
Abstract
Aims. This feasibility study evaluated the impact of a culturally consistent diabetes educational program, led by a Latino pastor, on Latino community diabetes knowledge levels. Method. Latino adults were recruited from two churches serving Latino populations, one identified as intervention, the other as nonintervention. Both churches received the American Diabetes Association’s booklets on diabetes education, “Four Steps to Control Your Diabetes for Life.” The intervention group also received weekly reviews of the booklet’s information from the church pastor, who was educated about diabetes by a Latino family nurse practitioner. Pre- and postintervention levels of diabetes knowledge were measured using the Diabetes Knowledge Questionnaire. Results. Mean changes in the Diabetes Knowledge Questionnaire (DKQ-24) survey from pretest to posttest indicated a significant increase in knowledge in both groups. Only the grades for the participants from the pastor-led group, however, moved from failure in knowledge to high levels of passing. One hundred percent of intervention group participants reported having read the literature. Conclusions. This pilot study supports the feasibility of a local Latino pastor, as a culturally consistent diabetes educator, to increase Latino parishioner’s knowledge of diabetes.
Keywords
Introduction
Diabetes, according to the Centers for Disease Control and Prevention (2011), is the leading cause of kidney failure, lower limb amputation, and adult-onset blindness, and a major cause of stroke and heart attack in the United States. Death from heart disease is between 2% and 4% higher for persons living with diabetes (American Heart Association, 2013). The current estimated annual financial impact of diabetes is 245 billion dollars, a significant rise (41%) from the 174 billion dollars spent in 2007 (American Diabetes Association [ADA], 2010; ADA, 2014; U.S. Department of Health and Human Services, 2012).
One and a half million people were diagnosed with diabetes in 1958 and, by 2010, that number increased to 18.8 million. More than 29 million people in the United States have been diagnosed with diabetes, an increase that fits the description of epidemic proportions (National Diabetes Education Program [NDEP], 2013; NDST, 2014). Diabetes is the fifth leading cause of death in minority groups, with minority cases representing 25% of all adult patients with diabetes in the United States (U.S. Department of Health and Human Services, 2012). The Latino communities are especially hard hit, with almost 13% of Latinos affected by this disease, compared with only 7% of non-Latino Whites (ADA, 2012). Vincent (2009) identified that current methods used in educating non-Latino populations have not been effective for increasing knowledge about diabetes or in changing high-risk behaviors in the Latino community.
This article describes a pilot intervention, Por Nuestra Salud, that aimed at increasing diabetes knowledge in two predominantly Latino churches. To get a better understanding of the effect a culturally consistent diabetic educator can make in increasing understanding and prevention practices in a Latino community, this pilot study, Por Nuestra Salud, identified a community leader as a potential basic diabetes educator. This pilot study is congruent with the mission statement of linking research to practice as it demonstrates, through the implementation and evaluation of an evidence-based program, that used a respected Latino community member as a trained, culturally consistent, basic diabetic educator may increase participant knowledge and engagement.
Background
Traditional diabetes management strategies in the United States have not been demonstrated to have a significant impact with the Latino population (Vincent, 2009). Multiple barriers impeding optimal management of diabetes in the Latino community still exist (Chilton, Hu, & Wallace, 2006). These barriers include language, difficulty in lifestyle transitions, financial constraints, and incomplete acculturation (Chilton et al., 2006).
The language barrier has been identified as one of the greatest obstacles that Latinos have to overcome in order to obtain optimal diabetes management (Cefalu & Golden, 2015; Institute of Medicine, 2006; Pares-Avila, Sobralske, & Katz, 2011). Limited English proficiency among Latinos increases the likelihood of poor communication between patient and health care provider, escalating poor health outcomes and other health care disparities in the Latino community (ADA, 2009; Fernandez et al., 2011). Fernandez et al. (2011) demonstrated that limited English proficiency in the Latino community has a direct negative effect on glycemic control, an effect that was not seen using a language concordant provider. Cefalu and Golden (2015) addressed the need to develop culturally appropriate interventions, including removal of the language barrier, that addresses the specific needs of the Latino population, a group that carries a disproportionally high diabetes burden.
Ruiz, Gallardo, and Delgado-Romero (2013) identified multiple psychological barriers that also affect health-seeking behaviors in Latino communities. These include the recent rise of racism, xenophobic reactions of non-Latino Americans toward Latino’s and the existence of ongoing, pervasive negative press related to Latino immigration. These social obstacles, coupled with the language barrier, have been identified as factors that prevent Latino’s from seeking access to public health and also failing to obtain equal medical treatment. Studies that provided education from community health workers who shared common language and culture demonstrated increased diabetic knowledge and skills (Prezio et al., 2013; Shepherd-Banigan et al., 2014).
A randomized control trial tested the impact of an educational diabetes program provided by a culturally consistent community health worker on uninsured Mexican Americans. Results indicated that the intervention group had lowered HbA1c (glycated hemoglobin) at the end of the intervention (Prezio et al., 2013). Ongoing community-based education was needed for reinforcement of knowledge and skill gains to maintain the programs efficacy.
