
Abstract
Background. The prevalence of e-cigarette use among youth is rising and may be associated with perceptions of health risks for these products. We examined how demographic factors and socioeconomic status (SES) are correlated with the perceived health risks of e-cigarette product contents among youth. Method. Data were from a national online survey of youth aged 13 to 18 between August and October 2017, weighted to be representative of the overall U.S. population in age, sex, race/ethnicity, and region. Survey analysis procedures were used. Results. Of 1,549 e-cigarette users and 1,451 never-e-cigarette users, 20.9% were Hispanic, 13.7% Black, 21.7% LGBTQ (lesbian/gay/bisexual/transgender/queer), and 49.3% in low-income families. With adjustment for e-cigarette use status, perceived health risks of nicotine and toxins/chemicals in e-cigarettes significantly differed by gender, race, sexual orientation, and SES (ps < .05). For example, adjusted odds of perceiving harm from nicotine were 60% higher in girls versus boys, 34% lower in non-Hispanic Blacks versus non-Hispanic Whites, 33% lower in urban versus suburban residents, 40% higher in LGBTQ versus straight-identifying individuals, and 28% lower in low-income versus high-income families. Lower parental education level also was associated with children’s lower health risk perception of e-cigarette product contents. Conclusions. For youth, the perceived health risks of e-cigarette product contents were associated with demographics, sexual orientation, and SES. The findings may have relevance for developing communication and education strategies addressing specific youth audiences, especially those in vulnerable groups. These strategies could improve awareness among youth concerning the health risks of e-cigarettes, helping to prevent or reduce e-cigarette uptake and continued use.
Introduction
Electronic cigarettes, also called e-cigarettes, e-cigs, vapes, or electronic nicotine delivery systems, are battery-operated devices that deliver an aerosol containing nicotine and other chemicals to users. Between 2008 and 2015, four countries (Poland, Korea, New Zealand, and the United States) saw the prevalence of current e-cigarette use among youth increase (Yoong et al., 2018). In fact, by 2018, over 3.6 million U.S. youth were current users of e-cigarettes (U.S. Food and Drug Administration, 2018). Although data are not yet available on the long-term health effects associated with e-cigarette use, available data indicate that short-term adverse effects are evident, and there are concerns regarding the possibility of more serious long-term consequences (Farsalinos et al., 2017; National Academies of Sciences, Engineering, and Medicine, 2018; Uchiyama, Ohta, Inaba, & Kunugita, 2013). The U.S. Surgeon General has concluded that e-cigarettes may contain harmful constituents, including nicotine and other toxins/chemicals, such as diacetyl, benzene, aldehydes, nickel, tin, and lead, with several delivered as ultrafine particles (U.S. Department of Health and Human Services, 2016). As we finalized this article, a number of e-cigarette-related lung problems, some resulting in death, were reported across the United States (Davidson et al., 2019; Layden et al., 2019). While investigations seek to uncover the cause of these lung diseases, reported incidents continue to rise, underscoring the fact that the risks of using e-cigarettes are not fully known. Public health experts caution the public on e-cigarette use and urge youth, young adults, pregnant women, and nontobacco users to refrain from using e-cigarettes (U.S. Department of Health and Human Services, 2019).
In addition to the potential direct health risks of e-cigarette use, studies have shown that youth who use e-cigarettes are more likely than nonusers to progress to combustible cigarette use (Klein, 2015; Lanza, Russell, & Braymiller, 2017; Primack, Soneji, Stoolmiller, Fine, & Sargent, 2015), the consequences of which are well established (U.S. Department of Health and Human Services, 2004). Therefore, the rapid increase in e-cigarette use, especially among adolescents/young adults over the past several years, is problematic and requires the attention of health care professionals as well as public health policy makers and planners (World Health Organization [WHO], 2014).
