
Abstract
Disparities in chronic disease and life expectancy remain a significant public health problem and are largely attributable to social determinants of health. Community health workers (CHWs) promote health equity through individual- and community-level activities, and leadership and advocacy skills training make CHWs more likely to catalyze structural change. CHWs are increasingly being integrated into clinical practices to support care management, creating a need for new grassroots community-level advocates. We adapted for community residents an existing CHW training curriculum focused on social determinants of health and effecting community change. We offered 36 hours of training at community-based locations in New Orleans, Louisiana. We assessed baseline civic and community participation and pre- and postknowledge for each lesson. Among 43 enrollees, 42 completed the program. The majority were Black (92.7%), female (92.7%), and retired or unemployed (77.5%), with a median age of 61.5 years. In the past year, 85% of participants had volunteered, 57.1% had been involved with a community organization, and 32.4% had contacted the city council. Participants demonstrated statistically significant increases in knowledge in 5 of 6 lessons. Our success in increasing knowledge of advocacy among a civically engaged group suggests that trainees may become community leaders in addressing social determinants of health.
Introduction
Racial and ethnic health disparities in rates of chronic disease and overall life expectancy remain a significant public health problem (Centers for Disease Control and Prevention, 2013). For example, obesity affects roughly 47% of African Americans, as compared to 38% of Whites (Hales, Carroll, Fryar, & Ogden, 2017). In 2015, there was a 3½-year difference in life expectancy between African Americans (75.5 years) and Whites (79.0 years; National Center for Health Statistics, 2017). It is well-established that poverty, unequal access to education, housing quality, the community environment, and other social and economic factors underlie health inequity (Braveman & Gottlieb, 2014), and they require attention to achieve the national priority of reducing disparities (Agency for Healthcare Research and Quality, 2016).
Although many interventions aim to address health disparities by changing individual behavior—essentially teaching individuals to make healthy choices in spite of unhealthy environments—upstream solutions that address economic and social inequity are both more effective and sustainable (Braveman & Gottlieb, 2014). There is a particular need to change structures and policies related social determinants of health that institutionalize differential access to resources (Jones, Jones, Perry, Barclay, & Jones, 2009) related to health such as quality education, transportation, and community environments that promote physical activity.
As trusted members of underserved communities who promote health equity through a variety of individual- and community-focused activities (American Public Health Association, 2009), community health workers (CHWs) have become widely recognized as a resource for promoting health equity (U.S. Department of Health and Human Services, 2011). They have been successful in addressing structural, or upstream conditions in underresourced neighborhoods by collaborating with coalitions to effect changes in policy related to air pollution (Minkler, Garcia, Williams, LoPresti, & Lilly, 2010) and installing walking trails (Cohen, Meister, & de Zapien, 2004) to promote physical activity and prevent chronic disease. There are existing models to train CHWs in leadership and advocacy skills (Reinschmidt et al., 2015; Wennerstrom, Johnson, Gibson, Batta, & Springgate, 2014). There is evidence that CHWs who have received this type of education are more likely to engage in advocacy activities (Sabo et al., 2013) and that such actions catalyze structural change (Sabo et al., 2017).
Although CHWs have historically been employed by nonprofit organizations, health and social services agencies, universities, and other entities, they are increasingly being integrated into hospitals and health systems (Malcarney, Pittman, Quigley, Horton, & Seiler, 2017) because they improve health outcomes and reduce health care costs (Brown et al., 2012; Wilkinson et al., 2016). However, there is evidence that CHWs employed in hospitals and clinics that are not community-based are less likely to engage in political advocacy than those employed in community settings (Sabo et al., 2013). This move toward basing CHWs in clinical practice may leave a vacuum of grassroots community-level advocacy that could be filled by other community residents who are similar to CHWs, if appropriately trained. Lay members of communities have been trained as volunteers to deliver a host of health promotion interventions related to cancer (Hinton, Downey, Lisovicz, Mayfield-Johnson, & White-Johnson, 2005), cardiovascular health (Karwalajtys et al., 2009), and chronic disease management (Dye et al., 2018). However, little is known about strategies for preparing lay community residents to become involved in advancing structural and policy change.
