
Abstract
Adolescents face a number of barriers to accessing high-quality, confidential sexual and reproductive health (SRH) services. Although federally qualified health centers (FQHCs), a type of community health center (CHC), are a critical source of health care for medically underserved adolescents, they often lack the capacity and resources to provide specialized SRH services to adolescents. In this article, we describe the development and implementation of an initiative aimed at improving an FQHC’s capacity to provide high-quality confidential SRH services to adolescents. For this initiative, a team of clinical and quality improvement staff developed a set of six strategies to improve adolescent SRH services at an FQHC: (1) building community relationships and galvanizing internal organizational support to improve adolescent access to confidential SRH services, (2) developing a long-acting reversible contraception (LARC) program, (3) training clinic staff on SRH and adolescent health topics, (4) adapting the adolescent patient workflow to improve SRH service delivery during appointments, (5) updating and implementing a universal adolescent health assessment tool, and (6) developing billing and registration policies that allow adolescents to receive confidential SRH services. We identified several factors that we believe were key to the successful implementation of our approach in other CHC settings, including encouraging cross-sector collaboration and community focus, providing training as a tool to engage and empower staff as agents of change, involving interdisciplinary staff, piloting on a small scale, and establishing consistent meetings with a clinic champion and improvement team.
Keywords
Assessment of Need
Federally qualified health centers (FQHCs) are a critical source of health care for nearly 3 million adolescents in medically underserved U.S. communities, providing care to 10% of all 12- to 18-year-olds (Mead et al., 2015). Designed to offer subsidized, high-quality care to low-income individuals, FQHCs are well-positioned to play a significant role in providing comprehensive sexual and reproductive health (SRH) services to vulnerable adolescents despite substantial financial and structural barriers (Mead et al., 2015). In an effort to increase the capacity of publicly funded health centers to provide adolescent SRH services, the Centers for Disease Control and Prevention (CDC) funded the Teen Access and Quality (TAQ) initiative (Brittain et al., 2020). As part of TAQ, Sexual Health Initiatives for Teens–North Carolina (SHIFT-NC), a non-profit in Durham, North Carolina, partnered with Lincoln Community Health Center (LCHC), an FQHC system also in Durham, from 2015 to 2020. We received institutional review board approval for this project through Chesapeake Institutional Review Board (Protocol #00022471).
In 2019, 66% of LCHC adolescent clients were Latinx and 26% were Black; these demographic groups, respectively, experience adolescent pregnancy rates 11 and 5 times higher than White adolescents in Durham County (Garrison, 2017; SHIFT-NC, 2019). To reduce unintended pregnancy, SRH service providers need to address the barriers adolescents encounter in accessing SRH services, including prohibitive financial costs, inadequate access to highly effective contraceptives, and a lack of confidentiality (Brittain et al., 2020). LCHC faced significant challenges in providing confidential, low-cost contraceptive and sexually transmitted infection services for adolescents because it does not receive Title X funds, serves a large number of uninsured patients, and operates in a state that did not approve Medicaid expansion. LCHC has a strong commitment to equity and only offers services that can be provided to all patients, regardless of their insurance status. Therefore, LCHC absorbs costs for uninsured patients.
At the start of our collaboration, we initiated an assessment in 2016 exploring LCHC’s practices regarding adolescent SRH services using three tools: an assessment of organizational policies, a survey of provider attitudes and practices, and a survey of adolescent patient satisfaction. We identified three main areas for improvement from the results of these tools: (1) standardizing SRH service provision to adolescent patients, (2) decreasing structural barriers to confidential adolescent SRH services, and (3) increasing receipt of minor’s rights information and time alone with a provider.
Standardizing SRH Service Provision to Adolescent Patients
Our assessment revealed variability in providers’ approach to adolescent health needs, sexual health assessments, and counseling practices. Adolescents reported inconsistent receipt of information about contraception (40% received information) and sexually transmitted infection prevention (58% received information; CDC, 2017a, 2017b). To further understand these issues, we used process mapping, which revealed use of differing assessment tools and inconsistencies in the delivery of SRH services. Less than 25% of staff had been formally trained on adolescent or SRH topics (Garrison, 2017). On a scale of 1 to 5 (1 = never, 5 = always), providers reported an average of 3.1 for assessing reproductive life plan, a reflective protocol that supports individuals in identifying reproductive intentions and effective family planning strategies (Files et al., 2011).
