
Abstract
Background. Parent involvement varies widely in school-based programs designed to promote physical activity and healthy nutrition, yet the underlying factors that may limit parent’s participation and support of learned behaviors at home are not well understood. Method. We conducted a qualitative study that consisted of one focus group (n = 5) and 52 in-depth interviews among parents whose children participated in a school-based physical activity and nutrition (PAN) promotion program in Williamsburg, Virginia, United States. We sought to identify factors that enabled or constrained parent’s support of and involvement in children’s programs and to understand the underlying factors that contribute to family success in making dietary and physical activity changes at home. Results. Parents identified their physical and mental health, self-confidence, time, and decision making as underlying “capacities” in the family health pattern. When strengthened, these capacities encourage healthful family behavior and support of school-based PAN programs. Families that succeeded in adopting lessons learned from school-based PAN programs identified four primary strategies for success: shared goals, meal planning, modeling of good behaviors, and collective activities. Conclusions. Interventions that aim to improve child nutrition and physical activity and the broader family health environment should consider underlying capacities of parents and the importance of joint goals and activities.
Introduction
Parental involvement varies widely in school-based physical activity and nutrition (PAN) programs from active participation of parents to limited awareness of children’s activities in programs (Zenzen & Kridli, 2009). Numerous child health programs have found that meaningful parental involvement increases successful dietary change (Golley, Hendrie, Slater, & Corsini, 2011; Hingle, O’Connor, Dave, & Baranowski, 2010; Veracini, Leonardi, Girotti, & Thrasher, 2014;). More direct parental involvement in school-based PAN programs results in greater healthy weight outcomes in children (Hingle et al., 2010) and has been identified as a critical factor for program impact using pathway analysis (Veracini et al., 2014). Effective methods to engage parents in children’s PAN programs can be as simple as worksheets sent home with children as a means of stimulating conversations with children (Kipping, Jago, & Lawlor, 2012).
Parenting practices and behavior modeling at home are strongly associated with healthy weight maintenance in children, including children’s diets (Faith et al., 2012; Matheson et al., 2006; Ventura & Birch, 2008). Modeling is particularly important for helping children accept new and healthy foods as parental food preferences have been linked to child preferences (Stang & Loth, 2011). Part of parental modeling entails parental control practices; older parents with a lower body mass index who were stay-at-home parents are more to use control strategies, as opposed to “pressure to eat” (Brown, Ogden, Vögele, & Gibson, 2008). Student’s environmental factors, including family influences and the availability of health foods at home—especially at breakfast—are a noted “Critical Quality Control Point” in the impact of school-based programs to promote healthy eating (Dokter & Horst, 2014). Parental participation in child nutrition is throughout to operate at multiple levels of the Ecological Framework, particularly at the meso-system level that influences the immediate environment surrounding a child’s food and physical activity choices and modeled behaviors (Bronfenbrenner, 1979). Beyond specific feeding practices and activities, parents can influence a child’s weight through their family style and family functioning (Rhee, 2008). There is a positive association between in-home parental involvement and food behaviors among students; however, some studies have shown that the involvement of parents in nutrition efforts at schools exerts no additional influence on these behaviors (Diallo, Potvin, Bedard, & Larose, 2014). Due to the influence of modeling on children’s weight and overall health, policy makers and program planners are increasingly interested in engaging parents with the goals and activities of PAN programs (Van Lippevelde et al., 2012). Parental engagement in PAN programs is the first step to considering and addressing the implications of family style and functioning on child nutrition (Rhee, 2008).
Parenting capacities represent intrinsic parental attributes that may enable or constrain parents’ abilities to support their children’s nutrition and health. Previous studies have discussed the underlying causes of individual parenting practices (Golan & Weizman, 2001; Ritchie, Welk, Styne, Gerstein, & Crawford, 2005; Wright, Wilson, Griffin, & Evans, 2010). These studies recognize that individual family characteristics and attributes affect parental abilities to support healthy child PAN habits (Ritchie et al., 2005). These studies have also attempted to improve parenting capacities by increasing parental knowledge of healthy eating and physical activity (Golan & Weizman, 2001). Studies that examine underlying parenting capacities (e.g., time management, stress) often focus on a single capacity that relates most clearly to a health outcome or target behavior.
The goal of this study was to understand the influences to parental involvement in a school-based nutrition and physical activity promotion program among underprivileged elementary and middle school students in southeastern United States. To this end, our study had two objectives: (1) to identify barriers to parental participation in a school-based PAN program and children’s nutritional habits and (2) to understand the relevance of parenting capacities to parent’s abilities to be involved in children’s PAN. By describing relationships between parenting capacities and parental abilities and practices for supporting children’s PAN, we identify areas for future attention in interventions that attempt to influence child nutrition by involving parents.
Method
We recruited parents in the Williamsburg, Virginia, area to participate in semistructured, in-depth interviews or focus groups. Recruitment efforts were designed to purposively sample ethnic minority households that qualify for free and reduced-price lunch in the Williamsburg-James City County School system in the Hampton Roads region of Virginia. Participants were recruited from two rosters provided by the Williamsburg Community Health Foundation and Williamsburg-James City County Schools: (1) parents of children who participated in “Challenge Club” programs through the School Health Initiative Program (SHIP) that operates in local public schools (n = 978) and (2) parents of fifth graders from local elementary schools with a free and reduced-price lunch participation rate over 50% (n = 271). Participant recruitment continued to the point of data saturation around key themes. We recruited 36 parents in Phase 1 and 21 parents in Phase 2, for a total of 57 study participants, including 54 mothers and 3 fathers. Parents’ ethnicity was 67% African American (n = 38), 26% Caucasian (n = 15), and 7% Latino (n = 4). Children of participants were in first through eighth grade (see Table 1). One student was in first grade, 8 were in third grade, and 15 were in fourth grade. Fifth grade had the most students with 25. An additional 11 students were in sixth through eighth grade. Fifty-three interviews were conducted with only mothers, two interviews were conducted with only fathers; mothers and fathers were interviewed simultaneously in two cases.
