
Abstract
Purpose and Objectives
This article describes the implementation and evaluation of a chronic disease mini-grant initiative, coordinated by a state health department in collaboration with multiple stakeholders. Braided funding from federal and state sources was used to build and implement the initiative.
Intervention Approach
Mini-grants, facilitated by five different facilitating organizations, were funded to promote implementation of policy, systems, and environmental (PSE) changes at the local level. Grant recipients represented a variety of sectors, including education, government, and nonprofit organizations.
Evaluation Methods
Primary (surveys) and secondary (final reports) data documented achievement of PSE changes.
Results
A total of $196,369 was dispersed to 65 organizations; 126 PSE changes in the areas of physical activity, nutrition, and tobacco were reported. Challenges in implementing and evaluating mini-grants were identified, including the heterogeneity of the sectors/settings involved and associated variability of proposed activities, time lines, measurement, and evaluation activities. COVID-19 (coronavirus disease 2019) also disrupted the plans for many projects.
Implications for Public Health
The success of this initiative can be attributed to four main elements: (1) the use of intermediary organizations to facilitate the mini-grants; (2) a participatory evaluation process, combined with early and ongoing communication among all stakeholders; (3) a braided funding strategy; and (4) a multisector approach that engaged both traditional and nontraditional public health organizations. The processes and outcomes, including challenges, can inform other state health departments’ efforts in braiding funding and engaging intermediary organizations to expand the reach of PSE changes at the local level.
Keywords
Heart disease and cancer remain the leading preventable causes of death in the United States (Centers for Disease Control and Prevention [CDC], 2020). Physical inactivity, excess body weight, and tobacco use increase risks of various cardiometabolic diseases and cancer (Physical Activity Guidelines for Americans, 2018; Warren et al., 2014). West Virginia residents experience enormous burdens related to chronic disease. Compared with the rest of the U.S. population, West Virginia has a disproportionate number of adults with cancer, heart diseases, diabetes, obesity (United Health Foundation, 2019), and among the highest rates of physical inactivity and poor nutrition (Segal et al., 2017). Poor economic conditions, lower levels of educational attainment, the state’s geography, and lack of access to health care compound these public health challenges (Marshall et al., 2017). These disparities suggest that West Virginia will continue to experience public health challenges without comprehensive interventions that address policy, systems, and environmental (PSE) changes. Implementation of PSE changes at the population level has a high impact relative to expenditure strategy, and over the past 10 years, public health practitioners have been encouraged to focus on PSE change strategies to address major risk factors for chronic disease (Bunnell et al., 2012; Frieden, 2010).
A community-driven approach to health promotion that engages key stakeholders is widely recognized as an effective way to prevent or reduce the impact of chronic disease (Bunnell et al., 2012; Lyn et al., 2013). Mini-grants, also known as microfunds, have gained traction as an innovative way to build community capacity for health promotion as, even with small amounts of funding, they provide a mechanism for community-driven approaches (Bobbitt-Cooke, 2005; Hartwig et al., 2006). Mini-grants have been used to fund rural churches and worksites to disseminate evidence-based nutrition programs (Honeycutt et al., 2012), African American churches to offer arts-based education to increase awareness of the importance of colorectal cancer screening (Friedman et al., 2019), community-based cancer survivor organizations to increase physical activity among cancer survivors (Perry et al., 2020), economic development organizations (Abildso et al., 2019), community coalitions (Kelly et al., 2019) to improve access to healthy food and physical activity, and schools to increase youth physical activity (Moore et al., 2016). Although existing studies point to the potential of mini-grants to improve community health, few have an explicit focus on promoting and evaluating PSE changes. Furthermore, limited information is available about how mini-grants are funded. As state health departments are looking for more flexibility in using categorical funding, it is important to highlight creative uses of funding.
This practice-focused article describes how braided funding and intermediary organizations were used to provide mini-grants to a variety of health and non-health-related organizations to promote PSE changes in the areas of nutrition, physical activity, and tobacco. Implementation occurred in a primarily rural state with a high prevalence of chronic disease. Furthermore, as mini-grant implementation unfolded during the COVID-19 pandemic, information about how the pandemic affected implementation is also described. The processes and outcomes described here can inform other state health departments’ efforts in partnering with intermediary organizations to promote and evaluate PSE changes at the local level. This article is responsive to the call for public health practitioners to generate practice-based evidence and for Prevention Research Centers to support state health departments in generating such evidence (Ammerman et al., 2014). It also is responsive to the recommendation to engage diverse sectors in health promotion and PSE change endeavors (Hartwig et al., 2006; Lyn et al., 2013) and to this journal’s expressed purpose to publish articles focused on the practical application and evaluation of public health interventions.
