
Abstract
This article reports on a social marketing campaign directed toward high-risk men who have sex with men in Toronto and Ottawa to encourage testing for HIV and syphilis; improve knowledge about HIV transmission, seroconversion symptoms, and the HIV window period; and heighten awareness of syphilis transmission and its relationship to facilitating HIV transmission. Evaluation data were collected from a large-scale online pre-and postcampaign survey of sexually active men who have sex with men and from laboratory testing data. Men who turned up to be tested also filled out an exit survey. The campaign websites attracted some 15,000 unique visitors, 54% of whom had an IP address in Toronto or Ottawa. Laboratory data showed a 20% increase in HIV testing in Toronto over the campaign compared to the previous year. The overall rate of HIV-positive tests remained relatively constant. Knowledge levels about seroconversion symptoms, sexually transmitted infection and HIV transmission, and the HIV window period were significantly better among postcampaign survey respondents aware of the campaign compared to postcampaign respondents who were not aware and compared to precampaign respondents.
Introduction
With HIV transmission rates among gay, bisexual, and other men who have sex with men (MSM) at a plateau or even increasing in the advanced industrial nations, there is renewed concern about encouraging them to test for HIV. Perhaps as many as half of new HIV infections among MSM are being transmitted from those who are unaware of their own infection (Birrell et al., 2013; Brenner et al., 2008). Testing is the first step in linking people who test HIV-positive to care and in reducing onward transmission, as risk behavior may change after people become aware of their infection, and antiretroviral treatment works to reduce viral load and thus infectivity. Studies of unprotected sex among MSM show that HIV risk is unevenly distributed across the population: Many men have one or no partner over the long term; many others consistently practice safe sex. A minority of MSM have occasional or repeated unprotected anal or vaginal intercourse (UAVI) with partners whose HIV status is positive or unknown. Given good knowledge of the basics of HIV prevention among MSM, it appeared to be time to move beyond simple exhortations to test in order to (1) encourage high-risk men in particular to test for HIV and syphilis; (2) improve knowledge about HIV transmission, seroconversion symptoms, and the HIV window period; and (3) heighten awareness of syphilis transmission and its relationship to facilitating HIV transmission.
Systematic reviews of social marketing of HIV prevention messaging show “demonstrated effects on behavior or behavioral intentions” when grounded in “formative research on and about the target audience,” a theory of social behavior change, and culturally appropriate messaging and communication channels (Noar, Palmgreen, Chabot, Dobransky, & Zimmerman, 2009). Social marketing campaigns directed specifically to MSM to promote HIV or syphilis testing have a less developed research tradition and a record of mixed success (Vega & Roland, 2005). An HIV testing campaign in London aimed at young gay men of Black or South European origin significantly raised testing rates among the intended population (McOwan, Gillece, Chislett, & Mandala, 2002), and a syphilis awareness campaign in Los Angeles County significantly increased syphilis testing rates among MSM aware of the campaign, which the authors attribute to “market research, audience segmentation, and building a strong brand” (Plant et al., 2010, p. 12). A San Francisco syphilis awareness campaign succeeded in raising syphilis testing rates among only HIV-positive men who recalled the campaign (Stephens, Bernstein, McCright, & Klausner, 2010). One major campaign conducted in Victoria, Australia, showed a significant increase in HIV, syphilis, and chlamydia testing among those aware of the campaign (Pedrana et al., 2012), but an earlier campaign in the same state was unable to raise HIV testing rates (Guy et al., 2009). The difference between the two may be due to the larger scale and multiple channels employed in the later campaign (Pedrana et al., 2012). A campaign in Washington state that measured not only testing but also seroconversion rates sought “to teach HIV-negative MSM the symptoms of AHI [acute HIV infection] . . . [but] had no apparent impact on the number of HIV-infected MSM diagnosed during AHI,” though it did improve symptom awareness (Stekler, Baldwin, Louella, Katz, & Golden, 2013).
