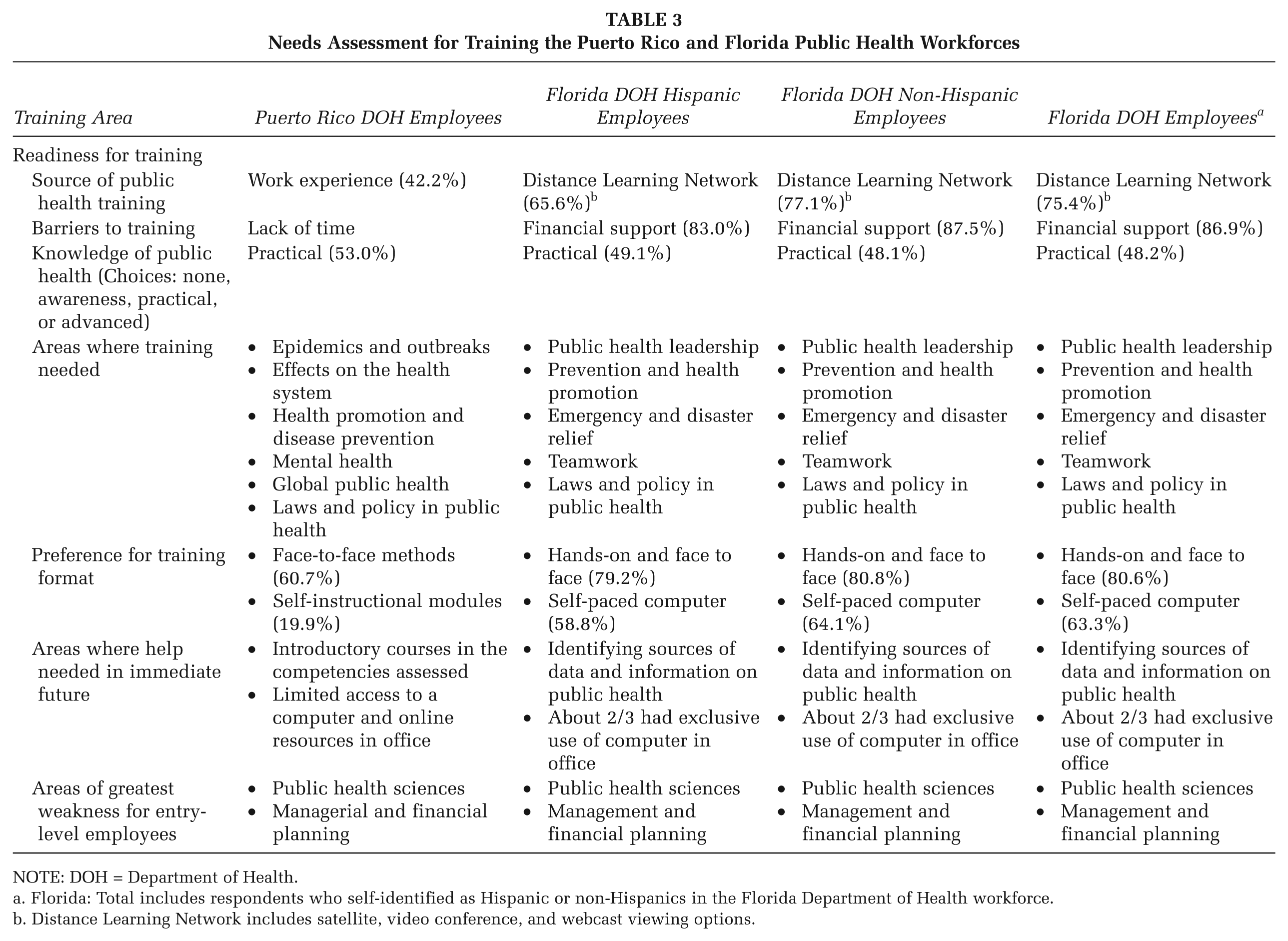
NOTE: DOH = Department of Health.
Florida: Total includes respondents who self-identified as Hispanic or non-Hispanics in the Florida Department of Health workforce.
Distance Learning Network includes satellite, video conference, and webcast viewing options.
The training readiness concerns of Hispanic Florida Department of Health respondents were similar to those of Puerto Rico Department of Health respondents (see Table 3). Florida Hispanics and non-Hispanics reported that their primary source of public health training is the Distance Learning Network, an online system available to state and local government employees in Florida. The greatest barrier to participation in professional development activities was lack of financial support. About half (49%) reported practical knowledge in public health. Self-assessed needs of Hispanics and non-Hispanics included (1) leadership, (2) health promotion and disease prevention, (3) emergency and disaster relief, (4) teamwork, and (5) laws and policy in public health. Immediate needs included identifying sources of data and information on public health. As in Puerto Rico, Hispanic and non-Hispanic entry-level Florida employees cited training in public health sciences and in management and financial planning as priority continuing education needs. Both Hispanic and non-Hispanic Florida employees indicated a preference for hands-on and face-to-face training, followed by self-paced instruction.
Discussion
The twin problems of a public health workforce shortage and underrepresentation of Hispanics in senior public health management positions can be addressed by attracting new professionals to the field and providing enhanced training for current public health employees. Surveys of public health professionals in the Puerto Rico and Florida departments of health highlight self-identified training needs and also demonstrate the relative advantages and disadvantages of two distinct evidence-gathering methodologies.