Method
Intervention Methods
In 2019, the West Virginia state health department implemented a chronic disease mini-grant initiative focused on PSE change strategies. The focus on PSE changes represented a shift in how this state issued mini-grants—previous mini-grants primarily supported individual-level interventions, which are known to have limited effectiveness (Bunnell et al., 2012; Frieden, 2010). This initiative was informed by social ecological models (SEMs), which have long been used in health promotion to conceptualize and design health interventions (Sallis & Owen, 2015) as well as the Health Impact Pyramid (Frieden, 2010). Both models encourage a focus on more population-based upstream strategies (e.g., policy, organizational, and community levels) rather than focusing solely on individual-level strategies (Leeman et al., 2015). PSE change strategies are conceptually supported by both the SEM and the Health Impact Pyramid as they focus on changing the context to enable healthy decision making.
A fiscal method of combining funds from multiple sources, called braided funding, was used to fund the initiative. Braided funding is increasingly being used by public health agencies to amplify their efforts beyond what is currently possible through categorical funding alone (Ensign & Kain, 2020). Although the technique of braided funding is not new per se, its use in this mini-grant initiative represented a departure in how the West Virginia state health department typically funded mini-grants (previous practice used categorical funding). The move to braiding funding enabled PSE changes to be a focal point, while still allowing for tracking and reporting back to the original source of categorical funding.
Key stakeholders included the West Virginia Prevention Research Center, one of 26 federally funded Prevention Research Centers, and five statewide intermediary organizations, hereafter referred to as facilitating organizations. The use of intermediaries who serve and work with rural communities is a recommended means to leverage rural communities’ strengths to improve health and health equity (Walsh Center for Rural Health Analysis, 2018). These particular facilitating organizations were chosen for their subject matter expertise and access to local-level organizations and included Worksite Wellness—Active Southern West Virginia, Cancer Prevention—Mountains of Hope Cancer Coalition, Physical Activity—Center for Active West Virginia, School-Based Health Centers—West Virginia Primary Care Association, and Community–Clinical Linkages—West Virginia University Office of Health Services Research. The implementation and evaluation period for these mini-grants was from July 2019 to June 2020.
The West Virginia state health department expected the facilitating organizations to incorporate several components in every mini-grant—Request for Proposal (RFP)—regardless of the funding purpose and source, including PSE change strategies, addressing health inequities, joining West Virginia Health Connection, and incorporating sustainability planning. Details about the rationale for each of these components are provided below.
PSE change strategies are deemed essential to changing the context within which chronic disease risk behaviors occur (Bunnell et al., 2012). Effective PSE change involves multiple sectors (Lyn et al., 2013). Policies can include “big-P” policies enacted by elected officials, such as adopting complete streets legislation to promote physical activity, or “small-p” policies that focus on organizational guidelines and social norms, such as allowing physical activity breaks during the workday (Brownson et al., 2009). Grant applicants were encouraged to propose both “big-P” and “small-p” policies in their applications and were provided with examples.
Because mortality and prevalence rates for chronic diseases vary greatly among population subgroups, reducing these disparities is a major public health priority and an underlying principle of health equity (CDC, 2015). Mini-grant recipients were encouraged to articulate how they proposed to address health inequities in their applications. This expectation was partially built on findings suggesting that one way to improve disease-related disparities is to make health equity a documented part of chronic disease prevention practice (Eyler et al., 2019).
Community–clinical linkages are considered an effective approach to prevent and control chronic diseases (Dietz et al., 2015). West Virginia Health Connection is a statewide system that facilitates community–clinical linkages by linking health care providers to local chronic disease prevention services and connecting patients to health promotion programs. Mini-grant recipients were encouraged to register with and use the technical assistance/resources provided by West Virginia Health Connection.
Ensuring the sustainability of public health interventions is challenging and critical to address, and attentiveness to sustainability throughout the planning phase of interventions is highly recommended (Shelton et al., 2018). Mini-grant applicants were encouraged to articulate clear and succinct plans for sustainability of their efforts beyond when the mini-grant funding ends.
