
Abstract
Background. African Americans suffer a disproportionate burden of tobacco harm and researchers have posited that menthol cigarettes are a key contributor to this disparity. In 2015, a county health department and African American community-based organization (CBO) in Minnesota partnered to educate and engage the African American community on menthol and its role in tobacco-related health disparities. The following case study describes successes, challenges, and recommendations from this work. We focus on the role of a public health and community partnership in menthol policy adoption so others can more effectively implement a community-driven approach in their own communities. Methods. Interviews were conducted with local and state public health staff, leadership from the CBO, youth coordinators, and change agents—that is, leaders in the African American community recruited to educate and engage the community on menthol. Interviews were transcribed verbatim and analyzed in Atlas.ti using thematic analysis. Results. Participants identified several successes: (1) assessment data from community members helped inform policy decision making, (2) collaboration between local public health and CBO was powerful and a key to success, and (3) change agents were trusted communicators and effectively engaged and provided education to the community. Participants faced challenges related to stylistic and cultural differences in communication. Participants recommended engaging youth and incorporating cessation into the broader context of issues systemically affecting African American communities (e.g., economic inequity, police violence, incarceration). Implications. Menthol tobacco restrictions have the potential to reduce tobacco-related health inequities for African Americans. Findings highlight the role that public health and community partnerships can play in supporting this critical work to effect policy change.
Background
Menthol tobacco use is more common among African Americans than among other racial/ethnic groups. An estimated 72% of African American adult smokers and 88% of African American youth smokers report smoking menthol cigarettes compared to 22% and 26% of white adult and youth smokers, respectively (Giovino et al., 2013; Keeler et al., 2016); similar disparities exist in Minnesota, where 79% of African American adult smokers smoke menthol compared to 19% of white adult smokers (D’Silva, Amato, & Boyle, 2015). The Truth Initiative defines menthol as a chemical compound that is extracted from peppermint or corn mint plants, or is created synthetically. Menthol increases the likelihood of initiation and progression to established smoking among youth (Nonnemaker et al., 2013), enhances the addictiveness of tobacco (Henderson et al., 2016), and decreases the likelihood of successful cessation for adults—especially among African Americans (Delnevo, Gundersen, Hrywna, Echeverria, & Steinberg, 2011; Okuyemi et al., 2003; Stahre, Okuyemi, Joseph, & Fu, 2010). Researchers have suggested that menthol is a key contributor to tobacco-related health disparities experienced by African Americans (Alexander et al., 2016; Gardiner, 2004; Garrett, Gardiner, Wright, & Pechacek, 2016; Pletcher et al., 2006).
Menthol tobacco sales restrictions have the potential to help reduce these disparities by limiting access to menthol (Fagan et al., 2004) and promoting quit attempts (Chaiton, Schwartz, Cohen, Soule, & Eissenberg, 2018). Progress on menthol policy is relatively recent, with 32 cities and counties in the United States implementing policies as of June, 2019. Given the nascent stages of menthol policy passage, literature documenting the menthol policy process is scant. More work is needed to document how best to support these policies. In addition, while many studies have examined community partnerships through community-based participatory research (Israel et al., 2019; Israel, Schulz, Parker, & Becker, 1998), few have investigated public health and community partnerships in the context of tobacco policy. Little is known about how such a partnership could strategically support work toward menthol tobacco sales restrictions. The current study aimed to examine how a partnership between public health and the community can support menthol policy change.
Menthol Cigarette Intervention Grant
In 2015, the Minnesota legislature passed legislation requiring the Minnesota Department of Health (MDH) to investigate menthol tobacco use among African Americans in Minnesota. This funding—the Menthol Cigarette Intervention Grant (MCIG)—was awarded to a metropolitan county health department who partnered with three other metropolitan health departments. MDH recommended that the awardee direct 70% of the funding to a community-based organization (CBO). When it began, MCIG was one of three funded projects in Minnesota that targeted menthol tobacco use between 2015 and 2017. Collectively, these projects built momentum that culminated in policy changes that restrict the sale of menthol tobacco to adult-only stores in three of Minnesota’s most populous cities between August, 2017 and February, 2018 (ClearWay Minnesota & Blue Cross and Blue Shield of Minnesota, 2019).
