
Abstract
This study identified inconsistencies in physical activity (PA) reported at screening and baseline of a 6-month health promotion intervention and explored how these inconsistencies influenced intervention effectiveness in African American and Hispanic women. Participants completed a telephone screener to determine eligibility for a PA intervention. Inactive participants (≤90 minutes of PA/week) were invited to a baseline assessment, where they completed the International Physical Activity Questionnaire, measuring work, transportation, gardening/housework, and leisure-time PA. Women returned after 6 months to complete an identical post-intervention assessment. Despite being screened as inactive, baseline Questionnaire data indicated that 85.0% of participants (N = 274, M age = 44.6 years, M body mass index = 34.8 kg/m2) were active (>90 minutes of PA/week). Women who reported any work-related PA were 20.9 times more likely to be active at baseline than those who did not (p < .001). Participants who were inactive at both screening and baseline reported greater increases in domestic and gardening PA and total PA from baseline to postintervention (ps < .05). Overweight/obese ethnic minority women may misreport being physically inactive during screening if specific questions about type of PA are not included. Post hoc analyses controlling for screening inaccuracies may improve effectiveness of PA interventions and help intervention programs reach women who may benefit the most.
Introduction
Physical inactivity and low physical activity accounted for over 200,000 deaths in the United States in 2010 (U.S. Burden of Disease Collaborators, 2013). Ethnic minorities, low-income populations, and women continue to suffer from health disparities related to physical inactivity (Centers for Disease Control and Prevention, 2007; Katzmarzyk & Staiano, 2012). Despite the evidence and numerous interventions to increase physical activity in ethnic minorities and women (Cleland, Tully, Kee, & Cupples, 2012), African American and Hispanic women in the United States remain insufficiently active (Gaskins, Baskin, & Person, 2012; Ladabaum, Mannalithara, Myer, & Singh, 2014), largely due to family priorities, gender and familial roles, and cultural and neighborhood barriers (Eyler et al., 1998; Eyler et al., 2002; Richter, Wilcox, Greaney, Henderson, & Ainsworth, 2002). Behavioral interventions that aim to increase physical activity among African American and Hispanic women have demonstrated mixed results (Cleland et al., 2012). Some have shown a significant increase in physical activity (Duru, Sarkisian, Leng, & Mangione, 2010; Hornbuckle et al., 2012), while others show no change in physical activity over time (Parra-Medina et al., 2011; Wilbur et al., 2008). Although some of the discrepancy in the effectiveness of physical activity interventions is accounted for by differences in study methodologies and measurement (Ferrari, Friedenreich, & Matthews, 2007; Slootmaker, Schuit, Chinapaw, Seidell, & van Mechelen, 2009), some of the discrepancy may be accounted for by inconsistencies in the participant screening process.
Most community-based interventions target insufficiently active individuals in the general population who may benefit the most from participation in a physical activity program. Physical activity screeners are designed to capture the intended intervention population and are usually brief and easily administered by telephone or through the Internet (Snyder et al., 2004). Studies typically use one question to determine whether an individual is meeting physical activity recommendations or not (e.g. “Do you do physical activity for at least 30 minutes on 3 or more days per week?”) or use a cutoff point (e.g. <150 minutes per week; Keller, Fleury, Perez, Belyea, & Castro, 2011; Martyn-Nemeth, Vitale, & Cowger, 2010). However, due to their brevity, screeners may not accurately capture the intended population and information needed to truly assess physical activity status in women, whose physical activity often cycles or changes over time (I. M. Lee et al., 1997).
Once participants are deemed eligible to participate in a physical activity intervention, baseline or preintervention physical activity is measured, often through more detailed self-report recall questionnaires (Foley, Maddison, Olds, & Ridley, 2012), like the International Physical Activity Questionnaire (IPAQ) (Bauman et al., 2009; Sjostrom, Bull, & Craig, 2002). The IPAQ asks detailed questions about the specific types, frequency, and duration of physical activities participated in over a specified amount of time. Because of the difference in measurement tools or time lapse from screening to baseline assessment, there may be variation in reports on level of physical activity or activity status (Snyder et al., 2004). These inconsistencies in activity status between screening and baseline may lead researchers to include participants who should be excluded and exclude participants who should be included, greatly affecting observed changes in physical activity during an intervention. Therefore, assessing the consistency in self-reported physical activity from screening to baseline and controlling for inaccuracies may clarify why physical activity intervention effectiveness varies in ethnic minority women.