The state health department funded the five facilitating organizations to issue RFPs and provide technical assistance for mini-grants. Although all five mini-grant mechanisms were supposed to address the expectations described above, facilitating organizations had considerable latitude in shaping their RFPs. Consequently, proposed activities, schedules, and measurement and assessment plans varied considerably across all the mini-grant projects. Table 1 shows the range of focus areas, eligible grantees, and funding source(s) across all mini-grants.
Mini-Grant Focus Areas, Eligible Organizations, and Funding Source(s)
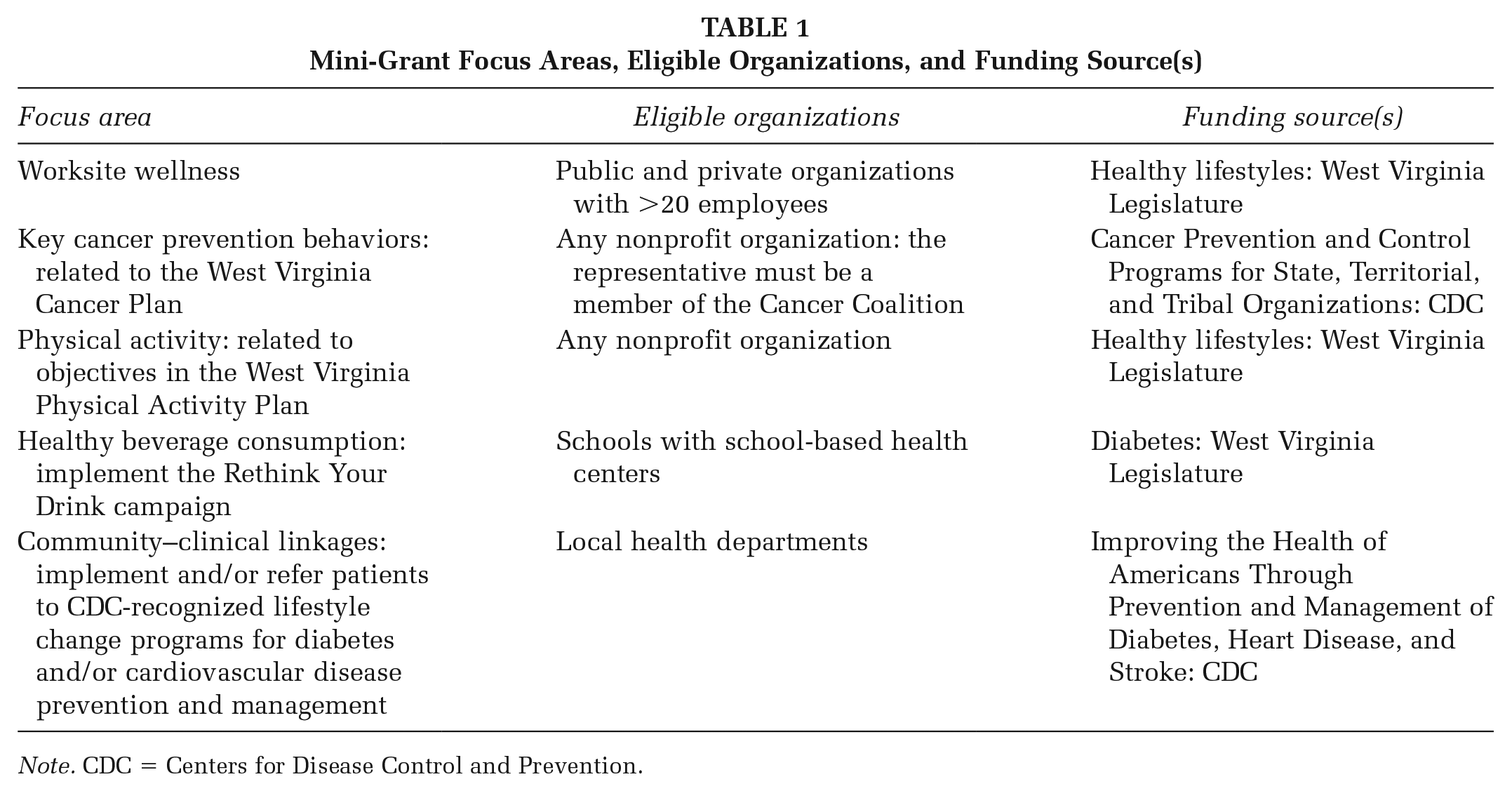
Note. CDC = Centers for Disease Control and Prevention.
