
Abstract
Food insecurity is a significant public health problem in the United States leading to substantial social, economic, and health care–related burdens. While studies continue to estimate the prevalence of food insecurity, the long-term outcomes are not extensively explored. The purpose of this study was to assess the impact of food insecurity on mortality. We analyzed data on adults (≥ 20 years) from the 1999–2010 National Health and Nutrition Examination Survey, with mortality data obtained through 2015. Among the total study participants (n = 25,247), 17.6% reported food insecurity. Food-insecure individuals were more likely to be younger in age, minorities, poorer, with lesser education, obese, smokers, and with diabetes compared to food-secure counterparts. During a 10.2-year follow-up, among the food insecure, 821 individuals died (11%). The hazard ratio (HR) for mortality among the food insecure compared with the food secure, with adjustment for age and gender only, was 1.58; 95% confidence interval [CI: 1.25, 2.01]. The adjusted HRs for all-cause mortality, HR = 1.46, CI [1.23, 1.72], p < .001, and cardiovascular mortality, HR = 1.75, CI [1.19, 2.57], p < .01, were statistically significantly higher among food-insecure individuals, after adjustment for multiple demographic and health risk factors. Individuals who are food-insecure have a significantly higher probability of death from any cause or cardiovascular disease in long-term follow-up. Comprehensive and interdisciplinary approaches to reducing food insecurity–related disparities and health risks should be implemented. Including food insecurity in health risk assessments and addressing food insecurity as a determinant of long-term outcomes may contribute to lower premature death rates.
Background
Food insecurity, a complex and serious public health problem, is associated with lack of dietary diversity and can affect health through malnourishment, undernutrition, or overnutrition (Coleman-Jensen et al., 2019; Cook et al., 2013; Crawford & Webb, 2011; Hendriks, 2016). Food security can be defined as “assured access at all times to enough food for an active, healthy life” (U.S. Department of Agriculture [USDA], 2019). As per this definition, more than a tenth of the U.S. population is food insecure every year. A total of 14.3 million households experienced food insecurity at some point in 2018, and food insecurity is still above the prerecession rates of 2007 (Oliveira, 2019). Furthermore, the levels of individuals remaining in the category of very low food security, characterized by hunger, remained unchanged since the previous year. Prevalence rates may differ by race, gender, age, and a variety of other sociodemographic indicators, with the most vulnerable groups being children, the elderly, and racial and ethnic minorities. For example, food insecurity is typically associated with lower socioeconomic status in American households. Poverty is strongly associated with food insecurity in American adults who tend to have lower quantity and quality of food intake (Coleman-Jensen et al., 2019; Cook et al., 2013). However, some individuals of higher socioeconomic status are also susceptible to food insecurity during economic downturns or in instances where there is loss of employment or life of a head of household. Consequently, food insecurity remains a dynamic challenge that must be assessed in the context of a variety of individual, household, and community characteristics (Birkenmaier et al., 2016; Coleman-Jensen et al., 2019; Cook et al., 2013; Hendriks, 2016; Myers & Painter, 2017; Oliveira, 2019; USDA, 2019). While the concepts of food insecurity and hunger are interrelated, sometimes food insecurity can be considered a precursor to hunger, which is a more well-defined concept.
Food insecurity is typically associated with lower socioeconomic status and is a dynamic and cyclic condition. Poverty is one of the risk factors for food insecurity in that food-insecure individuals tend to have lower quantity and quality of food intake (S. Banerjee & Radak, 2019; Berkowitz et al., 2018; Froissart et al., 2005; Levey et al., 2015; USDA, 2018). However, some individuals of higher socioeconomic status are also susceptible to food insecurity. For instance, sometimes an economic downturn or death of a sole breadwinner may lead to bouts of food insecurity. Consequently, food insecurity should be assessed even after controlling for socioeconomic status.
Mortality outcomes are especially important to assess since this is a concrete metric of the specific effect of food insecurity. There are multiple mechanisms, like poor nutrition, through which food insecurity may be connected with mortality. Multiple researchers have demonstrated the connection and impact of food insecurity on nutrient intake, as it relates to health (Birkenmaier et al., 2016; Myers & Painter, 2017). More specifically, the leading causes of death in the United States (i.e., cardiovascular disease [CVD], cancer, and stroke) are associated with unhealthy diet, and conversely, specific disease conditions are predictive of food insecurity (Birkenmaier et al., 2016; USDA, 2019). Also, it has been well established that poor nutrition can negatively affect physical and mental health, leading to a variety of chronic diseases. Without proper nourishment, people experience poor wound healing, more infections, more comorbidities, reduced quality of life, and longer lengths of stay in the hospital (T. Banerjee et al., 2017; Berkowitz et al., 2017; Men et al., 2019; Wang et al., 2011). For these reasons, food insecurity leads to higher health care costs (Men et al., 2019).
Although the connections between poverty, social determinants of health, hunger, and poor health are well known, there is a paucity of research regarding the connection between food insecurity and long-term mortality outcomes. In this study, we explored the long-term connections between food insecurity and all-cause and cardiovascular-related mortality. Furthermore, we assessed if after controlling for cardiovascular conditions like heart failure food insecurity individually or independently leads to increased 10-year CVD mortality. Furthermore, we applied the World Health Organization’s Commission on Social Determinants of Health (CSDH; 2008) theoretical framework to guide our study.