In this article, we describe the implementation and initial evaluation of a community health leadership program that was adapted from an existing CHW training curriculum and designed to bolster the capacity of lay community residents in New Orleans, Louisiana, to make improvements in the structural and social conditions that affect health. Our intervention was based on Rothman’s (2004) locality development model of community organizing, which aims to raise consciousness about the root causes of problems and implement action strategies to address them. We used an ecological framework (McLeroy, Bibeau, Steckler, & Glanz, 1988) to introduce the concept of social determinants of health and various causes of health inequity. We hypothesized that training individuals on the underlying causes of health disparities, strategies for social action to address these root causes (e.g., coalition building, implementing community development projects, conducting health assessments, communicating community desires to policymakers, etc.), and leadership skills would be feasible, increase knowledge of community health improvement strategies, and ultimately, lead to an increase in trainees’ participation in civic and political activities to address health.
Method
Study Design and Setting
This quasiexperimental study was conducted in New Orleans, Louisiana, through a partnership between Tulane School of Medicine and the Tulane Prevention Research Center and its community advisory board (CAB). Roughly three fifths (61.2%) of the New Orleans population is African American, and there is a 25 year difference in life expectancy between residents who live in the poorest zip code (55 years) and the one with the lowest rate of poverty (80 years; Joint Center Political and Economic Studies, 2012). In some communities, as many as 72% of residents have less than a high school level of education. Louisiana has the second highest rate of incarceration in the United States (Wagner & Sawyer, 2018), with disproportionate representation of African Americans behind bars (Prison Policy Initiative, 2016).
Participant Recruitment
To gather local buy-in, we introduced the concept of the program to CAB members during a quarterly meeting. We requested input regarding perceived feasibility of the program and specific social determinants of health, if any, on which the program should focus, as well as program delivery methods. We also invited CAB members to serve as co-trainers if they were interested. Because the goal of this program was to expand local community residents’ understanding of and capacity to address structural issues that affect health, we sought a wide variety of participants who were interested in community improvement but new to working on health-related issues. Specifically, our requirements for participation included being at least 18 years of age, not having participated in previous health leadership training and not having a formal background in health care or public health. Based on CAB member input that some New Orleans residents are transient, we required at least 3 years of residence in the Greater New Orleans area to ensure that participants would have some familiarity with local culture and context. To increase the likelihood that participants could contribute to local public health capacity, we also required that participants not have any self-reported immediate intention to move to another city or state. We recruited participants through a partner program at a local community health center, the Tulane Prevention Research Center newsletter, e-mails to an existing CHW listserv, members of the CAB and organizations with which they were affiliated, and word of mouth.
