
Abstract
New, comprehensive, approaches for chronic disease management are needed to ensure that patients, particularly those more likely to experience health disparities, have access to the clinical care, self-management resources, and support necessary for the prevention and control of diabetes. Community health workers (CHWs) have worked in community settings to reduce health care disparities and are currently being deployed in some clinical settings as a means of improving access to and quality of care. Guided by the chronic care model, Baylor Health Care System embedded CHWs within clinical teams in community clinics with the goal of reducing observed disparities in diabetes care and outcomes. This study examines findings from interviews with patients, CHWs, and primary care providers (PCPs) to understand how health care delivery systems can be redesigned to effectively incorporate CHWs and how embedding CHWs in primary care teams can produce informed, activated patients and prepared, proactive practice teams who can work together to achieve improved patient outcomes. Respondents indicated that the PCPs continued to provide clinical exams and manage patient care, but the roles of diabetes education, nutritional counseling, and patient activation were shifted to the CHWs. CHWs also provided patients with social support and connection to community resources. Integration of CHWs into clinical care teams improved patient knowledge and activation levels, the ability of PCPs to identify and proactively address specific patient needs, and patient outcomes.
Keywords
Background
Diabetes mellitus is a growing epidemic in the United States, affecting approximately 25.8 million individuals (Centers for Disease Control and Prevention, 2011). In particular, individuals of minority and low socioeconomic status suffer a disproportionately high risk for diabetes morbidity and mortality (Centers for Disease Control and Prevention, 2011; Heisler et al., 2009). New, multifaceted, systems-based approaches for chronic disease management are needed to ensure that patients, particularly those more likely to experience health disparities, have access to the clinical care, self-management resources, and support necessary for the prevention and control of diabetes.
The chronic care model (Figure 1) was developed by Wagner (1998) to promote high-quality patient-centered care. Wagner (1998) asserted that effective disease management programs are delivered in partnership with health care systems and communities and recognized that traditional primary care models were designed to treat acute illness rather than provide chronic care. As a result, many patients are not adequately taught to care for their own illness, primary care visits are too brief to address chronic conditions, and physicians do not have support staff trained in chronic disease management; all these factors lead to unproductive clinical visits between uninformed patients and an unprepared practice team (Bodenheimer, Wagner, & Grumbach, 2002). The goal of the chronic care model is to transform care for patients with chronic illness from reactive to proactive and improve the delivery of ambulatory care (Coleman, Austin, Brach, & Wagner, 2009). The model emphasizes health care delivery redesign, self-management support, and access to community resources as essential elements for the provision of comprehensive chronic care. The incorporation of these elements can help patients become more engaged in their care and ensure that providers are prepared to address patient needs, resulting in more productive interactions between patients and providers and improved patient outcomes.