The local public health departments (LPHD) worked closely with the CBO in the two primary phases of MCIG: assessment and community engagement. In the assessment phase, MCIG staff identified key stakeholders and potential partners, conducted community assessments and interviews with community members, and developed community awareness and outreach strategies based on assessment data. In the engagement phase, community members were asked for input on the direction of the grant, and media activities (e.g., radio, newspaper, social media) and community events were held to mobilize the community and educate on the harms of menthol tobacco use. “Change agents” (i.e., community leaders who were recruited to educate and engage the community on menthol) delivered education and engagement presentations using a slide deck developed by a local tobacco prevention and control nonprofit organization. Many of the change agents were leaders in the faith communities and thus had regular contact with community members. In addition to change agent presentations, youth groups helped educate the community. With the help of youth coordinators, youth collected data by taking photographs of how menthol had affected their community, conducting interviews with community members, or hosting community discussions. The youth then analyzed the data and presented at community events about menthol harms, industry targeting, and what they were seeing and hearing in their community (see Kingsbury & Hassan, 2018, for a more complete description of grant activities). Data collected during the assessment phase informed advocacy efforts including policy recommendations to state and local government and city council testimony by youth, change agents, and the CBO. In addition, partner organizations (e.g., faith-based organizations, other CBOs) who were introduced to menthol work through MCIG joined advocacy efforts by writing letters to the editor and met with decision makers after MCIG ended.
Interviews with key MCIG personnel were employed to evaluate this work. Our specific research questions were
Method
Participants
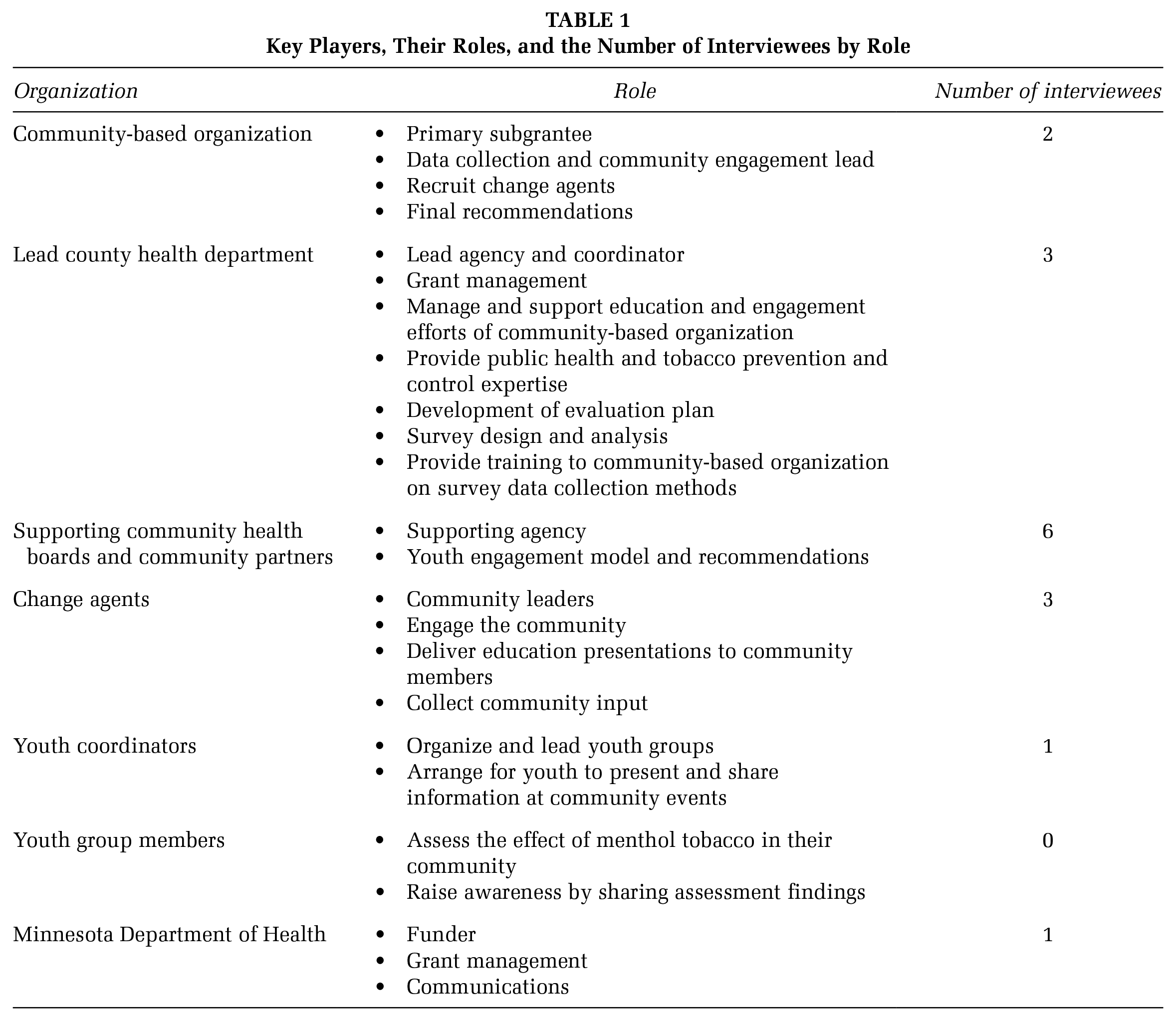
Individuals who played an integral role in the execution of the grant or implementation of grant activities were identified as prospective participants. Eighteen prospective participants were recruited via email invitation. Two individuals who accepted the invitation were not interviewed due to scheduling difficulties. Participants from the same institution were given the option to conduct a joint interview in lieu of individual interviews. A total of 12 in-person, semistructured interviews were conducted with 16 participants (8 individual interviews and 4 joint interviews with 2 participants each). For joint interviews, each participant was given the chance to answer questions individually or delegate answers to one another. Study participants were the state grant manager, local health department staff (e.g., project coordinators, evaluators, program managers), CBO project coordinator and executive director, youth coordinators, and change agents (see Table 1 for role descriptions).
Key Players, Their Roles, and the Number of Interviewees by Role
Procedure
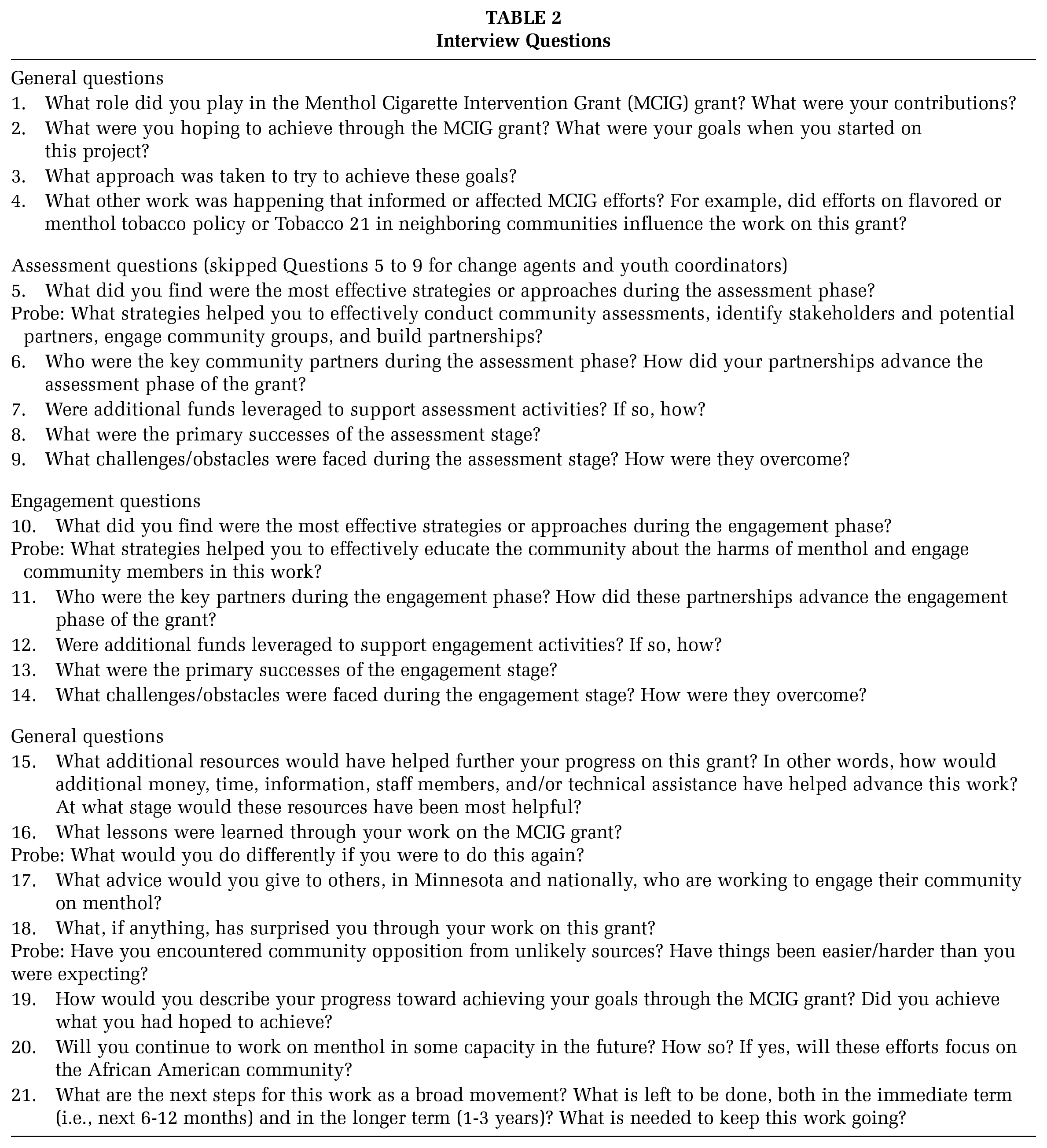
