
Abstract
Objective. To evaluate a training workshop for law enforcement as first responders for the purpose of increasing officers’ cultural competency in working with Deaf and hard-of-hearing people (Deaf/HH) during domestic violence (DV) emergencies. Method. This evaluation assesses the efficacy of a 2-hour training workshop for law enforcement. Thirty-four participants completed questionnaires at pre- and postintervention to assess participants’ (1) satisfaction with training; (2) skills in responding to Deaf/HH individual(s) in a DV emergency; (3) attitudes toward the Deaf/HH, including bias recognition, self-assessment of cultural competency, and perceived self-efficacy; and (4) knowledge of communication. Focus groups (FGs) were also conducted (n = 6 for FG1, n = 13 for FG2). SPSS software was used to analyze survey data; principal components analysis was conducted on the survey instruments. Results. There were significant differences between pre- and posttests for several targeted outcomes, including knowledge and perceived self-efficacy. Both survey and FG results demonstrated that participants gained cultural competency skills as indicated by changes in attitudes toward the Deaf/HH, both in DV emergencies and in large-scale emergencies. Conclusion. Significant differences were evident between pre and posttest results in terms of knowledge and perceived self-efficacy. Nonetheless, survey participants demonstrated a lack of knowledge about policy and the law. Survey findings also suggest that while a onetime training can improve the perceived self-efficacy of participants, shifting attitudes about the capabilities of the Deaf/HH may require different training strategies. FG participants demonstrated a greater awareness of the complexity of working with this population in a DV emergency.
Keywords
Introduction
An estimated 36 million Americans are Deaf or hard of hearing (Deaf/HH; National Institute on Deafness and Other Communication Disorders, 2012). Although there are few reliable statistics on the incidence of domestic violence (DV), according to a study by Pollard, Sutter, and Cerulli (2014), Deaf respondents reported higher rates of some forms of interpersonal violence. According to the Centers for Disease Control and Prevention (2011), interpersonal violence causes approximately 2.2 million medically treated injuries annually, at a cost of $37 billion, which includes lost productivity. Survivors of violence are more likely to experience mental and physical health problems from posttraumatic stress disorder to depression, cardiovascular disease, and diabetes (Meyer, 2010).
Studies have examined cultural competency training for medical professionals working with the Deaf but not for first responders in DV emergencies, including police and firefighters, who work with the Deaf/HH 1 (Boyd, 2011). Past research underscores the importance of cultural competence training for health professionals and first responders working with ethnic minorities (Dass-Brailsford, 2008; Harris, McQuery, Raab, & Elmore, 2008; Reimann, Talavera, Salmon, Nuñez, & Valesquez, 2004; Webb & Sergison, 2003). Cultural competency training can help professionals communicate with the Deaf/HH in DV incidents (Obinna, Krueger, Osterbaan, Sadusky, & DeVore, 2005).
Research has shown that the ability to understand emergency communications messages is significantly impaired during a time of stress (Centers for Disease Control and Prevention, 2011; Vanderford, Nastoff, Telfer, & Bonzo, 2007). Deaf survivors of DV are often further vulnerable due to communication obstacles (Anderson & Kobek Pezzarossi, 2014; Pollard et al., 2014). For the Deaf/HH, the challenges of locating and evaluating information for credibility and analyzing relative risks are more pronounced (Ad Hoc Committee on Health Literacy for the Council on Scientific Affairs, American Medical Association, 1999). Language and cultural barriers with first responders can make typical services (shelters, legal advice, and medical assistance) difficult to obtain for the Deaf/HH (Boyd, 2011).
With the aim of improving first responders’ capacity to respond to the Deaf/HH, it is hypothesized that gaps in the knowledge of law enforcement officers have negative repercussions for the Deaf/HH. Trained officers can become more culturally competent and effective in responding to the Deaf/HH and thereby provide better services. Increased awareness about the needs of Deaf survivors in the legal system may lead to important policy changes in emergency management.
Moreover, studies examining attitudes toward people with disabilities by medical professionals have found that providers who have more frequent contact with people with disabilities have more personal acceptance of people with disabilities (Antonak & Livneh, 2000; Kottke, 1987; Mitchell, Hayes, Gordon, & Wallis, 1984; Tervo, Azuma, Palmer, & Redinius, 2002; Tervo, Palmer, & Redinius, 2004).