Curriculum
The basis for the program was an existing 80-hour CHW training curriculum that was originally created as a local workforce development initiative (Wennerstrom et al., 2014). The original program was created in partnership with community organizations. Over the course of 2 years, CHWs, academic partners, and community stakeholders engaged in an iterative process to produce a CHW core competency–based curriculum that was reflective of local community strengths and culture and addressed unique community health issues. The program was shown to support engagement in community-level activities (Wennerstrom et al., 2014).
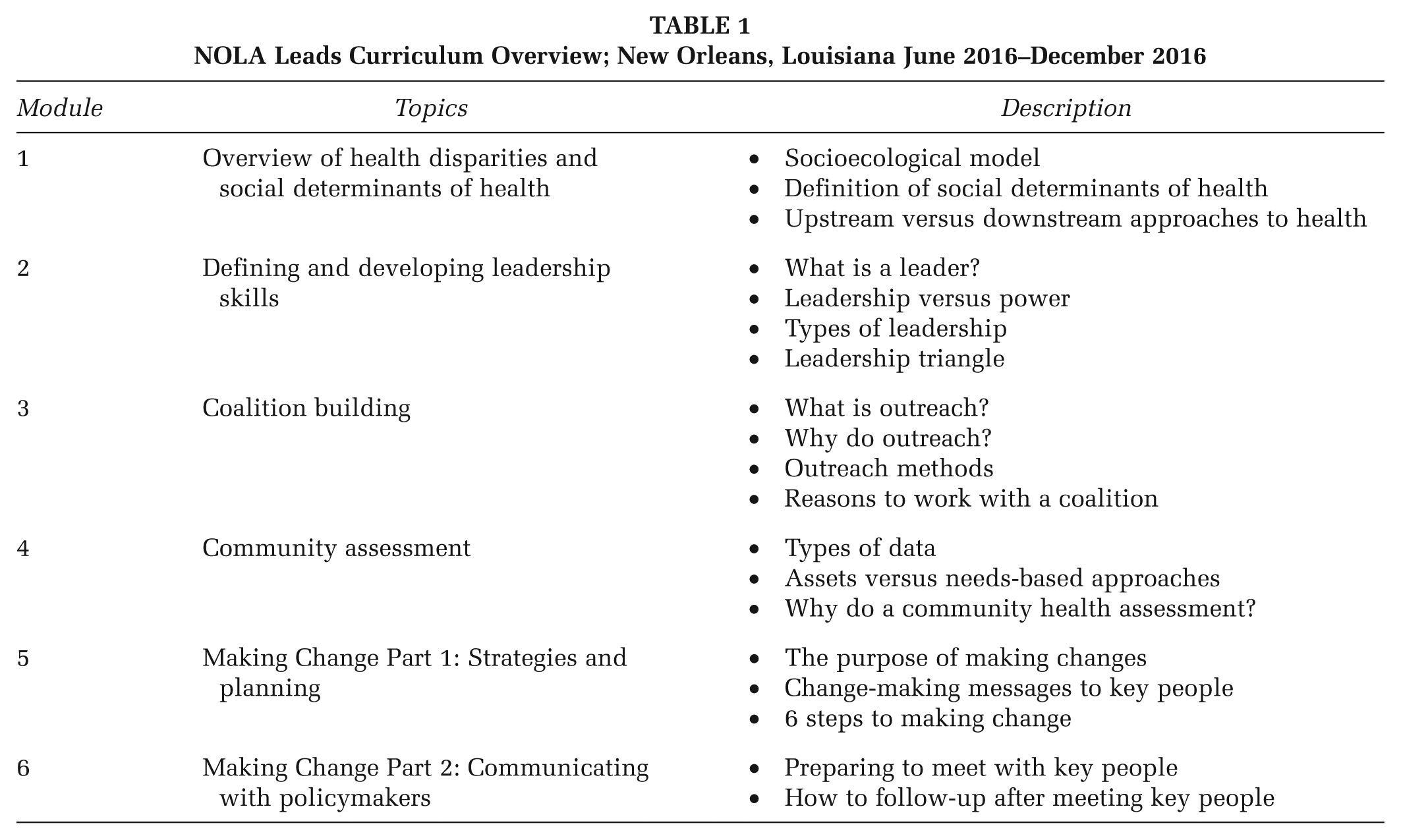
For this project, we removed elements of the existing curriculum such as case management, navigating the health care system, and individual-level health coaching that were not relevant for nonprofessionals, but kept topics and skill development elements related to understanding and addressing the root causes of community health problems. Specifically, we retained modules focused on social determinants of health, leadership, creating coalitions, conducting strengths-based community assessments, strategies for making change, and communicating with key leaders. An overview of the final 36-hour curriculum topics is included in Table 1.
NOLA Leads Curriculum Overview; New Orleans, Louisiana June 2016–December 2016
As with our previous training, the curriculum was based on adult learning principles that allowed participants opportunities to draw on relevant life experience and apply knowledge outside the course (Cranton, 2014). Specific teaching and learning techniques included small group activities, large group discussion, paired work, icebreaker activities to encourage interaction, and limited lecture. We also included a total of six local co-trainers who conveyed information about specific social determinants of health identified as important by CAB members (e.g., mental health and the criminal justice system) and led group activities related to strategies for making change such as engaging leaders, creating coalitions, and communicating via social media.
In addition, at the beginning of each cohort participants collaborated to create a list of social determinants of health in which they were interested. To ensure that participants had sufficient background information on these issues, we discussed them at length in class. We also created and distributed to participants a brief report including local background information and data on these social issues to serve as a reference. Participants then individually ranked topics from the list the class created based on personal interest and formed small groups in accordance with their rankings. Throughout the course, each group then worked on a series of successive activities to create a concrete plan that could be reasonably implemented outside of class to address the social issue of interest. Some of these activities included planning a needs assessment, cataloging existing community resources, identifying relevant stakeholders to develop a coalition, determining a policy action to address an issue, and creating a plan to contact and engage with a policymaker with authority to address the selected issue. Participants received a binder of materials to support in-class discussion and activities and serve as a reference for anticipated postcourse actions.