Interviews were conducted by an MDH intern and averaged 60 minutes in length. The interview guide was developed after a review of the literature for case studies that focused on partnerships with communities. This review helped inform the development of questions that would help capture the nuances of the work in the community. Key MDH staff were also involved in the development of the interview questions as these individuals had a pulse on what made this project unique and what might be useful to others doing similar work. Interview questions were structured to assess perceptions, key successes and challenges, and lessons learned from each phase of the grant, followed by questions about the grant as a whole and future directions (see Table 2). The same interview guide was used for all participants, although questions that were irrelevant for particular participants were skipped (e.g., asking change agents about the assessment phase). Participants were not compensated for the interviews. This study was approved by the MDH Institutional Review Board.
Interview Questions
Data Analysis
Interviews were audiotaped with participant permission and transcribed verbatim. The authors used an iterative process of coding and thematic analysis (Braun & Clarke, 2014). Transcripts were initially reviewed for emergent themes and concepts and then were coded using ATLAS.ti (Friese, 2019). The authors met several times to discuss initial results, reach consensus on primary themes, and interpret the results.
Results
Several major themes emerged from the interviews (see Table 3). Themes were similar across participant role so were summarized in aggregate as opposed to by role. Themes were grouped into three categories: successes, challenges, and lessons learned/recommendations.