Method
Study Participants
We used data from the National Health and Nutrition Examination Survey (NHANES), six cycles between 1999 and 2010 (Centers for Disease Control and Prevention [CDC], 2020). Every year approximately 5,000 infants, children, and adults from the United States are selected to participate in the NHANES. Survey participants are asked to complete the in-person household interview by completing an interviewer-administered questionnaire. Next, the health examination components of the survey are administered in Mobile Examination Centers throughout the United States. The laboratory component of the health examination includes an extensive array of laboratory tests that are performed on blood, urine, and other types of specimens. Sample weights were derived to account for oversampling of young children, adults 60 years of age and older, non-Hispanic Black individuals, and individuals of Mexican American ethnic origin in the NHANES survey. The analysis sample is representative of noninstitutionalized U.S. adults 20 years and older, to restrict the analysis to adults. The procedures and protocols for NHANES are approved by the National Center for Health Statistics before data collection. Data are available for public use through the CDC website. We received additional ethical approval through the Walden University Institutional Review Board for data analysis using publicly available files.
Measures
All-Cause Mortality
Vital status was determined using the Continuous NHANES Public-Use Linked Mortality File, which provides vital status follow-up data in person—months from the date of NHANES survey participation through the date of death or December 31, 2015. Mortality was ascertained by the National Centers for Health Statistics (NCHS) through a probabilistic match between NHANES participants and National Death Index (NDI) death certificate records. This probabilistic match approach is a modification of the probabilistic match approaches developed by Fellegi and Sunter (1969) and Rogot et al. (1986). Each NDI possible match record is assigned a probabilistic match score. The probabilistic match score is the sum of the weights assigned to each of the identifying data items used in the NDI record match, where the weights reflect the degree of agreement between the information on the submission record and the NDI death record. Participants who were not matched with death records were considered to be alive through the follow-up period.
Cardiovascular Mortality
Cause of death was assigned by the NCHS based on the International Classification of Diseases, 10th revision. For this study, cardiovascular mortality was defined as death due to diseases of the heart, essential hypertension and hypertensive kidney disease, cerebrovascular disease, atherosclerosis, and/or other diseases/disorders of the circulatory system (Codes I00–I99; S. Banerjee & Radak, 2019; CDC, 2020; NCHS, 2020).
Food Insecurity
The USDA developed the Household Food Security Survey Module (HFSSM), a well-validated questionnaire, in order to measure household food security over the prior 12 months (S. Banerjee & Radak, 2019; Berkowitz et al., 2018; USDA, 2018). In our study, we focused only on adult health outcomes and therefore used responses to only the 10 household and adult items in the 18-item scale. The rest of the responses were not applicable to adults. In the HFSSM, more than 99% of the eligible sample participated. We ran analysis with food insecurity classified as four categories—food secure, marginally food secure, low food secure, and very low food secure. Next, we dichotomized the HFSSM responses using validated cut points. The respondent was deemed food secure if no items in the scale were answered affirmatively. Those referred to as marginal food security, low, and very low food security or if ≥1 item(s) were answered affirmatively were deemed to be in a state of food insecurity (S. Banerjee & Radak, 2019; CDC, 2020; NCHS, 2020). We ran sensitivity analysis and found that results were robust across the successive models when food insecurity was determined through two- or four-category classification systems.
Chronic Disease Covariates
Various chronic diseases were assessed as covariates. Preexisting CVD was determined from the in-person interview conducted by trained personnel. The presence of CVD was determined by the presence of coronary heart disease, angina, stroke, congestive heart failure, or heart attack. All respondents over the age of 20 years were asked, “Other than during pregnancy, have you ever been told by a doctor or other health professional that you have diabetes or sugar diabetes?” For the purposes of this study, the participants who answered “borderline” or “yes” were considered as having diabetes. However, those participants who answered “no” were considered as nondiabetic (S. Banerjee & Radak, 2019; Berkowitz et al., 2018; CDC, 2020).
We included chronic kidney disease (CKD) as a covariate due to previous studies demonstrating the connection between CKD and food insecurity (T. Banerjee et al., 2017). Specifically, we determined CKD by using glomerular filtration rate (GFR). GFR was derived from the Cockcroft-Gault equation (S. Banerjee & Radak, 2019; Froissart et al., 2005). Even though, technically, a GFR less than 90 ml/min per 1.73 m2 is considered CKD, the high number from advanced age places most people in this age-group in either Stage I or Stage II CKD. Therefore, in ascertaining the presence of CKD, individuals had to have a GFR of less than 60 ml/min per 1.73 m2 or a urine albumin-to-creatinine ratio of less than 30 as previously validated (Levey et al., 2015).
Finally, obesity data were subdivided into four categories according to body mass index (BMI) derived from physically assessed height and weight measurements in mobile examination centers. The categories were as follows: Participants with BMI < 25 were considered normal weight; participants with BMI = 25 to 29 were overweight; participants with BMI = 30 to 39.9 were considered obese; and participants with BMI > 40 were considered severely obese. For the multivariate models, obesity was dichotomized and considered present for BMI ≥ 30 and considered absent for the rest (S. Banerjee & Radak, 2019; Berkowitz et al., 2018; CDC, 2020).
Demographic Covariates
Demographic and health behaviors were also assessed as covariates. Age and gender information was collected at the in-person interview. Smoking data were subdivided into a trichotomous indicator as a smoker versus former smoker versus never smoker. Smoking status was determined by asking the questions “Have you smoked at least 100 cigarettes in your entire life?” and “Do you now smoke cigarettes?” Those individuals who answered “yes” to the first question and “not at all” to the second were considered “former smoker”; individuals who answered “yes” to both questions were considered “current smoker”; and individuals who answered “not at all” to both questions were categorized as “never smokers.” The education-level data were subdivided into a trichotomous indicator as “completing some high school” versus “high school graduate” versus “some college or above.” To ascertain the race/ethnicity of the subjects, the interviewer asked, “What race do you consider yourself to be?” Within the NHANES questionnaire, respondents were allowed to select one of four categories. The different categories were coded as follows: non-Hispanic White, non-Hispanic Black, Hispanic, and Other. For socioeconomic status, an individual was considered to be below poverty threshold when poverty–income ratio (PIR) was less than 1. This is equivalent to less than 100% of the federal poverty level. PIR greater than or equal to 1 was considered above poverty threshold.