Method
A working group of researchers, clinicians, community members, and health ministry staff met to organize a social marketing campaign in order to reach a broad range of MSM in local communities. It was subsequently launched with support of the AIDS Bureau of the Ontario Ministry of Health and Long-term Care, the Ontario HIV Treatment Network, and public health partners. Running from October 2011 to March 2012, it was based in Toronto and Ottawa, the two cities that account for 82.8% of HIV diagnoses among MSM in Ontario (Remis & Liu, 2011). With previous research on the target audience showing that the leading reason for not having an HIV test was perceiving oneself as “at low risk” (Myers et al., 2011, p. 87), the Ontario campaign was developed to heighten the personal relevance of testing for HIV and syphilis, a key element of persuasive messaging (Devos-Comby & Salovey, 2002). In particular, the media campaign intended to impart the following five messages:
Unprotected anal intercourse with an HIV positive partner or a partner of unknown status is a high-risk activity.
Symptoms such as fever, night sweats, or body rash may be signs of recent HIV infection.
An accurate HIV test result may take up to 3 months; however, early testing technologies are available.
Having a sexually transmitted infection (STI) facilitates HIV transmission.
With syphilis rates rising among MSM, syphilis should be tested along with HIV.
The campaign was developed with a professional marketing agency and centered on a cartoon figure, dubbed “Casey,” who experiences flu-like symptoms after having unprotected sex (see Figure 1). The imagery and message were reviewed for acceptability by a diverse set of focus groups of gay men before being promoted through a dedicated campaign website, posters and wall projections in gay neighborhoods in Toronto and Ottawa, banners for the testing clinics, advertisements on websites oriented to gay men, newspaper and magazine ads, ads on the gay radio station (Proud FM), walking billboards at gay community events, giveaway cards from walking billboards, and postings on construction site barricades, on building façades, and in alleyways. In common with successful social marketing campaigns reported in the research literature, this one grounded itself in recent research on the local population, was tailored to sexually active MSM, and promoted recognizable branding across several platforms.

Testing Campaign Image
In addition, the Hassle Free Clinic in Toronto supplemented the main social marketing approach with social media outreach via Facebook and notices posted on Craigslist and gay.com in accord with past practice of messaging to at-risk audiences. Media messaging directed people to the English- and French-language campaign websites, www.come-on-in.ca and viens-nous-voir.ca, respectively. As well as providing information on testing clinic hours and locations, the site provided detailed information on the campaign’s key messages and additional resources.
Regular testing sites in Toronto and Ottawa extended their hours, and supplemental point-of-care testing sites were opened during the campaign; in all, there were nine testing sites in Toronto and three in Ottawa. All clinics were drop-in, where clients did not have to make an appointment. Two primary questions were posed to assess the campaign’s objectives: (1) Did the campaign attract high-risk MSM to be tested for HIV and syphilis? (2) Did awareness of HIV and syphilis symptoms, and the advisability of testing, increase among MSM as a result of the campaign? To address these questions, data were collected from a large-scale online pre- and postcampaign survey of sexually active MSM and from the Public Health Ontario Laboratories (PHOL) test records. The latter consisted of a summary of the number of HIV tests per months by health region of Ontario for MSM from January 2010 to June 2012. The total number of tests for this time period was 77,686, adjusted for unknown region, sex, and exposure category.
The research evaluation was approved by the ethics review boards of the University of Windsor and the University of Toronto.
Pre- and Postcampaign Online Surveys
A precampaign survey was disseminated a few weeks prior to launch, and the postcampaign survey was conducted several weeks after the close of the campaign. Respondents were recruited through two major gay contact sites, Squirt (www.squirt.org) and Manhunt (www.manhunt.net). Previous research done at Toronto Pride showed that squirt.org and manhunt.net are among the larger contact sites, with 11.4% of Toronto men indicating that they have a profile on squirt.org and 10.2% on manhunt.net (Adam, Husbands, Murray, & Maxwell, 2007). An e-mail message with a survey link was sent to the inbox of account holders at both websites who were located in Toronto, Ottawa, and other Ontario locations. The precampaign survey asked 40 questions in total: 12 demographic, 17 behavioral, 6 knowledge, and 5 specific to health history, including HIV status. The postcampaign survey asked the same 40 questions plus 10 questions about the campaign that had just concluded. The median completion time for the precampaign survey was 7 minutes with an interquartile range of 5 to 9 minutes.