Shepherd-Banigan et al. (2014) conducted a household level educational program for Hispanics, led by community health educators. The program evaluated home-health parties that provided diabetes education. The qualitative results indicated the participant’s need for diabetes education that included social support, education, trust, and cultural understanding between the recipient and the educator. The educators, promotores, provided information and were identified as credible role models, “offering social support in the context of shared cultural perspective” (p. 513). This study underscored the importance of the credibility and cultural consistency of the health educator with the population being served.
These cultural, social, political, and economic factors place the Latino population at higher risk for isolation from health education, increasing the likelihood of developing diabetes and the sequelae of complications that follow. Schyve (2007) identified the triple threat to patients with limited English proficiency. The primary barrier is the language itself, followed by the cultural difference, which impedes the communication further, and the patient’s low level of health literacy. Low-health literacy might be a result of the cultural and linguistic differences existing between provider and patient (Schyve, 2007). The Joint Commission report, as reported by Schyve (2007), examined the issue of safe, effective care in light of this triple threat. Health care providers need to address the disparity caused by the difficulties experienced communicating with patients from different cultures, who speak different languages, and who have low health literacy for making medical decisions (Schyve, 2007). Providing the Latino community with culturally consistent, Spanish diabetes education, delivered in a safe environment, free of judgment and/or fear, is the first step to improving diabetes education and providing safe and effective diabetes treatment to this high-risk population.
This study, Por Nuestra Salud, specifically investigated the impact of diabetes knowledge, when the diabetes educator was a local Latino pastor. A Latino family nurse practitioner (FNP), specializing in diabetes, identified this problem in the Latino community. On evaluation of the problem, the FNP identified the need for linguistically and culturally consistent diabetes education. Taking these barriers into account, the FNP devised an intervention and a method for evaluation of its efficacy. Identifying two Latino churches, the FNP provided the American Diabetes Association’s diabetes education booklets, written in English and Spanish and referral numbers, for those who wanted to seek follow-up care, to both churches. Only the intervention church had the FNP deliver diabetes education to the Latino pastor. The aim was to determine whether utilization of a local, respected Latino leader as a diabetes educator could increase knowledge about diabetes.
The community-based social marketing (CBSM) model was chosen as the framework for this study. The CBSM has been used to develop programs that can produce effective behavior change resulting in sustainable health promoting behavior (McKenzie-Mohr & Schultz, 2014). Five steps required for implementation of the CBSM include the following: identifying the problem, evaluating the barriers and benefits for change, choosing an approach that takes the barriers and benefits into account, piloting the new program, and finally, evaluating the pilot program (McKenzie-Mohr & Schultz, 2014).
One of the main barriers identified by the FNP, with regard to this population, was the lack of community health providers with cultural consistency. Festinger (1957) and Heider (1958) originally identified the construct of cultural consistency as the desire of a group of people to seek others who share related beliefs, attitudes, and behaviors. Petrova, Cialdini, and Sills (2007), applying the construct of cultural consistency, demonstrated that group compliance increased when individual members identified with the social behaviors of the leader, or in this case health educator. Cultural consistency has the capacity to bind together personal and cultural variables, improving individual and collective intrinsic motivation and compliance (Petrova et al., 2007). The FNP tested if the use of a culturally consistent community educator (the Latino pastor) would improve the individual and collective compliance of these parishioners.
Method
Design
A prospective, two-group, pretest–posttest, randomized control trial was employed to compare the levels of diabetes knowledge between parishioners at two churches. One received standard information published in the NDEP’s diabetes education booklets (nonintervention) and the other received standard information, with the addition of six, Latino, pastor-led seminars that provided an introduction to the program, reviewed the chapters in the diabetes education booklets and a summary seminar in the sixth week (intervention).
Setting
The study was implemented in two Latino faith-based, Roman Catholic, community churches located 34 miles apart (1 hour by car) in northeast United States. Both churches provided services in Spanish and English to predominantly Latino populations.
Procedure
Two churches, identified for their predominantly Latino parishioners and their substantial distance from each other, agreed to participate in the study. Both churches held health fairs and were provided with the American Diabetes Association’s booklet, “Four Steps to Control Your Diabetes for Life.” One church, by way of a coin toss, was selected to be the intervention church. The pastor from the intervention church was provided with a brief education on diabetes.
Components of Intervention
The National Diabetes Education Program Booklet: Four Steps to Manage Your Diabetes for Life
The booklet used to educate the pastor and the parishioners is an evidence based, Natioanl Institutes of Health–supported (NDEP, 2012), which is published in multiple languages and available online. For this study, the Spanish NDEP booklet was used. The steps included the following: (1) basic facts about diabetes, (2) The ABC’s of diabetes (A1c, blood pressure, and cholesterol), (3) how to live with diabetes (coping strategies), and (4) how to remain healthy if you have diabetes (doctor visits, eat well, exercise). Each step, or chapter, has tips about actions that can be taken to improve healthy lives, with or without diabetes, and is self-explanatory. The end of the book also includes some record keeping hints like doctor’s visits, blood sugar test cards, and a place to take notes (http://ndep.nih.gov/media/NDEP67_4Steps_4c_508.pdf).