Training Sessions
Between July and December of 2016, we conducted two rounds of training at local churches in two different neighborhoods that faced disparities in life expectancy. In one area, life expectancy was 70.6 years and in the other, it was 67.6 years, as compared with 72.0 years in Orleans Parish overall and 74.0 years in all of Louisiana (Joint Center for Political and Economic Studies, 2012). Classes met for 6 hours on Saturdays for 6 weeks, and we provided breakfast and lunch each day. We offered a $150 gift card to thank participants for their time on successful completion of the program.
Data Collection
At baseline, participants received a brief survey that included items assessing demographics, level of confidence in government institutions, and several measures of civic and political participation in the past year.
At each of the six sessions, participants completed a brief five-question pre- and posttest to assess baseline knowledge and immediate retention. We were interested in changes in knowledge. Questions addressed the topic for each session and consisted of multiple choice and open-ended questions. Participants were scored as to whether they answered the questions correctly or not. Participants also completed a session evaluation each day. We asked participants to rank on a 5-point scale how useful they perceived each topic and guest speaker to be (0 = not useful at all to 4 = extremely useful).
Data Analysis
Frequencies were determined for the demographic characteristics. Median age and interquartile range (IQR) were calculated as the majority of participants were older. T tests were used to assess differences between pre- and posttest score for each lesson. A p value of .05 or less was considered significant. To evaluate knowledge gained from the sessions, means scores and standard deviations were calculated for the course evaluation data by session. SAS Version 9.4 was used to analyze the data.