Clinic Exit Survey
Attendees at supplemental point-of-care testing sites, who did not receive a reactive test result, were given a survey to fill out after their appointment was complete to measure campaign reach. The clinic counselor left the room, allowing the client to decide if he wanted to complete the questionnaire, and time and privacy if he did. This survey focused on the reach and resonance of the campaign and what features were important to individual testers. The survey was composed of 19 questions: 4 questions about what is important to getting tested (e.g., location, anonymity, immediacy of results), 2 questions concerning the time and convenience of the clinic, and 13 questions about awareness of the campaign.
Analysis
Data were imported into SAS Version 9.3 for analysis and were cleaned and queried prior to analysis. Descriptive summaries of data included proportions for categorical data and means for continuous data and 95% confidence intervals (CI) where appropriate. Exact binomial 95% CI were reported for positivity rate calculations. For univariate group comparisons, chi-square and Fisher’s exact tests were used for categorical data and t tests for continuous data. A p < .05 was considered significant. Logistic regression, Poisson regression with robust variance, and autoregression for time series methods were used for multivariate modeling with manual selection of covariates. Some nonsignificant variables remained in the models if these variables were considered to be confounders.
Results
A total of 1,183 responded to the precampaign survey. Twenty responses were excluded because it was not clear if the respondent was a man who has sex with men. Because one of the participating websites sent the postcampaign survey to members in all of Ontario rather than just Toronto and Ottawa, it garnered 3,704 responses; 129 were excluded from the analysis. This essentially had the effect of increasing the number of respondents who were unaware of the campaign. Region has been controlled for in subsequent analysis where appropriate. Completion of the survey was related to the following characteristics: Older participants were more likely to complete (91% for those 55 and older vs. 84% for 15- to 29-year-olds), gay-identified more likely to complete (90%) than bisexual or heterosexual (84%), having had at least one instance of UAVI in the last 6 months with a regular or casual partner more likely to complete (92%) compared to having consistent condom use (86%), and having sex with consistent condom use in last 6 months more likely to complete (86%) than not having sex (68%).
Eighty-six percent reported having some college or university education or more (no significant difference between pre- and postcampaign). Approximately 30% reported an annual income between $20,000 and $49,999 a year, and 38% reported earning between $50,000 and $99,999 annually. These numbers were consistent in both surveys (i.e., not significantly different, p = .09 and p = .12, respectively). Respondents were significantly older in the postcampaign survey compared to precampaign (p < .01). Approximately three quarters (74%) of respondents in the precampaign reported their sexual orientation as gay or homosexual. Around 87% (N = 4,146) reported they were HIV-negative, whereas 7% reported they were HIV-positive, and the remainder reported being unsure of their HIV status. Eighty-three percent of respondents to the online survey reported having had a casual partner in the last 6 months. Those who had a casual partner (N = 3,065) also answered the question inquiring into protected and unprotected sex with casual partners. Overall, half (50%) reported having had UAVI with a casual partner in the past 6 months. Forty-six percent of HIV-negative men reported UAVI, while 78% of the HIV-positive men reported having had UAVI with a casual partner (p < .01). There is no significant variation by age or sexual orientation in the rate of unprotected sex (p = .59).
The dedicated campaign website attracted over 17,000 visits of which 15,249 were unique visitors: 89% of all traffic was Canadian, 45% of users were Toronto-based, and 9% were from Ottawa. On both the French and English sites, 41% stayed on the site longer than 3 minutes. The Symptoms and Testing Options pages had the most page views and unique page views. Visitors spent the most time on the clinic calendar (1:31 minutes) and the clinic locator (1:14 minute) pages.
Looking specifically at the men who came in for an HIV test, 72% reported on the exit survey that they had recently engaged in UAVI, while 58% of the men drawn from the two sexual contact websites indicated that they had had UAVI.