As perception of risk can play an important role in youth’s decisions to use e-cigarettes (Tsai et al., 2018), an abundance of research has focused on youth and their perceptions of health risks of e-cigarettes, typically comparing perceptions across e-cigarette use status, as well as relative to conventional cigarettes (Ambrose et al., 2014; Amrock, Lee, & Weitzman, 2016; Cooper, Harrell, Perez, Delk, & Perry, 2016; Volesky et al., 2016). These studies have reported that, compared with combustible cigarettes, youth perceive e-cigarettes as less harmful, cleaner, and less additive (Ambrose et al., 2014; Amrock et al., 2016; Cooper et al., 2016; Volesky et al., 2016). These studies also suggest that e-cigarette risk perceptions relative to conventional cigarette vary by gender, race/ethnicity, and education levels (Ambrose et al., 2014; Giovacchini, Pacek, McClernon, & Que, 2017; Volesky et al., 2016; Webb Hooper & Kolar, 2017). However, little work has examined health risk perceptions of e-cigarette product contents across key subgroups of youth, such as gender, race, ethnicity, socioeconomic status (SES), and sexual orientation. Moreover, while disparities in e-cigarette use have been found among sexual minority populations (Nayak, Salazar, Kota, & Pechacek, 2017), places of residence (Noland et al., 2018), and parental education levels (Thrasher et al., 2016), no disparities in health risk perceptions of e-cigarette product contents have been explored, especially in youth. Given the potential role of the health risk perceptions in teens’ decisions to use e-cigarettes, such a comparative analysis should help us understand the relative likelihood of use among adolescents, especially for various vulnerable subgroups.
In this study, we examined how disparities in demographic factors and SES and differences in sexual orientation might correlate with the perceived health risks of nicotine and toxins/chemicals in e-cigarettes among youth. In addition, e-cigarette use status was taken into account in our analysis, given that health risk perceptions vary by e-cigarette use and cigarette smoking status, where e-cigarette users are likely to perceive e-cigarettes as less harmful than cigarettes (Ambrose et al., 2014). Findings from our study may have relevance for developing communication and education strategies addressing specific youth audiences, thereby helping to prevent or reduce e-cigarette uptake and continued use.
Method
Study Sample
Between August and October 2017, an established marketing research vendor specializing in youth conducted an online survey on behalf of the American Heart Association Tobacco Regulation and Addiction Center, recruiting 3,174 U.S. youth aged 13 to 18 years. Two groups, e-cigarette users, defined as youth who have ever tried any e-cigarette product, and never-e-cigarette users, were recruited. Non-Hispanic Blacks and Hispanics were oversampled to ensure sufficient sample sizes for comparison by race and ethnicity. The data were weighted to be representative of the overall U.S. population in terms of age, sex, race, ethnicity, and region.
Procedures for obtaining proper online consent were implemented. No identifying information was collected, and guidelines established by the Children’s Online Privacy Protection Act were followed. Youth participants were given assent forms and could elect not to participate. Parental consent was obtained for teen panelists younger than 18. The study team had no direct contact with recruited individuals. The Chesapeake/Advarra Institutional Review Board reviewed and approved this study.
Measurements
Demographic and Socioeconomic Variables
Participants were categorized by age-group (13-14, 15-16, and 17-18), sex (girls or boys), race/ethnicity (Hispanic, non-Hispanic White, non-Hispanic Black, and non-Hispanic other racial groups including more than one race, Asian or Pacific Islander, or unspecified race), and place of residence (urban, suburban, or rural). Household income status was categorized as low versus high, with low-income status defined as the respondent participating in a free/reduced-cost lunch program at school or family receiving government public assistance (Medicaid, Section 8 housing, Obama phone, food stamps, the link card/SNAP [Supplemental Nutrition Assistance Program], or other government financial help; U.S. Government, n.d.). Parent education levels (years in school) were categorized as low versus high, with low education levels defined as none of the parents graduating with an associate degree or higher.
In addition, participants were asked to indicate their sexual orientation, and were classified as straight or lesbian/gay/bisexual/transgender/queer (LGBTQ).
E-Cigarette and Other Tobacco Product Use Status
As previously mentioned, two groups were recruited and categorized according to never use of e-cigarettes or ever use of e-cigarettes. The ever use group was subcategorized: current e-cigarette-only users, current dual/poly e-cigarette users (e-cigarettes plus one or more other tobacco products), and former e-cigarette users (ever e-cigarette use but not in the past 30 days, regardless of any current other tobacco product use). The definitions of ever or current e-cigarette use have been described in previous publications (Ma et al., 2019; Vu et al., 2019) and were based on the definitions from the Population Assessment of Tobacco and Health Study (Rodu & Plurphanswat, 2018). In short, if participants had ever used an e-cigarette, they were included in the ever use group. Participants were considered current users of e-cigarettes if they reported using the product(s) within the past 30 days.