All research procedures were approved by the Tulane University Institutional Review Board, and all participants provided written informed consent to participate in the study.
Results
A total of 64 individuals submitted applications to attend the course. All were notified via their preferred contact method (e-mail or phone) that they were eligible to participate. A total of 43 people enrolled and attended at least one class, and 42 people successfully completed the course by attending at least four of six sessions. The majority of participants were female (92.7%), Black (92.7%), and had completed at least some college (69.0%). Nearly half (45.2%) of the sample had an annual household income of less than $20,000 per year. Most (73.8%) were retired or unemployed, and the median age was 61.5 years (IQR: 55.0-71.0 years). Participant demographics are detailed in Table 2.
Demographic Characteristics of Community Health Training Participants (n = 42); New Orleans, Louisiana, June 2016–December 2016
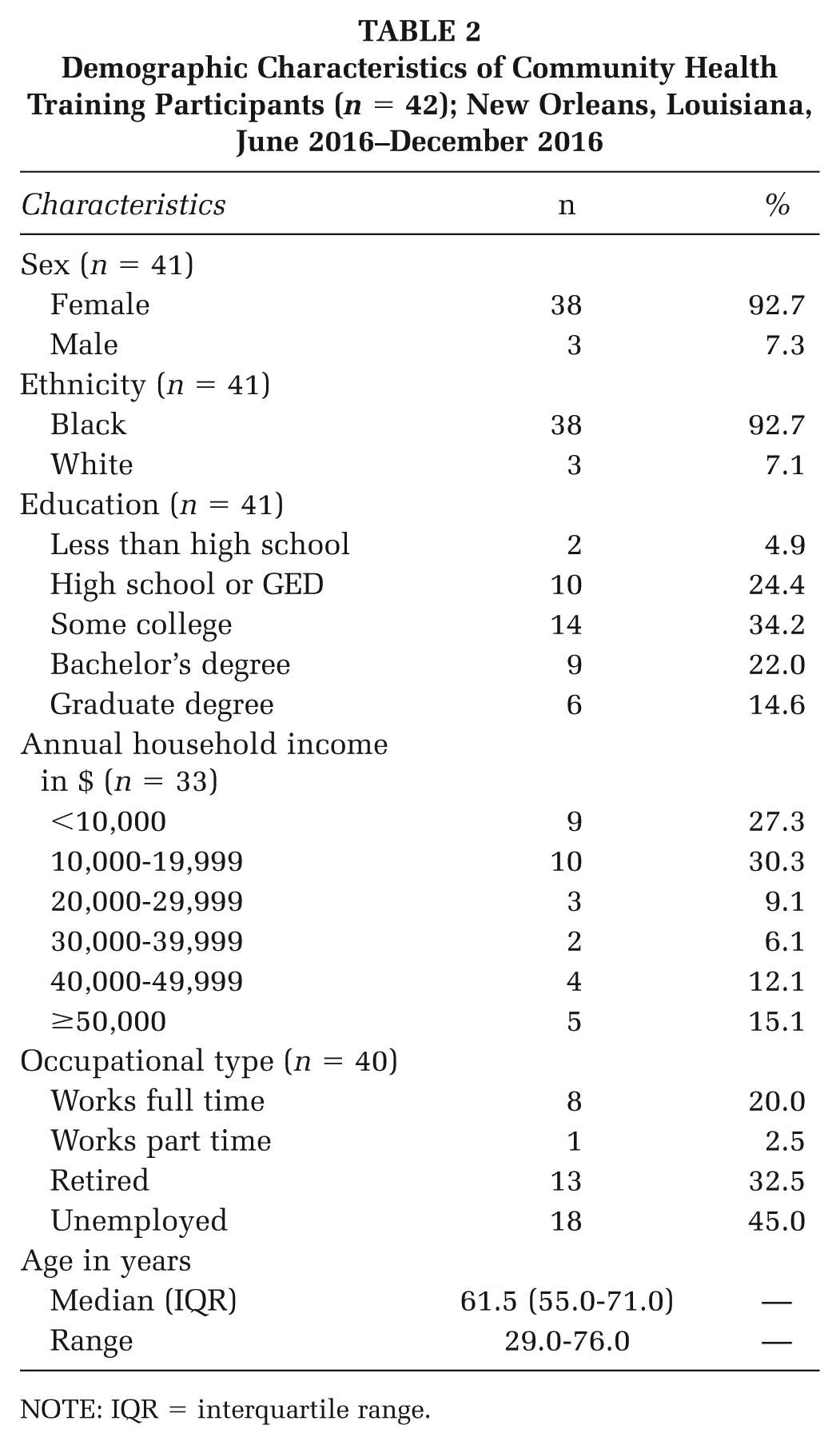
NOTE: IQR = interquartile range.
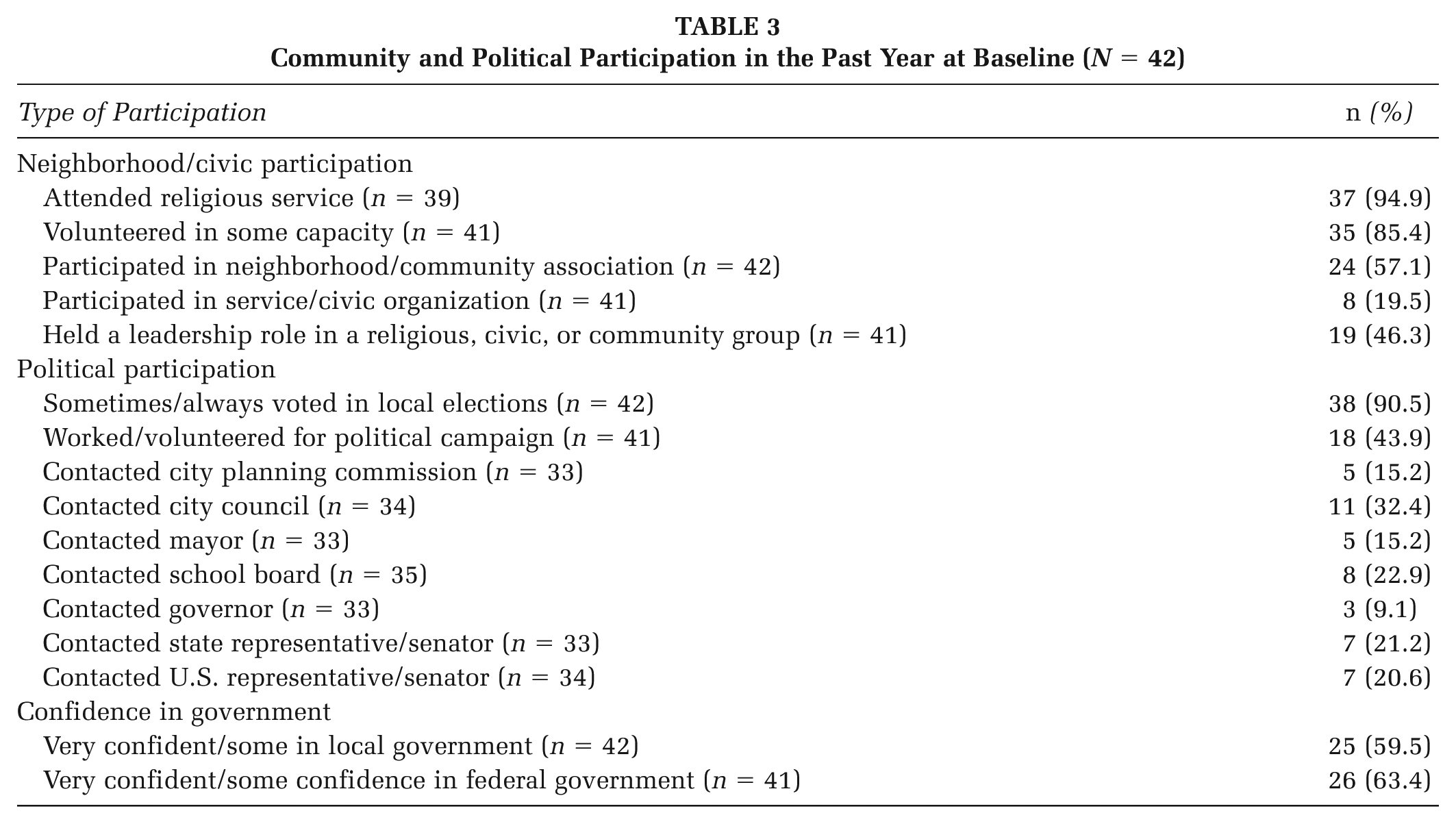
At baseline, 95% of participants reported having attended religious services in the last year, 85% had volunteered in some capacity, and nearly three fifths (57.1%) reported recent participation in a neighborhood or community organization. Roughly one in five had been involved with a civic or service organization, and nearly half (46.3%) reported holding some leadership role in the previous