
Abstract
Purpose. To design and test the effectiveness of a text messaging intervention to promote condom use and STI/HIV testing among American Indian and Alaska Native youth. Method. A total of 408 study participants, 15 to 24 years old, were recruited, consented, surveyed, were sent intervention messages, and were incentivized via text message over a 9-month period. Complete pre- and postsurvey data were collected from 192 participants using SMS short codes. A mixed-effects logistic regression model was used to analyze before–after change in responses assessing sexual health knowledge, attitude, self-efficacy, intention, and behavior. Results. Participants’ condom use attitude, condom use behavior, and STI/HIV testing intention improved after the intervention (p < .05). Frequent condom use increased from 30% to 42% and was retained by participants at least 3 months postintervention, and the intervention improved participants’ intention to get tested for STI/HIV after changing sexual partners, increasing from 46% to 58% postintervention. Conclusions. Given the widespread use of cell phones by youth, text-based interventions may offer a feasible and effective tool to promote condom use and STI/HIV testing.
Keywords
American Indian and Alaska Native (AI/AN) youth experience persistent disparities related to teen pregnancy and sexually transmitted infections (STIs; de Ravello, Jones, Tulloch, Taylor, & Doshi, 2013). Demographically, about 658,208 AI/ANs are 15 to 24 years old (U.S. Census Bureau, Population Division, 2017). Although pregnancy rates fell for teens and young adults in the United States overall between 2014 and 2015 (AI/AN teens 15-19 years old experienced a 6% decline), AI/AN teen birth rates remained almost 1½ times higher than White teen birth rates (Martin, Hamilton, Osterman, Driscoll, & Mathews, 2017). AI/AN teens also experienced the second highest rates of chlamydia and gonorrhea among all racial/ethnic groups (Centers for Disease Control and Prevention, 2016).
A variety of structural, environmental, and cultural factors contribute to these disparities. Inadequate funding for health services (U.S. Commission on Civil Rights, 2004) and insufficient STI/HIV screening are common at Indian Health Service, tribal, and urban Indian health clinics (Rushing & Stephens, 2012; Tingey et al., 2015). Mainstream sexual health curricula that have improved sexual health outcomes for teens and young adults in the general population (Guse et al., 2012) often do not align well with the cultural values and life contexts of AI/AN youth (Rushing & Stephens, 2012). Native communities celebrate new life regardless of the parent’s age—a perspective that often conflicts with conventional teen pregnancy messages (Rushing & Stephens, 2012). Sexual health messaging is thus highly nuanced in Indian Country, requiring thoughtful consideration.
As cell phone use has skyrocketed among teens and young adults, text messaging has emerged as a promising tool to promote adolescent health (Bryant, Sanders-Jackson, & Smallwood, 2006; Gold et al., 2010; Guse et al., 2012). Text messaging offers users privacy and discretion, particularly important for sensitive topics, like sexual health (Perry et al., 2012). Additionally, mobile phones and text messaging are portable, real-time, affordable, asynchronous, interactive, and above all, convenient. Short message service (SMS) messages also possess one-to-many capacity that can be disseminated across large geographic regions with ease, maintaining intervention fidelity.
Embracing this potential, text messaging has been successfully used to improve help-seeking behavior and health outcomes for a variety of topics, including weight management (Patrick et al., 2009) and smoking cessation (Smith & Harris, 2009), and has been used to disseminate sexual health tips and clinic referrals (Levine, McCright, Dobkin, Woodruff, & Klausner, 2008). Gold et al. (2010) concluded that SMS was a “feasible, popular, and effective method of sexual health promotion to young people with a relatively low withdrawal rate, positive feedback, and an observed improvement in sexual health knowledge and STI testing” (p. 247).
In 2010, Kew demonstrated that text messaging was a viable instrument for data collection, achieving a 100% response rate in his study. With the small screen, but faster operating system, the simplicity of SMS aligns with the consolidated usability model, defining usability “as a combination of effectiveness, efficiency, . . . learnability, and security” (Nayebi, Desharnais, & Abran, 2012).
A meta-analysis by Head, Noar, Iannarino, and Harrington (2013) found that SMS message tailoring and personalization were significantly associated with greater intervention efficacy. Minority groups were more likely to use text messaging, and youth sent more text messages per day (averaging 50 messages) compared to adults (Head et al., 2013). A systematic review of mobile text messaging interventions by Hall, Cole-Lewis, and Bernhardt, (2015) concluded that strong evidence supported their use in public health practice. Their team called for additional research to determine the optimal use and limitations of text messaging, including the number, frequency, and duration of text messages required to achieve behavioral outcomes—all features that are likely to vary from audience to audience. Most recently, interactive text messages have been used to reduce binge drinking (Suffoletto et al., 2015), improve treatment outcomes in patients with depression (Agyapong et al., 2017), and increase medication adherence (Badawy & Kuhns, 2017).