Evaluation Methods
This evaluation was informed by CDC’s Framework for Program Evaluation in Public Health (CDC, 1999), wherein key stakeholders, namely, the intermediary organizations, were engaged in a participatory evaluation process that involved frequent meetings to focus on the evaluation. Evaluation questions included (1) How many and what type of PSE changes did grantees achieve? and (2) What challenges arose from a state-funded, multiagency mini-grant intervention effort?
We conducted a content analysis of the RFPs and funded applications and then created a high-level/macrologic model to provide a big picture view of the entire mini-grant initiative. High-level logic models are recommended to illustrate relationships among inputs, activities, focus areas, and outcomes (Fulmer et al., 2019). Figure 1 displays the funding inputs, focus areas, and proposed outcomes gleaned from reading each RFP and grant recipients’ applications. This figure also presents the organizational relationships and structure of the funding, facilitating organizations, and community grant recipients.
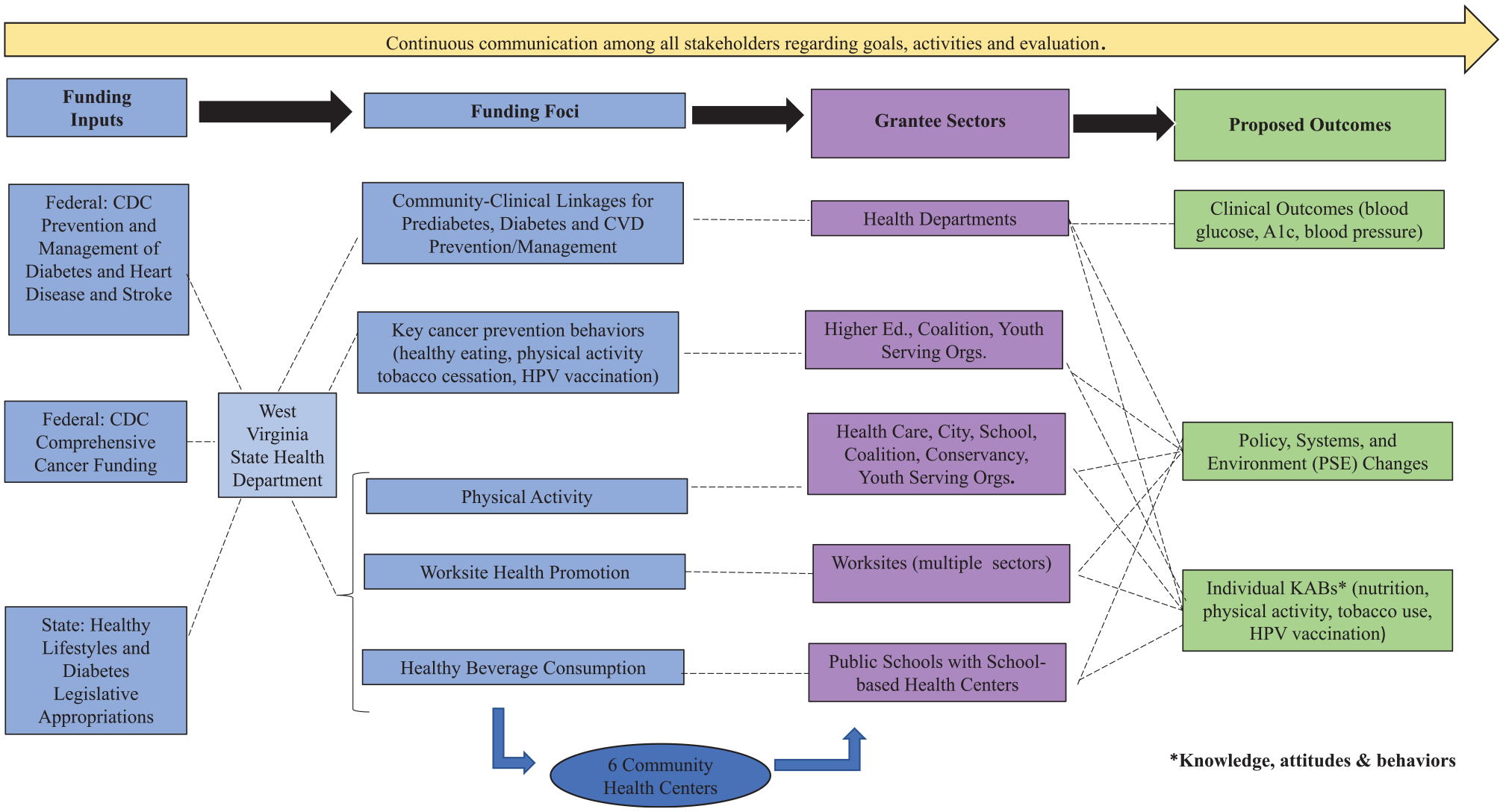
Chronic Disease Macro Mini-Grant Logic Model
We also developed specific (nested) logic models for each of the mini-grant focus areas. Nested logic models are useful for depicting complex initiatives and enable drilling down to specific details that cannot be captured in a big picture view (Newbill et al., 2017). Participatory methods were used to develop this logic model, as both the macro and the nested logic models were developed in collaboration with the grant facilitators. (The nested logic models are available in the Supplemental Material).