Grade Level of Participant’s Children (n = 60 a )
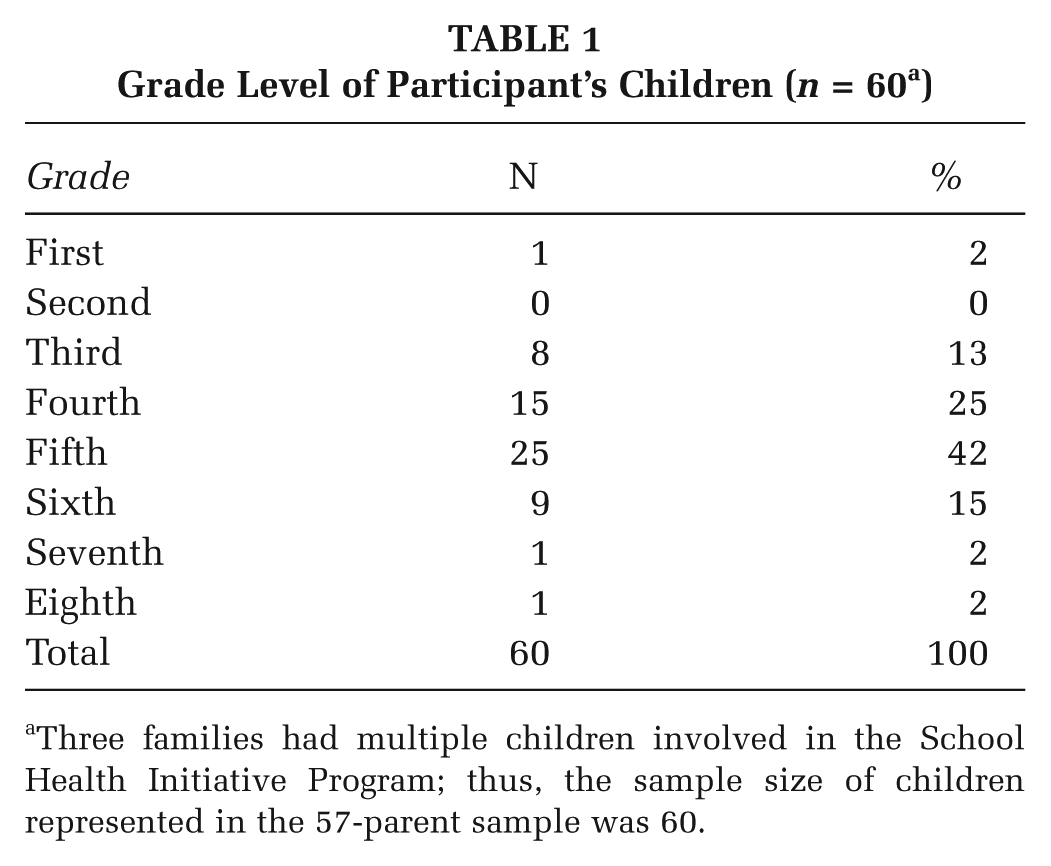
Three families had multiple children involved in the School Health Initiative Program; thus, the sample size of children represented in the 57-parent sample was 60.
Study participants were first contacted by phone to schedule an interview time. Interviews took place at local schools, in participant homes, and over the phone. Participants were asked to participate in a study that sought to understand challenges and successes that parents experienced with being involved in their children’s nutrition and physical activity. We recruited participants from the entire list of students who participated in the past school year in Challenge Clubs in Phase 1. During Phase 2, we recruited participants from a list of student names that were provided by the elementary schools in the district that reported participation of 40% or higher in the free and reduced lunch program. We used a systematic procedure of calling all eligible participants using these criteria to enroll as many parents as possible in the study within a 5-month period, the length of time for which study resources allowed us to collect data.
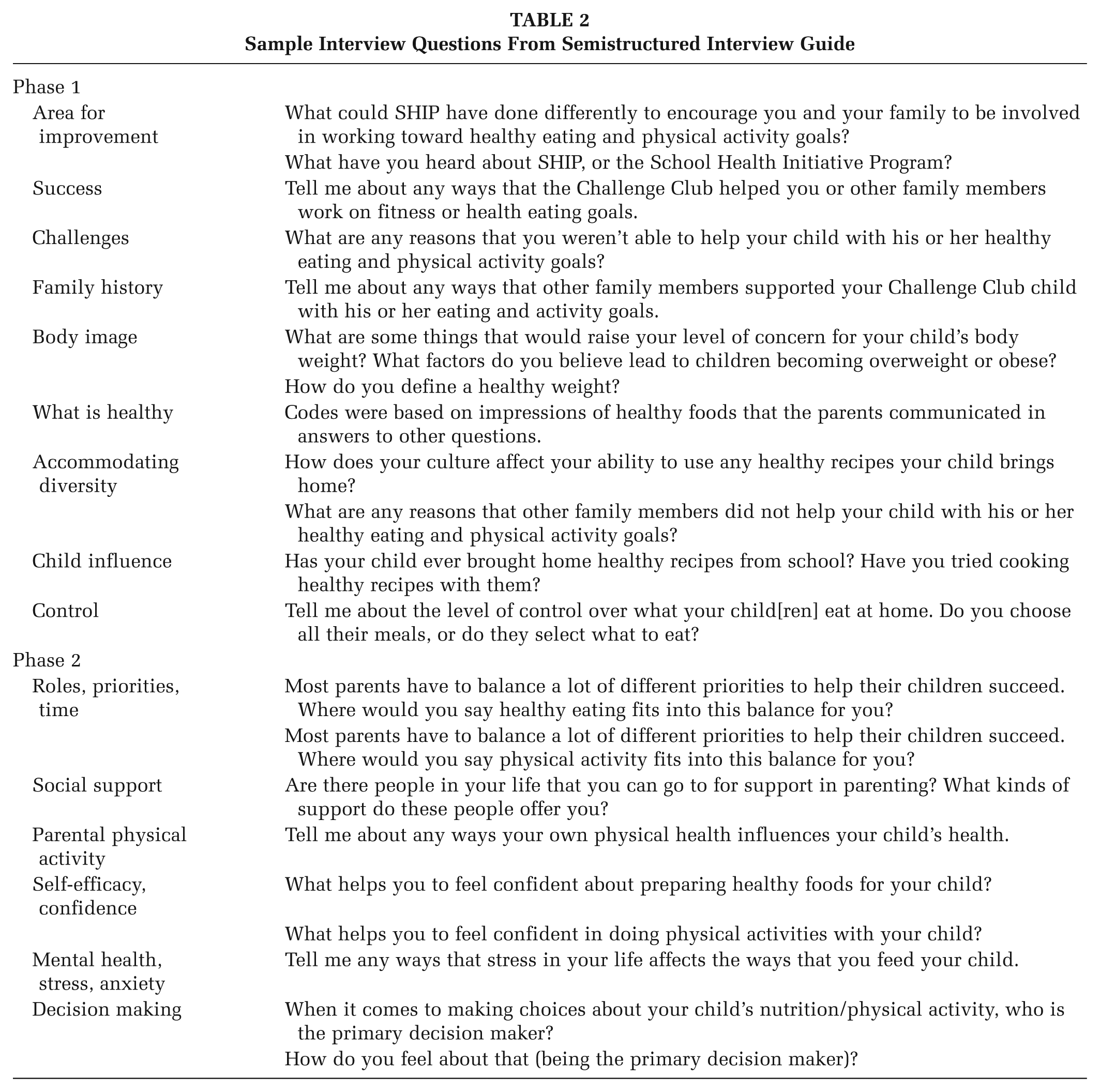
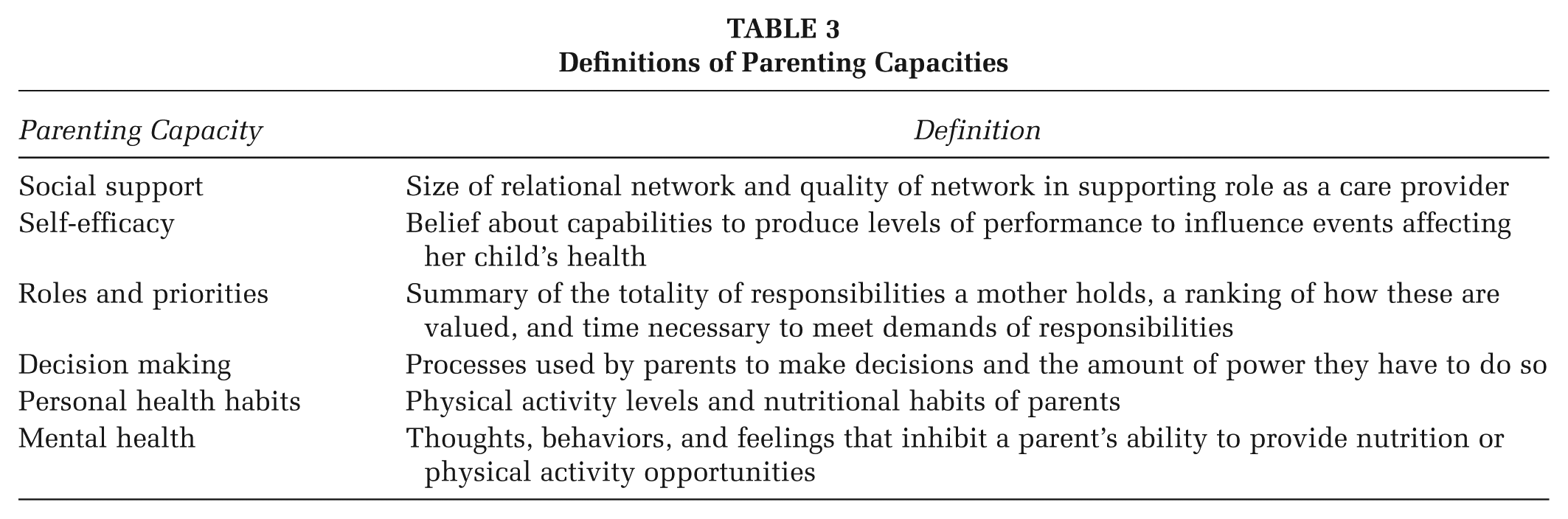
Interview guides were created for two study phases (Table 2). Phase 1 guides were designed to understand if and how participation in the school-based child health program (SHIP) influenced family PAN practices. Phase 2 guides examined how parenting capacities related to key parenting practices to support children’s PAN. Parental capacities were defined as the perceived and expressed abilities of parents to provide their children with healthy food and physical activity opportunities. We developed the following preliminary list of capacities from a literature review and sought to determine their relevance throughout the interviews: (1) roles, priorities, and time; (2) social support; (3) parental physical activity; (4) mental health, stress, and