In 2009, 78% of AI/AN youth in the Pacific Northwest reported using cell phones on a daily or weekly basis (Rushing & Stephens, 2011). Given the successes demonstrated by previous text message studies, we believed that an SMS intervention tailored to the unique needs and culture of AI/AN youth could improve sexual health outcomes for Native youth living across the United States.
The aims of our study were twofold: (1) to use formative research methods to design a culturally relevant text messaging intervention for AI/AN youth and (2) to test whether the intervention could improve sexual health knowledge, attitude, self-efficacy, and intention among AI/AN teens and young adults, with the overall goal of improving sexual health behaviors related to condom use and STI/HIV testing. This study offers insights for designing, implementing, and evaluating a culturally sensitive text messaging intervention for AI/AN youth, a high-risk, underserved population. This novel approach offers promise to address other health promotion and education topics important to teens and young adults.
Method
Population and Setting
The study—Texting 4 Sexual Health—was conducted in partnership between the Northwest Portland Area Indian Health Board (NPAIHB) and Oregon Health & Science University (OHSU), using We R Native, a multimedia health resource for Native teens and young adults. Established in 2012 by the NPAIHB, the service includes a website (http://www.weRnative.org), a text messaging service (Text NATIVE to 97779), a YouTube channel, and social media pages. We R Native offers over 350 health and wellness webpages covering a variety of topics important to Native youth, including sexual health (NPAIHB, 2016). Through these platforms, We R Native had an existing relationship with Native teens and a well-established SMS service that could be used to recruit study participants and carry out intervention activities.
Intervention Development
The intervention included 24 text messages designed to improve condom use and STI/HIV testing: both behaviors associated with STI transmission among teens and young adults. The team blended insights from the health belief model, social cognitive theory, and the theory of planned behavior to concentrate on factors associated with behavior change (Glanz, Rimer, & Viswanath, 2008). For each behavior change construct (knowledge, attitude, intention, and self-efficacy), we drafted one to three corresponding intervention text messages. Given the heterogeneity of youth expected to participate in the study, the messages were written to resonate with young adults who were male or female, sexually active or not yet sexually active, and of differing sexual orientations (heterosexual, lesbian, gay, bisexual, transsexual, Two-Spirit).
To ensure their relevance and acceptability to the intended audience, formative research activities were carried out with 60 AI/AN youth living throughout the United States. We received permission from four health promotion conferences attended by AI/AN youth to solicit their feedback; all participants received a printed consent form approved by the OHSU and Portland Area Indian Health Service Institutional Review Board. The anonymous, paper-based survey took approximately 20 minutes to complete and included mock images of 43 text messages. Participants were asked to rate each message as “cool, alright, or real bad” and provide edits to any messages that were merely “alright.” They were asked if they would respond to the survey questions or click on proposed links. Participants were also asked about the acceptable frequency of SMS health messages.
Fourteen (n = 14) AI/AN young adults who attend a weekly Two-Spirit youth group reviewed a second draft of the text message sequence and survey questions, proving similar input. Finally, during a 2-hour advisory meeting with seven (n = 7) AI/AN college students, participants used their own phones to test the functionality of the SMS delivery software and our intended data collection plan. Messages were sent to each attendee to determine how long it would take to get messages from different cell phone carriers and how long it would take to receive their responses. Participants were asked about their preferred survey sequencing and timing between questions. All participants received compensation for their time and contributions.
After each round of review, qualitative data were systematically transcribed and analyzed. Through this iterative process, the intervention methods and messages (Table 1) were honed to reflect the sexual health needs of AI/AN youth of varying genders, ages, and sexual orientations, while maintaining cultural relevance and sensitivity. Privacy and confidentiality were distinctly noted by formative research participants as important factors to explain during recruitment to ensure participation.