The evaluation included both primary and secondary data. Primary data came from end-of-project surveys sent to physical activity and worksite wellness grant recipients using the Qualtrics Survey System (Provo, Utah). The surveys were developed in collaboration with grant facilitators to enable tailoring of the survey questions to their particular focus area(s). Given the conceptual focus of the SEM and Health Impact Pyramid and implementation of PSE change strategies, the main portion of the surveys asked respondents to report attainment (yes/no response format) of the PSE changes they proposed to implement. Other questions queried grant recipients about their implementation of the RFP expectations: health equity, engagement with West Virginia Health Connection, and sustainability. These questions used a combination of closed and open-ended response formats. Questions about other areas of interest, for example, the coronavirus disease 2019 (COVID-19) disruptions and description of actions to adapt to COVID-19, used an open-ended response format. Finally, since some facilitating organizations conducted their own evaluations, we reviewed their final reports for evidence of PSE changes; these were considered secondary data for this evaluation.
Data Analysis
We categorized PSE changes using commonly used definitions, such as those in the Communities Putting Prevention to Work initiative (Bunnell et al., 2012). Policy change was defined as a written plan or course of action, systems changes were changes to practices or procedures within an organization, and environmental change was changes made to the physical, social, or economic environment.
Survey data were downloaded from Qualtrics into an Excel spreadsheet. We then conducted descriptive analyses for the closed-ended items to quantify the frequency and percent of PSE changes achieved. This allowed us to sum the total amount of money disbursed and PSE changes by various sectors (e.g., schools, health departments, community