The purpose of this study was to identify inconsistencies between physical activity status reported at screening and baseline of a health promotion intervention and to explore how these inconsistencies influenced changes in physical activity over time between women who reported being (a) inactive at screening and baseline and (b) inactive at screening but active at baseline. We hypothesized that there would be a discrepancy in physical activity status from screening to baseline, and that women who reported being inactive at both screening and baseline would experience greater changes in physical activity over time than women who reported being active at baseline.
Method
Study Design and Participant Selection
Health Is Power (HIP) was a 6-month, randomized controlled trial to increase physical activity or improve dietary habits in ethnic minority women residing in Harris County, Houston, Texas (R. E. Lee, Medina, et al., 2011). HIP study procedures and materials were reviewed and approved by the University of Houston’s Committee for the Protection of Human Subjects, and participants provided written informed consent prior to completing any study activities.
African American and Hispanic women 25 to 60 years old who were insufficiently active, or doing less than 90 minutes of physical activity per week, were recruited to the study. Interested participants completed a telephone screener to determine eligibility, as described previously (R. E. Lee, Mama, et al., 2011). Participants completed an in-person health assessment at baseline Time 1 (T1) and postintervention Time 2 (T2). Figure 1 describes the flow of participants through the study. Only participants (n = 274) who successfully completed T1 and had complete data were included in the current study. There were no significant demographic differences between those with and without complete physical activity data at T1.
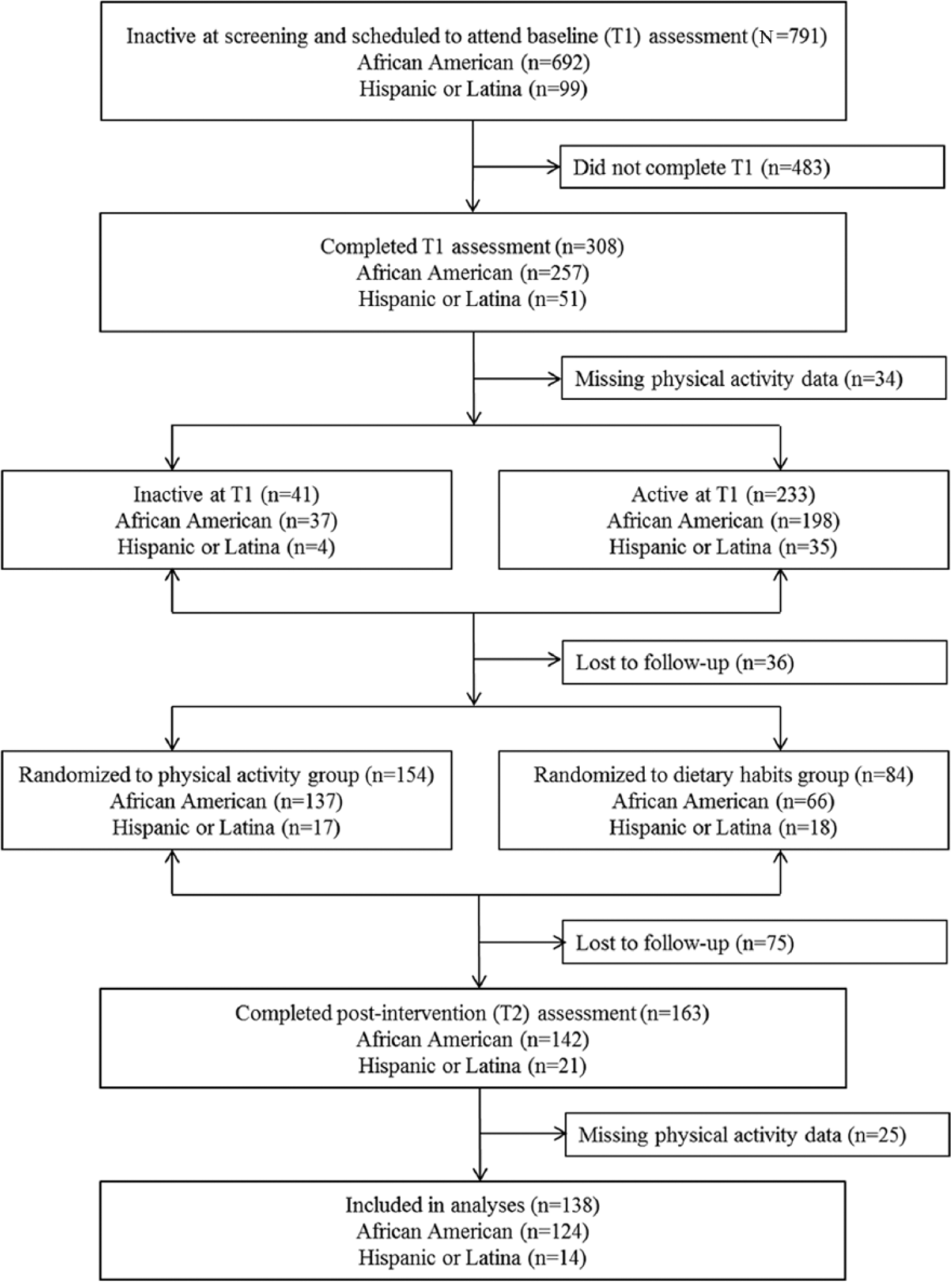
Flow of Participants Through the Study
Intervention and Data Collection
The ecological model of physical activity and group cohesion were used as guiding conceptual and theoretical frameworks to promote healthy behaviors in HIP by focusing on environmental and social constructs related to physical activity (Carron & Hausenblas, 1988; R. E. Lee, Medina, et al., 2011; Spence & Lee, 2003). Details on the development and implementation of the HIP study have been published previously (R. E. Lee, Mama, et al., 2011; R. E. Lee, Medina, et al., 2011; R. E. Lee et al., 2012) and are described briefly below. Eligible participants completed anthropometric measures and questionnaires during a scheduled health assessment that took place at the University of Houston and took 60 to 90 minutes. Women who completed a T1 assessment were invited to participate in a 6-month health promotion intervention and were randomized to a physical activity intervention or a dietary habits attention control intervention. Women met in their groups six times over the 6-month intervention period. Intervention sessions were led by a trained health educator and covered topics such as goal setting, self-efficacy, the benefits of healthy behaviors (physical activity, vegetable and fruit consumption), neighborhood influence on health behaviors, and relapse prevention (R. E. Lee, Medina, et al., 2011). After 6 months of intervention activities, women returned to the University of Houston to complete their T2 assessment.