Education of the Pastor
A Latino nurse practitioner, specializing in diabetes, provided the pastor with 6 hours of one-to-one education over a 5-week period. The pastor’s education was restricted to reviewing and explaining the contents of the NDEP booklet and discussion related to the problem of diabetes in the Latino community. The education was conducted in Spanish discussing all aspects of the four steps explained in the NDEP booklet.
The pastor was instructed in providing six seminars, the first to establish expectations and determine that each participant had an NDEP booklet. Then, the next four seminars reviewed one step per week, from the booklet, over a 4-week period. The last seminar reviewed the four steps and discussed the NDEP booklet. There was no researcher present in these seminars. Each of the pastor-guided seminars, which lasted 30 minutes reviewed the step of the week and guided the participants in engagement in the weekly booklet suggestions. The pastor only responded to questions that reflected information that could be found in the ADA booklet. The telephone numbers of a local diabetes clinic and the nurse practitioner were at the back of each booklet for questions that needed more information than what was included in the booklet. Utilization of the community pastor as the health educator was the operationalization of cultural consistency in the CBSM framework.
Health fairs were small informational gatherings, set up as tables with posters, that provided blood pressure screening, as well as information about heart disease, diabetes, and smoking. During the fair, participant recruitment took place. Parishioners visiting the diabetes table were told about the study, and asked to take the Diabetes Knowledge Questionnaire (DKQ-24) pretest survey, which was available in English and Spanish. Each parishioner had a unique identification for the survey. All parishioners were invited to participate, but only surveys from Latino parishioners were entered into the study.
The NDEP diabetes pamphlet was introduced and distributed at the health fairs. The intervention and nonintervention groups continued to have access to the pamphlets, which were placed at the entrance of each of the churches’ sanctuaries. The parishioners at the intervention church also received 6 weeks of informal education from the pastor (Weeks 6-11). A second small health fair was held simultaneously at both churches in Week 12. Once again, at the diabetes information table, parishioners were asked to take the DKQ-24 survey (posttest). Only surveys with matched unique identifiers from pretest to posttest were used to evaluate the intervention.
All recruitment materials, surveys, study protocols, and consent documents, were approved by the institutional review board of the participating university. Participants provided informed consent and were assigned a unique identifier for pretest–posttest comparisons. No external funding was received in the implementation of this study.
Study Sample
Recruitment efforts included announcements at church masses, church gatherings, and through distribution of flyers at the church masses in the weeks preceding the health fairs. The actual recruitment of participants took place during the health fairs. Participants were required to read and speak English and/or Spanish, be of Latino heritage, be older than 18 years, and not have a disorder that would prevent them from learning (Alzheimer’s disease or other brain-based disease that impede memory). Participants were not required to have diabetes, as their heritage (Latino), was the identified variable for inclusion in the project. No incentives were provided to any participant for participation.
Measurement Tool
The DKQ-24 assess overall diabetes knowledge with a reported Cronbach’s alpha of .78 (Brown, Garcia, Kouzekanani, & Hanis, 2002). Lujan (2008) implemented the DKQ-24 testing the psychometric properties and determined that it was a reliable and clinically applicable tool to measure the level of diabetes knowledge in a Spanish-speaking urban population, establishing a Pearson’s r of .90.
Three response choices include “Yes,” “No,” and “I don’t know.” Items were scored as either correct or incorrect, with the correct items, computed to attain a possible total diabetes knowledge score of 100. Items are written in English and Spanish, using simple language no higher than six grade-reading levels. Content validity of the items was established by a panel of expert nurses and researchers familiar with diabetes-related issues of Mexican Americans (Garcia, Kouzekanani, Villagomez, Hanis, & Brown, 2001). A short survey collecting respondents demographics of interest (age, gender, marital status, medical insurance and family history of diabetes) was included as part of the questionnaire. Age was divided into three categories, 18 or younger, over18 but younger than 50, and above 50 years of age. Each participant had a unique identifier, which served to compare pre- and posttest responses.
Strategies for Statistical Analysis
Data were analyzed using SPSS/PC software Version 19.0. Descriptive statistics and frequencies were tabulated to describe the participants. All p-values were two-tailed, and the significance level was set, a priori, to p < .05. After determining a normal distribution among the respondents, independent-samples t tests and paired t tests were employed to compare within and between group responses on demographics as well as responses to the DKQ-24. An analysis of the variance (ANOVA) was calculated to determine if any of the demographics between groups accounted for the differences in scores.