Thus, we examined whether exposure to a Deaf trainer, as well as receiving training about working with the Deaf community, could improve attitudes, in addition to knowledge and skills, among emergency responders. Cultural competence training is useful for first responders in emergencies given a lack of widespread awareness of disability culture (Barnes, Oliver, & Barton, 2002; Davis, 2006; Drum, McClain, Horner-Johnson, & Taitano, 2011; Office for Victims of Crime Office of Justice Programs, 2009; Fleischer & Zames, 2001).
DeafHope, a nonprofit organization that serves Deaf/HH survivors of DV, in partnership with the Oakland Police Department (OPD), aims to develop a model training framework to create access for safety for the Deaf/HH. This current study assesses the efficacy of a training workshop for law enforcement on how to interface with the Deaf/HH as first responders at the scene of DV emergencies (see Table 1).
Learning Objectives
Method
Study Design
This study is designed to measure the domains of a tripartite model widely used in cross-cultural education: knowledge, skills, and attitudes (Chiu, Lonner, Matsumoto, & Ward, 2013, Harris et al., 2008).
Recruitment
Individuals working in law enforcement in the San Francisco Bay Area were eligible to receive P.O.S.T. (Peace Officer Standards Training) certification in California. Recruitment efforts were focused in Oakland, and later expanded to include San Francisco, Contra Costa, Alameda, and Sonoma counties.
Participants
A total of 41 training participants, ranging in age from 24 to 51 years, attended one of two available trainings. Sixteen participants attended the first (10 male), and 25 participants attended the second (16 male). Of the 34 survey respondents, 21 participants (62%) were male.
Procedure
Intervention
DeafHope provided 2-hour cultural competency training sessions on two separate occasions to law enforcement officials with the objectives of improving communication, knowledge, and skills when working with Deaf survivors (Table 2). The training, cotaught by one law enforcement representative and one Deaf instructor, was conducted using a combination of lecture, interactive activities, and a Q/A discussion. American Sign Language interpreters facilitated communication.
Sample Training Content
NOTE: HH = hard of hearing; DV = domestic violence; ASL = American Sign Language.
Law enforcement personnel attended the training workshop, and were invited to (1) take a 15- to 20-minute, 43-item pre- and 48-item posttest survey and (2) participate in semistructured focus groups (FGs) afterwards (see Appendixes A and B; available online at http://hpp.sagepub.com/supplemental).
Measures
Survey items were adapted from several extant, validated instruments: (1) Office of Minority Health (n.d.), (2) American Association of People With Disabilities survey (n.d.), (3) Cultural Competence and Linguistic Competence Policy Assessment (National Center for Cultural Competence, 2006), (4) Course Evaluation Instrument from Peace Officer Standards and Training (Commission on Peace Officer Standards and Training, 2001), (5) Community Emergency Response Team evaluation form (Community Emergency Response Team, n.d.), (6) Self-Assessment of Cultural Competence (Goode, 2009), and (7) Self-Efficacy for Cultural Competence in Patient Counseling Scale (Assemi, Cullander, & Hudmon, 2006). The questionnaire and FG instrument were pilot-tested in consultation with DeafHope and OPD.
Survey items and FG questions measured baseline and posttraining knowledge and skills of best practices for first responders when communicating with a deaf person involved in a DV or large-scale emergency, as well as attitudes, which include (1) beliefs about the competence of deaf people and (2) perceived self-efficacy measuring current and future behavior.
Survey
Indicators in the quantitative and qualitative survey instrument measured the following: (1) participant satisfaction with the training (13); (2) skills in responding to Deaf/HH individual(s) in a DV emergency (2); (3) attitudes toward the Deaf/HH, including bias recognition, self-assessment of cultural competency, and perceived self-efficacy (16); and (4) knowledge (32) about communication with the Deaf/HH (12), translation (American Sign Language interpreters) (12), accessible technology (2), myths about deafness (4), legal rights of Deaf/HH individuals (1), and language access and barriers (1; see Appendixes A and B).
Attitudes Scale
A 16-item Likert-type scale was used in both pre and postsurveys to compare attitudes toward the Deaf/HH with response options ranging from strongly disagree to strongly agree. This scale comprised two subscales assessing (1) perceived capabilities of Deaf people (6 items), which included items such as “Deaf people can make their own life decisions,” and (2) perceived self-efficacy when working with the Deaf/HH with 10 items, such as “I feel confident I could figure out a way to communicate with Deaf people in an emergency.” The overall Attitudes scale exhibited good internal reliability (Cronbach’s α = .88 pretest, .89 posttest).