Measures
Anthropometry
Height was measured twice using a portable stadiometer (Seca 225, Chino, CA), and body weight was measured twice using a body composition analyzer (Tanita TBF-310GS, Arlington Heights, IL) by trained personnel using established protocols (R. E. Lee, Mama, et al., 2011). Measured height and weight were used to compute body mass index (BMI = kg/m2). An average of the two measurements was used in analyses.
Demographics
Participants were asked to self-report their birth date to compute age at T1. Items assessing participant education and household income were drawn from the Maternal Infant Health Assessment survey, which has been used successfully with diverse samples (California Department of Public Health, 2010).
Physical Activity
At screening, participants were asked, “Are you now doing physical activity, like walking, jogging, or dancing, more than 3 days a week for more than 30 minutes each time,” and they responded yes or no. The IPAQ long-form was used to measure physical activity at T1 and T2 and asks about specific types of activities, including work-related, transportation-related, domestic and gardening, and leisure-time physical activities (Sjostrom et al., 2002). Participants report activities in terms of days per week and minutes and/or hours per day over the past 7 days. The IPAQ has been used to measure physical activity in diverse populations and is reliable (r = .8), with acceptable validity (r = .3) compared with accelerometry (Craig et al., 2003). For the purpose of this study, the IPAQ total physical activity score, a summation of activities across domains over the past 7 days, was treated as a continuous variable and dichotomized into inactive (<90 minutes/week) versus active (≥90 minutes/week) to be comparable to what participants reported during screening.
Data Analysis
Previous work by this team found that women in both the physical activity and dietary habits intervention groups increased their physical activity over time (R. E. Lee et al., 2012). Therefore, participants were treated as one group for analyses. Prior to analyses, normality was checked for all variables; IPAQ data were transformed using an exponential transformation to create a symmetric distribution. Pearson chi-square analyses and computed odds ratios were used to determine how the type of physical activity reported (work-related, transportation-related, domestic and gardening, and leisure-time) affected the likelihood of being categorized as active (doing ≥90 minutes of physical activity per week) at T1. Independent samples t tests were used to determine differences in physical activity by ethnicity, and Pearson correlations were used to explore associations between demographic and physical activity variables and to inform models. Paired samples t tests were used to assess changes in physical activity from T1 to T2 across groups. Assumptions of sphericity were tested, and repeated measures analysis of variance was used to test differences in changes in self-reported physical activity over time between groups (inactive vs. active at T1) adjusting for ethnicity. Analyses were post hoc and completed in SPSS 22.0 (IBM SPSS Statistics, Armonk, NY), and alpha level was set to .05.