Knowledge and Awareness
The pre- and postcampaign surveys were conducted through two gay contact websites independent of the campaign website to assess the reach and impact of the campaign. Six knowledge questions regarding HIV and STI were included prior to campaign launch and then posed again in the postcampaign survey. After the survey participant selected an answer of “true,” “false,” or “don’t know” to each question, the correct answer was provided so that the survey itself acted as an educational tool. Because of the online structure of the survey, study participants could not go back to correct their answer once they had proceeded to the answer provided by the site. Approximately 88% (N = 4,156 of 4,738) of online participants answered at least one of the HIV/STI knowledge questions; 86% (N = 4,092) answered four or more questions. For most questions, the level of knowledge was high, that is, more than 80% answered the questions correctly. The survey showed almost universal awareness (97%) that UAVI is high-risk behavior for HIV transmission. Least well known were seroconversion symptoms (49%) and the increase in risk of HIV transmission of one partner having syphilis (72%).
When four or more questions were answered correctly, we ranked respondents as having “good knowledge” (73%, N = 3,479). They were compared to those who answered three or more incorrectly or “did not know” (27%, N = 1,259). Univariate analysis showed that those who reported being bisexual, heterosexual, or other had less knowledge (63%) than men reporting their sexual orientation as gay (79%, p < .01). Correct knowledge scores were slightly higher for those living in Toronto or Ottawa compared to less urban locations.
Overall, 31% of postcampaign online survey respondents indicated that they were aware of the campaign. Being aware of the campaign was significantly associated with better knowledge scores. These findings continued to hold using multivariate analysis when modeling the outcome of “good knowledge” for those who answered four or more questions (N = 4,092). Multivariate modeling showed no significant differences in knowledge according to website from which they were referred, region, sexual risk behavior, or immigration status. The variables that did predict statistically significant better knowledge scores were being aware of the campaign (93%) compared to not being aware postcampaign (82%) or precampaign (87%); having an HIV test within the last year or already HIV-positive (91%) compared to being HIV-negative and tested more than a year ago (83%) or never tested (73%); ever having a syphilis test (90%) compared to never having a syphilis test (79%); identifying as gay (89%) compared to bisexual (77%); younger age, 82% for 15 to 24 and 90% for 25 to 44 age-groups declining to 79% for the 55+ age group; and higher education, high school or less 74% rising to 91% for postgraduates (see Table 1). Overall, knowledge scores were higher among postcampaign survey participants who indicated they were aware of the campaign but not among those unaware of the campaign, when compared to precampaign scores suggesting that the campaign had measurable effect on HIV knowledge among MSM in the larger community.
Probability of Having Good HIV Knowledge (N = 3,756)
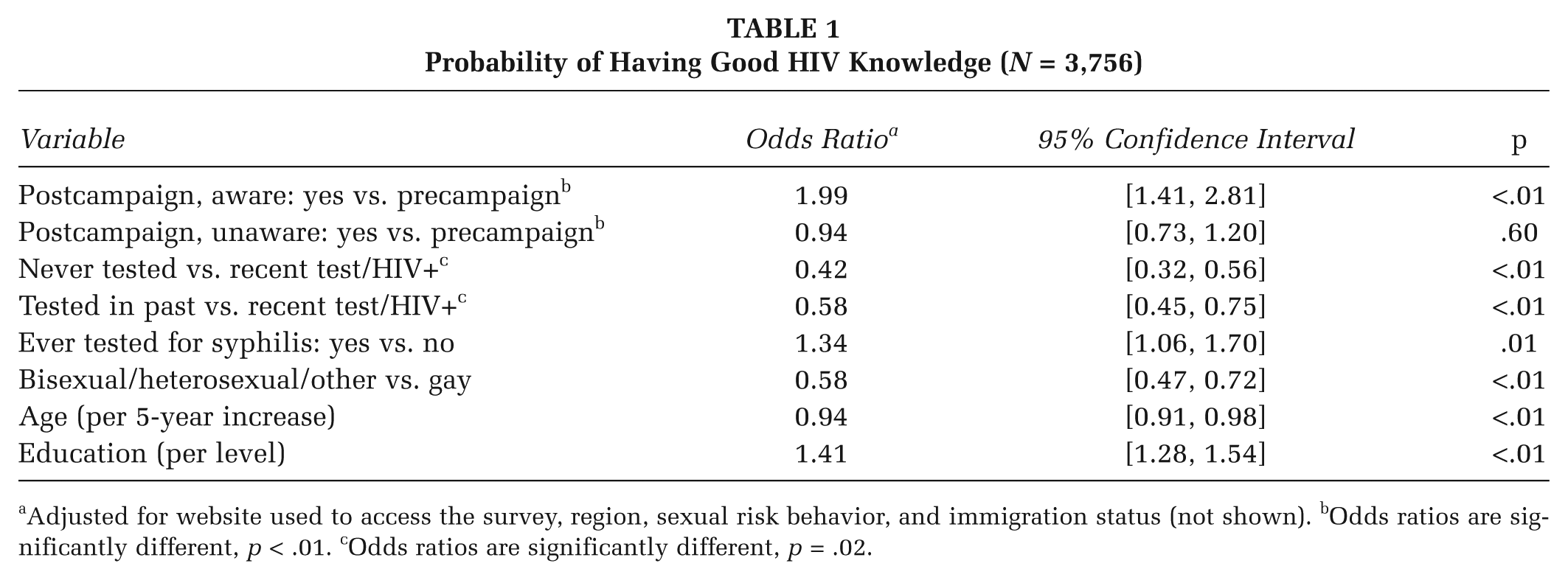