Condom Use and STI/HIV Testing Behavioral Constructs, Text Messages, and Survey Questions
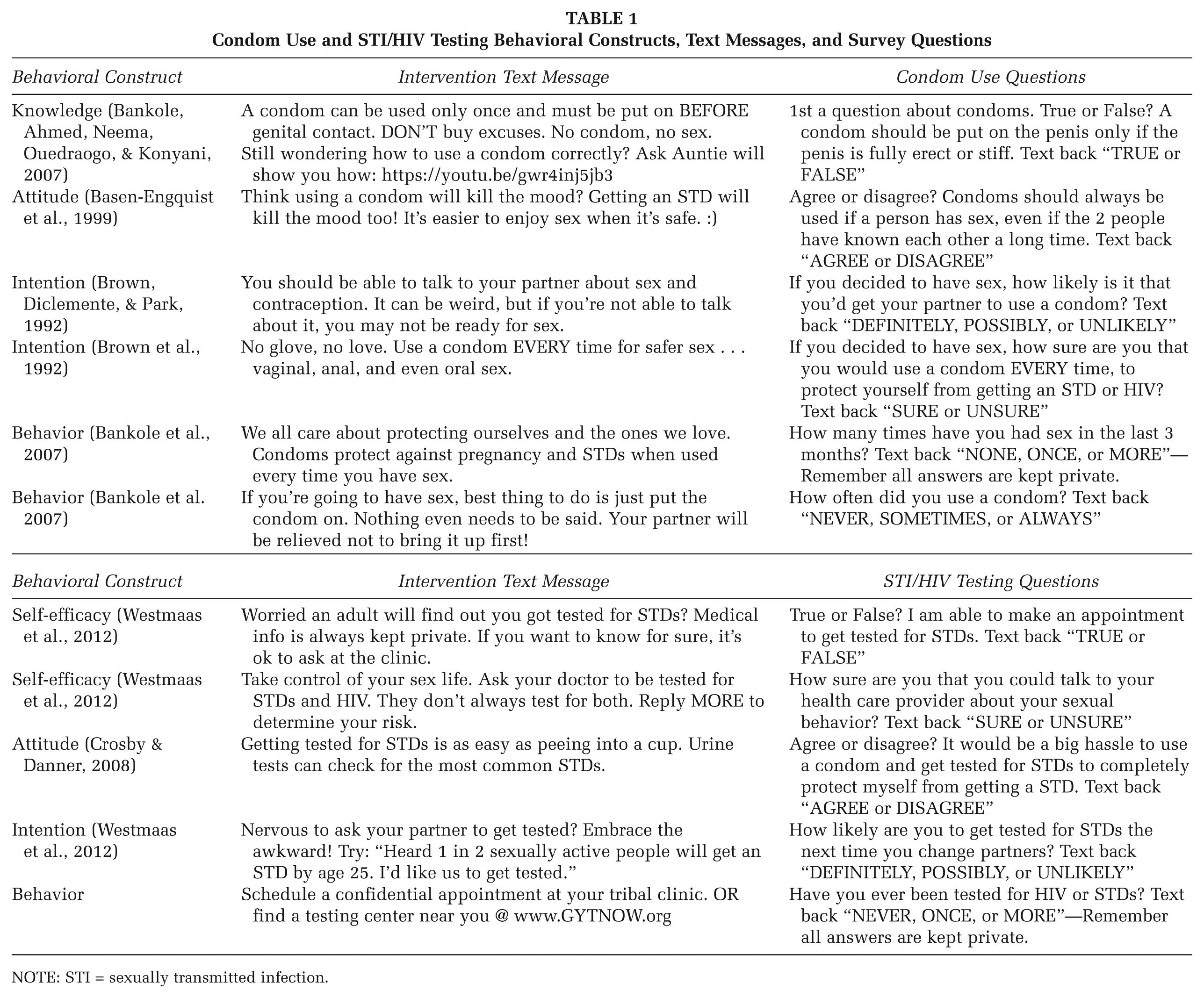
NOTE: STI = sexually transmitted infection.
To evaluate the efficacy of the text messages, we selected six questions to assess condom use and six questions to assess STI/HIV testing that were derived from validated survey tools (Table 1). The questions were reformatted for SMS delivery (e.g., condensed to 160 characters) with unique response options, a step that triggered the next survey question.
Study Protocol
The study received a waiver for parental consent, allowing teens 15 to 18 years of age to participate without parental permission. Teens and young adults who had already subscribed to the We R Native weekly text messaging service were invited and consented via text message:
Message 1: We R Native is doing a research study: Texting 4 Sexual Health. The goal is to reduce STD/HIV rates among Native teens and young adults.
Message 2: You must be AI/AN & 15-24 yrs. You will get 2 sexual health msgs per week for 3 months. All texts are private. Earn $40 for answering 40 Qs over 6 months.
Message 3: We won’t collect your name, just cell # to analyze results. To protect your privacy, you can delete our messages from your phone.
Message 4: Reply AGREE if you want to join. Reply LEAVE to quit. Go to http://mozeo.me/WoGe to learn more about the study and your rights.
All consented participants (1) self-identified as AI/AN, (2) were 15- to 24-year-olds, and (3) had access to a cell phone with texting capability. Respondents who were outside the specified age-group were excluded from the study. If a participant reported being 25 at the time of the demographic survey (conducted midway through the intervention), we included them, since they could have been 24 at the start of the study. All communications related to recruitment, consent, intervention delivery, pre–post testing, incentives, and data collection were conducted through an online SMS delivery platform: Mozeo.
We employed a before–after study design to assess the impact of the text messages on condom use and STI/HIV testing behavior. Over a 4-week period, 12 questions (6 questions per survey, Table 1) were sent through two text message sequences to establish baseline responses, followed by intervention messages twice a week for 12 weeks. After a 1-week quiet period, the survey questions were sent out again, to measure the immediate impact of the text message intervention. Another 8-week quiet period followed, with the survey questions issued for a third and final time. A demographic survey was conducted midway through the 12-week intervention, which collected information on gender, age, and sexual orientation. (A text messaging time line, Supplemental Table A, is available with the online version of the article.) After each survey, $5 Amazon gift codes were sent to respondents in appreciation for their time and participation; incentives increased to $10 for the final round of surveys.