Results
In general, participants were middle-aged (M = 44.3 years, SD = 9.9) and obese (M = 34.5 kg/m2, SD = 9.0). Most women were African American (85.8%). Participants were highly educated (95.2% attended some college or were college graduates), and 52.3% reported an annual household income greater than $82,600. African American women were more educated, χ2(4) = 28.2, p < .001, and reported a higher household income, χ2(5) = 16.2, p = .006, than Hispanic women. Ethnicity was significantly associated with domestic and gardening (t = −2.114, p = .035) and total physical activity (t = −1.966, p = .050). Hispanic women did more domestic and gardening (M = 1761.3 vs. 858.8 MET [metabolic equivalent of task] minutes/week) and total physical activity (M = 3580.2 vs. 2599.9 MET minutes/week) than African American women at T1. There were no other significant differences by ethnicity or activity status at baseline.
Most participants attended their baseline assessment within 40.1 days (SD = 36.2) of screening. The time lapse between screening and baseline was greater in women who were inactive at T1 (M = 52.7 vs. 38.0 days) but not statistically significant. Despite reporting they were inactive at screening, 85.0% of women self-reported being physically active at T1 (i.e., were doing ≥90 minutes of physical activity per week). Figure 2 presents physical activity at each time point by group. Women who reported being physically inactive at T1 did significantly less total physical activity (t = −14.776, p < .001) and less work-related (t = −6.391, p < .001), transportation-related (t = −5.150, p < .001), domestic and gardening (t = −9.537, p < .001), and leisure-time (t = −5.087, p < .001) activities than women who reported being active at T1. Chi-square analyses revealed that participants who reported doing any work-related, transportation-related, domestic or gardening, or leisure-time activities were more likely to report being physically active at T1. Computed odds ratios for each type of physical activity are shown in Table 1.
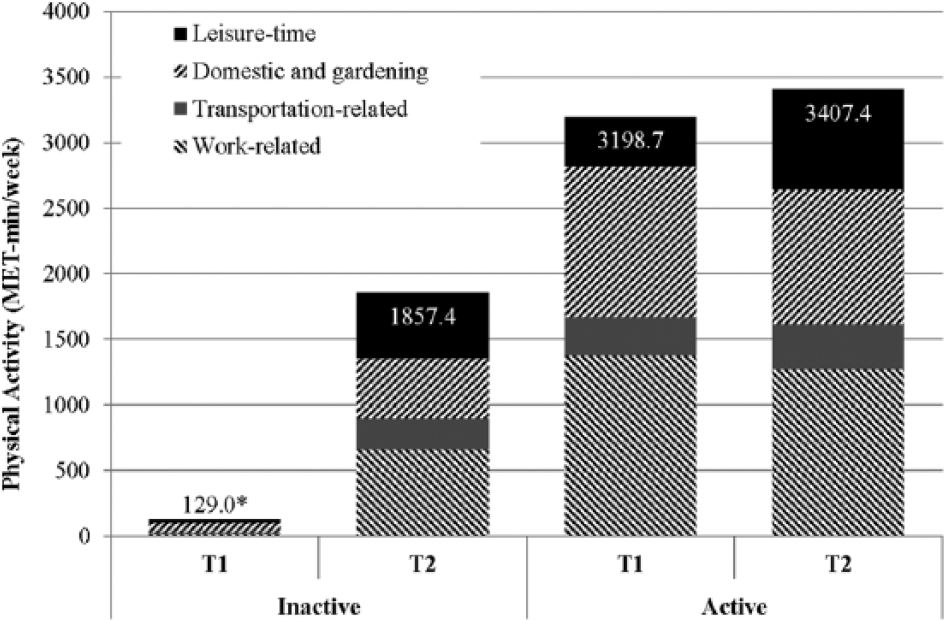
Physical Activity at Each Time Point by Group
Likelihood of Being Active at Baseline Based on Type of Physical Activity Reported
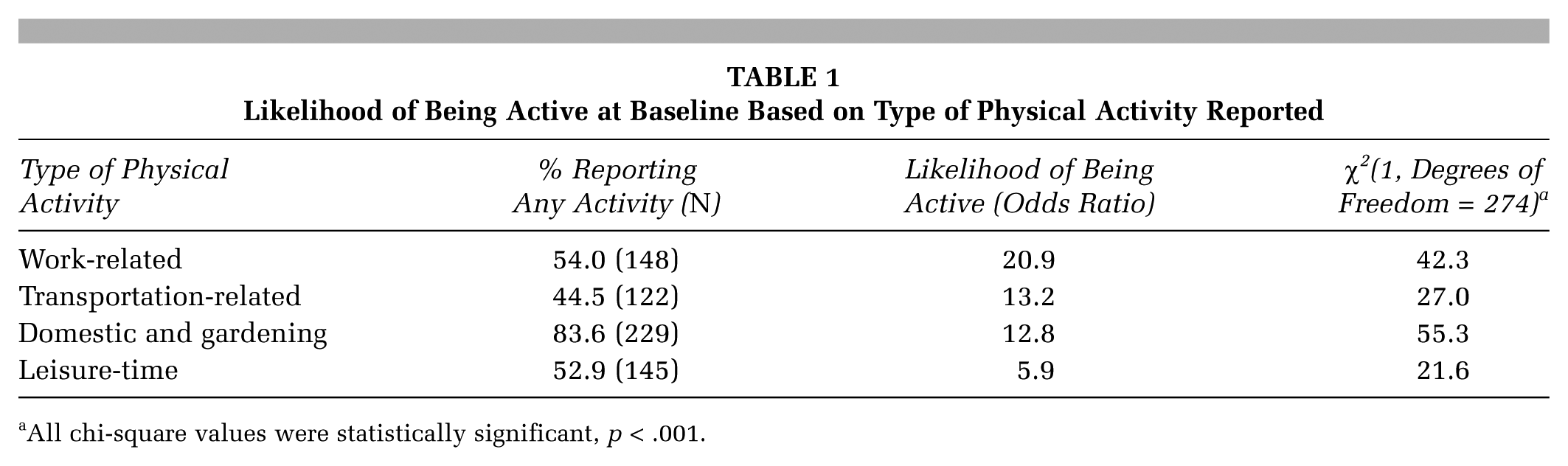
All chi-square values were statistically significant, p < .001.
Physical activity did not significantly change from T1 to T2 in the total sample (ps = .335-.948). However, women who were consistently inactive at screening and baseline reported significantly greater increases in domestic and gardening (Δ = 381.4 vs. -119.5 MET minutes/week, F(1, 135) = 16.918, p < .001), and total physical activity (Δ = 1728.4 vs. 208.7 MET minutes/week, F(1, 135) = 37.791, p < .001), from T1 to T2 than women who were active at baseline, after controlling for ethnicity. Inactive women also reported greater increases in work-related (Δ = 648.4 vs. −104.6 MET minutes/week), transportation-related (Δ = 227.2 vs. 51.0 MET minutes/week) and leisure-time (Δ = 471.4 vs. 381.7 MET minutes/week) physical activities, but these changes were not significantly different from active women (ps = .060-.370).
Discussion