year. More than 90% of participants indicated they sometimes or always voted in elections, and 43.9% had been involved in a political campaign. With regard to contacting local policymakers, roughly 15% each had been in touch with the city planning commission and mayor. Nearly one third (32.4%) had contacted city council, and almost one quarter (22.9%) reached out to the school board. Contact with state-level legislators included 9.1% and 21.2% of people having called on the governor or a Louisiana representative or senator, respectively, for help. Approximately one in five (20.6%) had approached a U.S. representative or senator. About three fifths reported some or high confidence in local government and 63.4% had the same perspective on the federal government. A summary of these results is presented in Table 3.
Community and Political Participation in the Past Year at Baseline (N = 42)
We found significant increases in knowledge in five of the six sessions. The largest increase in posttest scores occurred in Session 5, (Making Change Part 1: Strategies and Planning) followed by Session 3 (Coalition Building). The first session, which focused on health disparities and social determinants of health did not result in a significant increase in knowledge between the pre- and the posttest (p = .615). Figure 1 contains a summary of these results.
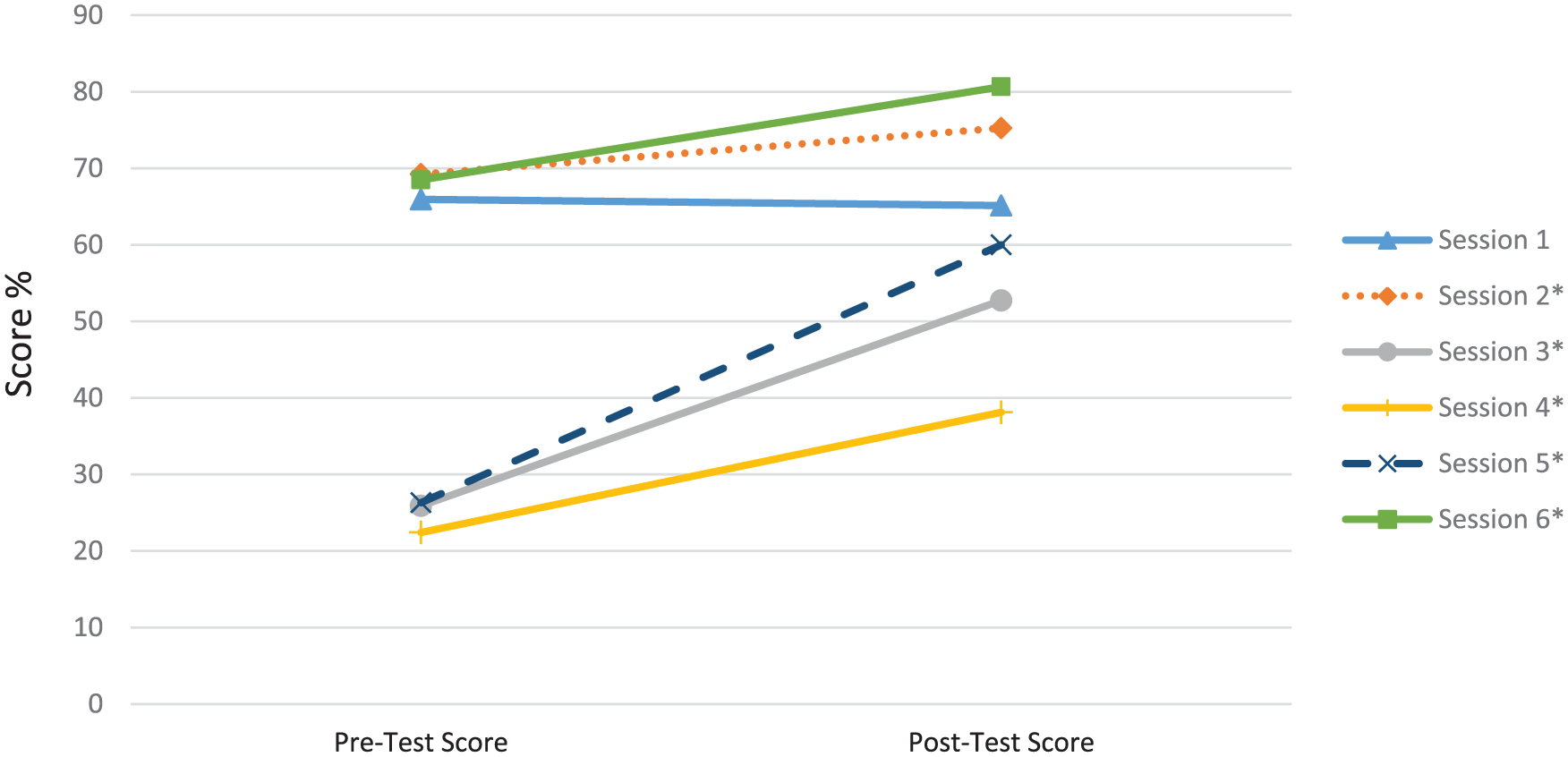
Mean Participant Knowledge Score From Pretest to Posttest, New Orleans, Louisiana, June 2016–December 2016