All told, the study involved a total of 97 SMS messages delivered over 9 months, including 32 intervention messages and 12 survey questions sent out three times (36 messages in total). The remaining messages were related to participant recruitment (3), consent and privacy (4), survey reminders (12), demographic questions (4), and incentives (6).
Data Collection
Data collection was carried out using keywords. A keyword response is a feature that allows certain words to trigger a specific response, if needed. Keywords are purchased from the SMS vendor and can be used only by the purchaser. As a result, not all the keywords desired for the study were available, as some had already been purchased. When that occurred we had to modify survey answers to include available keywords. For example, the keywords Yes/No were not available for the study so True/False were used instead.
An automated response is a feature that preprograms a response to an incoming text message. This feature was used in tandem with the keyword response to trigger the next survey question. Because keywords triggered the next survey question, response options could not be repeated in the sequence, requiring unique answer choices for every question in the sequence.
During the study, responses were manually checked for errors, and active steps were taken to improve survey response rates. One such strategy was to identify all nonresponders and those who did not receive a follow-up message due to keyword misspellings, and send them the last unanswered question as a prompt the following week. This allowed those who meant to respond but got distracted, or who submitted a misspelled keyword, to continue with the survey. Through our particular SMS vendor, this process proved to be time-consuming, requiring a new list of numbers to be compiled for each drop-off point and each SMS push.
Measures and Variables
Outcome variables were determined by responses to survey questions (Table 1). Most questions had binary responses, and questions with three response categories were dichotomized. For example, in analyzing responses of definitely, possibly, and unlikely, “possibly” and “unlikely” were combined, and responses were coded as yes (definitely) or no (possibly + unlikely) for analysis. The primary independent variable was the texting intervention, represented by the Pretest, Posttest 1 and Posttest 2. Information on age, gender, and sexual orientation represented the demographic variables for the study.
Statistical Analysis
Participant demographics and responses at baseline and at the two postintervention time points were summarized using descriptive statistics. Given that outcomes were analyzed as binary variables, odds ratios were used to quantify the association between individual variables (demographic, behavioral construct, and intervention variables) and each outcome variable using a mixed-effects model. In all models, the identification variable for each participant entered the model as a random effect to take the correlation among repeated measures with the same participant into account. Variables with a p ≤ .25 and the intervention variable were then analyzed in a multivariable model using a backward elimination manner; those variables that were not significant in the multivariable model were removed with the least significant one removed first. Some of the survey questions also served as independent variables in the analysis, in line with health behavior theories. For example, constructs such as attitude and self-efficacy are predictors for intention. In assessing intention, the two constructs were included in the initial full model analysis if they were found to be significant in univariate analysis. Although the intervention variable was retained in the model regardless of the significance level, other variables that were not significant were dropped.
In the logistic regression analysis for each outcome, only those who completed the demographic surveys were included. Once a preliminary parsimonious final model was built for each outcome, including the intervention variable and other significant variables, a common final model was built for condom use and STI/HIV testing behavior, separately, by including variables that were significant for any of the outcomes in each category to facilitate interpretation. Such a model quantified the difference in outcome variables, while adjusting for important participant characteristics. We also explored whether testing behavior was affected by the intervention using chi-square tests. All analyses were conducted using Stata/IC11.0 (Stata Corp LP, College Station, TX).
Results
The consort diagram (Figure 1) depicts participation throughout the study. Among those enrolled in the We R Native text messaging service (1,300 at the time of the study), 408 youth consented to participate. Based on cell phone area codes, participants were distributed across the United States, but more concentrated along the west coast. Among the 408 enrolled participants, 210 completed the demographic survey.
