
Abstract
In 2020, the HIV prevention clinical trials, HPTN (HIV Prevention Trials Network) 083 and 084, reported that long-acting injectable cabotegravir (CAB-LA) for HIV prevention was statistically superior to daily oral tenofovir disoproxil fumarate/emtricitabine (TDF/FTC) for pre-exposure prophylaxis (PrEP) in cisgender men and transgender women who have sex with men, and cisgender women. However, clinical efficacy does not translate to real-world effectiveness and clinical practice as evidenced by current global use of oral PrEP. There are ~626,000 users of PrEP, which is significantly below the 3 million goal set by UNAIDS for 2020. Implementation will be key to ensuring that CAB-LA reaches those who desire to use it. We describe the Layer Plus Approach for CAB-LA for PrEP dissemination and implementation. The “Layer” is focused on integrating CAB-LA into existing PrEP models of care and understanding the best delivery channels that could be established in existing programs. Important implications of layering include preparing health professionals to provide CAB-LA, improving access for potential users, and addressing existing PrEP structural and facility barriers. “Plus,” which accounts for the existing disparities in PrEP access and use, means expanding CAB-LA to reach individuals for whom HIV prevention options have not been accessible or who have lapsed on oral PrEP. Implications for Plus include the development of new structures, systems, policies, and processes. A key aspect to the Approach is building collaborations to aid successful implementation. The Layer Plus Approach is a simple but strategic framework or a tailored approach to guide dissemination research and implementation.
Keywords
In 2019, 1.7 million people became newly diagnosed with HIV globally (UNAIDS, 2020). Yet several evidence-based biomedical, behavioral, and structural strategies are available to prevent HIV acquisition (UNAIDS, 2020). Among the most efficacious biomedical strategies is preexposure prophylaxis (PrEP); however, its implementation has been slow with varied uptake since the FDA (U.S. Food and Drug Administration) approved Truvada as PrEP for adults in 2012 (AVAC, 2020). By the end of 2019, 120 (67%) countries with data adopted the WHO (World Health Organization) PrEP recommendations into national guidelines, but 42% of those reporting to the Global AIDS Monitoring system had yet to implement the adopted recommendations (Schaefer et al., 2021). Globally, there are approximately 626,000 users of PrEP, falling far short of UNAIDS target of reaching 3 million people with PrEP by 2020 (Schaefer et al., 2021; UNAIDS, 2020). As new biomedical options for prevention, such as the vaginal ring and long-acting injectable, become available and expand choice for individuals seeking HIV prevention, it is critically important that implementation science is at the forefront.
The HIV Prevention Trials Network (HPTN) 083 compared the efficacy of long-acting injectable cabotegravir (CAB-LA) with daily oral tenofovir disoproxil fumarate/emtricitabine (TDF/FTC) for PrEP in 4,570 HIV-negative cisgender men and transgender women who have sex with men in seven countries across the world (Landovitz et al., 2021). The HPTN 084 study evaluated the efficacy of CAB-LA compared with daily oral TDF/FTC in 3,200 HIV-negative women aged 18 to 45 in seven countries in sub-Saharan Africa (HPTN, 2020). The studies reported that the regimen containing CAB-LA was superior to daily oral TDF/FTC in July and November 2020, respectively. However, clinical efficacy does not translate to real-world effectiveness, including awareness, knowledge, demand, acceptability, and use. The superiority findings from the HPTN 083 and 084 trials highlight the importance of implementation for this HIV prevention option, especially as early acceptability research shows preference for an injectable over other prevention methods (Philbin et al., 2020). To effectively move from a clinical trial setting to real-world implementation and practice, the “key to maximizing the impact of long-acting therapy will be to ensure that it is implemented correctly, quickly, and with enough evidence and guidance around ‘what works, where, and, why?’” (Czarnogorski, 2019). Herein, we describe the Layer Plus Approach for CAB-LA for PrEP implementation research and collaboration as a resource for the identification of strategies that result in awareness, acceptability, access, and use.
The Layer Plus Approach
The Layer Plus Approach, depicted in Figure 1, posits that implementation research and dissemination are foundational and integral to ensuring that no one who wants access to HIV protection is left behind. First in the approach is implementation research, which is critical to the identification of strategies that will support the adoption, integration, and sustainment of CAB-LA for PrEP across existing and new settings, populations, and context. Second is dissemination, which is essential to relevant stakeholders (e.g., providers) adopting and effectively using the identified strategies. Third is collaborations, which is important to both resource mobilization and the widest possible access. The Layer Plus Approach is an overarching framework or guide to conduct implementation research and collaboration globally, particularly for new treatment modalities. However, the execution, focus, approaches, and strategies will depend on several factors, such as the epidemiology of the epidemic and the cultural context. The approach can be implemented concurrently or sequentially depending on context.