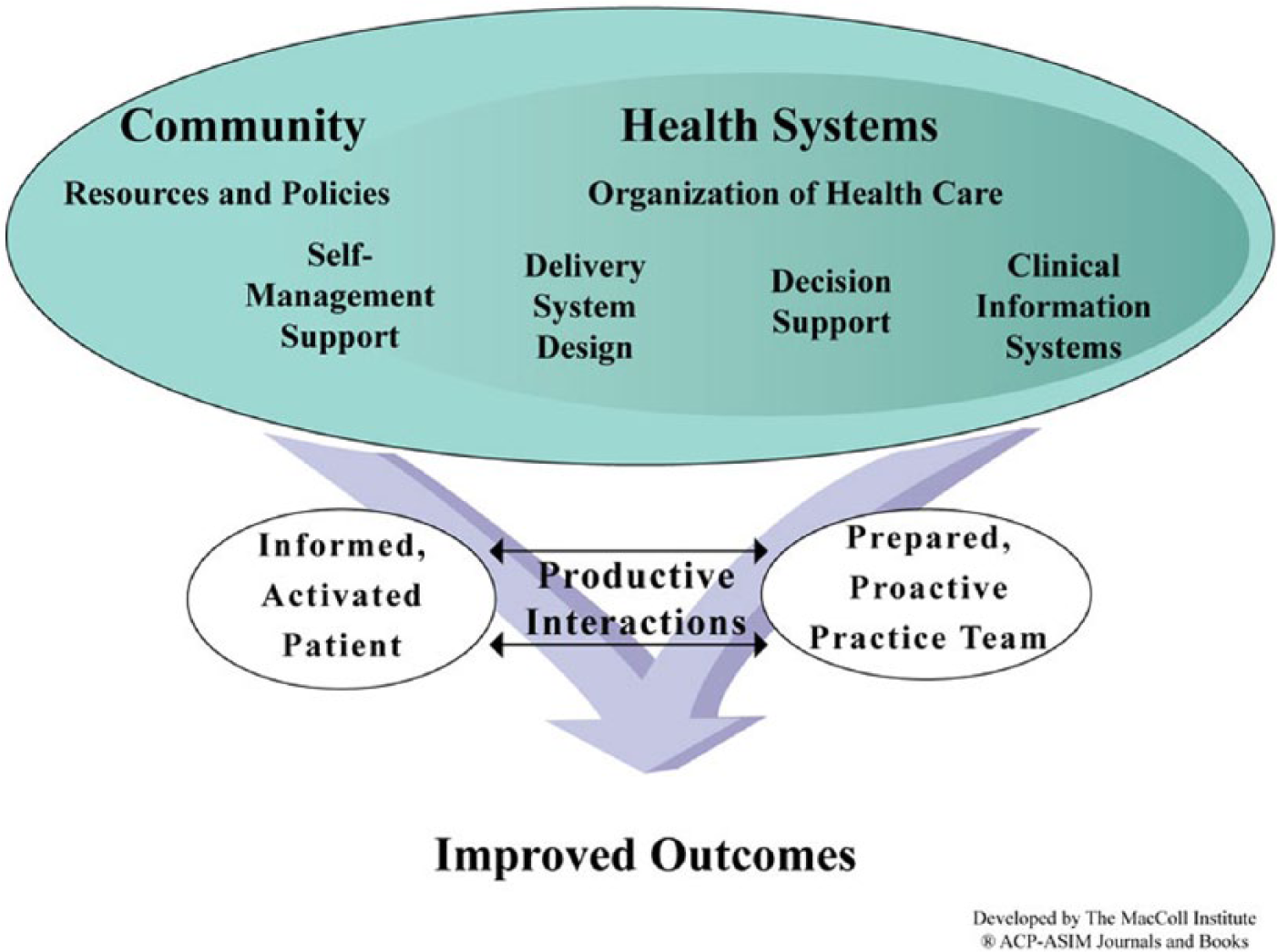
Theoretical Framework: The Chronic Care Model (Wagner, 1998)
Although the chronic care model provides a framework for improving chronic disease management, it does not offer specific solutions as to how to effectively redesign care in order to incorporate the essential elements of the model (Coleman et al., 2009). The use of community health workers (CHWs) has been advocated as a means to bridge the multiple components of the model, particularly the community component (Cherrington, Ayala, Amick, Allison, et al., 2008). CHWs are trusted members of the community who typically share the same ethnic, linguistic, or cultural background as patients (Ferguson, Lemay, Hargraves, Gorodetsky, & Calista, 2012). CHWs have been working within communities to improve health for more than 60 years and have demonstrated effectiveness in managing chronic disease. Several studies have indicated that CHW-led diabetes interventions improve health indicators such as glycated hemoglobin (HbA1c), blood pressure, lipid levels, and weight, (Babamoto et al., 2009; Brown, Garcia, Kouzekanani, & Hanis, 2002; Prezio et al., 2013; Spencer et al., 2011) and are associated with reduced health care utilization in terms of emergency room visits and hospital admissions (Fedder, Chang, Curry, & Nichols, 2003; Lorig, Ritter, & Gonzalez, 2003; Skelly, 2010; Whitley, Everhart, & Wright, 2006).