anxiety; (4) self-efficacy; and (5) decision making. Table 3 presents definitions for these capacities. Following the data analysis process, these capacities were organized into a theoretical framework to illustrate their relationship to home-based PAN practices and parental engagement with the SHIP program. Key relationships in the conceptual framework were identified from emergent themes in the data and corroborated with the existing literature on parental involvement in school-based programs and home-based support of healthy PAN practices.
Sample Interview Questions From Semistructured Interview Guide
Definitions of Parenting Capacities
The study relied on the social-ecological model as a framework for understanding the factors that enable or constrain parental involvement in children’s activities. This model was selected, because it considers the complex dynamics between individual (race and gender), relationship (ways families can help engage with goal activities), community (available resources for activities), and societal factors (barriers and dissemination of program information) that allowed the researchers to understand the range of factors that influenced parental engagement.
The SHIP addresses the issue of child health through a variety of strategies and programs. Its Wellness Councils provide a focal point for the program, where parents and staff can come together to create activities or initiatives to make their school healthier. Challenge Clubs are another key programmatic component. These after-school programs give students, especially at risk-students, the opportunity to engage in physical activity and encourage good PAN habits. SHIP works more directly with the school through its Wellness Integration Program and its partnership with Child Nutrition Services. Through its many branches, SHIP is able to affect child PAN through multiple avenues. The program has been recognized by the Centers for Disease Control and Prevention in 2007 and has been replicated in three other school districts in Virginia.