While Internet surveys provide the advantages of fast distribution and low cost (Andrews, Nonnecke, & Preece, 2003), the current study shows that pen-and-paper surveys may be advantageous in some contexts. The pen-and-paper survey administered in Puerto Rico produced a higher response rate (52.6%) than the online survey made available to all temporary and permanent Florida Department of Health employees (20.7%). The higher response rate in Puerto Rico probably resulted from the relative ease of administration of the pen-and-paper survey and the shorter survey length. A lower response rate in Florida may have resulted from the use of only one reminder—compared with two in Puerto Rico—a longer questionnaire, the placement of competency questions in tables, and, possible work distractions and time constraints (since the online questionnaire was only accessible from Florida Department of Health computers).
However, the Florida response rate is not out-of-range of rates achieved in previous surveys of public health workers. Professional characteristics of public health employees have been assessed using various self-administered survey methodologies (Aday & Cornelius, 2006). A systematic review of 17 Internet-based surveys conducted with samples of health professionals in the United Kingdom documented response rates ranging from 9% to 94% (Braithwaite, Emery, de Lusignan, & Sutton, 2003). The North Carolina Public Health Workforce Training Needs Assessment survey achieved a 67% response rate in a pilot study of local health department employees offered a paper questionnaire; then achieved response rates ranging from 42% to 95% for online versions of the questionnaire (Harrison et al., 2005). More recently, a 19-item instrument disseminated to public health employees in the state of Georgia via SurveyMonkey produced a 6% response rate (Emory Public Health Training Center & Georgia Public Health Training Center, 2011).
Despite the low response rate, our confidence in the representativeness of the Florida data is bolstered by the similarity between the demographic characteristics of Florida respondents to our survey and the demographic characteristics of those who responded to a slightly earlier Florida Department of Health survey, conducted by an independent contractor specializing in survey design and assessment methodologies (Hughes, 2011).
Results show small differences in the career levels of the survey populations. Most Puerto Rico respondents (69.8%) and most Hispanic respondents in Florida (75.3%) occupied entry-level positions, as did 64.0% of non-Hispanic Florida respondents. However, the Florida survey was open to clerical staff, while the Puerto Rico survey was not, and it is unclear how much this difference affects results; probably the percentage of entry-level workers in Florida would be lower if clerical workers had been excluded from the target audience. Nevertheless, Florida Hispanics are significantly more likely to be in an entry-level position than non-Hispanics. Just 2.3% of Puerto Rico respondents identified themselves as “senior staff,” compared with 9.5% of Hispanic Florida respondents and 9.4% of non-Hispanic Florida respondents. Likely, Puerto Rico’s smaller health agency has fewer upper echelon positions available.
Similarly, there was some difference in highest level of educational attainment. More than a third (36.1%) of Puerto Rico respondents reported having less than a bachelor’s degree compared with 51.7% of Hispanic Florida respondents and 44% of non-Hispanic Florida respondents. However, Florida Hispanic respondents were more likely to hold a master’s degree (13.6%) than Puerto Rico respondents (10.9%) and were more likely to hold a doctorate (5.4%) than either Puerto Rico respondents (4.8%) or non-Hispanic Florida respondents (4.7%).
Mean competency domain scores for both Puerto and Hispanic Florida respondents indicate relatively low to moderate competency in each of the domains. Although the competency domain scores were similar for Florida and Puerto Rico respondents, priority training needs differed. The only overlapping priority training needs are health promotion and disease prevention—ranked third among all survey groups respondents—and laws and policy in public health—ranked sixth by Puerto Rico respondents and fifth by Hispanic and non-Hispanic Florida respondents. Entry-level workers in all survey populations—including Hispanic and non-Hispanic Florida respondents—identified “public health sciences” and “managerial and financial planning” as areas of greatest weakness.
Findings suggest opportunities to augment skills in all competency domains for all survey populations. In particular, training activities that impart practical knowledge in the identified topics—ranging from public health leadership to outbreak investigation to prevention and health promotion—would best serve the training needs of Puerto Rico and Florida public health practitioners. It may be beneficial to base training on adult learning theory and to target activities to entry-level employees, who comprise the majority of respondents and who may one day advance into the positions of departing managerial and senior staff.
Conclusions
Training to address critical skill deficiencies and to help compensate for public health workforce shortages should be evidence- and competencies-based (Association of State and Territorial Health Officials, 2010, Chap. 4). The growing Hispanic population in the United States must be part of the solution to staffing shortfalls (National Hispanic Health Foundation & the Joshia Macy Foundation, 2009). Results of our needs assessment surveys—even with acknowledged threats to validity stemming from a low response rate in Florida—show pronounced gaps in knowledge and skills, including among Hispanic workers employed in the Puerto Rico and Florida departments of health. With new data available to guide inform next steps, the PR-F PHTC can begin to design and deliver courses to address the training priorities identified by survey respondents.
Footnotes
Supplement Note:
This article is published in the supplement “Public Health Training Centers,” which was supported by the U.S. Department of Health and Human Services (HHS) Health Resources and Services Administration (HRSA) through a Cooperative Agreement (UBGHP20199) to Rollins School of Public Health, Emory University.