Results
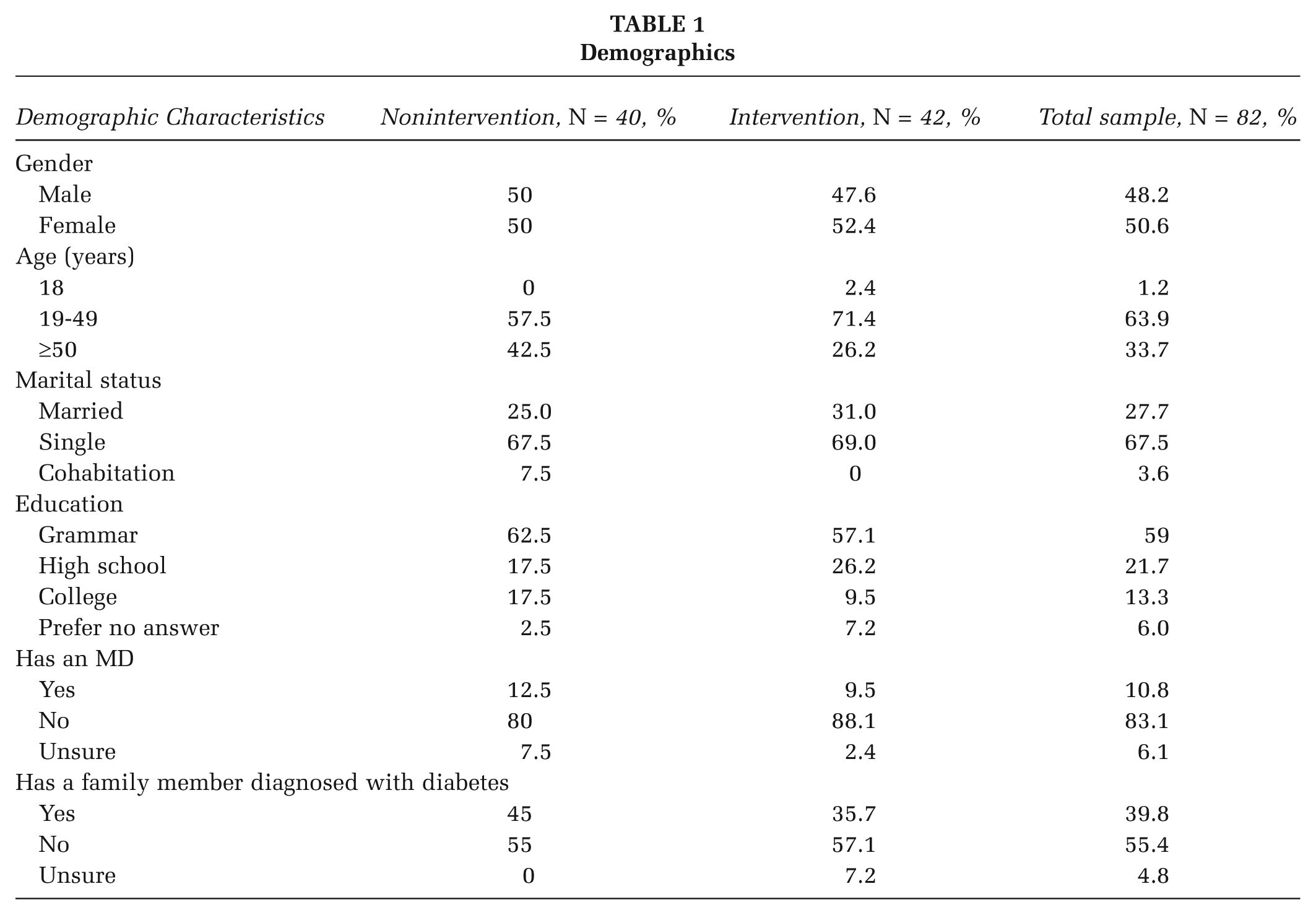
One hundred thirteen Latino volunteers completed the DKQ-24 survey. A total of 82 parishioners met the criteria and correctly completed the surveys (n = 40, nonintervention; n = 42, intervention). There were no significant differences between the groups in gender, age, marital status, medical history of family or personal diagnosis with diabetes, or medical coverage. The nonintervention group had a higher percentage of college-educated participants. The majority of participants were married (67.5%), 59% reported a grammar school education (K-8 grades), 21.7% high school or equivalent, and 13.3% had a college education. Sixty-five percent of the subjects had no medical doctor, 10.8% were diagnosed with diabetes, and 40% reported having a family member diagnosed with diabetes (see Table 1).
Demographics
Pretest and Posttest Results
Independent samples t tests were calculated, comparing the mean scores of the pretests from the two groups. Twenty-four correct answers equaled a score of 100%. A significant difference was found, t (80) = 3.33, p < .001, between the group pretests, with the intervention group achieving a higher level of knowledge than the nonintervention group. The mean of the nonintervention group (M = 4.20, SD = 1.305) was significantly lower than the mean of the intervention group (M = 5.33, SD = 1.439). The average score for the nonintervention pretest was17% compared to a score of 22% for the intervention group. Neither group, intervention or nonintervention, was close to the passing score of 65% (see Figure 1).