Participants rated the usefulness of each lesson and topic fairly uniformly highly. On a scale of 0 to 4, session component scores (M ± SD) ranged from 3.7 ± 0.5 for the introduction to Session 1 (Overview of Health Disparities and Social Determinants of Health) to 4.0 ± 0.0 for the overall class Making Change Part 2: Communicating with policymakers (data not shown). Reflecting the nearly uniform perceptions of participants toward the program, one respondent commented: “Every guest speaker has been outstanding in their presentation. The speakers are informative, educated and willing to share their knowledge with us. Very thankful and grateful for these classes.” Another stated that they could “. . . hardly wait for [the] next Saturday. I really enjoyed the class. It was educational and informative.” Another mentioned, “[I] learned a whole lot that I can take back to my family and friends.”
Discussion
In this article, we describe the implementation and immediate results of a using a modified CHW training curriculum to prepare lay community residents with knowledge and skills to address social determinants of health through implementing community development projects, creating coalitions, and communicating with policymakers to change laws. We found significant increases in knowledge for every session but the first. Overall, participants found the entire program highly useful.
We were very pleased with the program completion rate of 97.8%. Offering a significant incentive likely supported retention. We initially faced challenges with recruitment, with only nine people completing the first cohort. However, our enrollment increased substantially in the second cohort due to recruitment through word of mouth from previous attendees, one of whom engaged fellow members of a local nutrition education program for which she volunteered. Future leadership training programs may benefit from identifying trusted community members to support recruitment.