All interviews were conducted between January 1 and May 10, 2012. Interviews were conducted by two faculty members with graduate degrees in public health, one graduate student, and three undergraduate students. All students received training in qualitative research methods before the study began. Interviews were audio recorded and transcribed verbatim. Following transcription, interview content was double coded and checked for consistency by a team of five researchers. Codes were developed deductively from the interview guides and inductively from emergent themes from the interview data. The research team met periodically to refine our coding dictionary in order to ensure data coding used identical definitions. Data were analyzed using NVivo 9 Software to identify key findings within codes. Interview lengths ranged from 20 to 60 minutes, with a mean time of 45 minutes. Parents were only eligible for participation in one interview.
Results
Examples of Enabling Parenting Capacities
Each parent was asked to describe something that they already do, or would like to do, to help their children eat well or be physically active. We prefaced these questions by explaining that our primary interest was in understanding how parents can be involved in their children’s health. Four main parenting practices emerged: shared family goals, meal planning, modeling of healthy behaviors, and collective activities.
Shared Family Goals and Collective Activities
The establishment of shared goals among the family was important to achieving healthful changes in family diet and physical activity habits. Parents created these shared goals by making active decisions to change family nutrition habits or to engage in physical activity with their children. Parents described these goals in terms of what they wanted their children to be doing on a regular basis.
Well, they are supposed to be outside playing as much as possible. All my kids have competed in some type of sport, whether through school or club or something. And both my husband and I are pretty active, so they do things with us. (Respondent 24)
In some cases, these goals reflected seasoned household routines, but in others, they took thought and planning. This planning often involved overcoming barriers to create shared goals.
At first, it was I was in school and I was taking classes so it was more of time, and now I have a little break from school or whatever, so I was trying to incorporate the changes while I don’t have to think as much. So I can focus on eating healthier and getting physical activity myself also. (Respondent 36)
Parents who shared health goals with their children also frequently reported physical activity as a family.
Collective activities were identified as an important part of overall family health because they encouraged parental modeling and helped children be more active. SHIP provided opportunities for collective activity that some parents took advantage of, such as the yearly Sleigh Bell 5K sponsored by the SHIP program. Families identified this event as a culminating experience, marking the end of a semester-long activity, and indicated that this characteristic was important to them. The race provided an opportunity for children to showcase their hard work and offered parents an incentive to train as well.
We made it a family tradition to fun the Sleigh Bell 5K with the kids every year, so that’s something we’re going to do with the family every year and it’s been 2 years in a row that we’ve done it and we’re going to do it again this year. (Respondent 1)
Despite successes in some families, analysis revealed a fundamental division between parent and child physical activity in many cases.
Those things I mentioned—that’s about all we’ll do as a family. As an individual, my wife will sometimes go for a little jog or I think her school has a small fitness center—she’s also a teacher—I think they have one there. (Respondent 21)
Many self-described active parents did not often participate in activities with their children, which resulted in a lack of collective experience and limited opportunities for modeling.
Meal Planning
Meal planning described comments that referred to both the planning and preparation of healthy meals. Time was a major barrier for many parents. Consequently, meal planning was often overlooked. Parental stress and low self-efficacy also hindered meal planning. Parents described that successful meal planning helped promote healthier family eating habits.
[It] helps me when I have a routine—when I get off work, I have certain things I have to do, so when it’s time for dinner, it’s time for dinner, which I’ve started planning for since 4:30—I want them to eat at least by 5:30, no later than 6. And then, so you have enough time to play, to work the food off, and then go get ready for bed at around 9. My routine has a major role. (Respondent 36)
Modeling Healthy Behaviors
Mothers described the need for parents to act as good examples of healthy behavior. Some cited examples of already modeling healthy behavior, while others expressed a desire to improve this in their households. Parents explained that ideal modeling involved parents making changes in their habits that were visible to their children. Healthy parental behavior changes could improve overall family health.
[I think parents should] get out with them. Get out and participate in physical activities with them. Be encouraging. Just participating with them. If they see you do it, they will want to do it and you can do it together as a family, as a team. (Respondent 17)
Parents varied widely in their perception of how their own physical activity influenced the activity level of their children. However, the majority of respondents revealed a disconnect between their personal physical activity habits and those of their children. Many parents did not report extensive personal physical activity habits and reported few instances of joint activity with children.
I would say I would want my children to be outside more. I think they need to go outside and at least bounce the basketball because I am not physically active but I want my children to be. (Respondent 39)
Examples of Constraining Parental Capacities to Children’s PAN
Interviews identified three major barriers to both parental involvement in the school-based PAN program and support for healthy behaviors: time constraints, financial limitations, and family routines. These barriers were examined in relation to the underlying parenting capacities.
Time Constraints and Stress
Of the three major barriers identified, parents described busy schedules and time limitations as the most common barrier to their involvement in school-based programming and their ability to carry out healthy PAN practices in general. One major activity that was affected by busy schedules was meal planning and preparation.
I have a very hectic work schedule so I have to do quick meals. (Respondent 47)
Parents with jobs and other significant responsibilities often found they had to make a trade-off between nutrition and physical activity opportunities for their children. When asked how she felt about the amount of “processed foods” her family ate, one mother responded, I would like to cut it down, but that would mean someone wouldn’t be able to do an activity. (Respondent 41)
Many parents reported that their multiple responsibilities made it difficult to provide proper PAN for their children or to engage in activities with them.
Time constraints created stress for parents that influenced meal planning and parental self-esteem.
If I’m really stressed, [planning and preparing meals] is a job. It’s more of a chore to try to prepare a meal because I’m not really into it. . . . I’ll take the quicker route as opposed to fixing the vegetables and a starch and a protein or something like that. . . . And then I feel bad about it. (Respondent 46)
Stress was a major factor in parental decisions about PAN. Parent’s stress increased in response to worries about child health. When they could not provide their children with physical activity opportunities or nutritious foods, parents noted feelings of guilt.
You have a lot of regret, like gosh, what did I just do with my kids? (Respondent 42)
Parents identified time as a major barrier throughout both phases of interviews.
Financial Limitations
Parents indicated that their family financial situation prevented them from purchasing healthy foods and impeded meal planning. Parents’ ability to act on their preferences for healthy foods was shaped by their basic resources for eating nutritious meals.
We try to have not too much processed food, but we have 5 children, so it ends financially. Economically, it tends to be difficult to buy everything fresh. (Respondent 45)
In many cases, parents demonstrated a gap in knowledge about purchasing cost-efficient healthy foods.