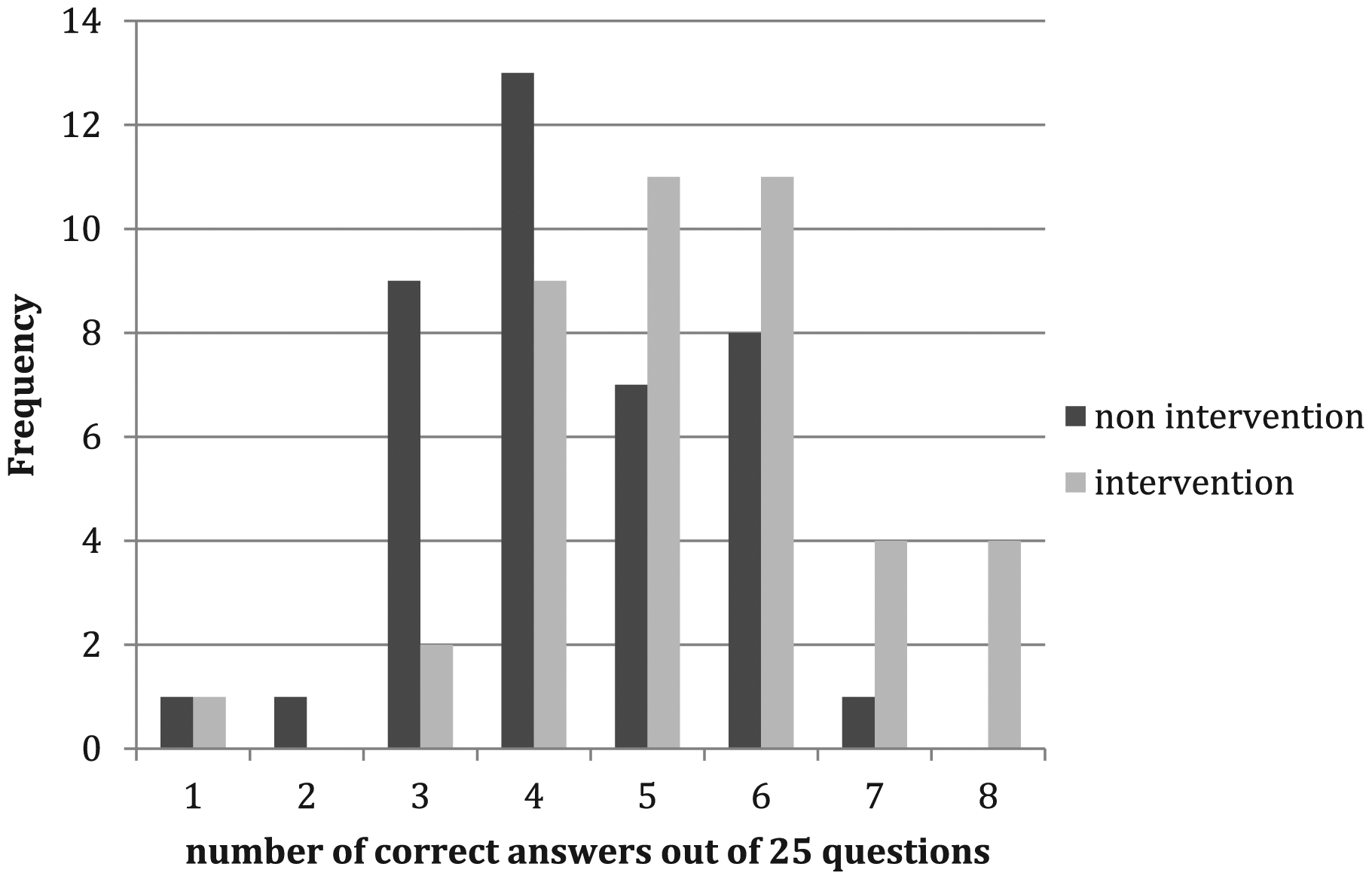
Results of Between Groups Pretest Scores (Out of 25 Questions)
Changes from pretest to posttest for both groups were statistically significant, with the nonintervention group increasing the mean score by 7.6%, from 4.20 (SD = 1.305) to 5.92 (SD = 1.118). The intervention group’s score increased from 5.33 (SD = 1.493) pretest to 19.14 (SD = 1.970) posttest, an increase of 57.75%.
The mean posttest scores for the nonintervention and intervention groups were compared using an independent samples t test. The t tests indicated a significant difference between the mean scores (t = 37.584, df = 80, p < .00). The mean score of the posttest for the nonintervention group (M = 5.92) was significantly lower than that of the intervention group (M = 19.14; see Figure 2).