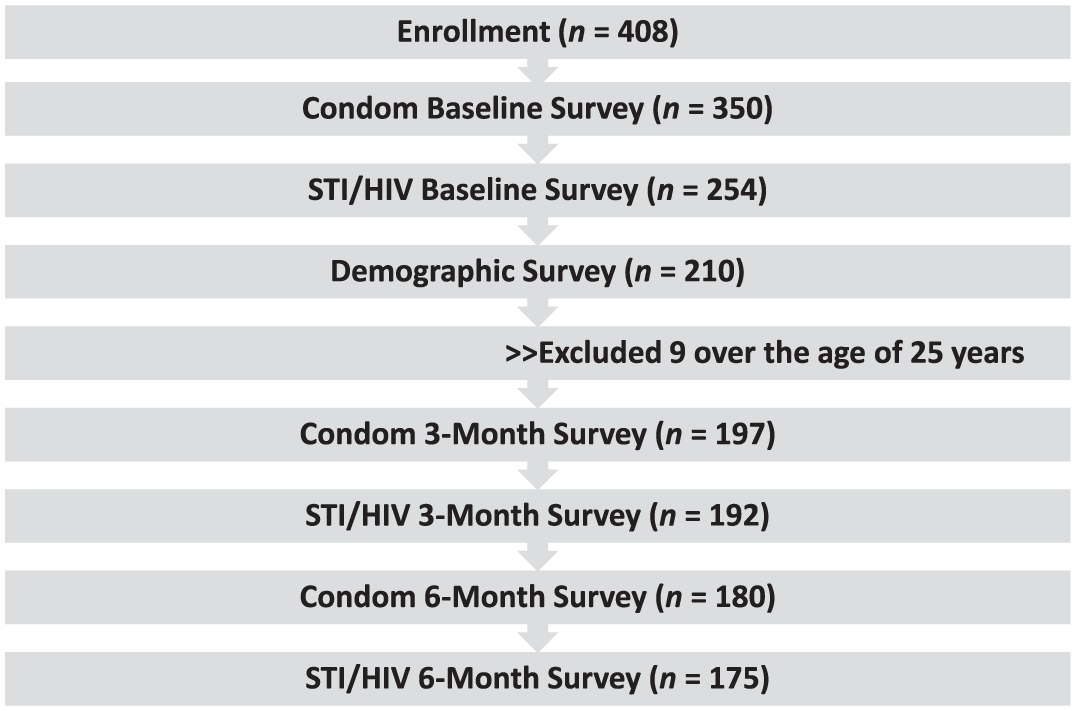
Consort Diagram
Participants were young women (77%) and young men (23%), between the ages of 15 and 18 years (41%) and 19 and 24 years (59%). Nearly 82% identified as straight, and 18% identified as lesbian, gay, bisexual, transgender, or Two-Spirit. (A demographic summary, Supplemental Table B, is available with the online version of the article.) Responders and nonresponders to the six sets of postsurvey questions were similar with respect to gender, age, and sexual orientation. To test for possible retention biases, we compared baseline responses to the sexual health questions between responders (those who completed the first postsurvey) to nonresponders (those who did not complete the first postsurvey). Using Pearson’s chi-square test, we found no significant differences in responses between responders and nonresponders.
Condom Use
The intervention text messages did not have a statistically significant influence on condom use knowledge or intention. In both cases, sexual experience was significantly associated with knowing how to use a condom, and with the intention to use a condom, either for oneself or for their partner (Table 2).
Multivariate Models for Condom Use
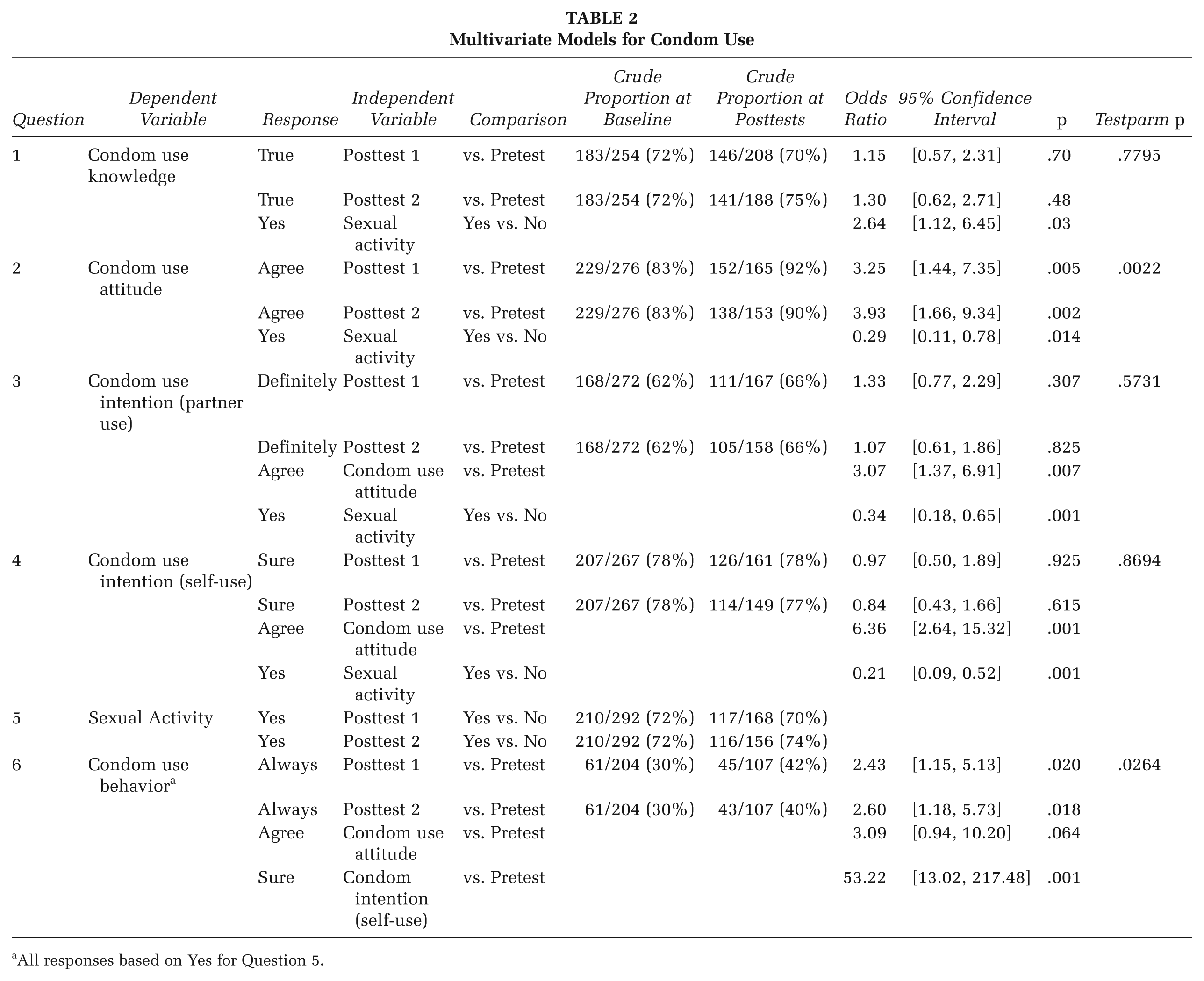
All responses based on Yes for Question 5.