A lot of families that are in situations like that don’t see or don’t know how to balance out or budget for the healthier foods. One of the things we’ve talked about at Weight Watchers is how much more expensive healthy foods are versus processed foods and that’s a real issue if you’re not taught how to shop or eat properly, you’re going to pick what is financially feasible for you. (Respondent 5)
Family Routines
Family behaviors were defined as cultural or familial practices passed from one generation to the next. These routines and habits, past and present, were a strong determinant of PAN behaviors. In some cases, ingrained family behaviors promoted healthy PAN practices. In others, respondents indicated that their culture made healthy habits difficult to adopt.
In my culture, what I grew up around, the foods we ate, I believe it was totally different cooking and it was more Southern soul food type, so lots of grease and fat back and everything might have had a little bit of sugar in . . . and that’s how I grew up and that’s how I learned how to cook. (Respondent 36)
Because parents reported that their parenting strategies and practices were derived from their own parents, extended family behaviors were an important predictor of current family health.
I’m sure I look to my parents, I definitely look to older siblings, what they do, and my husband and I always say we try to get the best of what our parents did—to take the best of what they’ve done and put it together. Because we don’t always agree with everything they’ve done, but we definitely look to our elders to see what they’ve done and what works. (Respondent 45)
Underlying Influence of Parenting Capacities
We defined parenting capacities as the perceived and expressed abilities of parents to provide their children with healthy food and physical activity opportunities. The capacities we identified were discussed with each parent interviewed, and major themes emerged that related these capacities to parenting practices.
Social Support
Families in our study noted varying levels of social support; however, the majority of parents reported little social support, and interviews indicated a latent desire for more help with providing proper PAN opportunities for children.
It’s mainly me. I get them where they need to be. . . . Usually I’m the one that goes out and buy more of the solid foods, things that we need. If I send [my husband] to the store, we’re subject to get donuts and potato chips and quick meals. (Respondent 47)
Parents noted that social support could help mitigate the negative effect of time on healthy parental practices. Some parents noted that support from friends or family increased their knowledge about available healthy foods.
Actually, a girlfriend told me it was a little cheaper—or more reasonably priced and all the foods are more fresh and don’t have all the extra hormones in and you actually know what you’re buying and so I was, like, good idea. (Respondent 36)
The presence of social support was limited among parents in the study population. Parents reported having few people to turn to for information and mostly used social support to mitigate stress instead of to gain knowledge.
Self-Efficacy
The perceived inability to purchase health foods negatively influenced parental self-efficacy for eating healthy as a family. Parents simultaneously expressed a desire to change their family meal structure and an inability to do so.
I think, the biggest thing I’d love to change is if I could eat healthier and have better selections here. We eat a lot of cheese and pasta, and I think there are better alternatives, but it’s not going to happen because financially, it’s not going to happen right now. (Respondent 45)
At first, many parents had little to say in response to the question about their level of confidence in providing healthy meals and physical activity opportunities. We then probed to ask, “What one thing would help you to feel more confident in your ability to provide healthy meals for your family?” Meal planning was a focus of parental desire for improvement. Some parents desired more ways to prepare healthy foods, including meats.
The cost of healthy food also influenced parents’ self-efficacy for purchasing healthy foods.
It’s hard providing [healthy foods] in this economy—it’s certainly more expensive to have the healthier foods, the organic foods in your home. I used to do all organic foods before my husband did his career change. . . . I sympathize with families who can’t provide those things and live on the processed or canned foods and I wish there was more access to some of the healthier foods that would benefit my family more. (Respondent 42)
Roles and Priorities
Parents often mentioned a conflict between their ability to provide healthy meals or physical activity with their many other responsibilities. This was especially a problem in single-parent households or families with a working mother. In some cases, participation in extracurricular activities and sports stood in opposition to “balanced” and “home-cooked” meals for families. A parent described how the family agenda was in competition with healthy eating: We tend to go out here and there. More often than we probably would if we weren’t so loaded up with appointments or after-school activities. So that’s going to be a less healthy choice to go out and have a hamburger somewhere. (Respondent 45)
Many parents described their preference for keeping a regular dinnertime and evening schedule, even if maintenance of this routine was difficult. Parents cited the weekends as a time when they could focus on family meals and health eating, more so than during the school week.
Decision Making
Decision making related to nutrition and physical activity was highly variable between families. Parent’s particular work situations and child personalities contributed to how household decisions were made. However, two common themes emerged from respondents. First, parents could easily describe an established system for how nutrition decisions were made in households. Second, many parents in two-partner households described some form of shared decision making.
My husband and I pretty much do everything together, so it’s a 50/50 for us. I guess you could say whoever is shopping at the time. When I wasn’t working, I shopped more, so it was me, but now he shops more. (Respondent 45)
Key factors that influenced family decision making about nutrition were media, child opinion, family history, and concerns for child health. Family history of nutrition-related disease and concern for child well-being were two of the most frequently noted influences.
Many mothers expressed the importance of making sure their child valued a healthy lifestyle.
No, I think it’s about the same and I think that my job as a parent is to—particularly with nutrition and exercise—make it so my children don’t think those are dirty words. So they know they have to think about nutrition. (Respondent 38)
Parents concerns about past health-related habits and their families’ future health status influenced parents’ decision making about their children’s nutrition and physical activity.
Personal Health Habits
While some parents noted a connection between their own health and that of their children, many parents indicated disconnection between their physical activity and that of their children. Some parents believed their own physical activity “doesn’t affect them at all” (Respondent 47). Regardless of whether parents could identify the importance of modeling physical activity, almost all parents described a desire for their children to be healthy and active. Yet parents rarely structured time to engage in physical activity with their children. Instead they emphasized that children get regular activity, albeit unstructured physical activity.
We’re pretty active people. We don’t have any set schedule of the exact things that we do . . . but overall, it’s just an idea that we’re outside all day long doing all sorts of things. (Respondent 25)
Walking was commonly cited as an activity families engaged in. Overall, parents understood the importance of physical activity for their children but not necessarily themselves.