Women who reported being physically inactive at screening were more likely to report being physically active at baseline if they reported any work-related, transportation-related, or domestic and gardening activities. This suggests that overweight/obese women may not perceive these activities as physical activity or exercise and may unknowingly classify themselves as insufficiently active. Previous studies have shown that misclassification of physical activity status is prevalent among overweight/obese individuals and may be due to the discrepancies in types of physical activities captured by questionnaires (Jones et al., 2014; I. M. Lee et al., 1997). However, whether the misclassification leads to agreement or disagreement between screening and more in-depth survey is still uncertain. Snyder et al. (2004) found that the discordant classification of activity status resulted in greater exclusion of inactive participants, whereas this study found it led to greater inclusion of active participants. These conflicting findings may be due to differences in ethnicity and weight status between studies. The current study sample was predominantly African American versus White and overweight or obese, and may be prone to overreporting physical activity due to social desirability bias (Adams et al., 2005; Jones et al., 2014).
Although the overreporting of physical activity is well documented (R. E. Lee, Mama, et al., 2011; Pietilainen et al., 2010), the influence of misclassifying individuals on physical activity adoption and intervention effectiveness is less understood. There were no significant increases in physical activity over time in the current study. However, intervention effectiveness was greatly improved after accounting for reporting differences in activity status between screening and baseline. Women who were consistently inactive at the start of the study benefited the most from the intervention and reported increases in all types of physical activity, whereas women who reported being physically inactive at screening but active at baseline decreased or reported relatively small increases in physical activity. Findings imply that brief screening instruments asking participants whether they are currently physically active or not may not accurately capture lifestyle behaviors due to misclassification errors, such as not including occupational activities in total time. In-depth surveys targeting specific types of physical activity may capture women’s true physical activity status and thus allow interventions to reach truly sedentary participants who have the most to gain from them. These results are in line with previous studies highlighting the limitations of using a single screening question, like those used in national and state-based surveillance systems, to gauge physical activity status (Macera et al., 2001). In-depth surveys targeting specific types of physical activity also helps researchers capitalize on the little physical activity women are already doing and tailor intervention content and messages for multiple settings, such as the worksite, home and active transportation settings, or spaces active commuters may access, like bicycle parking facilities or public transport stations and stops (Alliance for Biking & Walking, 2010; Mutrie et al., 2002; Wen, Orr, Bindon, & Rissel, 2005).