To assess condom use attitudes, we asked, “Agree or disagree? Condoms should always be used if a person has sex, even if the two people have known each other a long time.” After adjusting for all other variables in the model, the odds of agreeing that condoms should always be used was more than 3 times the odds (odds ratio [OR] = 3.25, p = .005, 95% confidence interval [CI; 1.44, 7.35]) 1 week after and almost 4 times the odds (OR = 3.93, p = .002, 95% CI [1.66, 9.34]) 3 months after the SMS intervention, compared to before the intervention. The difference in the responses between the two postsurveys was not statistically significant, indicating that the effects were maintained 3 months postintervention (Table 2).
After adjusting for all other variables in the model, the odds of agreeing “condoms should always be used” in those who were sexually active was 0.29 times the odds (OR = 0.29, p = .014, 95% CI [0.11, 0.78]) of those who were not sexually active (Table 2).
The question “How many times have you had sex in the past 3 months? Text back “NONE, ONCE, or MORE’” was used to establish context for Question 6, which asked how often condoms were used. Although sexual activity was found to be a significant independent variable in univariate analysis for some of the behavioral constructs explored, it was not expected to be affected by the intervention (Table 2).
To assess condom use behavior, we asked, “How often did you use a condom? Text back ‘NEVER, SOMETIMES, or ALWAYS.’” The responses were analyzed as always and never (never and sometimes were combined). After adjusting for all other variables in the model, the odds of having used a condom was 2.4 times the odds (OR = 2.43, p = .020, 95% CI [1.15, 5.13]) 1 week after the intervention and 2.6 times the odds (OR = 2.60, p = .018, 95% CI [1.18, 5.73]) 3 months postintervention, compared to rates reported at baseline (Table 2).
STI/HIV Testing
The intervention text messages did not have a statistically significant influence on STI/HIV testing self-efficacy or attitude. Most respondents were already very confident in their ability to make an appointment to get tested and speak to a health care provider about their sexual behavior. Their responses also reflected a positive attitude toward STI/HIV testing behavior and condom use, and the intervention did not change this (Table 3).
Multivariate Models for STI/HIV Testing
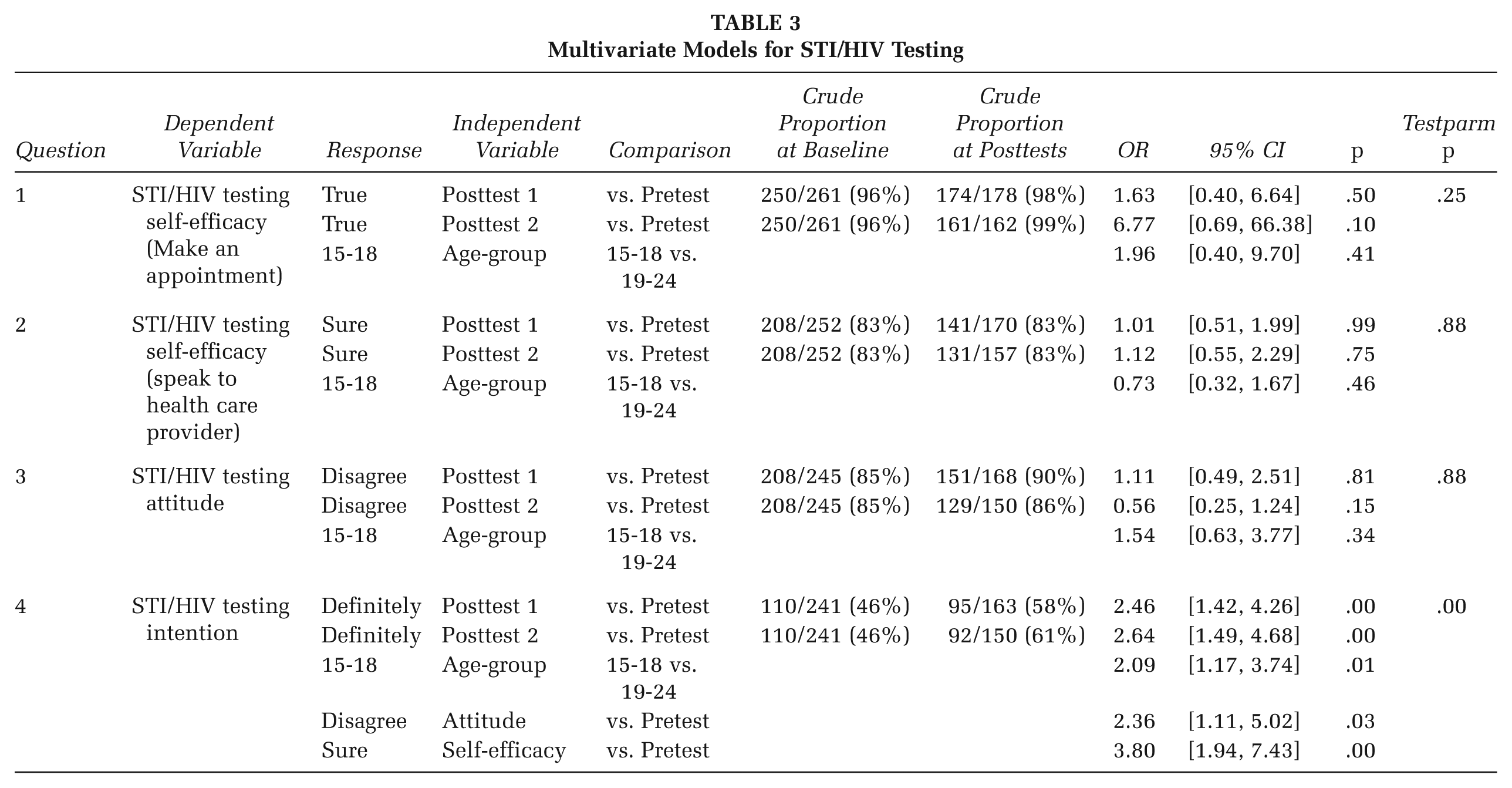
However, self-efficacy and attitude were significantly associated with intention to test. The odds of intending to get tested for STI/HIV in those having a strong sense of STI/HIV testing self-efficacy (captured as a “sure” response) was 3.8 times the odds (OR = 3.80, p < .001, 95% CI [1.94, 7.43]) compared to those reporting low self-efficacy. Also, the odds of intending to get tested in those with a positive attitude toward STI/HIV testing (as measured by a “disagree” response) was 2.3 times the odds (OR = 2.36, p = .026, 95% CI [1.11, 5.02]) of those who reported negative attitudes toward testing. Younger participants (15-18 years) reported twice the odds of intending to get tested for STI/HIV (OR = 2.09, p = .013, 95% CI [1.17, 3.74]) compared to those in the older age-group (19-24 years; Table 3).