groups) and focus areas. For the open-ended responses, we grouped common responses together and identified overall categories of responses. The content analysis of final reports involved reading the reports and extracting the number of reported PSE changes; these were added to the final total of PSE changes.
Results
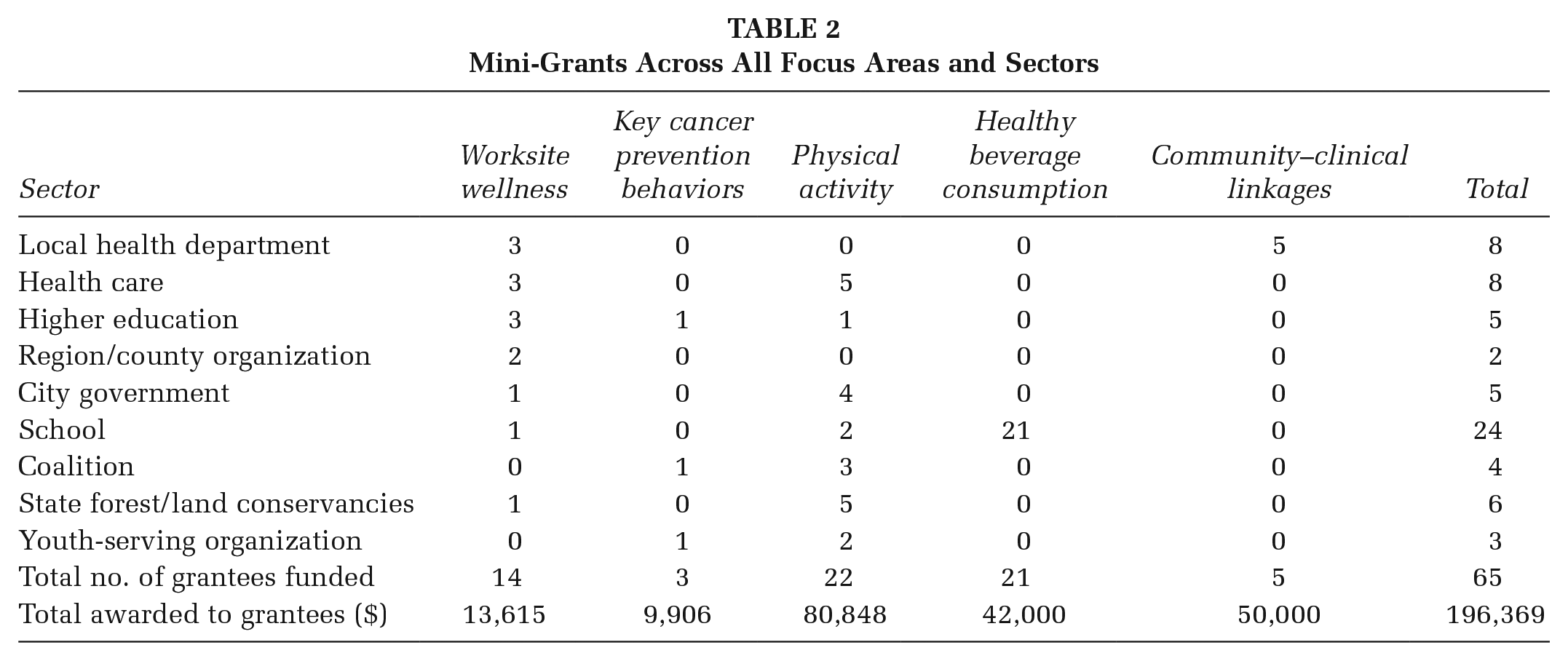
Table 2 displays the number of funded organizations by focus area and sectors across all funded mini-grants. A total of $196,369 was dispersed to 65 organizations, representing a wide variety of sectors. Notably, 65% were non-health-related community organizations: This was determined using definitions used in another mini-grant study (Hartwig et al., 2006). These included public schools, local and regional governments, and land conservation agencies.
Mini-Grants Across All Focus Areas and Sectors
PSE Changes
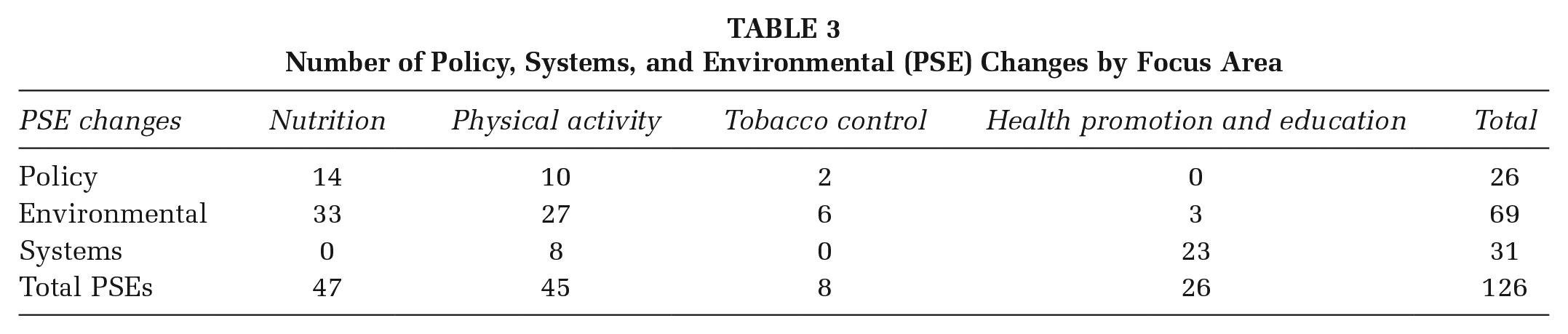
Table 3 displays the total number (n = 126) of PSE changes reported by grant recipients. Nutrition and physical activity accounted for the highest number of PSE changes, 47 and 45, respectively. Examples of policy changes included policies for no sugar-sweetened beverages at meetings and policies for flex time during the workday to enable physical activity. Systems changes included the establishment of a Walk With a Future Doc chapter at a medical school and a clinic adopting the practice of using electronic health records to assess and prescribe physical activity to patients. Environmental changes accounted for just over half of all PSE changes. Examples included community gardens and walking trails, provision of physical activity equipment at worksites, signage encouraging the consumption of water, and the creation of a wheelchair-accessible playground. Tobacco PSE changes were not as prevalent as those for nutrition and physical activity, as many recipients indicated that tobacco control policies and supportive environments were already established.