Decreasing Structural Barriers to Confidential Adolescent SRH Services
Concerns about financial burden to LCHC as well as Health Resources and Services Administration (HRSA) requirements regarding patient registration and proof of income had historically prevented uninsured and privately insured adolescents from registering as new patients without parental consent and, therefore, receiving confidential care in accordance with NC state law. Without Title X funds, LCHC would have to subsidize the cost of confidential adolescent health visits to avoid sending home an explanation of benefits or bill from LCHC.
Increasing Receipt of Minor’s Rights Information and Time Alone With a Provider
Sixty eight percent of adolescents reported receiving information about their rights to SRH services during their appointment (CDC, 2017b). In addition, providers reported having time alone with adolescents about 70% of the time (CDC, 2017a, 2017b). To address these areas for improvement, we utilized a multipronged set of strategies described below.
Description of Strategy
We created six strategies to improve the quality of adolescent SRH services at LCHC (Table 1). These strategies were the result of a close collaboration between a clinic champion (an LCHC provider) and a quality improvement (QI) specialist from SHIFT-NC. Our strategies included the following:
Relationship building and galvanizing internal support
Establishing a long-acting reversible contraception (LARC) program
Building knowledge through staff training
Adjusting workflow to allow for adolescent access to SRH services
Developing a universal adolescent health assessment tool
Changing billing and registration protocols
LCHC’s Strategies to Improve Adolescent Access to Confidential SRH Services, Details of Each Strategy’s Implementation, and Related Outputs
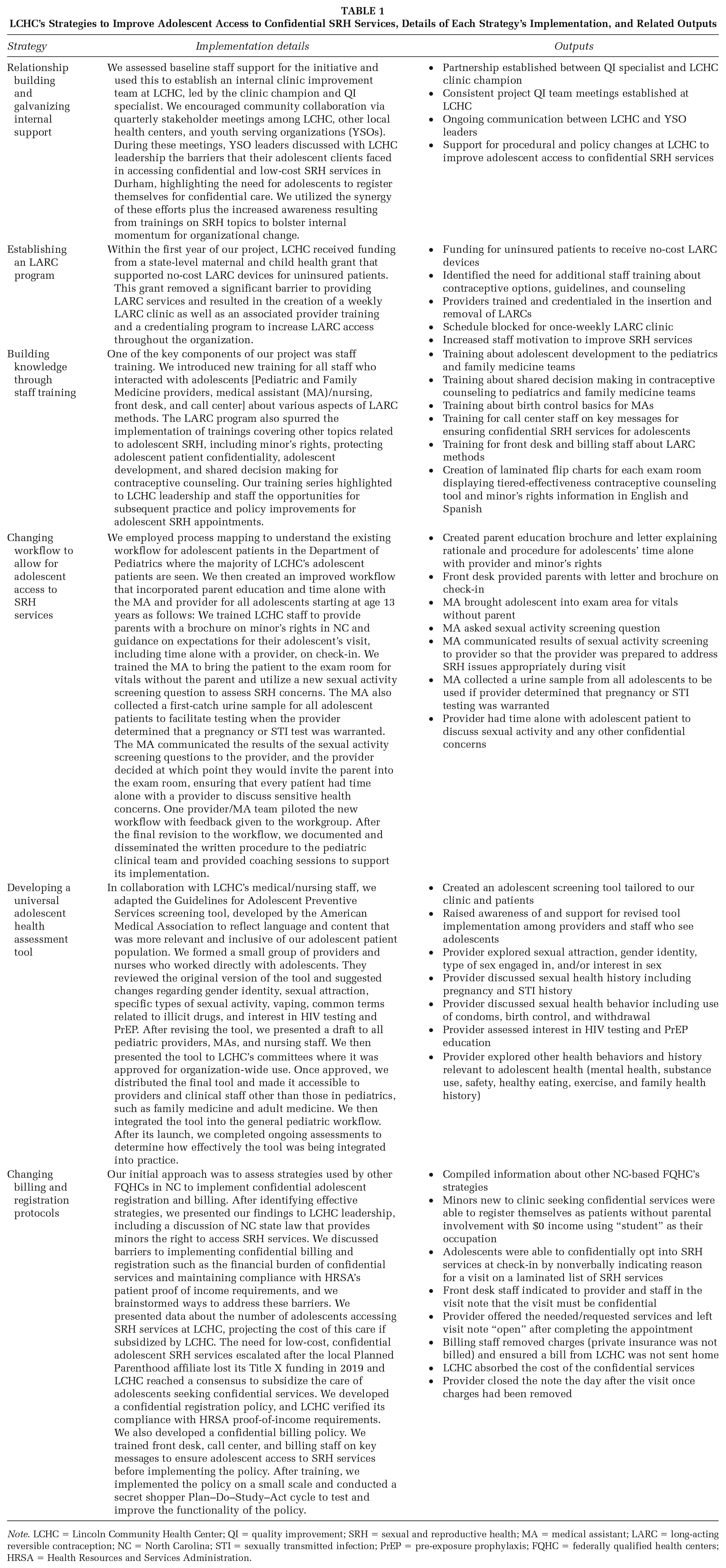
Note. LCHC = Lincoln Community Health Center; QI = quality improvement; SRH = sexual and reproductive health; MA = medical assistant; LARC = long-acting reversible contraception; NC = North Carolina; STI = sexually transmitted infection; PrEP = pre-exposure prophylaxis; FQHC = federally qualified health centers; HRSA = Health Resources and Services Administration.
Implications for Practice