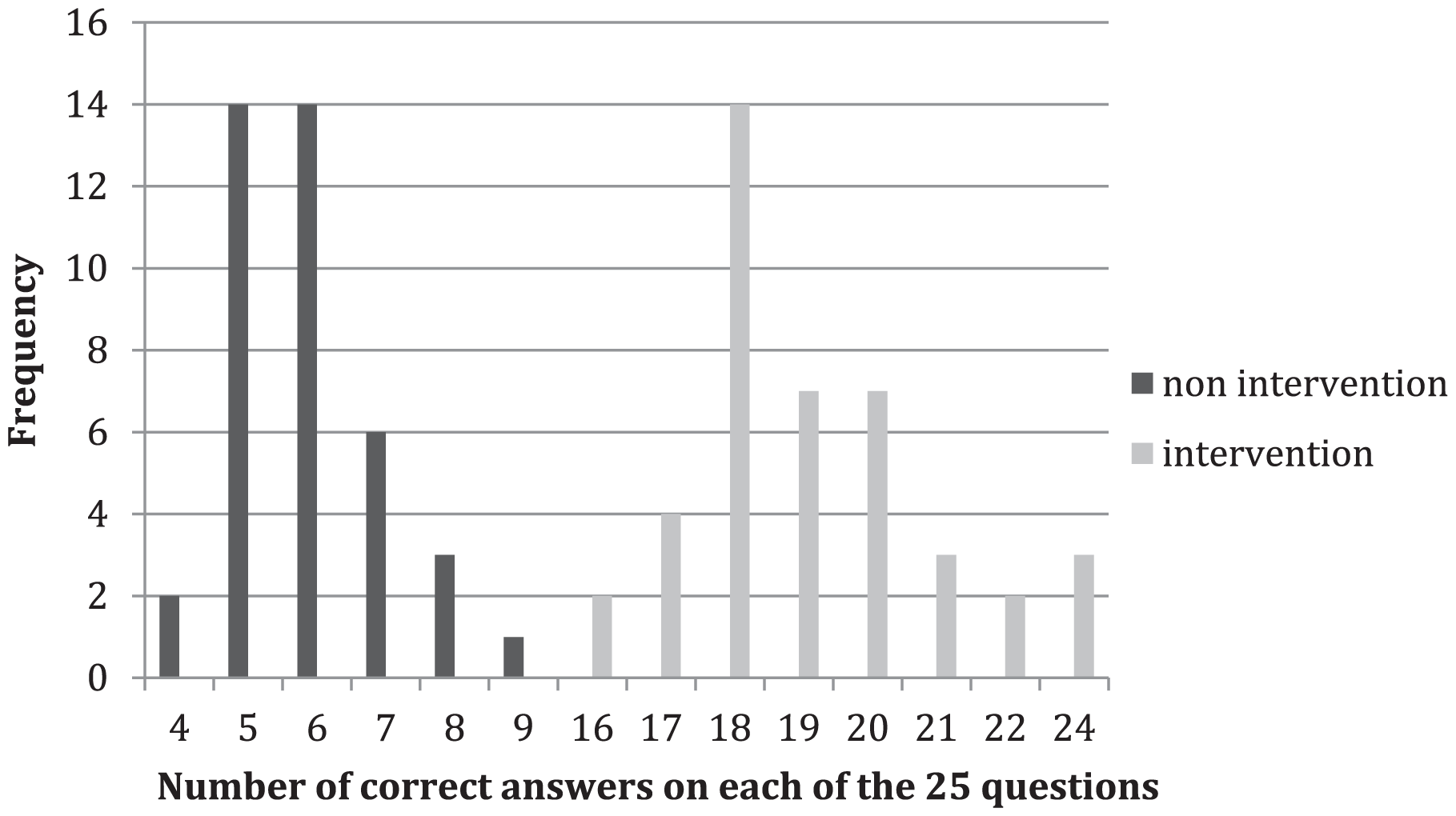
Results of Between Group Posttest Scores (Out of 25 Questions)
Analysis of the Intervention Between Groups From Pretest to Posttest
Although gains in knowledge of diabetes occurred in both groups, the posttest mean for the nonintervention group remained below passing (22%), with the difference between the pre- and posttest scores for nonintervention and intervention groups significantly different (t = 10.228, df = 39, p < .000; see Figure 3).