Statistical Analysis
A Cox proportional hazards model was used to calculate hazard ratios (HRs) and 95% confidence intervals (CIs) to determine whether food insecurity is a risk factor for all-cause and cardiovascular mortality. We adjusted all primary models for demographic and medical variables with a set of a priori covariates, which are potential confounders for overall mortality or CVD mortality. Furthermore, in the analysis, we weighted demographic and medical variables to approximate distributions in the United States by using the provided sample weights, which accounted for the unequal probabilities of selection and nonresponse. Also, we estimated the main effects and the interaction term to interpret the interaction of dichotomized food insecurity and smoking status. The reason this interaction term was assessed is because food insecurity was found to be associated with smoking status in previous studies (Armour et al., 2008). Statistical analyses were conducted using the SAS System for Windows (Release 9.1; SAS Institute Inc., Cary, NC) and SUDAAN (Release 9.0; Research Triangle Institute, Research Triangle Park, NC). All variance calculations incorporated the sample weights and accounted for the complex samples design using Taylor series linearization. All significance tests were two-sided using p < .05 as the level of statistical significance.
Results
Demographic Characteristics
A total of 25,247 study participants aged 20 years or older were included for analysis in this study. Table 1 provides the data for the distribution of the demographic characteristics, health behaviors, and chronic diseases among the study participants stratified by food insecurity status using bivariate analysis. The weighted prevalence of food insecurity in the U.S. population within the 20 years or older age-group was 17.6% (n = 6,086), 95% CI [16.6, 18.5], which is representative of 29,528,519 individuals in the total U.S. population. The average age of the participants within the sample was 46.5 years (SE ± 0.22) with statistically significant difference between individuals with food insecurity versus those with food security (41.1 years vs. 47.7 years, p < .001), where individuals with food insecurity were younger in age. There were statistically significant differences between individuals with food security and food insecurity based on gender, race/ethnicity, education level, PIR, smoking status, obesity status, and chronic diseases. Among the individuals with food insecurity, participants were more likely to be non-Whites (46.6%), with less than high school diploma (40.1%), poor (39% as defined by PIR), current smokers (37.8%), and people with diabetes (10.4%), compared to their counterparts who did not report food insecurity and were considered food secure (more likely to be Whites, with higher education, and less likely to be poor, be obese, have positive smoking status, or be people with diabetes).
Characteristics of Study Participants Stratified by Food Insecurity a
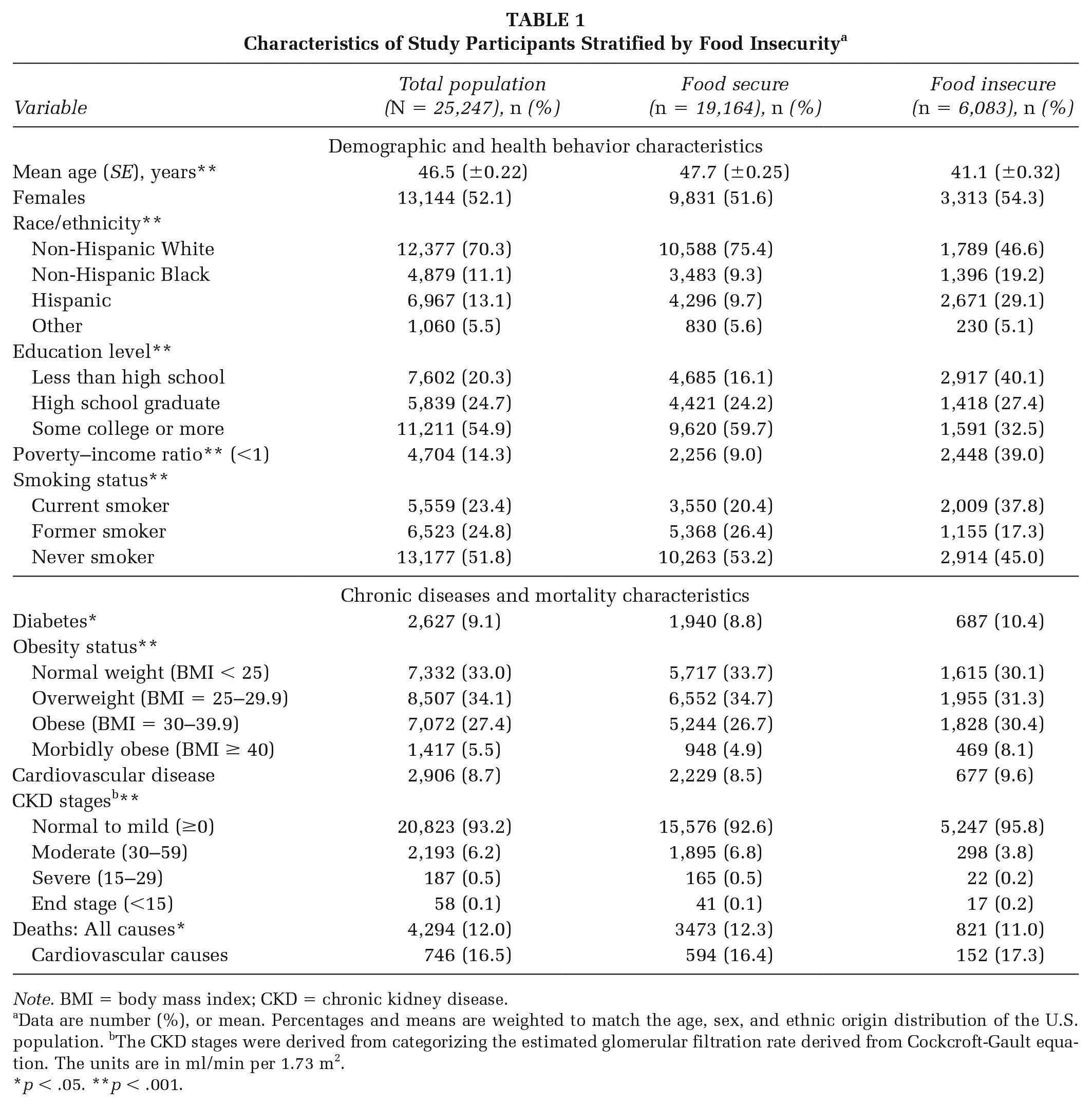
Note. BMI = body mass index; CKD = chronic kidney disease.