Other tobacco products addressed included traditional cigarettes, traditional cigars, little or filtered cigars, cigarillos, smokeless tobacco, dissolvable tobacco products, hookahs to smoke tobacco, bidis, and kreteks. The definition of current other tobacco product use was based on the past 30 days.
To decrease confusion about the products, photos and descriptions of e-cigarette and other tobacco/nicotine products were provided in the questionnaire.
Perceived Health Risks of Nicotine or Toxins/Chemicals in E-Cigarettes
Participants were asked, “In what ways might electronic nicotine products be dangerous?” with 13 response options, and they could choose all that applied. However, for the purpose of this analysis, only two options related to the health risks of the contents of e-cigarettes (nicotine; toxins/chemicals) were selected: (1) nicotine might cause health problems (yes vs. no) and (2) toxins/chemicals in the e-liquid might cause health problems (yes vs. no).
Statistical Analysis
All descriptive measures (means, proportions) and effect estimates (beta coefficients, prevalence ratios) were weighted to adjust for sampling probability. Descriptive statistics were conducted for the entire sample and stratified by e-cigarette use status. Rao–Scott chi-square tests were used for categorical variables to compare differences in proportions across e-cigarette use status. Pairwise comparisons were made between individuals in the never use e-cigarette category (reference) and the other three categories using chi-square tests with Bonferroni adjustment for multiple testing.
In multivariable analyses, logistic regression models were used to estimate the odds ratios of perceived health risks of nicotine and toxins/chemicals in e-liquid contents by demographic, SES, and sexual orientation categories.
All statistical tests were two-sided at a significance level of .05. Statistical analyses were carried out with survey procedures using SAS statistical software (Version 9.4 with SAS/STAT 14.1, SAS Institute Inc., Cary, NC).
Results