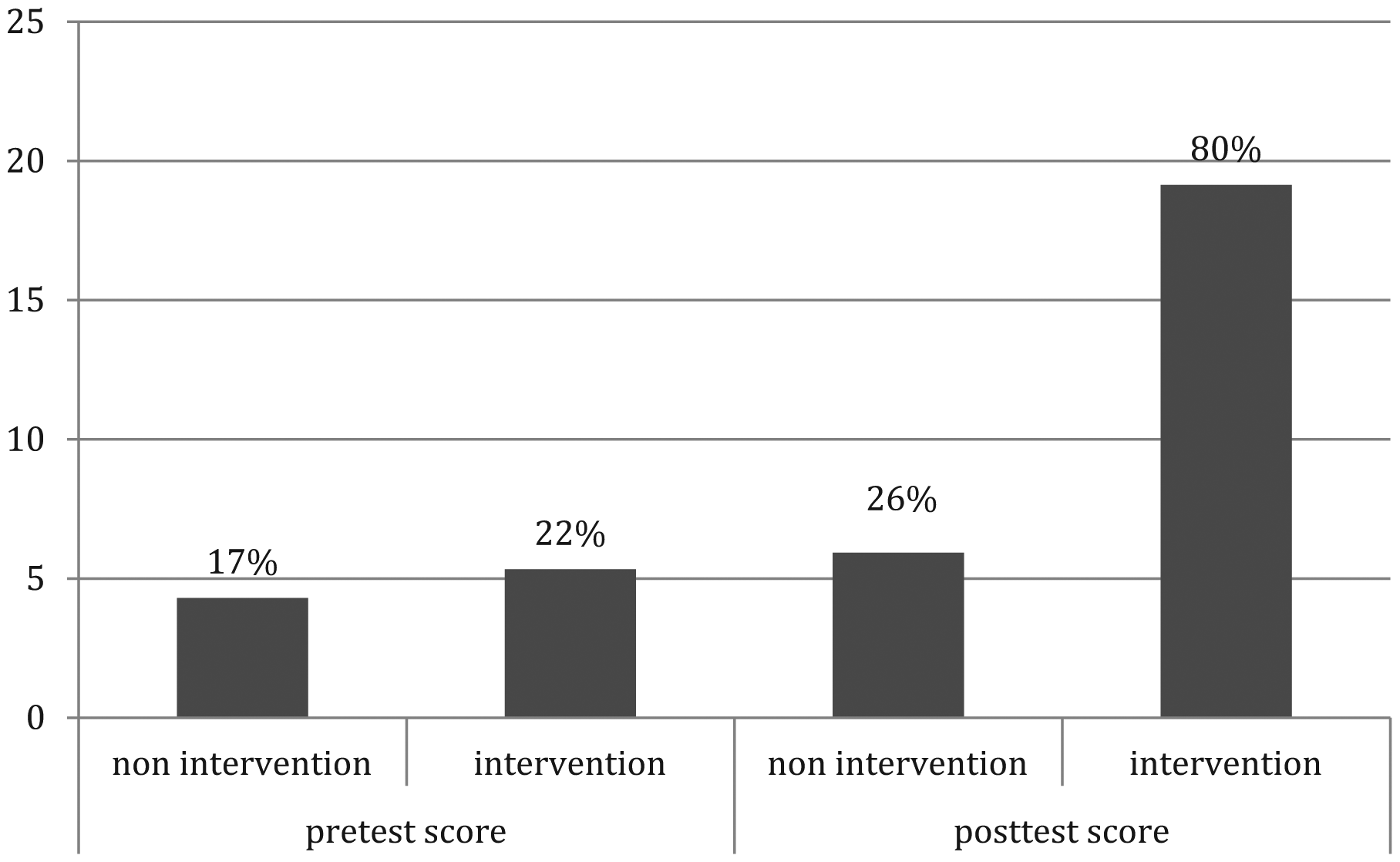
Mean Score for Nonintervention and Intervention Groups at Pretest and Posttest (Out of 25 Questions)
Evaluation of Possible Moderators for Pretest Scores
Evaluation of the specific demographic characteristic of age, as a possible moderator to explain the variance of pretest scores, was explored. The mean age for the intervention group was lower than the mean age for the nonintervention group, however, an ANOVA concluded that age did not factor in the determination of the differences in pretest grades (F = 0.015, df = 2, p > .05).
An evaluation of the engagement in reading the pamphlets between the intervention and nonintervention groups was assessed at the second health fair. Fifteen percent of the nonintervention group reported reading the pamphlet, compared with 100% of the intervention group.
Discussion
This study, combining the CBSM framework and cultural consistency, used a local pastor as the community health educator to bring together his “flock.” Utilization of the pastor’s weekly meetings established an extended pattern of social contact. In the groups led by the pastor, there was sharing of knowledge, attitudes, and social norms related to diabetes knowledge. It also facilitated the pastor’s ability to promote healthy behaviors among his parishioners. Henrich and Broesch (2011) identify the importance of selective learning bias found in cultural group learning. This culturally consistent method of creating a learning group in Por Nuestra Salud was also demonstrated to be more effective than individual, self-motivated learning.
The increase in scores in both groups indicated that the simple provision of information increased the knowledge level of all the participants. The increase in the nonintervention group, however, was not enough to bring the participants level to a passing grade. The pastor was the educator chosen for this study. Even so, the outcome of the evaluation is not specific to the fact that the educator was a pastor. However, the educator was the significant variable in the increase in knowledge between the groups.
The results of this study are supported by the findings of Brown et al. (2002), which proposed that employment of a Latino diabetes educator could increase diabetes knowledge, which could lead to improved health care outcomes for the Latino community. This pilot study added cultural consistency, within the CBSM framework, as the defining factor for improvement in knowledge scores.