Adjusted for website used to access the survey, region, sexual risk behavior, and immigration status (not shown). bOdds ratios are significantly different, p < .01. cOdds ratios are significantly different, p = .02.
Multivariate analysis of the postcampaign survey shows that variables associated with greater awareness of the campaign were similar to variables that predicted better knowledge of STIs and HIV. Greater than average awareness was associated at a statistically significant level with having tested for HIV within the year or already HIV-positive (49% aware) versus 36% aware among those who tested more than a year ago and 25% who never tested, ever having tested for syphilis (39%) versus not having tested (21%); younger age (33% among men 30-44 years compared to 25% among those over 55 years), higher education (38% with a postgraduate or professional degree compared to 21% with high school or less), and a Toronto (43%) or Ottawa (41%) postal code versus elsewhere (24%).
Over one third (33%) of the online survey respondents reported seeking more information after becoming aware of the campaign. For those aware of the campaign (N = 703), the following characteristics were significantly associated with seeking more information about HIV and/or syphilis: bisexual orientation (39%) compared to identifying as gay (32%; odds ratio [OR] =1.77, CI [1.18, 2.66], p < .01), younger age: 51% for 15 to 24 age-group declining to 34% for the 55 and over age-group (OR = 0.91, CI [0.85, 0.98], p < .01), less education (high school or less 50% declining to 31% for postgraduates, OR = 0.75, CI [0.62, 0.91] p < .01), born outside of Canada (44%) compared to Canadian born (31%; OR = 0.50, CI [0.32, 0.77], p < .01), and having had an HIV test because of the campaign (67%) compared to not having a test (26%; OR = 5.34, CI [3.48, 8.19], p < .01).
Testing
According to PHOL population data, there were 7,951 HIV tests during the campaign period in Toronto, a 20% increase in HIV testing among MSM compared to the same 6 months of the previous year (6,616 tests) and a 23% increase in Ottawa over the same period (see Figure 2; 2,832 and 2,300 tests, respectively). This compares to a 6% increase in the number of tests in the rest of Ontario (5,821 and 6,192 tests, respectively). The number of tests was significantly higher for the campaign period (p = .02, time series analysis of all 77,686 tests summarized by month and adjusted for region). Nevertheless, the seropositivity rate remained relatively constant in Toronto (p = .56) and the rest of Ontario (p = .12) and dropped slightly in Ottawa (p < .01). Toronto showed a nonsignificant (p = .32) decline in rate immediately after the campaign, whereas Ottawa and the rest of the province had a nonsignificant increase (p = .84 and p = .62). Among those who attended clinics, men reporting at least one instance of UAVI had a significantly higher positivity rate (2.57%, CI [1.60%, 3.91%]) compared to those for whom there was no record of UAVI (0.32%, CI [0.01%, 1.78%], p = .01). Eighteen percent of the survey participants reported getting an HIV or syphilis test after becoming aware of the campaign. For those aware of the campaign, the following characteristics are significantly associated with getting a test because of the campaign: correctly answering the HIV symptoms question (OR = 1.74, p = .02), Ottawa resident versus Toronto resident (OR = 0.49, marginally significant, p = .06), and seeking out more information (OR = 5.33, p =<.01).