Data are number (%), or mean. Percentages and means are weighted to match the age, sex, and ethnic origin distribution of the U.S. population. bThe CKD stages were derived from categorizing the estimated glomerular filtration rate derived from Cockcroft-Gault equation. The units are in ml/min per 1.73 m2.
p < .05. **p < .001.
Mortality
Out of 6,086 participants (54% females vs. 46% males) with food insecurity, 821 died (11% of the food-insecure population vs. 12.3% of the food-secure population, p = .02) during an average of 10.2 years of follow-up. This included 152 deaths due to CVD (17.3% of all deaths among food insecure). The HR for age- and gender-adjusted mortality among individuals with food insecurity compared with individuals with food security was 1.58, 95% CI [1.25, 2.01], indicating a 58% higher probability of death.
The adjusted HR for all-cause mortality, 1.46, 95% CI [1.23, 1.72], p < .001, was statistically significantly higher among individuals with food insecurity after additional adjustment for demographic (age, gender, ethnicity, and PIR) and health risk factors (diabetes, CKD, CVD, and obesity), as seen in Table 2, indicating a 46% higher probability of mortality among individuals with food insecurity. Similarly, the adjusted HRs for cardiovascular mortality, 1.75, CI [1.19, 2.57], p < .01, remained statistically significantly higher among food insecure after adjustment for age, gender, ethnicity, PIR, diabetes, CKD, preexisting CVD, and obesity (Table 3), indicating a 75% higher probability of CVD-related mortality among individuals with food insecurity. When interpreting the interaction of dichotomized food insecurity and smoking and adjusting for potential confounders, there was no significance (p = .71).
Food Insecurity and Its Association With All-Cause Mortality
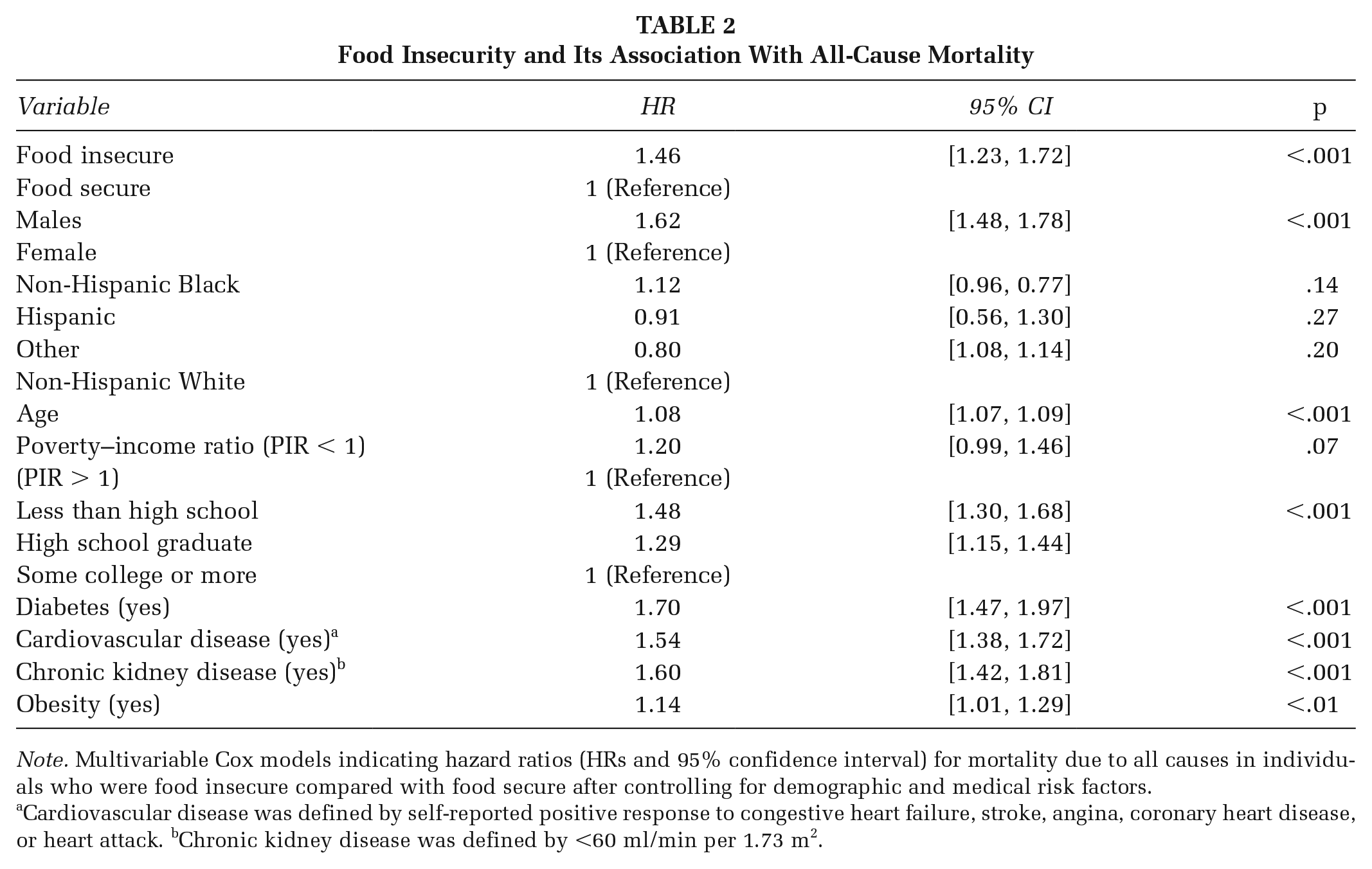
Note. Multivariable Cox models indicating hazard ratios (HRs and 95% confidence interval) for mortality due to all causes in individuals who were food insecure compared with food secure after controlling for demographic and medical risk factors.