Mental Health
Mental health was a difficult subject to obtain information on due to reluctance of respondents. However, multiple parents elaborated the role of stress in their lives. Stress had a large effect on meals for many families. The general result of more stress was less thought given to meal planning. One parent summarized the overall situation: If I’m having a very stressful day, I might say let’s go through the drive-through and get something because I don’t feel like cooking. (Respondent 39)
Stress seemed to have a less direct effect on children’s physical activity habits. However, shuttling children from one activity to another was a stated cause of stress in multiple families. Parents also recognized their stress could have a negative effect on their children’s attitude.
If I’m stressed, they’re stressed because they feel it and they can feel the tension and nobody wants to be around anyone. (Respondent 46)
While a few parents described that their stress affected their children, most acknowledged that stress had a negative impact.
Often, stress compounded with other barriers, such as time and finances, to produce greater anxiety. Parents felt they needed to provide better nutrition for their children and expressed worry or fear because they did not feel able to provide a resource that they identified as valuable for their children.
Interview findings were used to develop a conceptual frameworks of barriers to parents’ involvement in school-based PAN programming (Figure 1) and of the influences of parenting capacities on key practices that were identified as important for establishing healthy PAN routines in households (Figure 2).
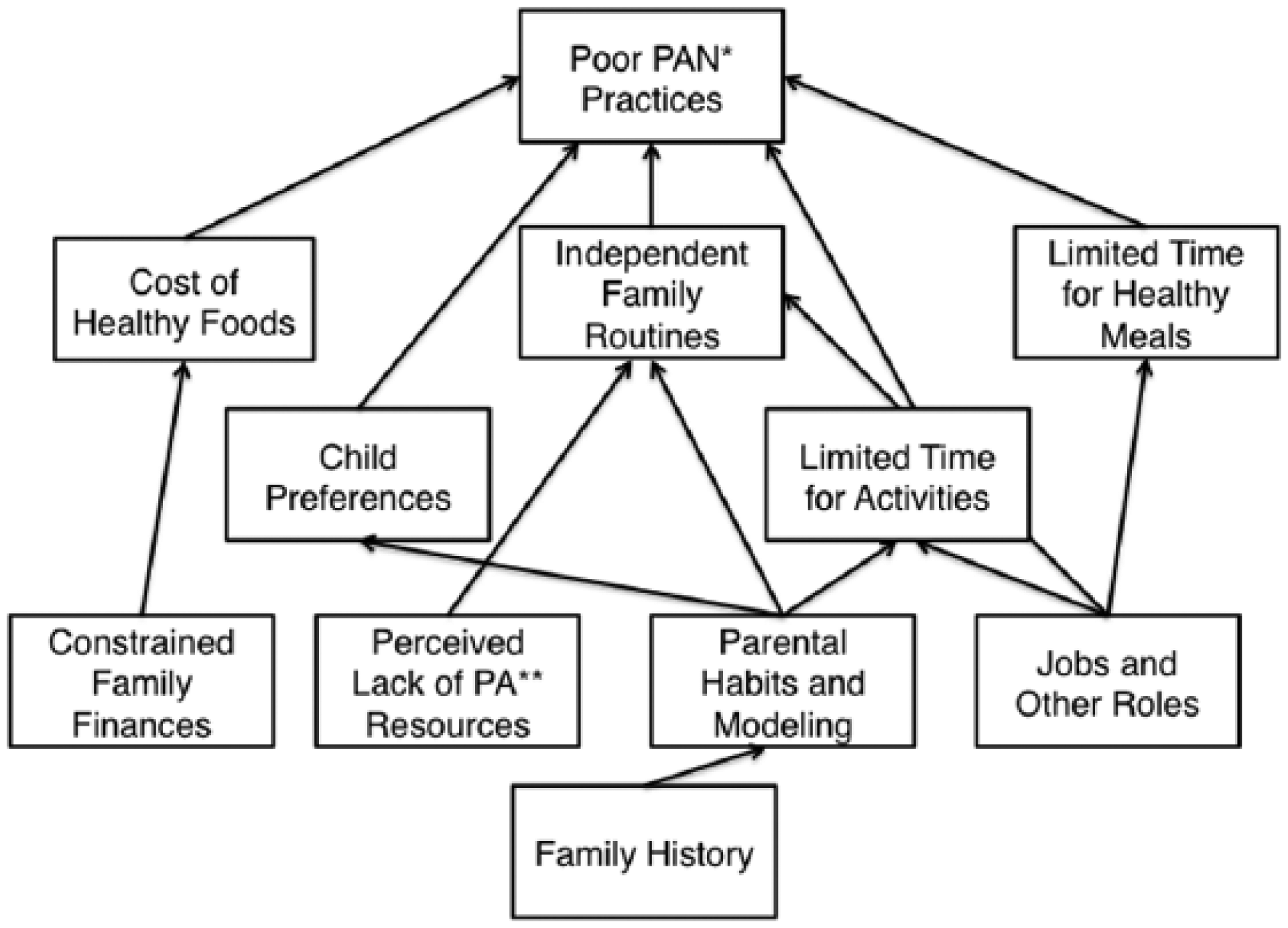
Relationships of Underlying and Immediate Influences of Unhealthy PAN Practices
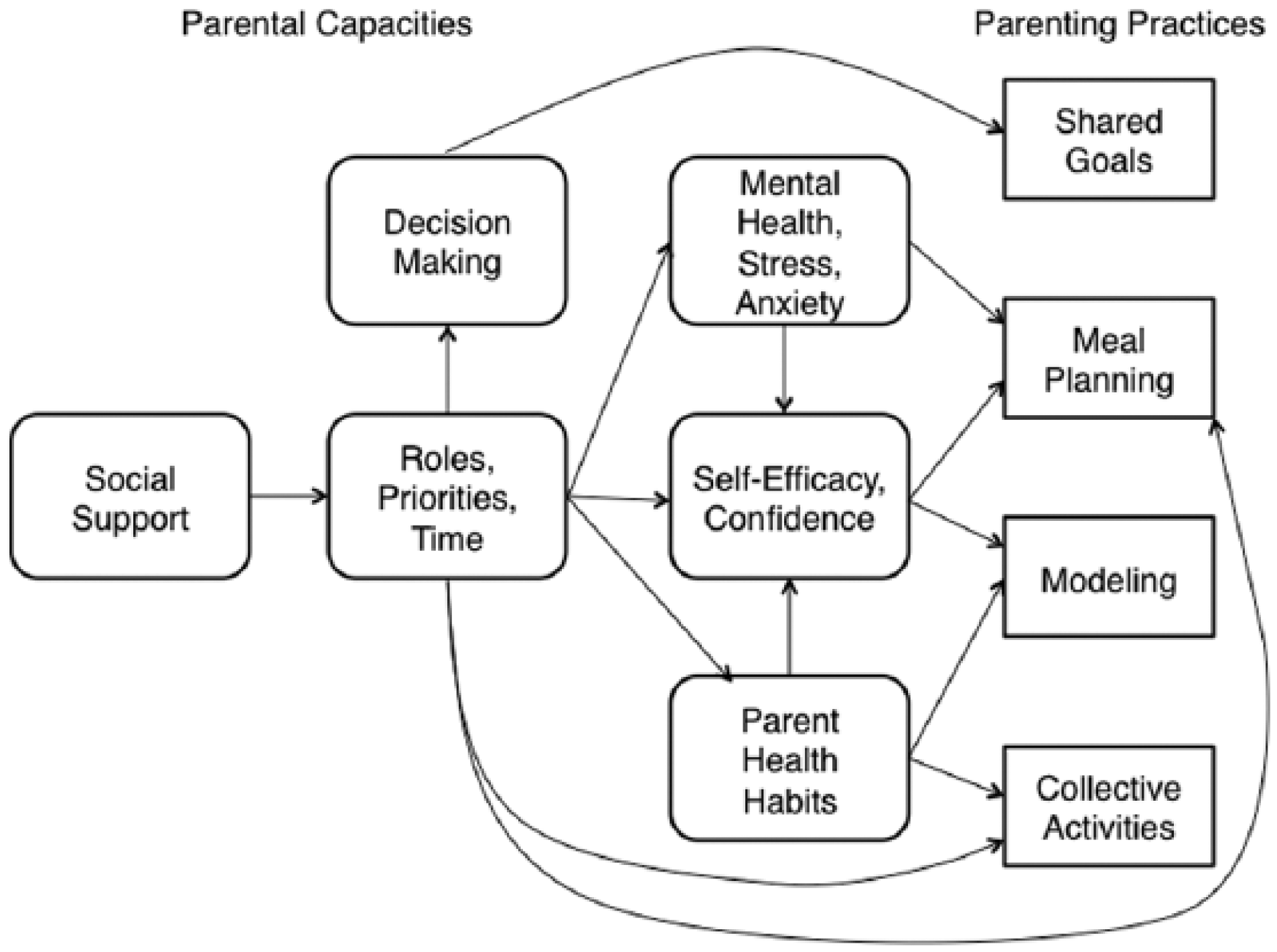
Relationships Between Parenting Capacities and Parenting Practices
A lack of social support among parents surveyed made it difficult for them to overcome barriers such as family financial situation and ingrained family routines. Advice from the community or support from specific family members could help parents find ways to buy healthier foods, but it is currently lacking for many participants in the study. Social support is also crucial to help parents deal with other barriers to meal planning and participating in activities with their children, such as time. Social support can increase parental ability to deal with roles, priorities, and time (Figure 2).
Discussion
The involvement of parents in school-based programs, and in children’s PAN more broadly, is an important and modifiable underlying influence of children’s nutrition. The results from this study provide support for the hypothesis that the abilities of parents to perform nutrition and physical practices relate to interrelated capacities for parenting. Our findings shed light on how these capacities relate to healthy and unhealthy familial PAN practices among members of a low- to middle-income population that is currently experiencing an obesity epidemic.