Embedding CHWs into primary care teams is a way to redesign health care delivery systems to assist patients with chronic disease care and connect them to community resources essential for disease management. The chronic care model emphasizes the need for delivery system redesign, including the formation of primary care teams with nonphysician staff who can provide patients with self-management support—tasks that physicians may not have the time or training to adequately provide (Bodenheimer et al., 2002). The rationale for incorporating CHWs into care teams is that they are able to build trusting relationships with patients based on their shared backgrounds and experiences, effectively link underserved populations to health care resources, and serve as a bridge between patients and providers through the communication of patient barriers to care (Allen et al., 2011).
Several studies have examined the use of CHWs to assist patients with diabetes management. In a 2006 systematic review, Norris et al. (2006) found that CHWs were used in a variety of roles in diabetes programs including patient care, education, care coordination, and social support; there was also some evidence that CHWs could improve patient knowledge and satisfaction. Although a few studies in the review included CHWs as members of primary care teams (Gary et al., 2004; Humphry, Jameson, & Beckham, 1997; Keyserling et al., 2002), these studies provided little detail regarding how to effectively redesign health care delivery systems to incorporate CHWs into the workforce. Norris et al. (2006) recognized the need for further research to determine optimal roles for CHWs in diabetes care, examine physicians’ and nurses’ views and expectations of CHWs, explore health care system barriers to implementation, and recommend strategies for integrating CHWs into health care teams.
A few recent studies have attempted to fill gaps in knowledge pertaining to the use of CHWs as members of clinical teams (Hargraves, Ferguson, Lemay, & Pernice, 2012; Otero-Sabogal et al., 2010). These studies assessed the extended roles of CHWs working within a primary care clinical team on patients’ diabetes self-management skills and clinical outcomes. One study noted improvements in patients’ glycemic control, cholesterol, and self-management outcomes, whereas another noted improvement in self-management goal setting. Otero-Sabogal et al. (2010) indicated that the successful deployment of this intervention required CHWs to undergo intensive training in diabetes and patient self-management techniques. Hargraves et al. (2012) found that CHWs needed to have a defined role within the care team. Although these studies provided valuable information regarding the incorporation of CHWs into clinical teams, more information is needed regarding how to redesign health care delivery systems to support the provision of care for diabetes and other chronic diseases and connect patients to community resources essential for ongoing disease management.
Guided by the chronic care model with an emphasis on delivery system redesign, Baylor Health Care System (BHCS) in Dallas, Texas, created the Diabetes Equity Project (DEP), a 5-year program supported with funding from a Merck Foundation grant, with the goal of reducing observed disparities in diabetes care and outcomes in the medically underserved communities surrounding BHCS hospitals. The program features specially trained, bilingual CHWs who serve as members of primary care teams in five community clinics and deliver a culturally relevant diabetes self-management and education curriculum targeting barriers to diabetes management commonly experienced by Hispanics. We have previously reported findings from our preliminary analysis of DEP clinical data and interviews with CHWs and primary care providers (PCPs) indicating that patients had a statistically significant reduction in mean HbA1c levels 1 year postbaseline and that CHWs and PCPs were able to work together effectively to improve patient care (Collinsworth, Vulimiri, Schmidt, & Snead, 2013; Walton, Snead, Collinsworth, & Schmidt, 2012). This qualitative study builds on that work by examining findings from patient, CHW, and PCP interviews to understand how health care delivery systems can be redesigned to effectively incorporate CHWs and how embedding CHWs in primary care teams can produce informed, activated patients and prepared, proactive practice teams.
