
Abstract
Background
The COVID-19 pandemic has illuminated the profound health and safety risks of precariously employed workers, many of whom are disproportionately Latinx and Black. Precarious employment (PE) is a social determinant of health (SDOH) characterized by low wages, hazardous conditions, unstable work schedules, no termination protection, and few benefits. Even before COVID-19, calls for more effective health promotion efforts to address SDOH like PE existed.
Purpose
The University of Illinois at Chicago Center for Healthy Work, Healthy Communities Through Healthy Work developed the Healthy Work Collaborative (HWC) as an evidence-informed capacity building policy, systems, and environmental change (PSE) initiative. The HWC aimed to facilitate cross-sectoral partnerships between health and labor sector partners. The labor sector provided technical assistance (TA) to participants to improve their ability to address PE through PSE.
Methods
This article reports findings from a mixed-methods evaluation using the Kirkpatrick training model including participants’ reactions, learning, behavior, and outcomes. A pre–post survey was administered to participants (N = 21) and analyzed descriptively; 3-month post HWC interviews were conducted (N = 13) and thematically analyzed.
Conclusion
Findings included positive results at all Kirkpatrick levels. Participants’ reported that the HWC curriculum and delivery was valuable and well received; they demonstrated gains toward addressing PE through PSE knowledge and skills and increased or strengthened health/labor partnerships. In addition, HWC influenced participants’ application of HWC concepts, and in a few cases, participants’ made changes in policies and plans in their organizational settings. The HWC may serve as a model to address other SDOH through cross-sectoral PSE change.
Keywords
Background
The COVID-19 pandemic has amplified the need for the U.S. public health system to address the profound health inequities resulting from long-standing historical and structural racism. Nowhere has this been more evident than in the ways the pandemic has illuminated the health and safety risks of essential workers, many of whom are precariously employed and disproportionately Latinx and Black (Egede & Walker, 2020).
Precarious employment (PE) is generally characterized as nonstandard, contingent, low-wage, and insecure work and been associated with adverse worker, family, and community health outcomes (Benavides & Delclos, 2005; Kreshpaj et al., 2020; Tran & Sokas, 2017). PE impacts an increasing number of workers across employment sectors, especially workers of color. During the COVID-19 pandemic, many precariously employed workers were forced to continue working to earn basic wages in unsafe working conditions, putting themselves and their families at risk.
There are few known health promotion initiatives aimed at improving the health of precariously employed workers and that of their families and communities. In the years prior to the COVID-19 pandemic, calls emerged for public health and health care to address structural factors, including PE, that influence health (Baron et al., 2014; DeSalvo et al., 2017). Cross-sectoral, multi-level initiatives that address upstream policy, systems, and environmental changes (PSE) are documented to be most impactful in addressing social determinant of health (SDOH) such as PE (Frieden, 2010; Golden et al., 2015; Wolff et al., 2017).
To address this gap, a multidisciplinary team of faculty, staff, and students from the University of Illinois at Chicago’s Healthy Communities Through Healthy Work (HCHW), part of the Centers for Disease Control and Prevention/National Institute for Occupational Safety and Health (CDC/NIOSH)-funded Center of Excellence for Total Worker Health® Center for Healthy Work, developed the Healthy Work Collaborative (HWC). The HWC was a capacity building initiative to facilitate cross-sectoral partnerships between public health and health care representatives (referred to as the health sector) and worker centers and labor advocacy groups (referred to as the labor sector). HWC’s focus was to address gaps in the health sector’s knowledge of, skills in, and ability to address PE through PSE identified through a year-long action research project (Welter, Jarpe-Ratner, et al., 2021).
Three overall conceptual approaches were used to guide HWC based on Welter and colleagues’ findings to support cross-sectoral PSE initiatives: action learning, technical assistance (TA), and transformative skill building. Action learning is known as a capacity building process to facilitate a diverse team of individuals such as health and labor sectors to undertake problem-solving that results in systems change (Marquardt et al., 2009). TA to support systems change has begun to show progress (Asada et al., 2019) and involves both process and content components (Le et al., 2016). In the HWC, TA occurred in two ways: (a) labor sector activists were paid to share content expertise on PE as well as to support transformative skill building process expertise (e.g., power analysis; Bonney et al., 2020); and (b) University researchers provided process TA to help facilitate action learning (Bonney et al., 2019).