We attributed our participants’ ability to attend a lengthy course to having limited other commitments since they were older and mostly retired or unemployed. We found their participation promising because retired and semiretired individuals have been shown to be a valuable resource and effective advocates in the fields of conservation (Fraser, Clayton, Sickler, & Taylor, 2009) and education about aging (Couper, Norsman, & Sulick, 1999), which suggests our trainees may also go on to advocate for issues about which they have a personal passion, including the social determinants for which they created action plans in the class groups. Having a strong psychological sense of community has been shown to predict volunteerism among retirees (Omoto & Packard, 2016) so our participants’ high rate of volunteerism suggests an existing community connectedness that, combined with newly gained knowledge about coalition building and strategies for implementing change, may prompt additional engagement with policymakers. Similarly, trainees’ propensity to vote regularly may also indicate confidence that engaging in political processes produces worthwhile results. Given their high rates of involvement with religious and civic organization, our participants, like CHWs, are likely well-known, trusted members of their communities who are natural helpers. As such, they are likely to be perceived as reliable sources of information if they share knowledge gained from the course with fellow congregants and group members. They may also speak on behalf of their communities, helping to support the work that existing CHWs are doing or even helping to fill a void that could be created if CHWs newly working in clinical, rather than community, settings are unable to engage in community advocacy.
Although most people expressed interest and were actively engaged in Session 1 (Overview of Health Disparities and Social Determinants of Health), the lack of increase in knowledge for that session may be attributable to community residents entering the course with an intuitive understanding of the relationship between social issues and poor health, as has been demonstrated elsewhere (Kaplan, Madden, Mijanovich, & Purcaro, 2013). Alternatively, our teaching techniques may have been too academic or otherwise inadequate to convey the complex causal relationship between social issues and health outcomes. We were encouraged that participants experienced a change in knowledge about leadership skills, as leadership training has been shown to be associated with community-level advocacy (Ingram, Sabo, Rothers, Wennerstrom, & de Zapien, 2008). Based on class discussions, we attributed the significant increase in knowledge in Session 3 (Coalition Building) to lack of prior experience working in organized groups to effect community change. Although participants demonstrated a significant increase in knowledge after Session 4 (Community Assessment), their relatively low mean posttest score (38.1%) was likely due to the complex nature of the topic. Our instruction about methods of collecting quantitative and qualitative data may have been overly complex and better illustrated through other methods such as community mapping. Positive changes in knowledge in Sessions 5 and 6, which detailed methods of reaching and communicating with policymakers (e.g., implementing letter writing campaigns and preparing for and conducting effective legislative visits) may be promising for future participant engagement with leaders.
Overall, program participants were enthusiastic, receptive, and found the sessions useful, as was the case for the course from which this curriculum was adapted (Wennerstrom et al., 2014). We believe these findings are likely attributable to our use of relevant information about social determinants of health, local expert guest co-trainers, adult learning techniques, and familiar community-based locations for training.
One unexpected outcome was that our second cohort requested physical activity during the class. One participant volunteered to lead the class in line dancing (a common activity in New Orleans) at the beginning of each day and after lunch. Our curriculum was flexible enough to allow for the adaptation, and the activity was well received. Although this may have been unique to our cohort, other programs may benefit from incorporating some movement or other culturally appropriate activities to keep participants engaged. In addition, in each cohort, one participant had childcare challenges, so we allowed that participant to bring children. Future programs may consider providing childcare.
This study is limited in that there was no control group and there may be selection bias, as people who chose to participate may differ from other community members. We have assessed only baseline community participation and changes in knowledge at this juncture, although we will conduct follow up to assess changes in behavior related to civic engagement at 6-month posttraining. This study took place in only one city, and results may not be generalizable to other areas or younger populations.
There are several strengths that are important to highlight. The curriculum was well-received, likely because it was modified from a previous successful training program (Wennerstrom et al., 2014). It is adaptable to other topics and social issues that could be incorporated depending on community needs. The sessions included guest speakers as topic experts who were from local organizations and offered their contact information to participants for follow-up at a later date. Participants provided encouraging feedback on the sessions and had a desire for more and continued training.
Conclusion
Overall, we found it was feasible to train lay community members in health leadership skills using an adapted existing CHW training curriculum. The significant increases in knowledge and high rates of participation are promising and provide initial support for the concept of training community members in leadership skills to address social determinants of health in underserved communities. Future work is needed to determine if the training program resulted in longer term retention of knowledge and motivated participants to take on any leadership roles or advocacy activities in their community.
Footnotes
Authors’ Note:
The authors thank the members of the Tulane Prevention Research Center Community Advisory Board for their contribution to this project. This publication was supported by Cooperative Agreement No. U48DP005050 and Special Interest Project No. 15-006, under the Health Promotion and Disease Prevention Research Centers Program, funded by the Centers for Disease Control and Prevention. The findings and conclusions in this journal article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention. Ashley Wennerstrom and Miranda Pollock are now at LSU Health Sciences Center–New Orleans.