Illustrative Quotes by Theme
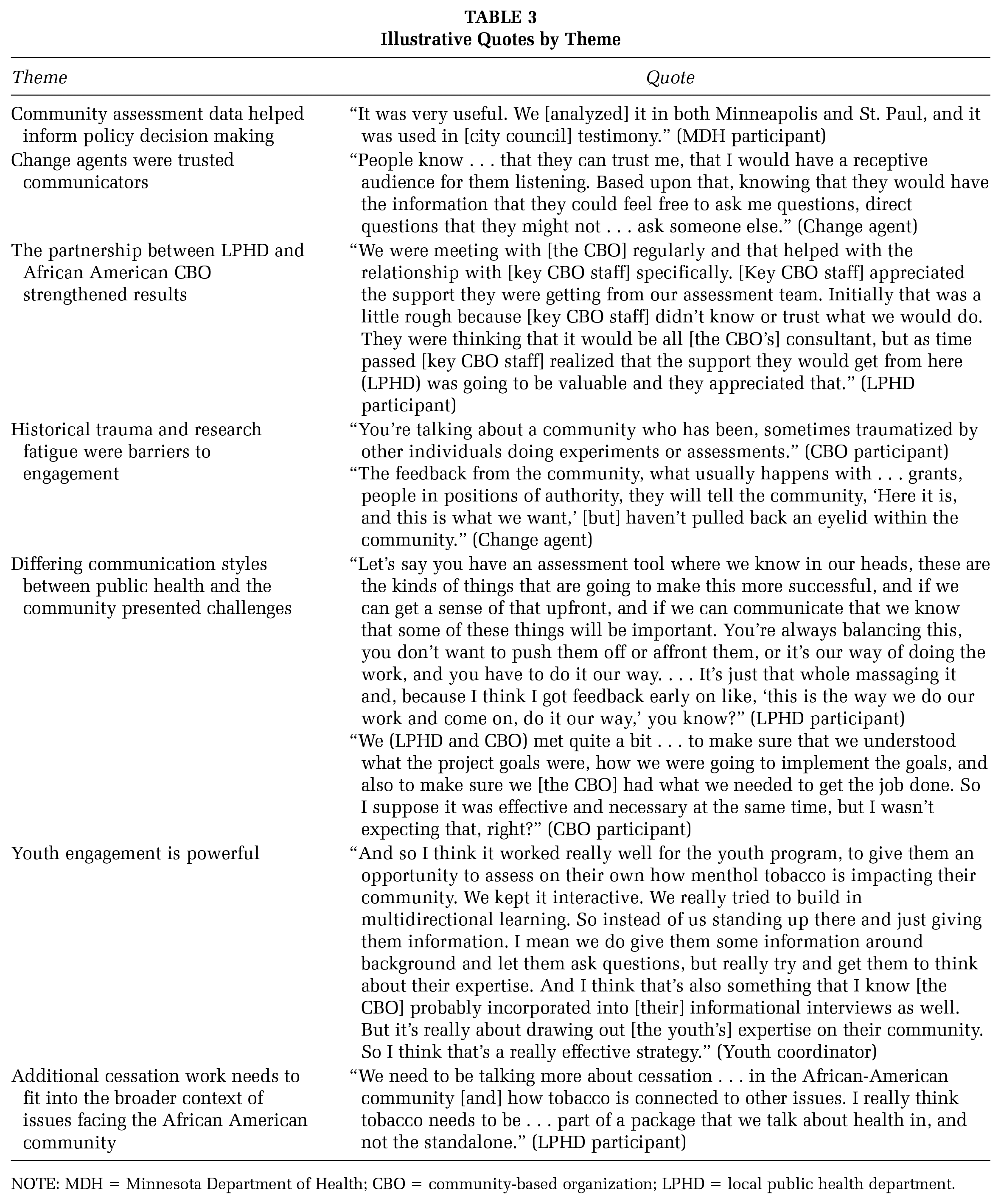
NOTE: MDH = Minnesota Department of Health; CBO = community-based organization; LPHD = local public health department.
Successes
Community Assessment Data Helped Inform Policy Decision Making
Assessment data were widely praised as not only being good data but useful in informing policy decision making. An MDH staff member said, “It was very useful. We [analyzed] it in both Minneapolis and St. Paul, and it was used in [city council] testimony.” By capturing “sort of a deeper, qualitative kind of pulse on the community,” a compelling and persuasive public health case was made. The data helped build a research-informed, community-driven case to support what later became successful policy changes that restricted the sale of menthol tobacco products to adult-only stores in Minneapolis, St. Paul, and Duluth. Assessment data were presented as part of city council testimony in each of the three cities. These presentations helped deepen knowledge about menthol tobacco among council members and in the community, and enhanced credibility of the arguments in favor of menthol restrictions (ClearWay Minnesota & Blue Cross and Blue Shield of Minnesota, 2019).