As shown in Table 1, 3,000 participants (1,549 e-cigarette users and 1,451 never-e-cigarette users) ages 13 to 18 were included in the analytic sample. Among them, 55.6% were female; 7.3% (n = 219) were current e-cigarette–only users, 10.8% (n = 323) were dual-/polyproduct users, 34.6% (n = 1,007) were former e-cigarette users, and 48.4% had never used e-cigarettes; 20.9% were Hispanic, 13.7 % were non-Hispanic Black; and 49.4% were in low-income households. Among the e-cigarette use status groups, the group never having used e-cigarettes had a significantly higher proportion in the 13 to 14 age group (38.2% vs. 13.2%, 10.6%, and 15.4% with ps for pairwise comparisons <.05), whereas this group had a significantly lower proportion of non-Hispanic Whites compared to the group of current e-cigarette only users (55.2% vs. 69.8%, with p for pairwise comparison <.05). The groups of current dual/poly users and former e-cigarette users had a higher proportion of youth from low-income households or low-educated parents (e.g., 68.2% of current dual/poly users and 49.6% of never users had low-educated parents).
Characteristics of Study Sample, Overall and by E-Cigarette Use Status
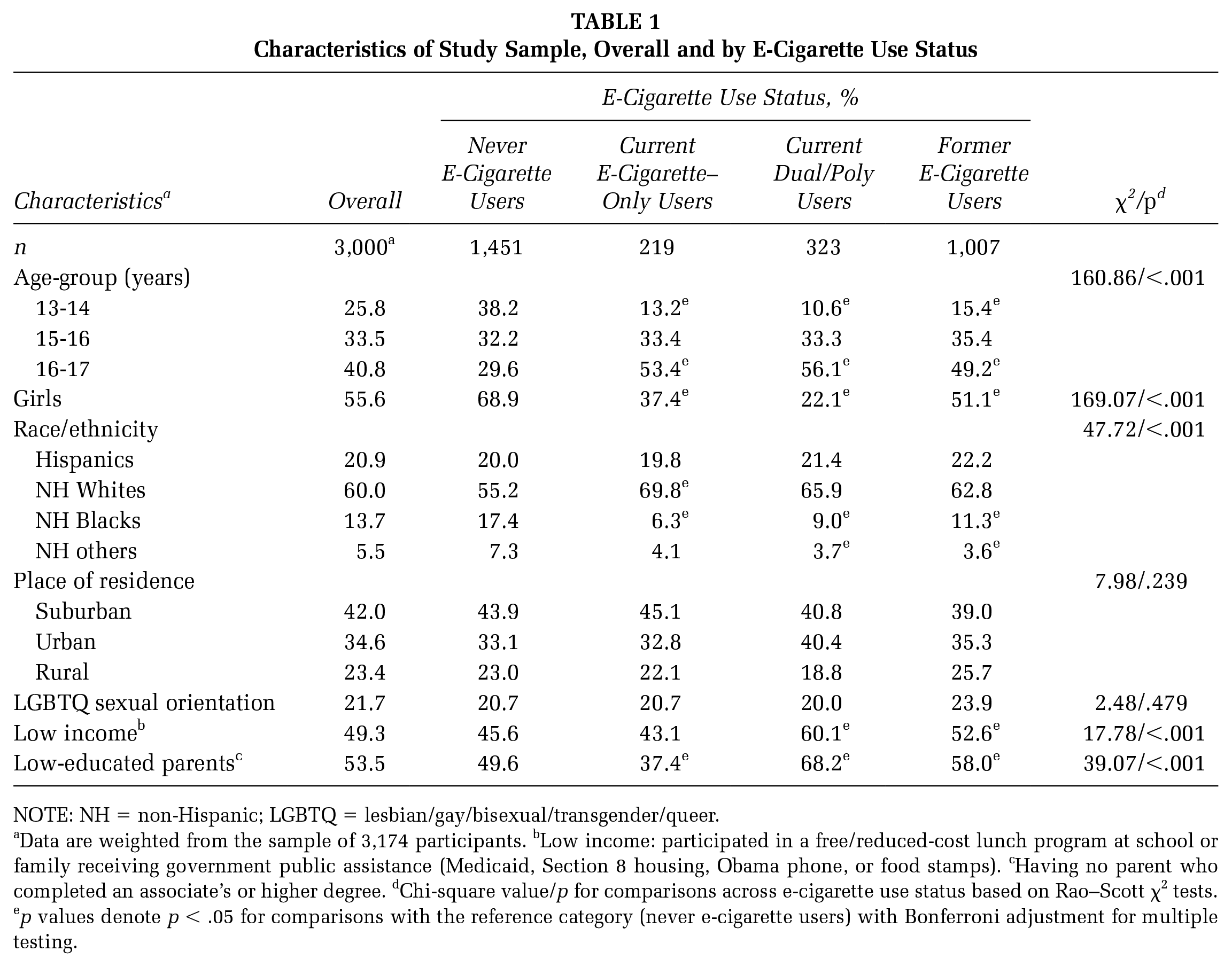
NOTE: NH = non-Hispanic; LGBTQ = lesbian/gay/bisexual/transgender/queer.
Data are weighted from the sample of 3,174 participants. bLow income: participated in a free/reduced-cost lunch program at school or family receiving government public assistance (Medicaid, Section 8 housing, Obama phone, or food stamps). cHaving no parent who completed an associate’s or higher degree. dChi-square value/p for comparisons across e-cigarette use status based on Rao–Scott χ2 tests. ep values denote p < .05 for comparisons with the reference category (never e-cigarette users) with Bonferroni adjustment for multiple testing.
The perceived health risks of nicotine and the toxins/chemicals in e-cigarettes, overall and by e-cigarette use status, are shown in Figure 1. About 60% of the participants perceived that nicotine or toxins/chemicals in e-liquids might cause health problems. As expected, the proportion of participants perceiving possible health risks with either nicotine or toxins/chemicals in e-cigarettes strongly differed by e-cigarette use status (ps < .001), with the highest proportion observed in the never-e-cigarette-users group compared to other e-cigarette use status groups (ps for pairwise comparisons <.05).