Communication Strategies Scale: Knowledge and Skills
A three-item dichotomous true/false response format was used to address some common myths about communication methods with Deaf people, such as the use of children as interpreters. Tetrachoric correlation on the Communication Strategies scale indicated good reliability. In addition, a case study of a DV emergency scenario involving a deaf person with a hearing abuser was presented, and respondents were asked to consider what they would do in that situation using qualitative, open-ended questions about communication and language access.
Participant Satisfaction
Posttraining, participants were asked to rate the quality of the training and any improvement in their knowledge, skills, and sense of self-efficacy or readiness to work with the Deaf/HH in an emergency. A combination of Likert-type scales and open-ended questions was used.
Focus Groups
Focus groups were semistructured; 15 questions covered the following thematic areas: (1) prior experience with the Deaf/HH, (2) perceptions of the Deaf/HH, (3) perceived skills in working with the Deaf/HH, (4) knowledge about Deafness, (5) knowledge about communication with the Deaf/HH, (6) knowledge of language access and barriers, (7) knowledge of community resources, and (8) participant satisfaction, which included a self evaluation of any improvement in participants’ knowledge, skills, and sense of self-efficacy or readiness to work with the Deaf/HH in an emergency.
Analysis
Pre- and Postsurveys
Data were examined for normality, and it was determined that parametric statistics should be used. Principal components analysis (PCA), a form of multivariate analysis to estimate the reliability of our questionnaire, was conducted on the Attitudes scale. Based on PCA results, the Attitudes items were split into two subscales: capabilities and perceived self-efficacy. Paired t tests were run on these two Attitudes groups separately to discern differences in the means of pre and post scores. SPSS software was used to conduct paired t tests for all 34 participants. Tetrachoric correlations were conducted on the knowledge and skills items to determine normal distribution of dichotomous variables. The open-ended questions were analyzed qualitatively to better understand and supplement the quantitative findings.
Focus Groups
Content analysis of transcripts from both FGs was conducted, which included coding, concept mapping, and thematic analysis of the text (Lincoln & Guba, 1985). Literal and analytical codes were developed in an iterative and reflexive process in Microsoft Excel and quotes were linked to participants’ demographic information. Transcripts were created in real time using CART (computer-assisted real-time transcription).
Results
Quantitative Survey Results: Attitudes
Participants who were multilingual, M = 40.39, t(32) = −2.33, p = .03, or had prior experience with the Deaf/HH, M = 39.59, SD = 6.24, t(30) = −2.95, p < .01, had greater perceived self-efficacy at baseline, compared with monolinguals, M = 35.51, SD = 6.02, or those without prior experience, M = 34.02, SD = 4.69; Figure 1). Overall, the training had a positive impact on perceived self-efficacy, t(33) = −5.02, p < .01, but no significant impact on capabilities, t(33) = −0.34, p = .74; Table 3). Pretraining differences between those who were multilingual or had prior experience with the Deaf/HH with the rest of the participants narrowed to a nonsignificant margin posttraining, indicating the trainings’ benefits.