Method
Setting
This study was conducted in five community clinics located throughout the Dallas metroplex. Primary care team personnel varied among the sites and included physicians, nurse practitioners, and medical assistants. None of the sites employed certified diabetes educators. The medical assistants were responsible for patient check-in, point-of-care testing, and follow-up calls.
DEP Intervention
The DEP began in 2009 with the hiring of the program manager and recruitment of the CHWs. As described previously, we created an official job description for the CHWs; position requirements included a high school diploma and fluency in Spanish, with a medical assistant background strongly preferred (Walton et al., 2012). Four of the five CHWs hired for the DEP were medical assistants; the fifth had a bachelor’s degree in community health. All five were Hispanic, female, and between the ages of 23 and 35 years and had 0 to 5 years of experience as CHWs. Once hired, all CHWs were required to complete the 160-hour Texas CHW Training and Certification Program and an additional 50 hours of instruction pertaining to diabetes management. The CHWs reported to the offsite nurse manager but worked under the direction of primary care clinicians to assist DEP patients with diabetes management through education and support services. CHWs reduced the workload of the medical assistants by providing point-of care testing for diabetes-related measures and follow-up calls for DEP patients.
During the first 18 months (September 2009 to March 2011) of the DEP, 806 patients enrolled. All patients were uninsured, and the majority were female (60%), between 40 and 59 years of age (64%), and Hispanic (70%). Mean Hba1c for DEP patients decreased significantly between baseline (8.7%) and 1-year follow-up (7.3%; p < .00; Collinsworth et al., 2013). Patients also experienced a statistically significant decrease in systolic blood pressure between baseline (129.8 mmHg) and 1-year follow-up (127.3 mmHg; p =.03). No statistically significant differences in body mass index or diastolic blood pressure were observed.
Interviews
Semistructured in-person and phone interviews were conducted by two of the researchers with all five DEP CHWs and a convenience sample of 12 DEP patients and seven of the PCPs (six physicians and one nurse practitioner). The CHWs recruited DEP patients who had scheduled visits during the interview period. The PCPs were recruited by the DEP program director. The sample included at least one PCP from each of the five DEP sites. CHWs were interviewed in October of 2011, and the patients and PCPs were interviewed in June and July of 2012.
All interviews were conducted using open-ended interview guides (see Appendixes A, B, and C). We developed separate guides for the CHWs, PCPs, and the patients. The CHW guide contained 20 questions regarding CHW roles and responsibilities in the delivery of the DEP intervention and within a health care system’s care coordination strategy. Similarly, the PCP guide contained 17 questions regarding the role CHWs play in improving diabetes-related outcomes for patients, how CHWs function within a clinical team, and how providers felt about working with the CHWs. The patient interview guide contained questions related to the patients’ experience with diabetes, the role CHWs played in helping them manage diabetes, and their satisfaction with the care provided by the CHW. All interview guides were written in English. The patient interview guide was translated into Spanish.
Interviews lasted approximately 30 to 45 minutes and were conducted in English with the CHWs and PCPs and in English or Spanish with the patients, based on patient preference. CHW responses were transcribed verbatim. The PCP and patient interviews were recorded and transcribed. All interviews conducted in Spanish were translated into English for analysis. The researchers used thematic content analysis to analyze the contents of the interview using both preset and emerging codes. The researchers grouped the responses from CHWs and PCPs by codes to identify frequency and patterns of responses and reoccurring themes.
Results
How Health Care Delivery Systems Can Be Redesigned to Effectively Incorporate CHWs
The PCPs and CHWs indicated they work together to ensure that all of the patients’ chronic care needs are met. The PCP provides patients with a clinical exam including diagnosis and treatment plans. CHWs said they provided diabetes management support, connections to community resources, and coaching and social support and served as a bridge between patients and PCPs. They emphasized that their main task was providing diabetes self-management education to the patients, including nutritional counseling, exercise promotion, and assessment of medication compliance. Patients said that CHWs educated them about diabetes and provided them with coaching and social support. One patient explained, “She is my counselor. She gives me advice.”