Providing high-quality, low-cost, confidential SRH services to adolescents is challenging for many CHCs due to lack of staff training, competing priorities with other high-need populations, and costs associated with subsidizing confidential services. Although it may be impractical for other CHCs to implement this approach holistically, the application of any of the identified strategies could improve the quality of adolescent SRH services. From our experience in implementing this approach we learned that (1) cross-sector collaboration and community focus helped garner both initial and sustained support for change initiatives, (2) training increased staff knowledge of adolescent SRH topics and also galvanized support for the implementation of further change in clinic operations, (3) involving LCHC staff from all disciplines in the QI process better informed the design and application of practice improvements and built staff investment in implementing changes, (4) small-scale piloting of change strategies increased engagement and confidence in enacting changes while also uncovering potential issues with new protocols before implementation on a broader scale, and (5) a clinic champion and improvement team dedicated to meeting regularly facilitated QI work, staff trainings, and progress toward outlined strategies.
We recognize that our CDC grant funding supported the clinic champion’s time, as well as the SHIFT-NC QI specialist’s time, to facilitate the improvement team and provide trainings. A challenge for other CHCs seeking to improve adolescent SRH services may be funding to support staff time away from clinical care, as well as an external QI specialist, although these resources and expertise may be available within the organization or through other partnerships. Given our experience, we believe that our approach provides practical guidance for CHCs to effectively improve SRH services for adolescents.
Footnotes
Authors’ Note:
We want to acknowledge the funding support for this project from the Centers for Disease Control and Prevention (CDC; grant # NU58DP006141) for the Teen Access and Quality initiative. We gratefully acknowledge the staff and leadership at Lincoln Community Health Center for their innovation and work implementing this project. We also want to acknowledge the contributions of our All Together Now project partners and the All Together Now project staff including Ashley Stewart, Beth Vazquez, Elise Berrier, Joy Sotolongo, Karin Ganter-Luker, LaQuana Palmer, Meredith Burns, Michela Garrison, Sarah Davis, and Tamara Roberston and SHIFT-NC Manuscript Consultant Amy Vincus. This manuscript was made possible through funding from the CDC. Its content is solely the responsibility of the authors and does not necessarily represent the official views of the CDC.