Our analysis found that time is the biggest barrier to parental support and healthy parenting practices. A similar study by Kipping et al. (2012) also found that work, which many of our respondents mentioned as a cause of time constraints, was a major barrier to parental involvement in children’s PAN. Capacities related to roles, priorities, and time affect the other capacities in a variety of ways. Limited time leads to poor meal planning, little collective activity, and overall poor parental modeling. Family goals are also restricted by time because families will often decide to prioritize other issues over proper PAN. Limited time also produces stress, which interferes with proper meal planning and decreases self-efficacy. Findings suggest that parents have a substantial knowledge regarding what is healthy but do not act on their knowledge. Parental stress and low self-efficacy can explain why parental knowledge and action are not always compatible.
Responses throughout the interviews suggest that parents perceive they are unable to provide healthy nutrition or physical activity opportunities. Weak parental capacities undermine the ability of parents to act on their own nutritional knowledge or use resources available to them because barriers are perceived as more serious. Parental perceptions must be addressed along with barriers to effectively involve parents in programs like SHIP.
In the case of school-based programs, opportunities for discussion between parents and program staff provides social support and can increase efficacy. Similar techniques in other school-based settings have helped increase parental knowledge and skills for providing healthy nutrition for children (Haire-Joshu et al., 2008). Past studies show parents with low self-efficacy will seek these programs out (Garvey, Julion, Fogg, Kratovil, & Gross, 2006). Engaging parents in program planning has also been shown to be an effective type of parental involvement (Golley et al., 2011). Engagement in program planning can be problematic if parents demonstrate a desire to minimize the time of their participation, leading to less direct involvement (Fitzgibbon et al., 2011). But direct parental involvement in programs has also been associated with programmatic success in changing child dietary habits (Hingle et al., 2010). The correlation between parental involvement and success supports the recommendation to provide parents with ways to actively become involved in the Challenge Clubs. In one study, 66 percentage of parents reported changing their own eating habits after attending two information sessions, demonstrating the positive effects of parental involvement (Kain, Uauy, Albala, Cerda, & Leyton, 2004). Finally, we hope that involving parents in the planning of SHIP Challenge Clubs will overcome any concerns further preventing parents from supporting the program as parental concerns or confusion can act as a barrier (Garcia-Dominic et al., 2010). Parental support of programs is extremely powerful, and our strategies aim to encourage it in SHIP and similar programs (Chang, Gertel-Rosenberg, Drayton, Schmidt, & Angalet, 2010).