Cardiovascular disease was defined by self-reported positive response to congestive heart failure, stroke, angina, coronary heart disease, or heart attack. bChronic kidney disease was defined by <60 ml/min per 1.73 m2.
Food Insecurity and Its Association With Cardiovascular Disease Mortality
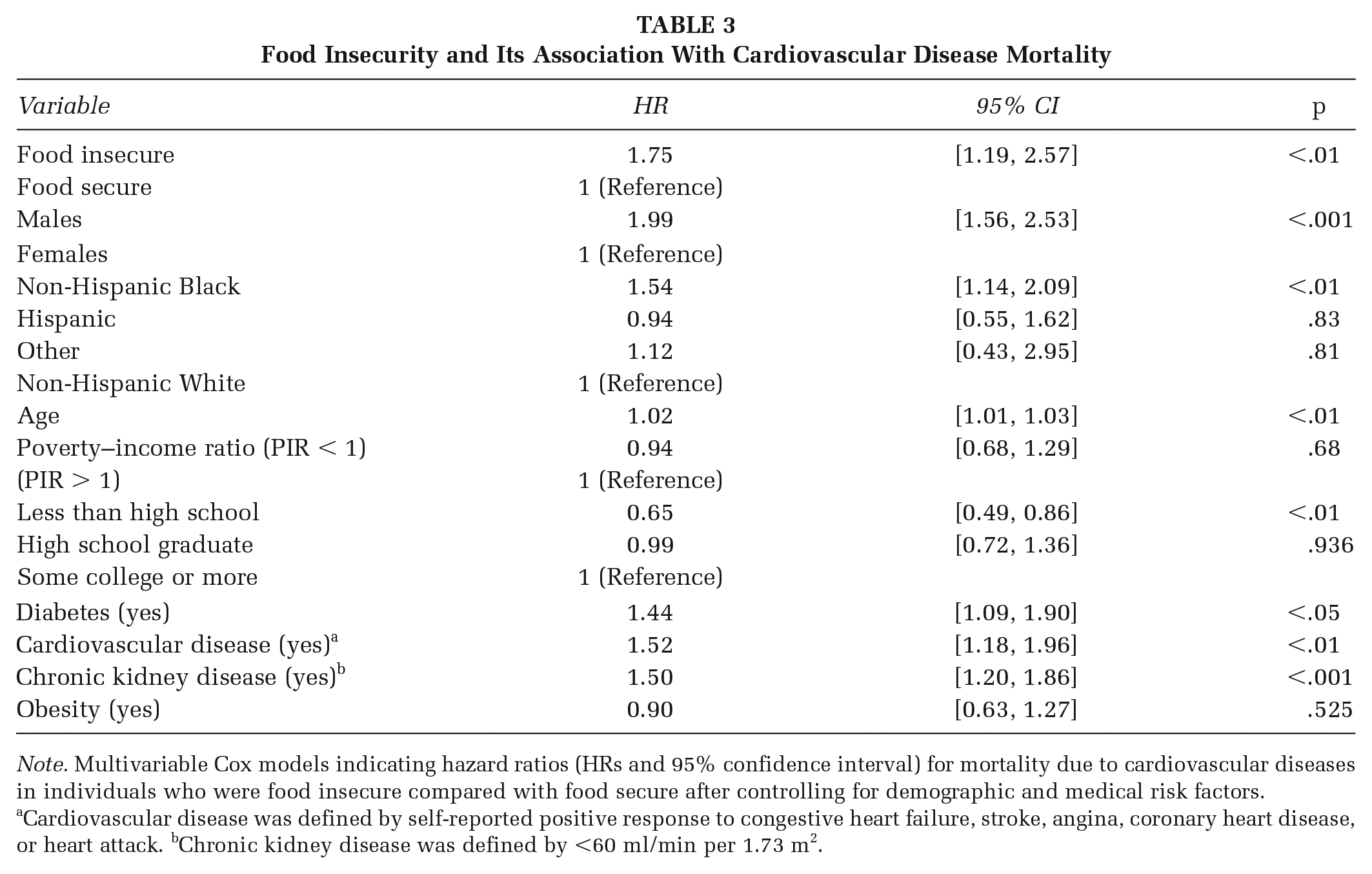
Note. Multivariable Cox models indicating hazard ratios (HRs and 95% confidence interval) for mortality due to cardiovascular diseases in individuals who were food insecure compared with food secure after controlling for demographic and medical risk factors.
Cardiovascular disease was defined by self-reported positive response to congestive heart failure, stroke, angina, coronary heart disease, or heart attack. bChronic kidney disease was defined by <60 ml/min per 1.73 m2.