Change Agents Were Trusted Communicators
Engagement and education efforts, which were primarily led by the change agents, assisted in building trust between LPHD and the community. Education focused on tobacco industry targeting of African American communities, breaking down myths and misconceptions about menthol, and providing guidance on obtaining cessation resources. One change agent described her mission: “To provide information to the community . . ., to educate them about the harmful effects of menthol, that the tobacco industry targeted particular African American people . . .”
Change agents conveyed public health knowledge with a combination of research, historical takes, anecdotes, and tangible aides. One change agent used visual aides to educate about menthol, relaying the following:
I held up Vicks Vapor Rub, I let some people smell it. I said, who grew up with this? Because it’s menthol . . . I said what’s in it? Menthol? Menthol. I said and what does it do? They said it soothes you, it refreshes you, and it calms you down. I said yes. The same . . . substance, menthol, is in cigarettes, these menthol cigarettes. It makes us feel calmer. It refreshes us, it calms us down . . . but it’s bad for you [because it makes it easier to initiate and harder to stop smoking].
All parties felt that the work of change agents made building trust easier. One public health staff member pointed out the change agents’ value by noting, “These are people who actually have connections to the radio advertisements [a component of MCIG media outreach], to people who maybe have been subjected to menthol in a harsher way.” The change agents’ ability to empathize from their own experiences served as a key tool to build trust and further the goal of community-driven solutions and policy.
The change agents recognized this advantage as well, characterizing it as a liaison role, communicating and facilitating information sharing between public health and the community. A change agent elaborated on how
people know . . . that they can trust me, that I would have a receptive audience for them listening. . . . They could feel free to ask me questions, direct questions that they might not . . . ask someone else.
This influence is coupled with the responsibility of conveying accurate information back to the community. “We have to have the facts to give to our community and let them know they [the tobacco industry] don’t mean us any good. You’re smoking your life away.”
The Partnership Between LPHD and African American CBO Strengthened Results
Staff from MDH, LPHD, and CBO identified the partnership between LPHD and CBO as a key strength of this project. Each partner played a unique and integral role in the planning and implementation of the project. As trusted messengers with relationships in the community, the youth groups and CBO staff brought insight and expertise to the project, effectively engaged the community, carried out assessment and education activities, and led the work in the community. LPHD provided ongoing support and technical assistance to the CBO throughout the project by connecting them with educational materials, providing public health and tobacco expertise, and offering tools to document community attitudes on policy options. LPHD also provided help with survey design, data analysis and interpretation, developed communication materials, and assisted in thinking through recommendations that would sustain the impact of the grant and inform future work.
Challenges
Historical Trauma and Research Fatigue Were Barriers to Engagement
Participants from public health were cognizant of the historical interaction between public health research and underrepresented communities. One CBO participant said, “You’re talking about a community who has been, sometimes traumatized by other individuals doing experiments or assessments.” Another CBO participant commented, “One of the big areas that we’re trying to get a foothold in is in the whole area of Culturally Sensitive Trauma-Informed Care, right? We have a lot of trauma in the community.” Some subsects of the African American community in the Twin Cities area have voiced research fatigue, particularly in contexts where repeated engagements are perceived as not leading to change. This sentiment was echoed by the change agents who were working directly with the community. One change agent reported: “what usually happens with . . . grants, people in positions of authority, they will tell the community, ‘Here it is, and this is what we want,’ [but] haven’t pulled back an eyelid within the community.” Public health and CBO staff were cognizant of this and expressed a strong commitment to involving community perspective in developing data collection methods and sharing results with the community in a way that incorporated historical context.
Differing Communication Styles Between LPHD and the Community Presented Challenges
Communication and mutual understanding of expectations, priorities, and adhering to rules and regulations proved to be an obstacle for all parties. However, many saw this positively as an opportunity to learn cross-sectoral perspectives on assessment and a learning experience overall.