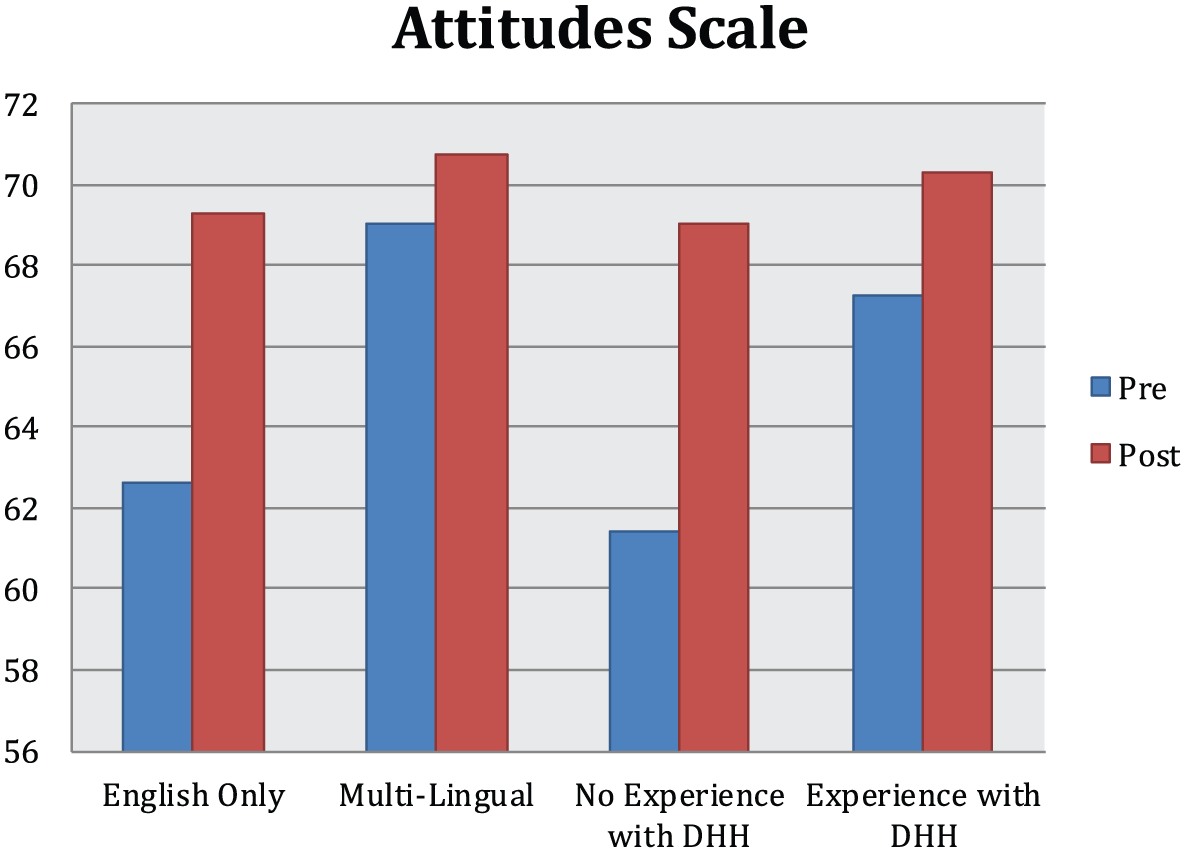
Mean Attitudes Scale Results by Languages Known and Prior Experience With the Deaf
Survey Results

Qualitative Survey Results: Knowledge
Among other questions, participants were asked to list three legal rights that the Deaf/HH have. Only 3 out of the 25 that responded to the presurvey question (12%) mentioned interpreters. Posttraining, 24 participants out of the 32 that responded (75%) mentioned interpreters. However, posttraining, only three participants (9.4%) were able to mention two laws by name—The Americans With Disabilities Act and Section 504 of the Rehabilitation Act (1973)—despite the fact that they were informed of these laws.
Focus Group Results
Ten interpretive codes emerged from both FGs, in order of frequency: attitudes (66), cultural issues surrounding law enforcement (59), participant satisfaction (59), knowledge about the Deaf/HH(40), potential communication solutions (26), responsibility of stakeholders (16), field experience (13), barriers in emergency response (11), involvement of the Deaf/HH (6), and skills/self-efficacy (2). Responses mirrored survey responses in terms of improved awareness of the needs of Deaf/HH individuals in DV emergencies. A female detective discussed the potential for miscommunication: I can see that if an officer does not know some of the stereotypes about lipreading . . . an officer assumes they . . . should take that as resistance or . . . Just not cooperating with the system.
Praise
Several officers voiced enthusiastic praise for the training: This could be a big jumping point for DeafHope working more with law enforcement. This is just the tip of the iceberg . . . (Female officer) It was brilliant . . . To attend a course led by a deaf person was amazing . . . (Male officer) [The training] made me more aware of how ill-prepared I am, and things to work on. (Female detective)
Perceived Self-Efficacy
After the training, participants in both FGs expressed great uncertainty about responding to the Deaf community during a large-scale emergency. After being questioned about this, despite the fact that a female child interview specialist had prior experience with the Deaf/HH, she said, “Goodness gracious! I don’t know.” A female detective, with no prior experience working with the Deaf/HH, was uncertain when asked to rate her sense of preparedness posttraining from 1 to 5: It’s still going to be tough. I still don’t know if they are going to be able to communicate with me by writing. I . . . know I can’t use children. Not only may they be witnesses. You don’t use witnesses to interpret . . . That changes the dynamics of the story. Then what are you going to rely on? . . . I don’t know anything about signing. I know they can’t read lips. I definitely cannot read lips . . . Where do I go from here? At 3 or 4 in the morning when I get called out, what do I do?