Our study was limited by several factors. We collected limited demographic information on participants, apart from racial/ethnic group. We found no substantial difference between participant groups by racial/ethnic group. Thus, we do not report results separately by this or other demographic characteristics. However, it would be useful to add more detailed demographic data, such as household income level and the number of school-aged children in the family, in order to stratify the sample by these potentially meaningful characteristics given the potential importance of such factors on parental uptake of school-based programs. Although a full ethnographic record was not collected, careful notes on the interactions within the group and the surroundings were preserved, coded, and analyzed with the purpose of collecting valuable ethnographic data for the focus group. Preserving this information provided an added analytical dimension through the ability to categorize and connect the themes by social dimensions. Specifically, this record revealed an important theme of engagement, which was translated into the recommendation for improving parental involvement with SHIP to be more participatory at the outset to improve the likelihood that recipes are used by families and incorporated into the caregiver meal routine.
Implications for Research and Practice
We applied our study results to develop strategies for improving parental involvement in the SHIP program (Table 4). Some of our recommendations, such as an expansion of the SHIP Challenge Clubs, were tailored specifically to this program. Programmatic expansions are beneficial because preventing obesity is easier than treating it, making enforcing good habits at young ages critical (Olstad & McCargar, 2009). Other strategies can be applied more widely to other school-based programs and to address parental capacities.
Strategies for Improving the SHIP and Justification
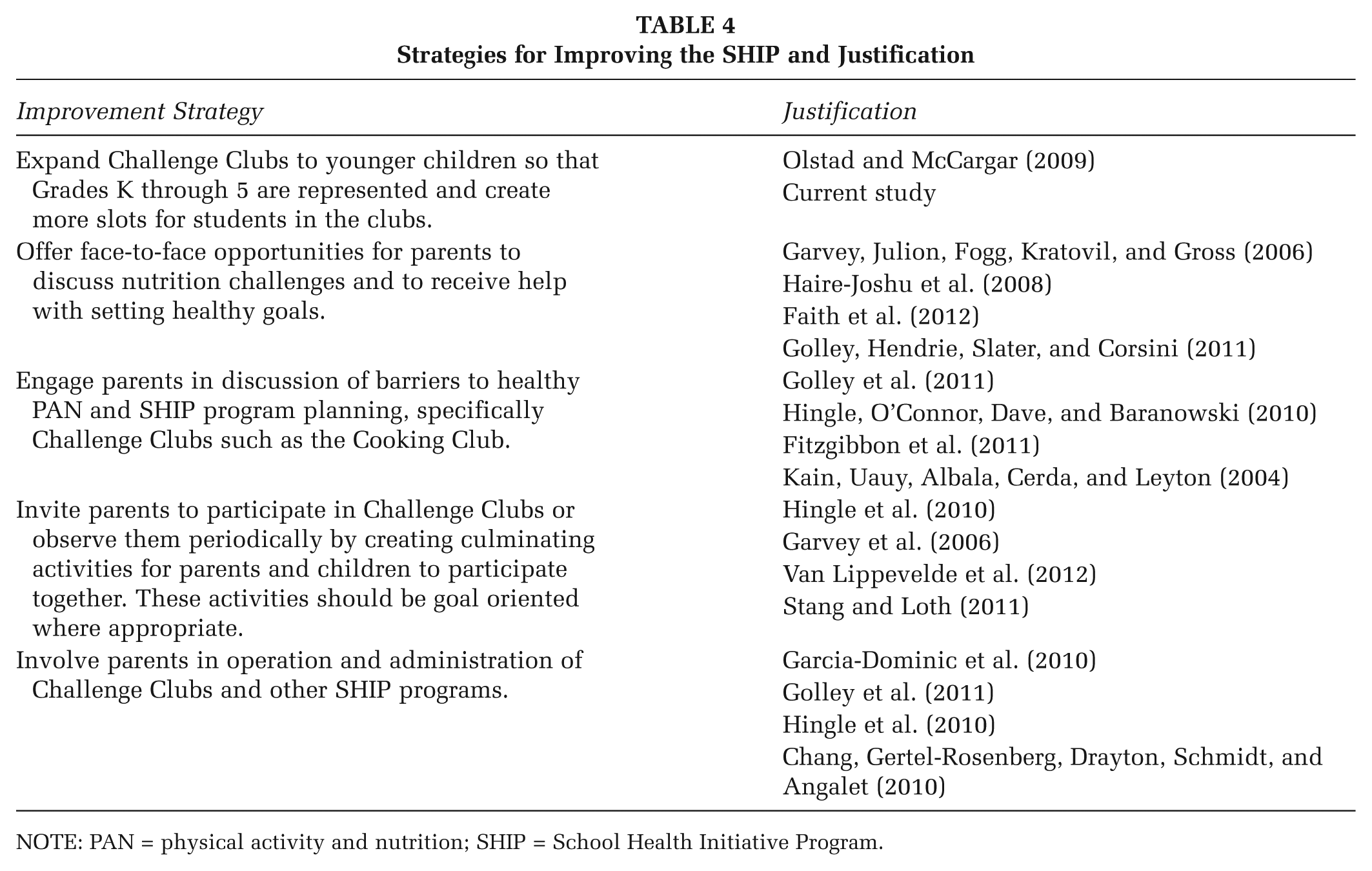
NOTE: PAN = physical activity and nutrition; SHIP = School Health Initiative Program.
As school-based programs evolve to reflect a growing interest in parent involvement, our recommended strategies may provide an useful example for other similar programs. The heterogeneity of programs makes it difficult to determine exactly which forms of parental involvement are most effective (Kipping et al., 2012). Therefore, understanding the major barriers to parent involvement will allow parental involvement components to target the most critical barriers and become more uniform. In addition, the parenting capacities framework we have applied can be used to understand influences and impacts of parental involvement and parenting practices in other communities.
Footnotes
Acknowledgements
The authors wish to thank Jane Ickes for her help in transcribing the interview transcripts. We also thank Grace Sherman for help in recruitment of study subjects and Catherine Alyssa Brahe for help in conducting study interviews.
SI conceived the study, secured funding, collected and analyzed the data, and coauthored the article. AR, CD, and EM collected and analyzed the data and coauthored the article. All authors read and approved the final article.