An alternative explanation of study findings is that women may increase their physical activity in preparation for participation in a physical activity intervention, resulting in higher self-reporting of physical activity at baseline and diminishing intervention effects. HIP used a rolling recruitment strategy to enroll women in study waves. About 30% of participants were screened within a few weeks, and 41% were screened within a month of their T1 assessment. The number of days between screening and baseline ranged from 0 to 234, depending on the intervention schedule and participants’ availability, and larger time lapses were often due to participants’ changing schedules. However, this time lapse did not lead to increased physical activity from screening to baseline in the current study. In an effort to reduce the risk of women engaging in physical activity prior to enrollment in the study, researchers should reduce this time lapse or implement a multistep screening process to screen participants prior to their assessment. Stewart et al. (2013) found a multistage screening process to be effective for identifying eligible participants for a behavioral intervention and showed that 78% of participants who passed the telephone screening phase were deemed ineligible or dropped out at the first visit. Similarly, our study found that 85% of participants would have been deemed ineligible if given a more in-depth questionnaire asking about specific types of physical activity.
Though the issue of screening inaccuracies is important and of interest to researchers and practitioners, this study is not without limitations. Future work should use objective measures of physical activity to capture activity status and reduce potential self-report, response, or recall bias, which may lead to over- and underreporting. However, objective measurement can be costly and time-consuming. Previous-day recalls may be a suitable alternative and have been found to be comparable to objective measures (Matthews et al., 2013). Due to its post hoc nature, the current study was not statistically powered to explore differences in physical activity adoption between active and inactive women and is subject to post hoc significance bias. Due to small sample sizes at postintervention, we were unable to explore effects over time by activity status and intervention group. However, previous work by this team found that women in both the physical activity and dietary habits intervention groups increased their physical activity over time (R. E. Lee et al., 2012), justifying their treatment as one group in analyses. Due to the largely homogenous sample, we were also unable to investigate other correlates of discordant physical activity reporting between screening and baseline. Additional research is needed to explore correlates (e.g., weight status, age, socioeconomic status) in a more heterogeneous sample. The screener used in the current study explicitly asked about walking, jogging, dancing, or similar leisure-time activities, and may only pick up recreational physical activity, compared to the IPAQ, which includes occupational, domestic, and gardening activities. Qualitative research may aid in understanding participants’ definition of physical activity, resulting in better screening measures and reducing inaccuracies. Last, the current study included a high–socioeconomic status population motivated to engage in a health promotion study, resulting in membership bias. Therefore, results from the current study should be interpreted with caution and may not represent low-income ethnic minority populations, who may be less active.
Conclusions
Physical activity interventions often rely on the enrollment of sedentary or physically inactive participants to establish effectiveness, but it is difficult to accurately identify participants who are sedentary. The current study found inconsistencies in physical activity reported at screening and baseline and showed that intervention effectiveness was greatly improved after accounting for inconsistencies. Controlling for inaccuracies may improve understanding of the effectiveness of physical activity interventions, which can be used to inform best practices and recommendations for future physical activity research. Clearer definitions of physical activity and more thorough assessments of type, intensity, and duration of physical activity can improve accuracy of self-reported physical activity and enhance screening. This can then be used to better target interventions and allocate resources to health promotion efforts benefiting those who have the most to gain.
Footnotes
Acknowledgements
The authors wish to thank the Understanding Neighborhood Determinants of Obesity research team and the Texas Obesity Research Center at the University of Houston for their help with data collection and processing throughout the study.
Funding for the Health Is Power study and this research was provided by the National Institutes of Health (R01 CA109403). Scherezade Mama was supported by a cancer prevention postdoctoral fellowship through The University of Texas MD Anderson Cancer Center, Cancer Prevention Research Training Program, funded by the National Cancer Institute (R25T CA057730, PI: Chang; P30 CA016672, PI: DePinho).