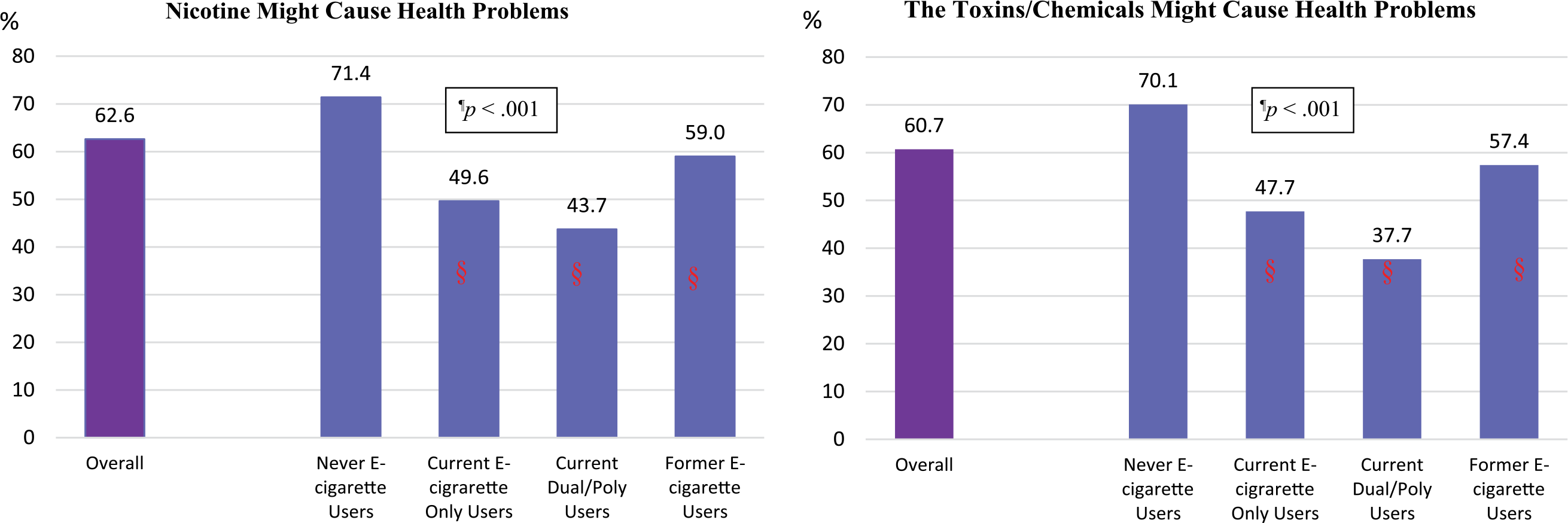
Perceived Health Risks of Nicotine and Toxins/Chemicals in E-Cigarettes
In multivariable regression models, perceived health risks of nicotine or toxins/chemicals in e-cigarettes also significantly differed by gender, race, sexual orientation, and SES regardless of e-cigarette use status (Figures 2 and 3).
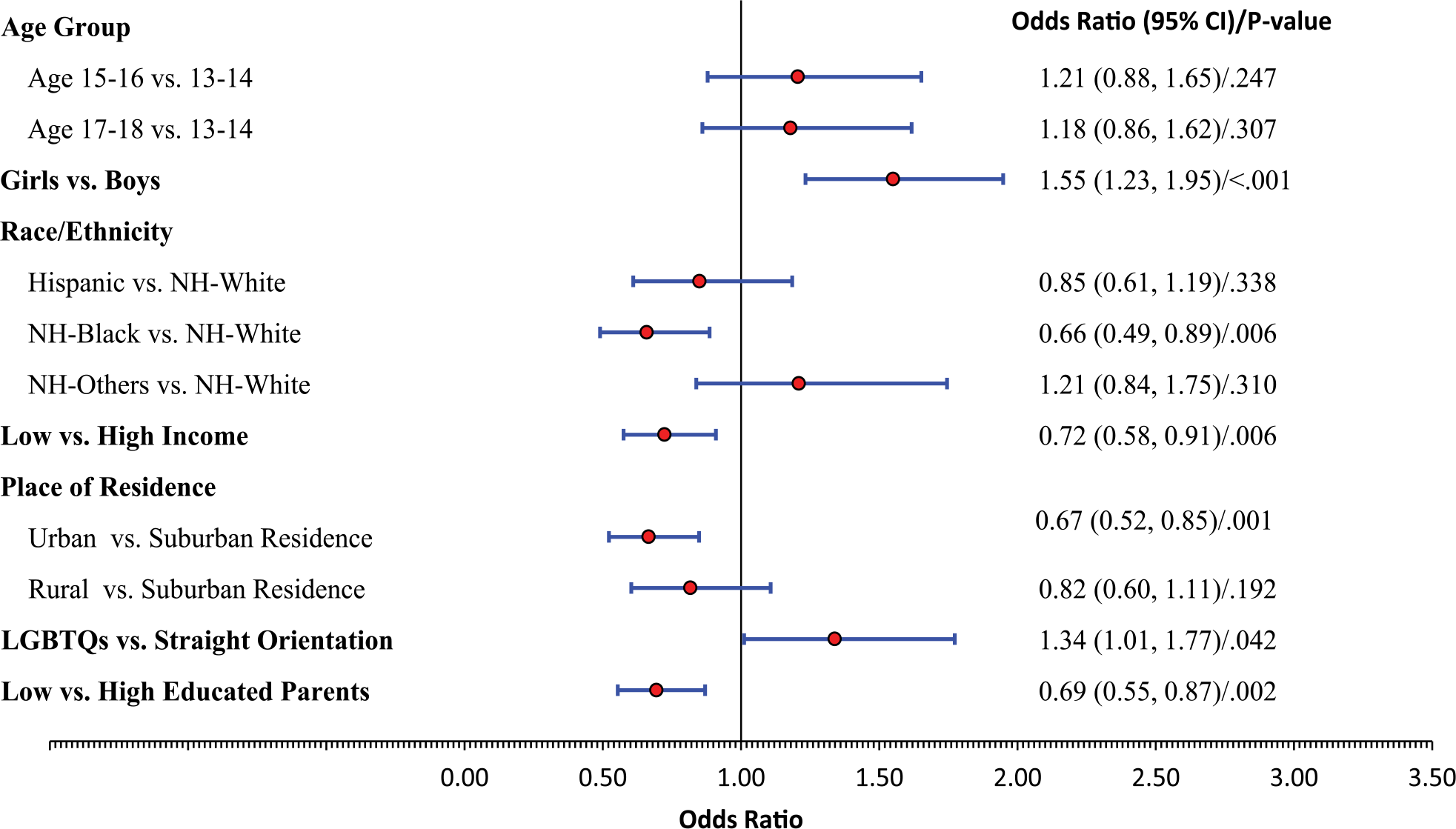
Odds Ratiosa and 95% Confidence Intervals (CIs) of Perceived Health Risks of Nicotine in E-Cigarettes
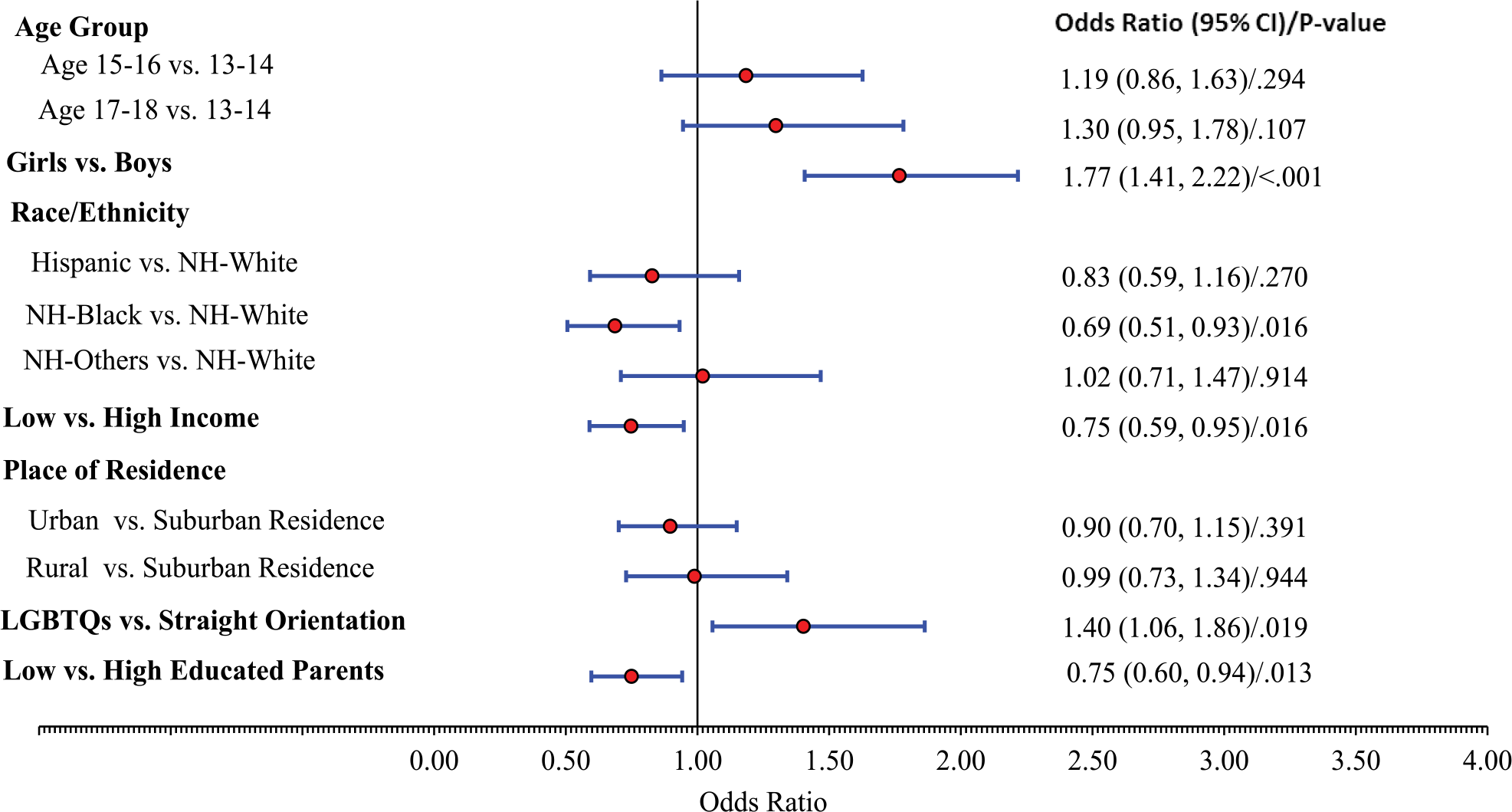
Odds Ratiosa and 95% Confidence Intervals (CIs) of Perceived Health Risks of Toxins/Chemicals in E-Cigarettes
For example, adjusted odds [95% confidence interval] of perceiving harm from nicotine were 1.55 [1.23, 1.95] in girls versus boys, 0.66 [0.49, 0.89] in non-Hispanic Blacks versus non-Hispanic Whites, 0.67 [0.52, 0.85] in urban versus suburban residents, 1.34 [1.01, 1.77] in LGBTQ versus straight-identifying individuals, 0.72 [0.58, 0.91] in low-income versus high-income families, and 0.69 [0.55, 0.87] in low-educated parents versus high-educated parents. Similar results were observed in the perceived health risks of toxins or chemicals in e-cigarettes.