Number of Policy, Systems, and Environmental (PSE) Changes by Focus Area
Incorporation of Other Grant Expectations
The extent to which grantees incorporated other project components, such as addressing health equity and efforts to sustain projects, was uneven. For example, health inequities were intentionally addressed by only one grantee that created a wheelchair-accessible playground with complementary storyboards composed in Braille. Most of the other grantees only provided general descriptions of how they addressed health inequities or made vague statements about serving all people in their community or organization.
Sustainability was addressed by most of the grantees, and applying for more funding to continue project activities was the primary means proposed to foster sustainability. Two grantees explained how integrating their projects into existing organizational practices would foster sustainability. For example, the Walk With a Future Doc project would be sustained by establishing an official chapter of the project at the medical school, with the school taking ownership after mini-grant funding ended. Another example is a storyboard project that entailed installing structures to display pages from children’s literature along a walking trail adjacent to an elementary school. This project would be sustained by requiring teachers at the elementary school to document their use of the storyboard trail in their lesson plans.
Challenges
Challenges in implementing and evaluating mini-grants included the heterogeneity of the sectors/settings across mini-grants and associated variability of their proposed activities, time lines, measurement, and evaluation activities. Likewise, the structural capacity of the funded organizations varied, and many of the projects implemented were led by individuals without formal education or training in public health or related fields. Nine different sectors/settings (see Table 2), with varying levels of capacity to implement and evaluate their activities, were involved in this mini-grant initiative. COVID-19 also disrupted plans for many mini-grant recipients. These included the inability to meet in public places for various community events, shifts in staffing responsibilities, postponements of in-person events, and supply chain challenges related to purchasing goods and services needed for the proposed projects. Nevertheless, the grant recipients made tremendous efforts to modify their proposed projects to move forward, including conducting virtual meetings, circulating digital newsletters, increasing email contact, and rescheduling events.
After the implementation and evaluation of the 2020 mini-grant initiative, key stakeholders convened to discuss strengths, weaknesses, and recommendations to improve the 2021 mini-grant cycle. Challenges in implementing and evaluating mini-grants facilitated by five different organizations were identified, including heterogeneity of priority populations, variability among proposed activities, time lines, and measurement and evaluation activities. Furthermore, part of the uneven attention to the grant expectations was attributed to the facilitating organizations not being explicit enough in their RFPs.
Collectively, the decision was made to house all the mini-grant RFPs and resources in one place/website—https://www.wvhealthconnection.com/hpcd-grants. Other enhancements include strengthened language in each RFP to be more explicit to each of the grant expectations. Scoring rubrics were also revised to evaluate applicants’ responsiveness to each of the grant expectations in their proposals. This process is underway. Future plans include conducting a process evaluation of the enhanced mini-grant process with grant-facilitating organizations, grant proposal reviewers, and grant recipients to identify strengths, weaknesses, and recommendations to improve the 2022 mini-grant cycle. An outcome evaluation of the 2021 cycle is also planned.
Discussion
This article describes how a state health department braided funding from multiple sources to support the implementation of chronic disease–focused PSE changes by local organizations. Despite COVID-19 disruptions, a wide variety of organizations—primarily non-health-oriented—implemented 126 PSE changes. Just over half of the PSE changes involved environmental modifications, including built and social environments.
This study has limitations similar to those reported in other evaluations of mini-grant programs (Abildso et al., 2019; Friedman et al., 2019; Perry et al., 2020). First, because the mini-grants were focused at the organizational or community level, we did not measure change at the individual level. Furthermore, the lack of a control group in this study precludes making assumptions about any causal effects of the mini-grant funding on implementation of PSE changes. Relatedly, we did not objectively measure any of the reported PSE changes, which opens up the possibility of social desirability response bias inherent in a self-report. Additionally, due to the short time frame of the project, we were not able to capture sustainability of any changes initiated with mini-grant funding, though this will be a focus of future investigation. Finally, this study was conducted in one state, and our findings may not be generalizable to other settings.