When food security was stratified into four categories, there was a statistically significant increased risk of all-cause and CVD mortality as well. Adults in households with marginal, low, and very low food security had statistically significantly higher risk of experiencing all-cause mortality than adults in households with full food security, marginal: HR = 1.45, 95% CI [1.16, 1.80]; low: HR = 1.56, CI [1.29, 1.89]; and very low: HR = 1.52, CI [1.16, 2.00] (Figure 1), after adjustment for age, gender, ethnicity, PIR, diabetes, CKD, preexisting CVD, and obesity. Additionally, adults in households with marginal, low, and very low food security had statistically significantly higher risk of experiencing CVD mortality than adults in households with full food security, marginal: HR = 1.79, CI [1.10, 2.93]; low: HR = 1.21, CI [0.64, 2.29]; and very low: HR = 2.00, CI [1.16, 3.44] (Figure 2), after adjustment for age, gender, ethnicity, PIR, diabetes, CKD, preexisting CVD, and obesity.
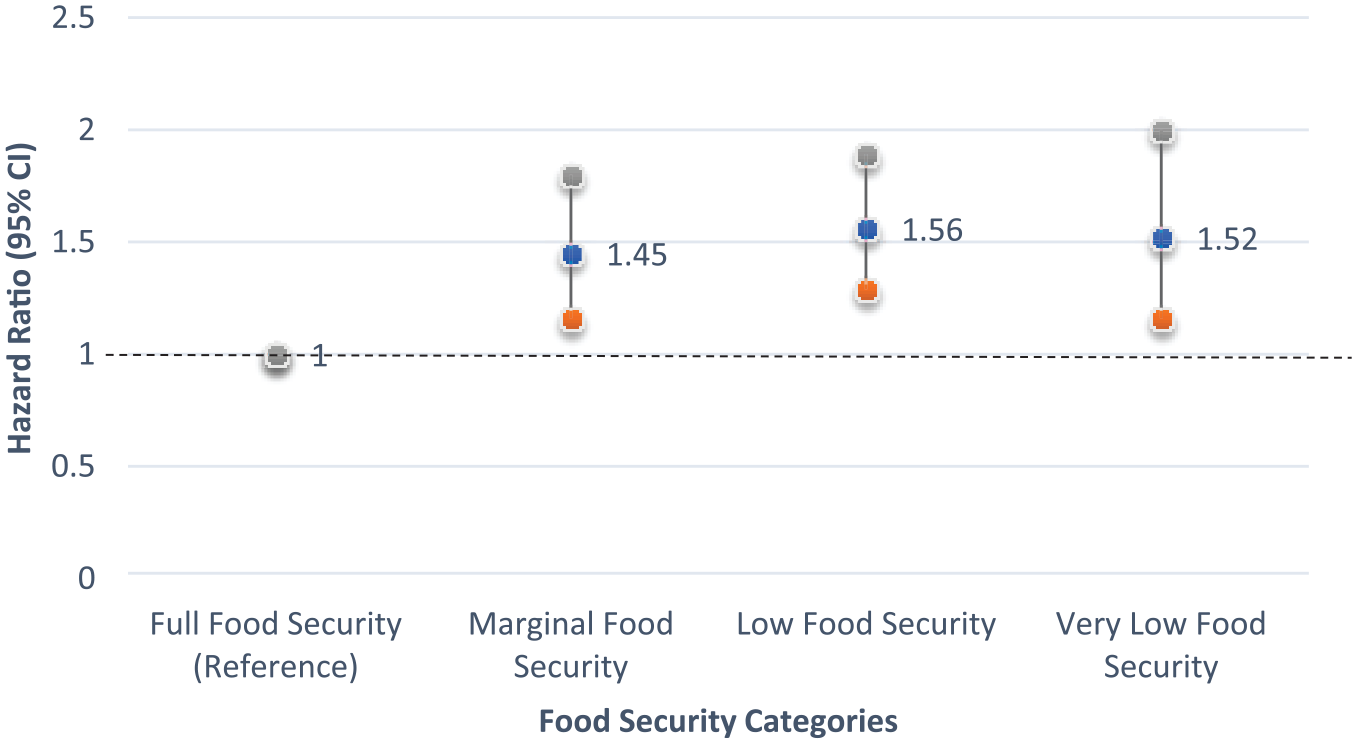
Food Insecurity Versus All-Cause Mortality
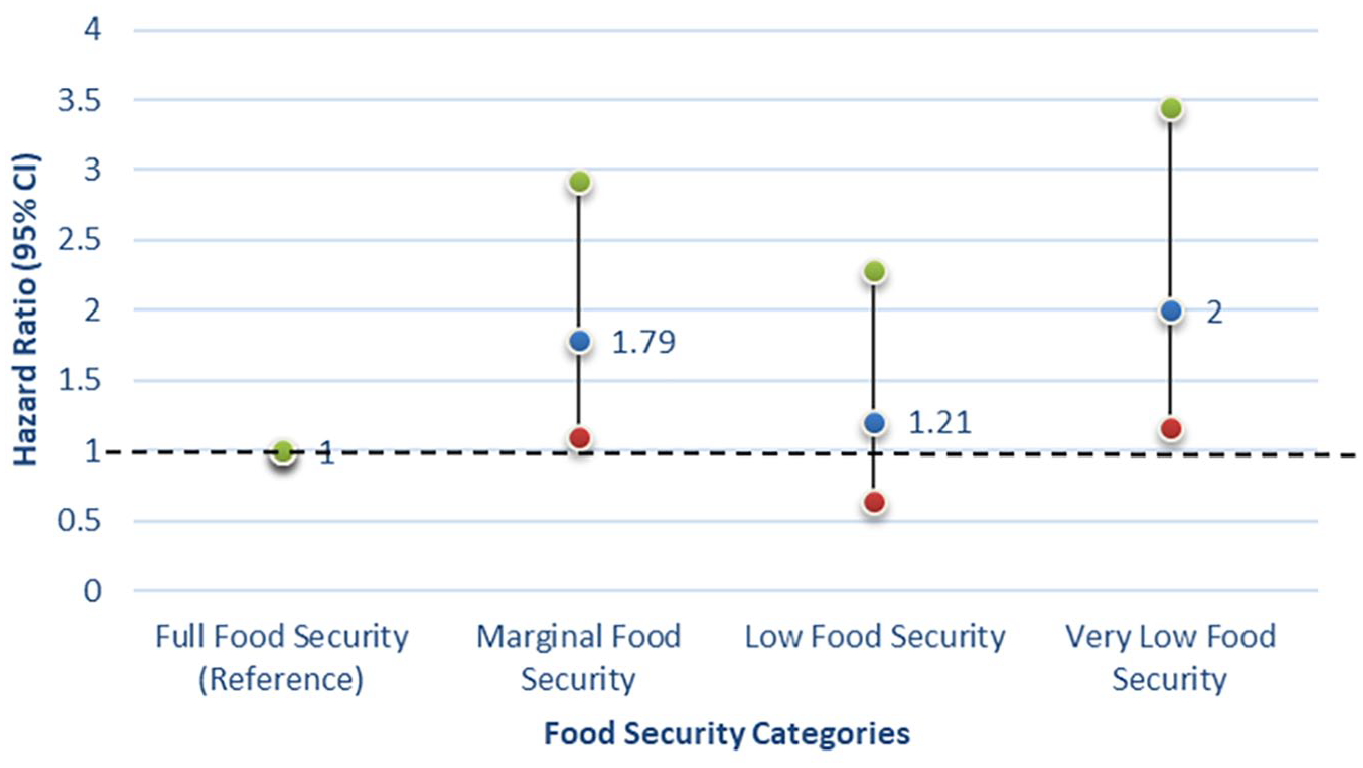
Food Insecurity Versus Cardiovascular Disease–Related Mortality
Discussion
In a large multiyear cohort of adults across the United States, the results of this study help establish the prevalence of food insecurity and mortality associated with food insecurity. The prevalence of food insecurity (17.6%) computed in this study is well within the range of statistics (15%–20%) demonstrated in earlier studies from United States within the past decade (S. Banerjee & Radak, 2019; Berkowitz et al., 2017; Palakshappa et al., 2019; USDA, 2018). In addition, the link between food insecurity and sociodemographic characteristics found in this study is well corroborated by earlier nationwide studies with food-insecure individuals more likely to be poor, have less education, be racial and ethnic minorities, be obese, be current smokers, and have chronic disease conditions such as diabetes and CVD (Berkowitz et al., 2017; Palakshappa et al., 2019).
The increased presence of food insecurity among racial minorities is an important finding. Overall, minorities within the United States face disproportionate hardships economically. Other researchers have also found that food insecurity is more disproportionately experienced by Hispanic and Black minorities than by White counterparts (Coleman-Jensen et al., 2019). More specifically, applying the minority stress theory, the cumulative effect of minorities facing discrimination and social prejudice compounded with food insecurity may lead to poor health outcomes. Potochnick et al. (2017) found that certain policies geared toward minorities had the unintended consequence of higher levels of food insecurity among Hispanic immigrant families. Policies need to be assessed before implementation regarding the potential for causing food insecurity, particularly in minority populations.