Participants were aware that it takes considerable time to develop strong relationships between the community and local/state government. If the relationship has not advanced far enough, dealing with issues that arise can be challenging. In some instances, one party may be forced to choose between maintaining the relationship and ignoring the issue or addressing the issue directly and risk fracturing the relationship. Participants mentioned issues with communication and transparency that stemmed from a difference in perspective. Sometimes, what LPHD felt was attention to detail and following grant requirements was interpreted as too much oversight by community partners. Community partners felt they had expertise on what works in their communities and how community members would respond which was not always consistent with the procedures stipulated by the grant. Communication barriers were overcome largely through compromise (e.g., softening deadlines) and became less prevalent toward the end of the two-year grant once a stronger relationship between LPHD and CBO had been built.
While less detailed grant requirements could address these specific issues, the broader message conveyed by participants was that establishing relationships with the community is critical to success of this work. Starting early and cultivating relationships well before the work begins allows for easier and smoother interactions and can provide a solid foundation for resolving any issues that arise as the work progresses.
Lessons Learned/Recommendations
Youth Engagement Is Powerful
Several participants expressed an interest in continuing to engage youth and recognized adolescence as an ideal time for tobacco intervention. Some participants had specific policy goals in wanting to engage youth. Other LPHD participants saw this as a long-term intervention strategy viewing it from the perspective that if, “you remove more of that social source, from that younger age, ultimately the goal is that we will have less and less kids smoking, and less and less kids addicted to menthol, too.” Participants felt that educating youth, and, in turn, having youth as educators—that is, giving presentations to community members and advocating for policy change via city council testimony—was an influential strategy and had an impact on decision makers.
Additional Cessation Work Needs to Fit Into the Broader Context of Issues Facing the African American Community
A clear theme that emerged throughout the interviews was advocacy for more cessation work, particularly cessation programming that is integrated and mainstreamed into a comprehensive public health response. A staff member from LPHD expressed that
we need to be talking more about cessation . . . in the African-American community [and] how tobacco is connected to other issues. I really think tobacco needs to be . . . part of a package that we talk about health in, and not the standalone.
The participants recognized that the African American community in Minnesota has many public health concerns, of which tobacco is only one. For example, high rates of violent crimes, parental incarceration, and police violence may be higher priorities and receive more attention. Tobacco and menthol work would be more impactful if it was reconfigured to acknowledge these larger constructs that interconnect to affect the health of communities. These efforts should consider the broader context of public health issues facing the African American community.
Discussion
Results of this study demonstrate how a strong partnership between public health and the community can support menthol tobacco policy change. This partnership collected data from the community on perceptions and use of menthol (Kingsbury et al., 2019), educated the African American community about menthol through presentations and media, and engaged the community on menthol policy change. These efforts, along with those of partner organizations, contributed to successful policy changes restricting the sale of menthol tobacco to adult-only stores in three of Minnesota’s most populous cities. While research evaluating menthol policies is scant, a recent study by Chaiton and colleagues (2018) reported that, following a ban on menthol sales, 29% of menthol smokers tried to quit. These findings highlight the potential for menthol sales restrictions to increase cessation; this may be especially true for African Americans given their disproportionately high use of menthol tobacco.
The themes identified from interviews with key MCIG personnel underscore the power of data and public health–community partnerships to effect change. Local assessment data, which provided insight into the community’s use and perceptions of menthol, strengthened arguments in favor of restricting menthol tobacco sales. This finding is consistent with previous research demonstrating that local data are particularly influential to decision makers (McGill et al., 2015). The partnership between LPHD and the CBO was integral to MCIG’s success and helped facilitate the work of those conducting community education (i.e., change agents and youth groups). LPHD served as a resource to the CBO, and the CBO served as a resource to the change agents. This collaboration allowed for the smooth transfer of information about the harms of menthol from public health to the community. Moreover, the presentation of this information was likely more effective because it was coming from a well-respected and usually well-known community leader as opposed to a public health official who may have been unknown in the community (Chen, Bell, & Taylor, 2016; Phua, 2016).
Despite the strength of this partnership, there were some challenges related to communication and understanding of grant requirements. These challenges highlighted the need for clear communication of expectations and requirements early on in the partnership to ensure mutual understanding of roles, responsibilities, and deliverables. While communication challenges may be unavoidable in many instances, forming a strong relationship can lead to easier resolutions when challenges arise.