The providers felt that the CHWs saved them time by performing basic clinical assessments and maintaining frequent contact with patients to identify health concerns. One PCP explained, She generally sees the patients at least every three months. [She] follows up, keeping up with their A1c, educating them regarding their diet and their medicine and treatment regimen. She keeps us informed of what’s going on with them, any changes in their condition.
All PCPs indicated that one of the CHWs’ most important responsibilities was to assess patient-specific barriers to diabetes care and communicate these barriers to the physician. One PCP commented, “[The CHWs] help surface what are the big barriers . . . is it that the person is really depressed, or is this person afraid of insulin?” The PCP and CHW then work with the patient to overcome barriers. The enhancement of clinic services through the incorporation of the CHW and the shifting of roles from PCPs to CHWs to improve the delivery of care are depicted in Figure 2.
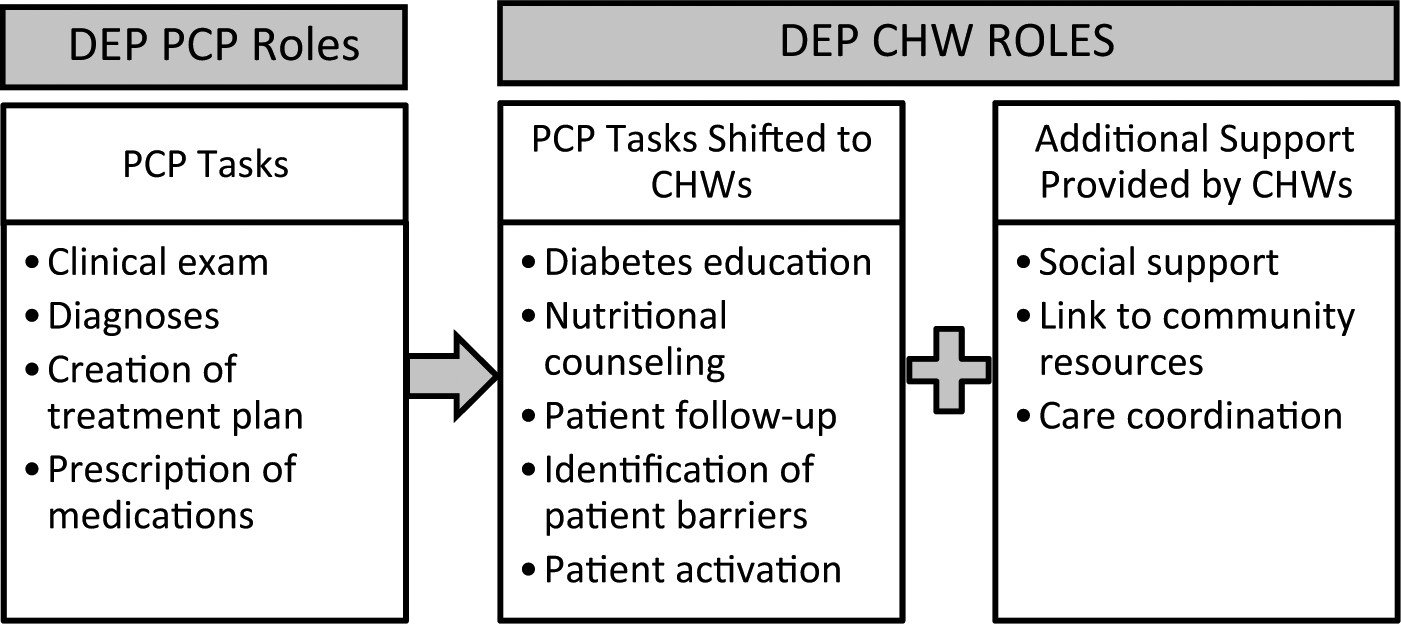
Redesign of Primary Care: Shifting of Roles From PCPs to CHWs
PCPs said that for CHWs to function as members of the clinical team, they must be able to work independently, yet recognize when a clinician needs to be involved. CHWs must feel comfortable communicating with physicians through various channels, including face-to-face communication and electronic health record notes. All PCPs indicated that the CHWs seemed comfortable communicating with them. A PCP explained, Typically if there is an area of concern, something abnormal on physical exam, someone with a sore on their foot, or if they’re having problems with really high or low sugar, anything out of the norm, she’ll either come find me physically to take a look at the patient while they are there or she will send me a note on the electronic medical record.