A unique finding of this study is the long-term effect of food insecurity on mortality. Food insecurity was associated with 58% higher probability of mortality compared to those who did not report food insecurity, after controlling for age and gender only. However, after adjusting for multiple demographic, health, and behavioral risk factors, the probability of mortality in food insecure remained 46% higher compared to food-secure individuals. This finding warrants additional research and investigation to ascertain causal pathways for premature mortality in food-insecure individuals. While our adjustment for well-known modifiable and demographic health risk factors found a reduction in likelihood of mortality among individuals with food insecurity, the reduction was modest. In a recent study by Walker et al. (2019), it was found that the adjustment for health behavior and chronic disease conditions could result in loss of a significant effect of food insecurity on mortality. However, unlike our study with 10-year follow-up time, the previous researchers had a shorter follow-up time, which is suboptimal for risk scoring. Additionally, we found significance and higher mortality risk among the marginal food insecurity group while Walker et al. did not find significance in the relationship with all-cause mortality. In another study using NHANES data, Vercammen et al. (2019) found a significant increase in CVD mortality with a ≥20% 10-year increased risk in very low food-secure individuals compared to fully food-secure individuals, odds ratio = 2.36, 95% CI [1.25, 4.46]. In our study, in the overall mortality group, marginal food security and very low food security (compared to full food security) were significantly related to higher mortality but not low food security. Lack of significance in the low food security group may have been due to lack of adequate power for this category. Marginally and low food-secure individuals did not have a statistically significantly association with CVD mortality in their study, while in our study, marginally food-insecure individuals had statistically significant higher CVD mortality. Their risk prediction model was only able to demonstrate a significant increase of ≥20% 10-year CVD mortality increased risk, while we were able to show more definitive risk due to actual mortality outcomes. However, unlike our study, Vercammen et al. (2019) did not base this on actual outcomes. Rather, they based cardiovascular mortality on calculated predicted outcomes based on predetermined equations. Finally, in another study, eating frequency rather than a formally validated HFSSM identified greater frequency of eating being associated with an increase in CVD mortality (Chen et al., 2016). We demonstrated through a formally defined HFSSM, which includes the concept of hunger, that food insecurity was associated with longitudinal higher risk of mortality.