A male detective worried, “How do I communicate real quick? If you are triaging down a disaster, how do you get people going using the least amount of communication?” Two colleagues, a male officer and a female detective, both of whom had no prior experience, expressed apprehension:
In terms of actual communication, I think I would be able to get by. I think it would look hideous. I think there would be stick figures and charades and grabbing people and moving them.
I think I could do it [communicate with a Deaf/HH person in an emergency], but yeah, it would be ugly.
Even hideous?
Perhaps even hideous.
Although this exchange was about serious communication barriers, participants found the banter humorous. A male officer with two Deaf/HH family members said that despite the fact that he had prior experience, “I started off with like a 5 or 4. Now I’m down to a 2 [on a scale of 1 to 5 with 5 indicating the most confidence about being prepared to serve the Deaf/HH community].” These responses indicate that the training might have provoked its participants to realize the complexity of communication barriers, rather than their lack of knowledge.
Participant Satisfaction
Participants recognized the benefits provided by the training. A male sergeant who had no prior experience with the Deaf/HH recalled, “A lot of my perception was based off TV. . . . They should be able to lip-read. Everyone can do it on TV. You know, so, I think the last two hours . . . just . . . eliminated a lot of the . . . falsehoods.” Another male officer recognized his own misconceptions: “I think people think the deaf communities are segregated on some island. Really they are not. They are part of our community and we are going to run across them . . .”
However, some FG comments illustrated that this brief training was not sufficient to fully educate officers: I’m aware there are methods for and I want to say TTY. There are methods for the deaf to access 911 . . . (Male sheriff) Note: TTY is a relatively obsolete form of communication. [Reaching Deaf/HH individuals during in an emergency] is not that much different from the general community. What does everyone do? They’ll go to whatever media. Radio or TV or talk to their neighbors. (Male officer) Note: Deaf/HH individuals are unable to access radios.
Interpreters
Several participants demonstrated a desire to provide communication access. A female evidence technician said, “[We need to start] educating everybody in my department—educating my sergeant and lieutenant and [explaining] why it’s a legal issue to get an interpreter and not blow it off . . .”
Need for Training
A story in which a police officer shot a Deaf/HH individual due to miscommunication prompted several participants to recognize that training could save lives.
That officer has to live with that for the rest of their lives. If we could prevent one incident like that because of miscommunication . . . [it would be worthwhile]. (Female detective)
Discussion
Studies measuring attitudes toward people with disabilities among medical professionals have demonstrated that having exposure to disability influences attitudes (Antonak & Livneh, 2000; Tervo et al., 2002; Tervo et al., 2004). Thus, the fact that law enforcement officers received training by a Deaf individual could have improved attitudes, regardless of training content. Despite an even mix of survey respondents having prior exposure to the deaf, most respondents (n = 26, 79%) reported no prior Deaf/HH–specific responder training (including law enforcement, fire, or emergency medical service). However, the majority surveyed (n = 21, 64%) reported prior responder training on disability issues, which indicates that there is a Deaf/HH–specific training gap.
Participants’ improvement in the self-efficacy subscale of the Attitudes scale indicates the potential for positive behavior change. When law enforcement participants encounter Deaf/HH individuals in the future, officials might be more likely to respond in a culturally appropriate way. However, a lack of significant improvement in the items measuring perceived capabilities of the Deaf indicates the following: (1) high initial scores with little room for improvement for some participants, (2) self-report bias, (3) improvement of attitudes about the independence of Deaf people may require more extensive training, and/or (4) some participants overestimated their capabilities at baseline and then realized their knowledge gap in the course of training.
When asked whether the training helped them reflect on their views about people with disabilities, including the Deaf/HH, most respondents answered in the affirmative. Nevertheless, participants continued to have conflicting attitudes and frustrations about their responsibilities toward the Deaf/HH in an emergency. Despite the fact that officers are trained to protect and serve, ingrained in some is the American notion that each individual’s needs are his or her own responsibility (Shain & Lippy, 2010).
Policy Challenges
Posttraining, most respondents were unable to answer an open-ended question regarding their departmental policy on communicating with deaf people. This indicates officers learned about the critical importance of interpreters but did not necessarily understand the need for a trained or certified interpreter or the specific laws behind communication access for the Deaf/HH. This may indicate that determining the right way to communicate at the time of an emergency is not always clear-cut, despite the general legal requirement for police departments to provide effective communication pursuant to Title II of the Americans With Disabilities Act (Smith, 2010; Summit County Sheriff’s Office & City of Lorain Police Department, 2004).