The CHWs and PCPs recognized the importance of having a trusting relationship. Some CHWs indicated that it took a year of working together to establish this trust. PCPs said they gained trust in the CHWs as they recognized their many competencies and saw the positive impacts of the intervention on patients. After recognizing the value of the CHWs, PCPs sought to provide the CHWs with “plenty of support” in terms of addressing patients’ clinical needs and helping CHWs deal with challenging situations.
How Embedding CHWs in Primary Care Teams Can Produce Informed, Activated Patients and Prepared, Proactive Practice Teams
Figure 3 depicts how the insertion of CHWs into primary care practices can help produce informed, activated patients and prepared, proactive practice teams. Patients indicated that CHWs were effective in educating them about diabetes, and many claimed that they had not understood the nature and seriousness of diabetes until they met with the CHW. One patient explained, “She’s teaching me how to take care of my body with diabetes. This is something I never had. I had it and didn’t know it. Now, she’s explaining it to me, how to work it, how to control it.” Another patient commented, “She taught me stuff like measuring my food, small portions . . . how to check my feet.”
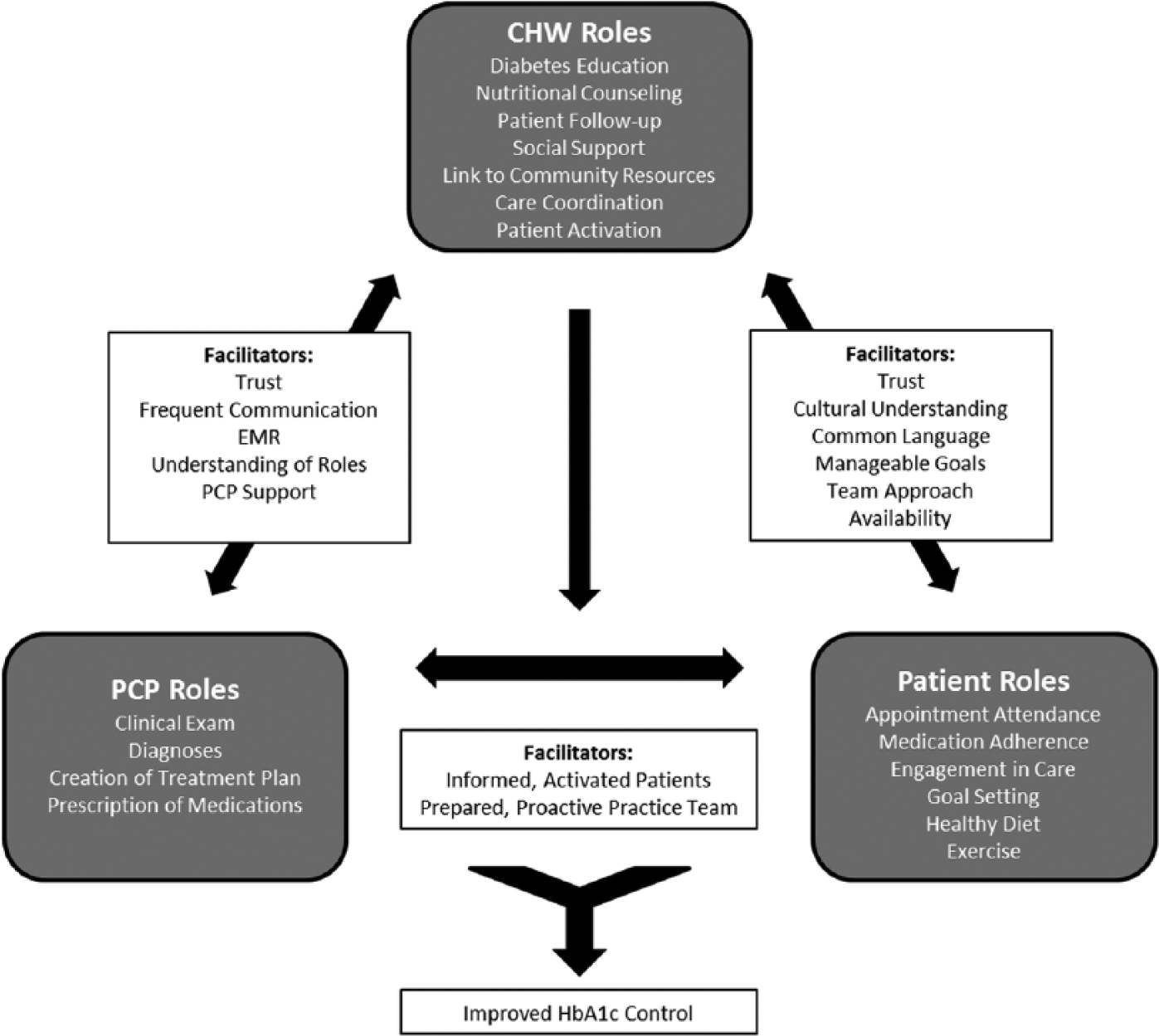
Use of CHWs in Primary Care Practices to Help Patients Achieve Improved Glucose Control
CHWs helped patients become activated and recognize that they must be responsible for improving their health. As one patient explained, “You gotta want to help yourself. They can give you all the tools and information you need, but unless I do my part I won’t get better.” Another patient explained, “Because of your illness, they give you guidelines to control it. But I had to be an active part of my healing process.” Patients said CHWs helped them set attainable goals. One patient explained, “She sets the goals. Small goals, what can you do. Like to run, to exercise, to improve.” Many patients reported that as a result of the CHW’s help, they had lost weight, increased their levels of physical activity, and experienced improved glycemic control.