A major novel finding of this study is that food insecurity had an independent effect on cardiovascular mortality even after controlling for known preexisting cardiovascular conditions as covariates like congestive heart failure, stroke, angina, coronary heart disease, or myocardial infarction. Men et al. (2020) found increases in mortality due to food insecurity on a population level in Canada. However, we conducted our study within the United States and specifically investigated the effect of food insecurity–related cardiovascular outcomes adjusting for existing CVD. Men et al. combined cardiovascular and respiratory outcomes, not allowing for proper discernment of cardiovascular outcomes. Ranking importance of risk factors based on HR in our study, food insecurity was found to be more important than preexisting CVD conditions in determining risk profile for cardiovascular mortality (Anderson et al., 2019; Ford, 2013; Fowokan et al., 2018; Saiz et al., 2016). This fact lends to the idea that food insecurity should be part of the clinical cardiovascular risk scoring algorithms.
Given the multiple causal pathway of development of CVD from gene–environment interactions, clinicians should emphasize and include food insecurity in cardiovascular mortality risk scoring algorithms in order to make treatment decisions. The interaction between genetic predisposition and environmental factors like food insecurity leads to a need to address these multiple causes simultaneously. This presumption is supported with previous research regarding food insecurity in adults being associated with an increased prevalence of cardiovascular risk as measured by the Framingham score (Anderson et al., 2019; Arnett et al., 2019; Saiz et al., 2016). This would mean that food insecurity could be linked to premature mortality through multiple causal pathways with overlapping risk factors indicating the need for a comprehensive approach to addressing food insecurity including interventions in community and health care settings (Anderson et al., 2019).
The connection between food insecurity and CVD has been previously attributed to the connection of food insecurity with risk factors like diabetes, hypertension, and hyperlipidemia (Berkowitz et al., 2017; Chen et al., 2016; Morales et al., 2016; Palakshappa et al., 2019; Vercammen et al., 2019; Walker et al., 2019). Specifically, this connection to CVD may be linked to the food-insecurity-obesity paradox. This paradox is supported by our research finding that those individuals with obesity are significantly more likely to be food insecure than those individuals without obesity. Additionally, food insecurity may also lead to chronic stress related to CVD. However, in our study, even after controlling for obesity and other cardiovascular risk factors, food insecurity was found to be a significant risk factor for CVD mortality. Therefore, food insecurity can be considered a fundamental risk factor for CVD and should be added as a guideline for the assessment of cardiovascular risk. This finding is especially important given that the American Heart Association is working to create innovative system-level approaches to improve individual-level diet-related health and create a sustainable food system (Anderson et al., 2019; Arnett et al., 2019; Ford, 2013; Saiz et al., 2016).
Revisiting and applying the CSDH framework, food insecurity is a major component of the intermediary social determinants of health, which eventually leads to poor health outcomes. As part of material circumstances, a subcategory of the intermediary determinants, food availability is part of the existing model (Dowler & O’Connor, 2012). While the concept of food availability is a part of food insecurity, we believe that food access and insecurity are more important metrics and indicators of determinants of health. As seen in the CSDH, these material circumstances have a major impact on equity in health and well-being. However, further upstream in the model, food insecurity can be considered a byproduct of social policy.
Practice Implications
Food insecurity should be considered an independent social determinant risk factor for morbidity and mortality. Public health practitioners should consider food insecurity and diet quality along with other social determinants of health, when determining an individual’s overall health risk and especially the risk for CVD. Recontextualizing from an individual health focus to application of the CSDH framework to food insecurity is important to protect vulnerable populations, especially during times of economic downturn and disrupted food supply chains. Nutritionists and health care providers should emphasize access and hunger issues rather than focus on individual food behavior issues, like avoidance of high-calorie foods, to address CVD risk factors like obesity. While it is important to restrict fast food and sugary drinks, lack of regular access to nutritious foods influences the type of diet the individual follows. Additional research is needed to explore culturally sensitive practices for assessing food insecurity in an effective, efficient, and dignified manner. Finally, long-term prospective studies with robust outcome ascertainment for premature mortality and CVD risk should include diet quality and food insecurity measures that can help understand the risk and causal pathways for premature mortality in American adults, given that heart disease is a leading cause of death (Anderson et al., 2019; Arnett et al., 2019; Chen et al., 2016; Ford, 2013; Fowokan et al., 2018; Lundeen et al., 2017; Morales et al., 2016; Saiz et al., 2016).
The results of this study should be considered in light of a few potential limitations. First, the data for this study come from a survey, and such self-reported data are susceptible to recall bias and social desirability bias, limiting the validity of findings. Second, including longer follow-up times and disease-specific mortality may have allowed further exploration of the specific impact of food insecurity, but the analysis was limited by data availability in the NHANES study. Specifically, the potential limitation is that participants sampled in later cycles of the NHANES had shorter follow-up data, resulting in varied follow-up among different cycles. Finally, mortality and health status can be influenced by a variety of factors that we may not have accounted for due to limitations of existing data availability. To the extent that this may have happened, this could be a threat to the validity of findings. However, we used previously validated and recommended operationalization of variables (Anema et al., 2013; Barger et al., 2016). Therefore, despite these limitations, we utilized a large national random sample of adults across the United States with high representativeness and a large number of demographic- and health-related variables, making this a unique contribution with findings that can be generalized across the adult population in the United States.
Conclusion
Food insecurity and hunger continue to be an important social determinant of health when considering health issues. Food insecurity leads to not only higher overall mortality but also higher levels of cardiovascular mortality, in spite of preexisting cardiovascular conditions. Awareness of this risk factor can lead to better informed screening for food insecurity by health care practitioners.