Implications for Practice
Promoting PSE changes is a recommended strategy to improve community health. Mini-grants are a promising approach to build community capacity and drive PSE changes at the local level and should be promoted. This initiative and its evaluation contribute to the practice-based evidence by demonstrating that, with relatively small amounts of funding, health and non-health-related organizations can stimulate PSE changes in their communities.
This evaluation offers implications for public health practice, and the success of this initiative can be attributed to four main elements: (1) the use of intermediary organizations to facilitate the mini-grants; (2) a participatory evaluation process, combined with early and ongoing communication between the evaluators and the intermediary organizations; (3) a braided funding strategy; and (4) a multisector approach that engaged both health and non-health-related organizations. The processes and outcomes, including challenges, can help inform other state health departments’ efforts in braiding funding and engaging intermediary organizations to facilitate the implementation of PSE changes at the local level.
Supplemental Material
sj-pptx-1-hpp-10.1177_15248399211039788 – Supplemental material for Maximizing the Potential of Mini-Grants to Promote Policy, Systems, and Environmental Changes: Outcomes and Challenges
Supplemental material, sj-pptx-1-hpp-10.1177_15248399211039788 for Maximizing the Potential of Mini-Grants to Promote Policy, Systems, and Environmental Changes: Outcomes and Challenges by Nancy O’Hara Tompkins, Jessica Wright, Peter Giacobbi, Bayan Alelaiwat, James Vance, Micah Gregory, Craig Bromley and Megan Ross in Health Promotion Practice
Supplemental Material
sj-pptx-2-hpp-10.1177_15248399211039788 – Supplemental material for Maximizing the Potential of Mini-Grants to Promote Policy, Systems, and Environmental Changes: Outcomes and Challenges
Supplemental material, sj-pptx-2-hpp-10.1177_15248399211039788 for Maximizing the Potential of Mini-Grants to Promote Policy, Systems, and Environmental Changes: Outcomes and Challenges by Nancy O’Hara Tompkins, Jessica Wright, Peter Giacobbi, Bayan Alelaiwat, James Vance, Micah Gregory, Craig Bromley and Megan Ross in Health Promotion Practice
Supplemental Material
sj-pptx-3-hpp-10.1177_15248399211039788 – Supplemental material for Maximizing the Potential of Mini-Grants to Promote Policy, Systems, and Environmental Changes: Outcomes and Challenges
Supplemental material, sj-pptx-3-hpp-10.1177_15248399211039788 for Maximizing the Potential of Mini-Grants to Promote Policy, Systems, and Environmental Changes: Outcomes and Challenges by Nancy O’Hara Tompkins, Jessica Wright, Peter Giacobbi, Bayan Alelaiwat, James Vance, Micah Gregory, Craig Bromley and Megan Ross in Health Promotion Practice
Supplemental Material
sj-pptx-4-hpp-10.1177_15248399211039788 – Supplemental material for Maximizing the Potential of Mini-Grants to Promote Policy, Systems, and Environmental Changes: Outcomes and Challenges
Supplemental material, sj-pptx-4-hpp-10.1177_15248399211039788 for Maximizing the Potential of Mini-Grants to Promote Policy, Systems, and Environmental Changes: Outcomes and Challenges by Nancy O’Hara Tompkins, Jessica Wright, Peter Giacobbi, Bayan Alelaiwat, James Vance, Micah Gregory, Craig Bromley and Megan Ross in Health Promotion Practice
Supplemental Material
sj-pptx-5-hpp-10.1177_15248399211039788 – Supplemental material for Maximizing the Potential of Mini-Grants to Promote Policy, Systems, and Environmental Changes: Outcomes and Challenges
Supplemental material, sj-pptx-5-hpp-10.1177_15248399211039788 for Maximizing the Potential of Mini-Grants to Promote Policy, Systems, and Environmental Changes: Outcomes and Challenges by Nancy O’Hara Tompkins, Jessica Wright, Peter Giacobbi, Bayan Alelaiwat, James Vance, Micah Gregory, Craig Bromley and Megan Ross in Health Promotion Practice
Footnotes
Authors’ Note:
This article was supported by multiple funding sources: Improving the Health of Americans Through Prevention and Management of Diabetes, Heart Disease, and Stroke (NU58DP006528), Cancer Prevention and Control Programs for State, Territorial, and Tribal Organizations (NU58DP006300), and Diabetes and Healthy Lifestyles funding from the West Virginia Legislature.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.