Participants offered recommendations for others pursuing menthol tobacco policy restrictions. The themes that emerged reflected the need for culturally relevant cessation for African American menthol smokers. Many African American menthol smokers report that they would quit if menthol was no longer sold in stores (D’Silva et al., 2015; Kingsbury et al., 2019). Public health and medical professionals need to complement new menthol policies with cessation resources that are tailored to African American smokers and take into account other important issues facing the community, including both those that are tobacco related (e.g., industry targeting, reduced success with cessation medications (Okuyemi et al., 2003) and those that are not (e.g., parental incarceration, police violence).
Implications for Practice
Menthol tobacco sales restrictions are becoming increasingly common. As the number of jurisdictions pursuing menthol restrictions increases, so too does the need for information on how best to support these policies. Results from this study suggest that community assessment, education, and engagement is a promising model for mobilizing the community and supporting menthol policy advocacy efforts. In this project, the CBO was very effective in recruiting other organizations to join this effort and to continue working on menthol. Sharing this work with youth and other organizations who were motivated to contribute helped increase momentum. Advocacy efforts, including letters to the editor, meetings with decision makers, policy recommendations from the CBO to local and state government, and city council testimony by youth, community members, and the CBO were influential and contributed to the passage of menthol sales restrictions.
Partnerships between LPHD and the community, which require time to develop mutual trust and understanding, can be powerful. LPHD can serve the role of experts on health risk information and data on menthol use and perceptions, and the community—and in particular, community leaders—serve as powerful messengers. This sort of model may be particularly effective in jurisdictions where there is a limited existing relationship between public health officials and the African American community.
Limitations
This study has a few limitations that should be considered when interpreting findings. These data were collected in a state with an advanced tobacco control program so results may not generalize to other locations with different political and social climates. Additional studies are needed to delineate how public health and community partnerships differ across political climates. Work from this grant coincided with two other funded projects targeting menthol tobacco so it is difficult to determine the precise affect this project had on the passage of menthol tobacco restrictions. Last, some interviews were conducted jointly for individuals from the same institution. It is possible that joint interviews yielded biased responses whereby a difference of opinion may not have been expressed. Future studies should conduct private interviews to avoid this potential bias.
Conclusion
The MCIG aimed to reduce menthol tobacco use in African American communities through educating and engaging the community, and by supporting policy advocacy efforts. The success of this project was due to a strong collaboration between LPHD and CBO, the collection of local assessment data which was used in city council testimony and helped inform policy decision making, and the use of change agents to educate and engage the community. Local and state health departments and advocacy organizations who will be pursuing menthol sales restrictions should allow time to develop a relationship with the community, engage youth in this work, and employ community leaders to mobilize and educate the community. Results highlight the powerful role that a public health-community partnership can have in advancing health equity through menthol policy efforts.
Footnotes
Authors’ Note:
We would like to thank the African American Leadership Forum for the exemplary job they did recruiting participants, collecting data, and engaging the African American community. They played an integral role in the success of this project and we are appreciative of these important contributions. We would also like to thank Hennepin County Public Health Department for their leadership in shepherding this project and all of its collaborators, and the Minneapolis, Bloomington-Edina-Richfield, and St. Paul-Ramsey Health Departments for their support in advancing this work. This work was funded by the Minnesota Department of Health’s Statewide Health Improvement Partnership and the Centers for Disease Control and Prevention (Cooperative Agreement Number, DP006005). Contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention or the Department of Health & Human Services.
Supplement Note:
This article is part of the Health Promotion Practice supplement, “Tobacco and Health Equity: Interventions, Research, and Strategies to Address Tobacco Use Among Diverse Populations,” developed under the guidance of the Society for Public Health Education (SOPHE). SOPHE received funding from the Food and Drug Administration’s Office of Minority Health and Health Equity (Grant number HHSF223201820377A) to support printing and open access dissemination. The views and findings expressed in these manuscripts are those of the authors and do not imply endorsement or reflect the views and policies of the U.S. Government. The entire supplement issue is available open access at ![]() .
.