CHWs also helped patients actively manage their diabetes and achieve glycemic control by providing them with resources or connecting them to community resources that could help them overcome barriers to diabetes management. One CHW explained, “I try to help with resources. A lot of patients say I don’t take my medications because I can’t afford it. We provide them with samples.” Several patients indicated that the CHWs had referred them for free counseling for depression, eye exams, medications, and diabetes testing strips.
PCPs felt that the DEP model was successful because it placed CHWs within the clinics allowing the PCPs and CHWs to work together as a team to identify patient barriers to diabetes management. As one PCP explained, “[The CHW] is very good at drawing things out of patients and making them feel very comfortable.” Another PCP commented, “[Patients] are not going to tell the doctor everything especially if Spanish is not his primary language.” Patients indicated that CHWs were able to bridge the gap between them and the providers by talking to them on a level they understood, understanding cultural barriers, and patiently answering questions. As one patient explained, “She helps me have a more open relationship with my doctor.” Another patient added, “[With the CHW], you can be part of the conversation in deciding your health.” A third patient explained, “There are no stupid questions—she doesn’t make you feel that way. She gives you the confidence to ask what you want to ask.”
Discussion
Our findings demonstrate how CHWs can help patients achieve improved diabetes control through health care delivery system redesign, self-management support, and connection to community care resources as outlined by the chronic care model. We incorporated CHWs into clinical care teams by creating official job descriptions, providing office space for them within clinics, giving them access to the electronic health record, and helping them build rapport with clinicians through effective communication and the delivery of high-quality care. Use of CHWs to assist patients with diabetes management appears to have improved patient knowledge and activation levels as well as the ability of PCPs to identify and proactively address specific patient needs. Patients and providers reported that CHWs improved the delivery of care and patient outcomes.