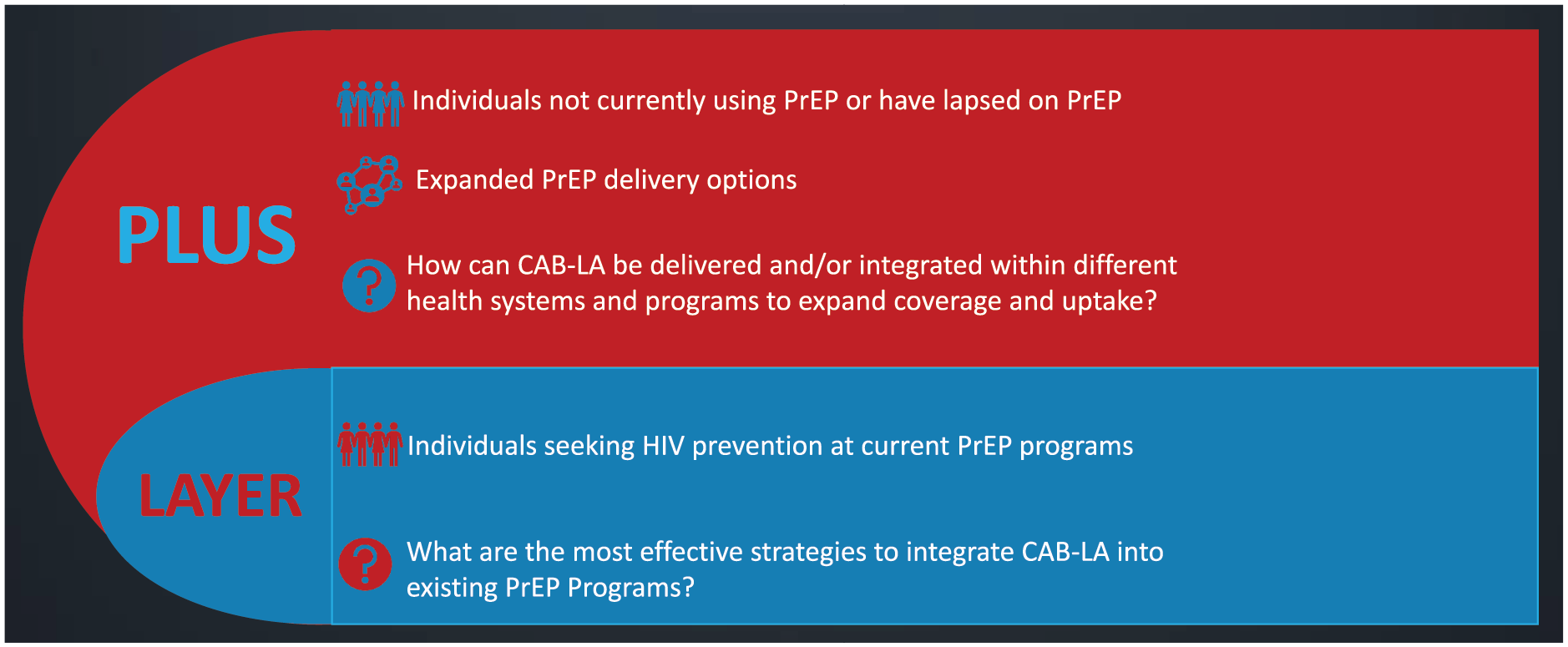
Layer Plus Approach
Defining “Layer”
The Layer part of the Layer Plus Approach is focused on dissemination and implementation of CAB-LA into existing PrEP models of care. Layer means providing CAB-LA as an additional option to individuals seeking PrEP at health care settings, community programs, and other locations already providing oral PrEP. The introduction of oral PrEP and other sexual and reproductive health prevention modalities (e.g., injectable contraceptives) has created systems, structures, and processes that CAB-LA can adopt and build upon. Although layering is a seemingly simple approach, CAB-LA will change the PrEP paradigm; as the first and only injectable HIV prevention modality, it will require changes to the current routine of prescribing oral PrEP therapy to accommodate the modality. On the implementation side, layering CAB-LA onto existing PrEP models of care will require the identification of strategies for understanding the best and maybe unique delivery channels and any changes that need to be established in existing PrEP programs, sexual and reproductive health programs, and systems. For example, existing PrEP programs will need to plan to administer injections every two months, which will change program logistics and workflow. Furthermore, understanding how to optimize the existing PrEP systems to deliver CAB-LA in a manner to reach populations who need it most will be important. Here, the identification and understanding of implementation strategies that make the delivery of CAB-LA efficient will be needed. Client-level factors associated with access and use, such as knowledge of CAB-LA efficacy, attitudes and beliefs about HIV prevention, experiences and perceptions of using HIV prevention, and interpersonal relationship factors, should be addressed to ensure implementation of a long-acting injectable medication is successful. Implementation of CAB-LA will require thoughtful consideration of how to make it work best for both providers and patients in a sustainable manner.