The 6-hour, one to one, educational preparation of the pastor by a Latino, doctorally prepared, Advanced Practice Nurse, answered all questions posed by the pastor related to diabetes as well as reviewing the information included in the pamphlet. The pastor was also capable of providing medical referrals to parishioners, referrals that were also indicated in the back of the four-step booklet. The 30-minute, pastor-led educational seminars, were demonstrated to be an efficacious educational method to increase Latino parishioner’s knowledge about diabetes. Fifteen percent (n = 6) of the nonintervention group reported reading the Four Steps to Control your Diabetes for Life booklet, compared with 100% (n = 42) of the intervention group.
Two statistical differences between the groups were identified in the demographics, participant’s age, and educational background. It was determined, through data analysis, that these differences had no statistical significance on the knowledge outcomes. A confounding variable was also identified. Participants reporting achievement of higher levels of education demonstrated lower diabetes knowledge. This indicator provides insight into a need for health education and outreach about diabetes in the Latino community regardless of participant’s academic preparation.
The only variable identified in this pilot study that predicted a significant difference in the scores of the participant’s diabetes knowledge was the pastor-led seminars. This initial finding demonstrated that, in this Latino community, using a trained, trusted, culturally consistent, minority community leader resulted in an increase in participant knowledge of diabetes. Providing educational programs capable of increasing an individual’s knowledge about diabetes is a first step in moving the community toward the life style changes that can promote better health.
Limitations
This 12-week feasibility study evaluated the Latino pastor as a culturally consistent, diabetes educator in a comparison of two Latino churches, one with the educator and one without. The small sample size (n = 82) of Latino men and women limits the ability to generalize these results to other communities. This study did not investigate the origins of the Latino subjects. The Latino population is a very diverse group of individuals, consisting of people from many distinctive Latino countries, including but not limited to Mexico, Peru, Argentina, Spain, and the region of Patagonia. All participants in this study were aggregated into one cultural group, Latino, however, each of these diverse groups, represent unique cultural identities, attitudes, customs, and beliefs that may affect attitudes and behaviors. This study was specific to levels of diabetes knowledge and did not triangulate the data to determine if the change in knowledge had any effect on participant’s attitudes or behaviors. This study did not investigate the role of having diabetes or having a family member with diabetes, on the motivation of the participants to learn about diabetes.
Conclusion
Basic diabetes knowledge can assist people to understand the importance of diet, exercise, and life style modifications in pursuing a healthy life. Latino men and women are seven times more likely to develop and suffer the complications from diabetes than Caucasians (ADA, 2010). There is a need in the Latino community for a new, effective method to educate Latinos about the risks of diabetes, and the benefits of making small lifestyle changes. Despite the fact that 41% of the participants in this study knew that one of their family members had diabetes, their scores on knowledge related to self-care, diet, and exercise demonstrated that they were not capable of providing the kind of care that would prevent negative diabetes-related consequences. Knowledge alone does not guarantee requisite behavior modification or effective self-management, however, the assessment of diabetes-related knowledge is an important first step from which to individualize diabetes education programs and make evaluations of their effectiveness (Garcia et al., 2001).
Recommendations for Research in the Future
Repeating this study with a larger population, using the CBSM framework and a culturally consistent community leader educator, can further test the efficacy of culturally consistent health education. The influence of gender, family, religious, and cultural beliefs should be considered in future research to explore the influence of those variables on diabetes knowledge and behavior change. Investigation of the level of education on the ability to gain health literacy in the Latino population can also shed light on the effect of academic education on knowledge, beliefs, and behaviors related to diabetes. Triangulation of data in future studies, collecting hemoglobin A1C levels and testing for attitude and behavior change in addition to knowledge levels, would strengthen the support for use of the culturally consistent diabetes educator.
The pastors who chose to participate with their congregation in this study were provided with all the pamphlets as well as two diabetes education health fairs and community contact numbers for follow-up questions and care. This study did not evaluate the pastor’s burden of educating his parishioners nor did it collect any qualitative data on the parishioner’s impressions of the experience. This could be of great interest in future studies regarding the use of a respected community leader as a diabetes educator.
Cultural competence refers to the knowledge and interpersonal skills that allow providers to understand appreciate and work with individuals from cultures other than their own (Caballero, 2007). Cultural consistency not only recognizes the differences between cultures but also identifies the desire for those within a culture to demonstrate consistency within a specific behavior (Bednar, Bramson, Jones-Rooy, & Page, 2006). The personal desire to identify, as part of a culture demands, both behaviorally based cultural conformity as well as individual consistency, which is why role modeling from community leaders is so important. This study examined cultural consistency, using a respected member of the community, to provide the diabetes education. The results of this pilot study indicated that by engaging a local, known, cultural consistent diabetes educator, the participants were more likely to remain engaged in the intervention and increase their knowledge of diabetes. Using a social marketing framework, specifically the CBSM, to implement a culturally specific, community-based diabetes education program may prove to be a successful strategy to educate the Latino community about diabetes.