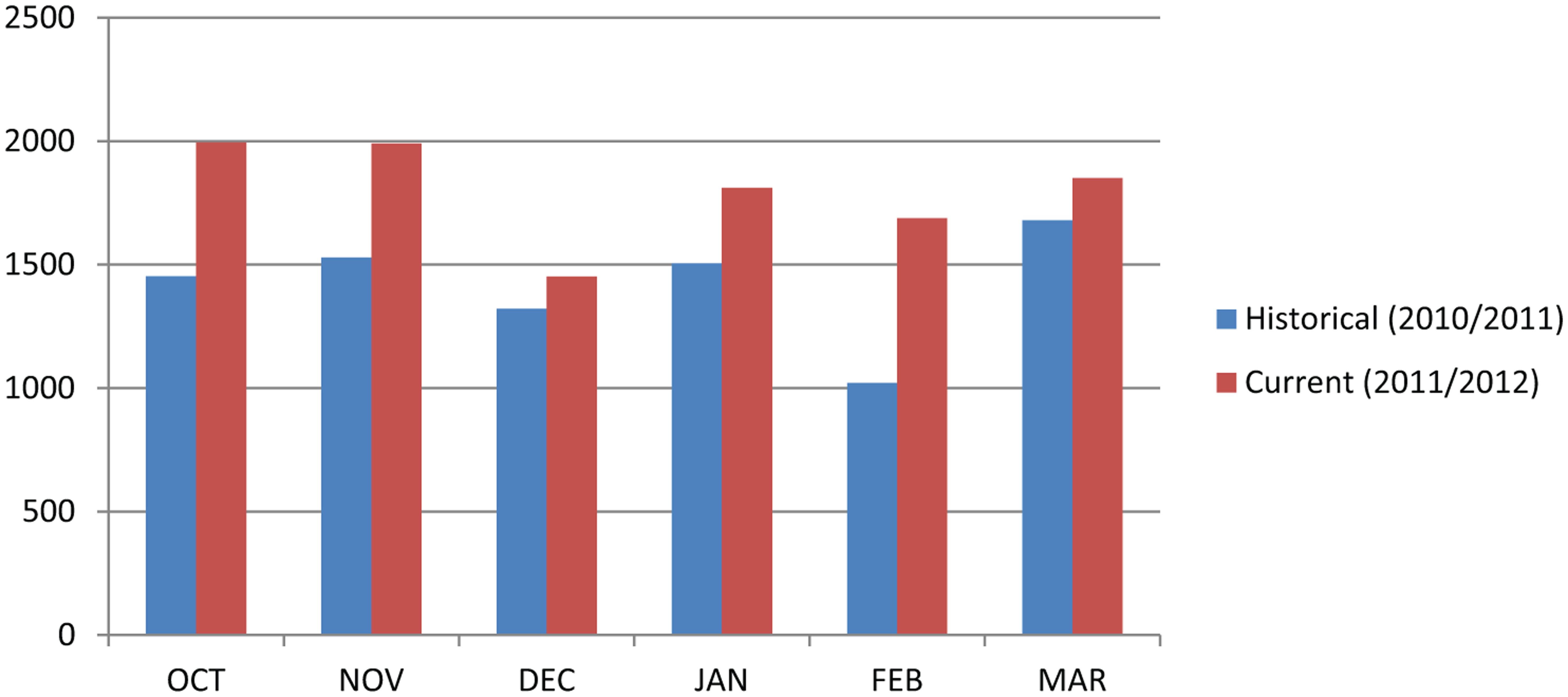
Number of HIV Tests in Toronto and Ottawa for Each Month of the Testing Campaign Compared to the Previous Year
In the online survey, men in Toronto and Ottawa were more likely to report having had a syphilis test compared to elsewhere in the province. Seventy-two percent of Toronto respondents (N = 1,275) reported having had a syphilis test, and 16% of those tested (N = 813) reported having a positive syphilis test result. Toronto rates were significantly higher than Ottawa (p < .01 and p = .04, respectively). Sixty-three percent of Ottawa respondents (N = 398) reported having had a syphilis test, and 11% of those tested (N = 226) reported being told they had syphilis. There were no significant differences within region from the precampaign survey to the post survey.