On the dissemination side, supporting and training health care professionals (e.g., providers, nurses) will be an important aspect to increase their knowledge, awareness, and acceptability of this new modality (e.g., side effects, scheduling, dosing regimen). Additionally, helping these individuals to overcome any biases from oral PrEP that are likely to extend CAB-LA will also be imperative. A study among 314 health care providers in Tanzania reported that only 60% would be willing to prescribe PrEP to adolescent girls and young women, a population disproportionately affected by HIV in sub-Saharan Africa (Pilgrim et al., 2018). Providers’ biases, as evidenced by higher negative attitudes toward adolescent sexuality, were associated with lower willingness to prescribe PrEP (Pilgrim et al., 2018). Providers noted apprehension toward providing sexual and reproductive health care to adolescents, especially unmarried adolescents. Studies have reported that structural and facility concerns are also critical barriers when prescribing PrEP, including staff shortages, lack of training, time constraints, and costs (Pleuhs et al., 2020). Therefore, implementation will need to account for and address these existing PrEP challenges for layering to work effectively.
As depicted in Figure 1, the layer is an important but smaller part of the approach because statistics show large disparities regarding PrEP access and use globally (Fitch et al., 2018; HIV.gov, 2018). For example, in the United States, the South accounts for greater than 50% of new HIV diagnoses but only 30% of all PrEP users (HIV.gov, 2018), while sub-Saharan Africa accounts for only 15% of PrEP initiations globally though about half of the number of new HIV infections occur in the region (Fitch et al., 2018). Stopping at integration into current PrEP programs and services will not lead to expanded prevention method choice but rather perpetuate existing disparities in knowledge, access, and use of PrEP. Therefore, Plus is the largest part of the described approach.
Defining “Plus”
Plus, in the Layer Plus Approach, means expanding the prevention method choice to reach individuals who are not aware of HIV prevention options, have not previously had HIV prevention options accessible to them, or have lapsed on oral PrEP. On the dissemination side, Plus will require a clear plan for diffusion, a process through which CAB-LA will need to be communicated and expanded into new contexts, including populations, geographies, and models of care. On the implementation side, Plus will require identifying and testing strategies to enhance the delivery and/or integration of CAB-LA into different health systems and programs to ensure access to those most vulnerable to HIV. These will possibly require system changes and new processes, including the development of new structures, identifying and changing of infrastructure requirements, developing new messages and means of message delivery, as well as new reporting requirements along with the necessary resources to make the implementation of CAB-LA feasible and adoption possible.
COVID-19 has had a devastating impact on the world. Yet the pandemic has provided pivotal lessons that can be applied to the implementation of CAB-LA for prevention. First, the strength and engagement of key collaborators—unprecedented global collaborations have been formed to create a vaccine against COVID-19. Similarly, what is needed for CAB-LA implementation is collaborations with existing and new partners with a focus on innovation and implementation sustainability (AVAC, 2021). Second, many were forced to rapidly adapt to using predominant technology for work, school, and health care. What can be learned from these rapid adaptations to expand CAB-LA to those who need it the most? Third, the voices of the communities calling for social change were more clearly heard, highlighting the importance of community voices when seeking to reach those who are often marginalized and stigmatized. Community-based models of delivery might be successful strategies for making CAB-LA for PrEP a viable and accessible option for some populations.
Implications for Practice
CAB-LA for PrEP, when available, has the potential to be a transformative prevention option in the HIV prevention toolbox. However, it will not have an impact on reducing HIV transmission globally if a clear and thoughtful dissemination and implementation strategy is not planned and executed. The key is starting with the essential implementation strategies needed to incorporate new prevention strategies into existing PrEP programs: (1) educating, training, and supporting health care professionals to provide CAB-LA for PrEP; (2) educating and improving access for populations who desire this modality; and (3) addressing existing PrEP structural and facility barriers by sharing best practices that have worked in comparable contexts, including those from COVID-19.
The next step is expanding the research focus to identify innovative strategies to increase access to PrEP in new contexts. Global collaborations between key stakeholders and innovative implementation research will be key to generating new evidence and insights to understand the best health care delivery strategies to ensure wider global access and uptake. The Layer Plus Approach is a simple but strategic framework to guide future research.
Footnotes
Authors’ Note:
N.A.P., T.M.E., and M.C. developed the conceptualization and design of the commentary. N.A.P. wrote the first draft. All authors contributed and approved the final version. The authors are employees of ViiV Healthcare, which is a pharmaceutical company that is studying long-acting injectable medications for HIV treatment and prevention.