Discussion
Our study examined a national sample of 1,549 e-cigarette users and 1,451 never-e-cigarette users, aged 13 to 18 with diverse demographic and socioeconomic backgrounds and sexual orientations. We found that the perceived health risks of nicotine or toxins/chemicals in e-cigarettes were highest in the never-e-cigarette-users group and lowest in the group of dual/poly users. Perceived health risks also significantly differed by gender, race, sexual orientation, and SES, regardless of the participants’ e-cigarette use status. Girls and LGBTQ individuals were more likely to perceive health risks from nicotine or toxins/chemicals in e-cigarettes compared to their counterparts. Participants classified as lower SES, non-Hispanic Blacks, from low-income families, or urban residents were less likely to perceive health risks of nicotine or toxins/chemicals in e-cigarettes. Lower parental educational achievement also was associated with lower perceptions of health risk from e-cigarettes among youth.
Prior research regarding youth perceptions of e-cigarette health risks has emphasized health-risk perceptions of e-cigarettes relative to conventional cigarettes across e-cigarette use status and found that e-cigarette risk perceptions relative to conventional cigarettes vary by sociodemographic characteristics among youth (Ambrose et al., 2014; Amrock et al., 2016; Giovacchini et al., 2017; Webb Hooper & Kolar, 2017). The relationship between sociodemographic characteristics and perceived health risks of e-cigarettes and their contents remains generally unexplored. Our study is among the first to address how different groups of youth, especially vulnerable groups, perceive the health risks of e-cigarette contents. With the serious vaping-related incidents of illness impacting both youth and adults across the country since summer 2019 (U.S. Department of Health and Human Services, 2019), our findings provide timely insights into a growing national health issue. Different groups may be more aware of, pay more attention to, and process information related to these illnesses and deaths differently. Understanding those differences will help in tailoring public health messaging and recommendations to health care providers and thereby influence how youth perceive the health risks of e-cigarettes, and subsequently perhaps their use.