To assess STI/HIV testing intention, we asked, “How likely are you to get tested for STDs the next time you change partners? Text back ‘DEFINITELY, POSSIBLY, or UNLIKELY’.” The responses were analyzed dichotomously by grouping “possibly and unlikely” into one group (unlikely). After adjusting for all other variables in the model, the odds for intention to get tested was 2.4 times the odds (OR = 2.46, p = .001, 95% CI [1.42, 4.26]) 1-week after the intervention, and 2.6 times the odds (OR = 2.6, p = .001, 95% CI [1.49, 4.68]) three months post-intervention, compared to rates reported prior to the intervention. The difference in responses between the two post-surveys was not statistically significant, suggesting that intervention effects were maintained three months later (Table 3).
To establish context for STI/HIV testing behavior, we asked “Have you ever been tested for STI or HIV? Text back ‘NEVER, ONCE, or MORE’.” If the response was once or more, the next question asked how long ago the respondent had been tested. 152/236 (64%) reported that they had gotten tested at pretest and the posttest responses reflected similar results (69%, 111/161, at Posttest 1; 62%, 90/146, at Posttest 2). Ninety subjects responded to these questions at both pretest and Posttest 1. When stratified the time of testing as >6 months or ≤6 months, among those who responded with having tested ≤6 months ago at pretest, 46% (17/37) reported having tested within 6 months at posttest. This was significantly higher compared to subjects who responded with having tested >6 months ago at pretest, where only 21% (11/53) reported having tested within 6 months at posttest (p = .011).
Discussion
In this study we used an iterative, formative research process to guide the design of a culturally relevant SMS intervention for AI/AN youth. While prior studies have demonstrated the efficacy of text messaging to promote sexual health knowledge and awareness among teens and young adults (de Tolly, Skinner, Nembaware, & Benjamin, 2012; Lim et al., 2011; Lim, Hocking, Hellard, & Aitken, 2008; Sheoran, Braun, Gaarde, & Levine, 2014), the Texting 4 Sexual Health intervention also elicited improvements in condom use and STI/HIV testing intention. The messages had a positive impact on youth’s attitudes toward condoms, with 9% more youth agreeing postintervention that “condoms should always be used if a person has sex, even if the 2 people have known each other a long time.” Frequent condom use increased from 30% to 42% and was retained by participants at least 3 months postintervention, suggesting that SMS messages can prompt immediate and short-term improvements in protective behavior. Sexual experience and younger age (15-18 years) were both associated with condom use, suggesting that early intervention may improve behavioral impact.