Many public health professionals, health organizations, and policy makers have recommended that the health workforce be expanded through the integration of trained health workers, such as CHWs, who have different levels of qualifications from physicians and nurses. However, few studies have tested this model or described how to integrate and sustain it in primary care practices. This study is unique in that it examines the perspectives of patients, CHWs, and providers regarding this new model of care, provides clarification regarding the specific roles of CHWs and PCPs within the model, and offers insight as to how this model improves health outcomes such as glycemic control.
Similar to the findings observed by Otero-Sabogal et al. (2010) and Hargraves et al. (2012), we found that CHWs could be integrated into primary care practices and effectively perform roles in diabetes management typically performed by physicians and other clinical staff. In the DEP model, the roles of diabetes education, nutritional counseling, and patient activation and follow-up that typically fall to the PCP in traditional care models were shifted to the CHW. CHWs also provided patients with enhanced care through social support, connection to community resources, and care coordination services. These tasks have typically been performed by CHWs in community settings. By embedding CHWs within primary care clinics, the DEP links clinical care to community support services, the two crucial components of Wagner’s chronic care model, and provides patients with comprehensive care and diabetes management (Cherrington, Ayala, Amick, Scarinci, et al., 2008).
The key to the success of the DEP in improving patients’ glycemic control ultimately may be the CHWs’ ability to improve patient activation. Many patients indicated that the CHWs taught them to assume responsibility for improving their own health by showing them how to set small, attainable goals and providing support. CHWs may be better positioned than other care providers to improve patient activation due to the shared cultural background, community connections, and trust between CHWs and patients.
This study has several limitations. The DEP was implemented in community clinics that serve uninsured patients and have constrained resources. As a result, study findings may not be generalizable to clinics serving other populations and with staffing models that include other disease management specialists such as diabetes educators. Interprofessional collaboration between CHWs and other health care professionals is likely to be more difficult in clinics that employ a mix of personnel. Boundary infringements, a lack of understanding of roles, and poorly coordinated teamwork could cause friction between team members and negatively affect the delivery of care (Reeves et al., 2008). The interviews were conducted as part of a program evaluation, and we used a convenience sample of patients and providers, which may have resulted in a selection bias. Informants may have been biased as to the success of the program or hesitant to reveal their true feelings about the DEP.
Conclusion
Our experience demonstrates that health care systems can be redesigned to incorporate CHWs as high functioning members of clinical teams and improve patient outcomes as described by the chronic care model. We recognize that incorporating CHWs in primary care practices may improve patient care and outcomes and facilitate efficient delivery of care, but this model of care requires development of supporting infrastructure to be effective. We have previously discussed infrastructure needed to support CHWs such as appropriate training, designated roles, support of clinical staff and infrastructure, and sustainable funding sources (Collinsworth et al., 2013). The use of CHWs in primary care is a viable way to transition care in the United States to a population health management model as promoted in the Affordable Care Act. Embedding CHWs into primary care practices appears to work well in clinics with limited resources serving uninsured populations, but it is not clear if this model can be expanded to traditional fee-for-service practices. Further research demonstrating the generalizability of this team approach to primary care and its cost-effectiveness may accelerate the adoption of CHW models of care.
Footnotes
Appendix A
Appendix B
Appendix C
Supplement Note:
This article is part of a journal supplement entitled “The Alliance to Reduce Disparities in Diabetes: Infusing Policy and System Change with Local Experience.” The supplement was supported by a grant to the Society for Public Health Education from the Merck Foundation. The Merck Foundation had no role in the development, writing, editing, review, or approval of the content of any of the articles in this issue.