For men who did go to a clinic to get tested and filled out an exit survey, 62% reported having seen the campaign image. They were also more likely to report that the campaign was attention-grabbing (71%) than online survey participants (41%), suggesting that the campaign did serve to motivate testing.
Discussion
Overall then, Toronto and Ottawa showed an increase in MSM testing over the campaign period compared to the same time period in the previous year corroborated by PHOL data and online survey responses. This was a larger increase in testing than was observed in the rest of Ontario. While more men took the test during the campaign, the overall rate of reactive tests remained relatively constant. Looking specifically at the men who came in for an HIV test and filled out an exit survey, considerably more indicated that they had recently engaged in sex without a condom, compared to men drawn from the two sexual contact websites. As well, more men who turned up for testing reported seeing the campaign image compared to those who filled out the online postcampaign survey.
The campaign also succeeded in improving knowledge about seroconversion symptoms, syphilis and HIV transmission, and the HIV window period. The campaign survey may as well have been a contributor to improved knowledge. Knowledge levels and interest in seeking more information were significantly better among the postcampaign survey respondents who were aware of the campaign compared to postcampaign respondents who were not aware and compared to precampaign respondents.
Over one third of the online survey respondents reported seeking more information after becoming aware of the campaign. Bisexual, younger or less educated men, men born outside of Canada, and men who had an HIV test because of the campaign were significantly more likely to seek further information. Improving access to HIV testing through the downtown Toronto clinic with an established reputation as a gay-friendly site also helped raise testing numbers. Clinic attendance numbers suggest considerable demand for being tested in a gay-friendly site over a site close to work or home if a choice had to be made as testing rates did not increase in supplemental clinic hours in other regular public health facilities. Rapid point-of-care testing and the ability to walk in without an appointment were cited by men who took the test as important considerations in their willingness to test.
These data have some limitations. Because of ethical concerns in preserving the anonymity of survey participants, IP addresses were not collected, and therefore responses to the postcampaign survey could not be matched to responses from the precampaign survey at the individual level. Some respondents may have had profiles on both Manhunt and Squirt and have received survey invitations through both sites. Though the e-blast message asked respondents not to fill the survey out again if they had already completed it, it is possible that there is some duplication or that some of the noncompletion rate is due to individuals discovering after a few questions that they had already filled out the survey through the other site. As well, additional clinic hours for HIV testing, created in anticipation of increased demand, may have in themselves helped improve testing numbers.
Conclusion
Gay, bisexual, and other MSM can be reached through social marketing techniques especially when they are addressed as such in a media environment where gay men are not often visible. There is, nevertheless, a social geography to messaging with urban, better educated, and gay-identified men more likely to be reached. As MSM are generally already well informed concerning the basics of HIV prevention, this campaign used multiple channels to provide a more advanced level of HIV and syphilis information with the particular intent of encouraging recognition of symptoms of possible seroconversion illness. The triangulation of data drawn from HIV testing rates, exit surveys, plus comparison of pre- and postsurvey results, and the responses of men aware of, and unaware of, the campaign point in the direction of significant knowledge and testing changes associated with the campaign.
Footnotes
The testing campaign and its evaluation were made possible by Frank McGee and Ken English of the AIDS Bureau of the Ontario Ministry of Health and Long-Term Care; Jane Greer and Shawn Fowler of the Hassle Free Clinic; G. Bruce Clarke and Carrie Johnston of Toronto Public Health; Robert Remis and Ashleigh Sullivan of the Ontario Public Health Laboratory; Christiane Bouchard, Marie-Odile Grayson, Billy Downer, Suzanne Rowland, and Tamatha Trenholm of Ottawa Public Health; and Brian Gahan, Rachael Muir, and Adam T. Smith of Top Drawer Creative.
Early results from this study were presented to the Canadian Association for HIV Research meeting in Vancouver.