Our findings that sex and race were associated with perceived health risks of e-cigarette contents are consistent with findings from previous studies. For example, Ambrose et al. (2014) analyzed data from 24,658 participants from the 2012 National Youth Tobacco Survey (NYTS) and found that female and Hispanic participants perceived e-cigarettes as more harmful than cigarettes compared to male and White participants. Our finding that youth from low-income families and with parents with limited education were less likely to perceive health risks from e-cigarette product contents also is consistent with findings such as those of Thrasher et al. (2016), observing that children whose parents had higher educational levels had higher awareness of e-cigarette products than those whose parents had lower educational levels. Place of residence was found to be associated with e-cigarette use in children as shown in the NYTS data, where among current cigarette smokers, urban youth were 86% more likely than rural youth to use e-cigarettes (Noland et al., 2018). Our finding that urban residents were less likely to perceive health risks of nicotine or toxins/chemicals in e-cigarettes than suburban residents may help explain the findings from NYTS. Finally, although prior studies found no difference in harm perception of e-cigarettes by sexual orientation in U.S. adults (Nayak et al., 2017), teens in our study who reported identifying as LGBTQ had a higher perception of the health risks of e-cigarette product contents. This is an unexpected finding, as the LGBTQ group has higher e-cigarette prevalence (Huang, Kim, Vera, & Emery, 2016).
Limitations
This study has several limitations. Because the investigation employed an online panel of participants, it is possible that their perceptions may differ from individuals without Internet access or recruited in person. Also, the data were cross-sectional, limiting the nature of our analyses. Furthermore, consistent with similar studies, self-reported data could be subject to potential recall and reporting biases. Despite these concerns, the use of such survey data has been validated in previous studies and is viewed as yielding valuable findings (Harrell, Loukas, Jackson, Marti, & Perry, 2017).
Conclusion and Implications
In conclusion, our findings demonstrate that for youth, the perceived health risks of e-cigarette product contents (nicotine and toxins/chemicals) were associated with sex, sexual orientation, household income, parent education status, and urban setting. The perceptions of e-cigarette harm were low in specific groups (e.g., male adolescents, non-Hispanic Blacks, residents of urban areas, and families with low SES and low-educated parents). The association provides insights into vulnerable populations on these issues. Communication strategies should address specific audiences, especially those in vulnerable subgroups, regardless of e-cigarette use status. Additionally, there is evidence that adults who work closely with youth (e.g., teachers and school administrators) are underinformed about e-cigarette products (Schillo et al., 2020). Health messaging should be designed not only for parents/guardians but also for other adults working closely with youth, such as teachers and coaches. Increased understanding of e-cigarette products and their health consequences may help prevent e-cigarette uptake or continued use among youth.
Our findings also support the Food and Drug Administration strategic research priority on public education with a focus on vulnerable groups as well as the WHO Framework Convention on Tobacco Control recommendation on regulations to improve awareness concerning the health effects of e-cigarettes to impede e-cigarette promotion and prevent uptake by youth, minimize potential health risks to e-cigarette users and nonusers, and prohibit unproven health claims from being made about e-cigarettes (WHO, 2014). These insights also support the need for continued monitoring of e-cigarette manufacturer advertising and promotion, particularly in low-income and urban settings.
Footnotes
Authors’ Note:
This research was supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health (NIH) and the Food & Drug Administration (FDA) Center for Tobacco Products under Award Nos. P50HL120163 and U54HL120163. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH, the FDA, or the American Heart Association. The authors have no other disclosures.
Supplement Note:
This article is part of the Health Promotion Practice supplement, “Tobacco and Health Equity: Interventions, Research, and Strategies to Address Tobacco Use Among Diverse Populations,” developed under the guidance of the Society for Public Health Education (SOPHE). SOPHE received funding from the Food and Drug Administration’s Office of Minority Health and Health Equity (Grant number HHSF223201820377A) to support printing and open access dissemination. The views and findings expressed in these manuscripts are those of the authors and do not imply endorsement or reflect the views and policies of the U.S. Government. The entire supplement issue is available open access at ![]() .
.