The intervention improved participants’ intention to get tested for STI/HIV after changing sexual partners, increasing from 46% to 58% postintervention. A positive attitude toward STI/HIV testing, self-efficacy to speak with a provider, and younger age (15-18 years) were all associated with STI/HIV testing intention. With respect to actual testing, our findings suggest that those who had been tested more recently (≤6 months) at pretest were more likely to continue testing than those who had been tested more than 6 months at pretest (46% vs. 21%, p = .01). However, some of these STI/HIV tests in the pretest may have overlapped the timing of the response of the first posttest, skewing results toward greater retesting. Further studies with a larger sample size are needed to better determine the effect of the text messaging intervention with relation to actual STI/HIV testing.
The measure that showed the most resistance to change was youth’s intention to get their partner to use condoms, which remained close to the preintervention rate of 64%. Additional messages supporting partner communication and condom negotiation skills may be needed to improve intention and self-efficacy surrounding these important, yet challenging skills.
To meet young people where they are and respond to their preferred communication channels, additional health interventions should be designed for delivery via text message. Nearly one third of We R Native’s SMS users agreed to participate in the study, suggesting both interest and acceptability for this geographically disbursed audience. Translating this research to practice, the Text 4 Sex Ed service is now available for any youth to enroll and receive the SMS sequence (text “SEX” to 97779); over 250 participants have enrolled in the service since its launch in February 2017.
Limitations
This study had several limitations. Participants were not randomly selected and therefore cannot be considered representative of all AI and AN youth across the United States. Among the 408 participants who consented to participate, 29 withdrew during the study. Only 210 respondents provided demographic data, and not all of them fully participated in all three pre–post surveys. There were no significant differences between those who completed surveys and those who did not, in relation to gender, age, or sexual orientation, which suggests that dropouts were random, reducing analytic power. Future studies would benefit from a larger sample size. It is also possible that those who dropped out of the study may have been less interested in sexual health and thus could have biased the results. However, we did use a mixed-effects model using all available data, which handles missing values better than other methods.
Online-based research can be subject to fraud, whereby study respondents participate multiple times or falsely report their eligibility (Teitcher et al., 2015). In our study, responses were tied to unique, U.S. cell phone numbers, eliminating the possibility of enrolling multiple times. If a respondent submitted more than one response, we recorded only the first response. To validate eligibility, a demographic survey was conducted midway through the intervention, which identified several ineligible participants.
Finally, a pre–post study design was used to evaluate the intervention, and while the changes in outcome indicators were significant among participants, we cannot attribute changes to the intervention alone because a control group was not employed.
The study was strengthened, however, by the long-standing partnership between the NPAIHB and OHSU, and our use of We R Native—a multimedia health resource that is known and trusted by AI/AN youth. While these topics are sensitive in Indian Country, the formative research activities used by the team to design the intervention improved the content and credibility of the text messages and helped sustain participation.
Conclusion
This study was the first of its kind to explore the potential of text messaging to promote healthy behavior among AI/AN teens and young adults. The Texting 4 Sexual Health study indicates that two SMS messages per week over 12 weeks may improve condom use and STD/HIV testing intention among at-risk youth. These findings suggest that SMS interventions could be a feasible, acceptable way to deliver culturally relevant health messages to unique, highly dispersed populations. With the widespread use of cell phones by AI/AN youth, text messaging remains a promising tool to promote healthy norms and behaviors across a wide variety of topics.
Supplemental Material
HPP761872_Supplemental_Table_A – Supplemental material for Texting 4 Sexual Health: Improving Attitudes, Intention, and Behavior Among American Indian and Alaska Native Youth
Supplemental material, HPP761872_Supplemental_Table_A for Texting 4 Sexual Health: Improving Attitudes, Intention, and Behavior Among American Indian and Alaska Native Youth by Patricia Yao, Rongwei Fu, Stephanie Craig Rushing, David Stephens, Joan S. Ash and Karen B. Eden in Health Promotion Practice
Supplemental Material
HPP761872_Supplemental_Table_B – Supplemental material for Texting 4 Sexual Health: Improving Attitudes, Intention, and Behavior Among American Indian and Alaska Native Youth
Supplemental material, HPP761872_Supplemental_Table_B for Texting 4 Sexual Health: Improving Attitudes, Intention, and Behavior Among American Indian and Alaska Native Youth by Patricia Yao, Rongwei Fu, Stephanie Craig Rushing, David Stephens, Joan S. Ash and Karen B. Eden in Health Promotion Practice
Footnotes
Authors’ Note:
Research was supported by the National Library of Medicine of the National Institutes of Health under Award No. T15LM007088, the Indian Health Service HIV Program, and the Tartar Trust Fellowship Award.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.