Triangulation of Data
Due to self-report bias, participants may have overrated their knowledge and perceived self-efficacy before training. Due to social desirability bias, survey participants may overrate their positive attitudes toward the Deaf/HH. However, in the FGs, participants who had originally rated themselves highly rated themselves lower posttraining. One explanation is that after the FG discussed the complexities of working with the Deaf/HH in emergencies, participants knew enough to admit their shortcomings.
Perceived Self-Efficacy
Neither FG felt adequately prepared to communicate with the Deaf/HH, let alone in an emergency situation. Both groups agreed that in an impending large-scale disaster, effective communication with the Deaf/HH is not feasible but can be done in queue while serving the needs of other populations. However, the first group seemed to have more knowledge of resources at their disposal that they used to reason through the disaster scenario. By contrast, the second group seemed unable to communicate an appropriate action plan for a large-scale disaster. The loudest voice asserted that in an emergency of that size, it is not first responders’ responsibility; it is incumbent on Deaf/HH people to be prepared.
Strengths and Limitations
To our knowledge, this is the first documented mixed-methods evaluation of law enforcement training in DV emergencies involving the Deaf/HH. Although the survey and FG instrument was new and we lacked a control group, investigators went to great lengths to ensure the reliability and validity of the instruments. For example, we used a theory-based approach, the tripartite model, to target specific concepts; drew on documented measures in related fields to generate survey items; had Deaf/HH experts review the instrument before administration; and pilot-tested the instrument with the target population to provide further refinement and triangulated survey and FG data. Scale, concept, and item development were all done in consultation with DeafHope staff and OPD officials, which maximized the strength of a culturally based approach. In addition, PCA testing on our scales exhibited strong internal reliability.
Findings support prior research about the benefits of cultural competence training for health professionals working with minorities; findings add an evidence-based research component to the small but growing literature on emergency preparedness and disability. Nevertheless, without longitudinal data, it is difficult to determine whether the material will be retained or applied in the field. The predictive validity of attitudes on future behavior is not well established in the literature (Ajzen & Fishbein, 2005). However, direct experience with the attitudes object, such as a Deaf/HH trainer, was found to be a moderating factor that could help predict future behavior.
Due to resource limitations, this study only measures short-term outcomes. The training provides continuing education; therefore attendees may be more motivated at baseline and thus more likely to have increased knowledge or sensitivity about Deaf issues. Regardless, this research is an important first step in determining the efficacy of this training.
Conclusion
This study contributes to the literature on DV and emergency response in the Deaf/HH community by exploring barriers, attitudes, and perceptions from the perspective of law enforcement personnel. Understanding and responding to the needs of law enforcement that interface with some of the 36 million Deaf/HH Americans can significantly advance culturally competent DV response for all populations, with particular relevance for linguistic minorities.
Study findings underscore the need for a standardized curriculum given that the few Deaf/HH–specific DV trainings available frequently lack evaluation and quality control measures. This study builds on previous research for developing best practices for emergency preparedness training and dissemination of an evidence-based curriculum across Deaf/HH–serving nongovernmental organizations (Engelman et al., 2013; Ivey et al., 2014; Neuhauser et al., 2013). Fragmentation of existing training efforts can hinder the resilience of Deaf/HH and other vulnerable populations. Integrating resources, strengthening public/private partnerships, increasing cultural competence of first responders, further evaluating existing trainings, and standardizing policy can enhance resilience in the diverse Deaf community.
Governmental agencies, first responders, and nongovernmental organizations can benefit from this evaluation of a Deaf/HH–specific DV training program for first responders, which can lead to the development of best practices to handle communication barriers that may emerge during a DV emergency.
Footnotes
Acknowledgements
Special thanks to Julie Rems-Smario, former executive director of DeafHope, and Randy White of the Oakland Police Department for making this community–academic partnership possible. Colleagues at Health Research for Action and members of the National Advisory Board on Emergency Preparedness Communications for the Deaf and Hard of Hearing provided guidance in the selection of research areas based on community-identified concerns.
This study was supported by a Preparedness and Emergency Response Research Center grant from the Centers for Disease Control and Prevention, under FOA RFA-TP-08-001, to UC Berkeley (Grant No. 5P01TP000295). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.