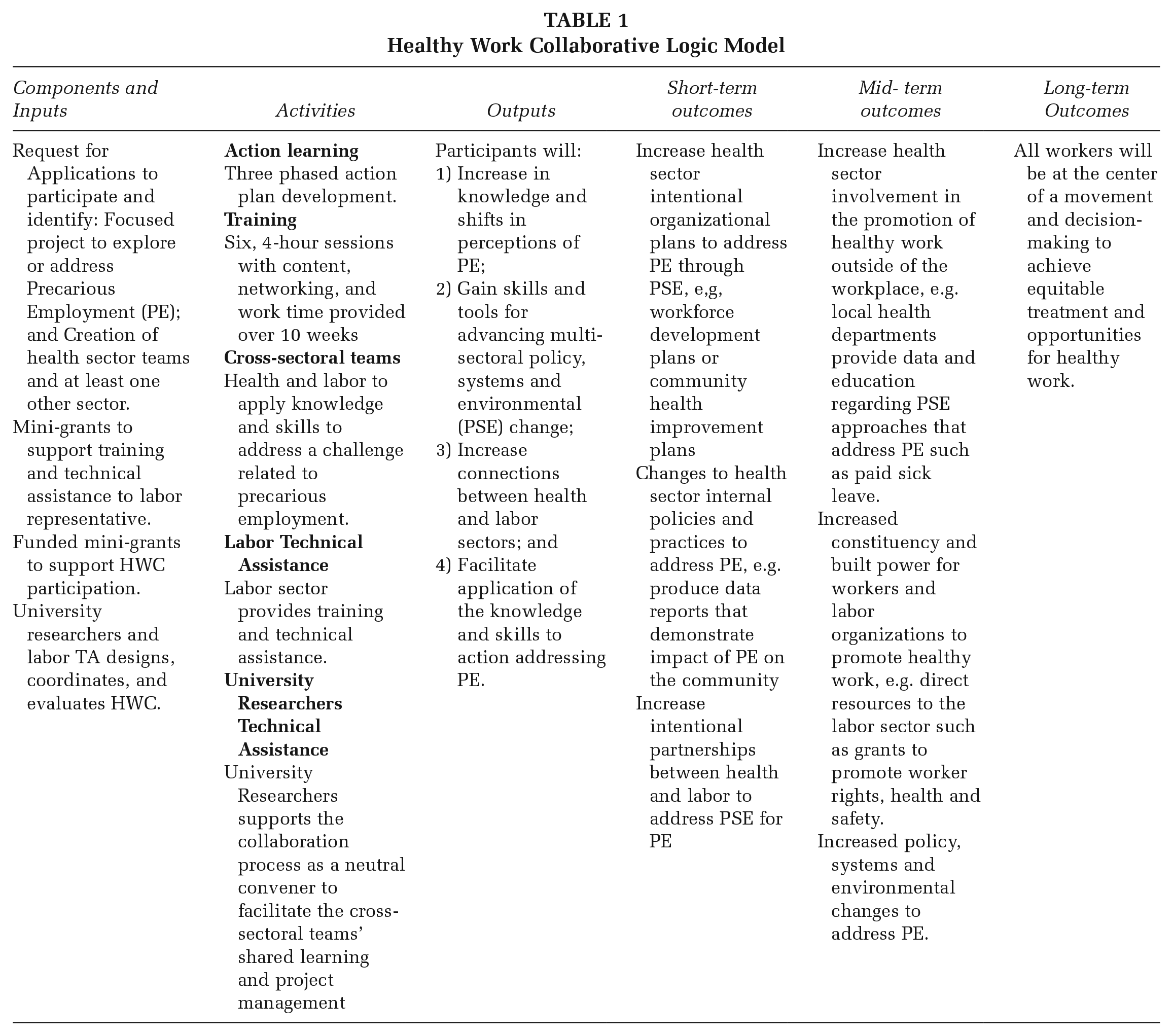
Given this conceptual and theoretical basis, HWC had four goals for participants: (a) increase and shift perceptions of PE, (b) gain skills and tools for advancing multisectoral PSE, (c) increase connections between health and labor sectors, and (d) facilitate application of the knowledge and skills to action addressing PE. Health and labor cross-sectoral teams applied to participate in HWC with general projects and attend six, 4-hour interactive sessions more than 10 weeks to develop specific action plans addressing PE using PSE strategies. The HWC included three phases: (a) understanding the problem; (b) systems, strategies, and approaches; and (c) planning for action. Participants learned tools such as Rich Picture—a systems-thinking-based participatory modeling exercise (Checkland, 2000) in Phase 1; Power Analysis—a process for analyzing individual, group, organizational, and systems power and privilege (Power Analysis, Racial Equity Tools, n.d.) and Current State/Future State—an adapted strategic planning tool for action planning (Conner, 1993) in Phase 2; and Theory of Change—a planning and measurement tool used in complex contexts (Center for Theory of Change, Theory of Change Community, n.d.) in Phase 3. HWC has been described elsewhere in more depth (Bonney et al., 2019); Table 1 presents the HWC Logic Model.
Healthy Work Collaborative Logic Model
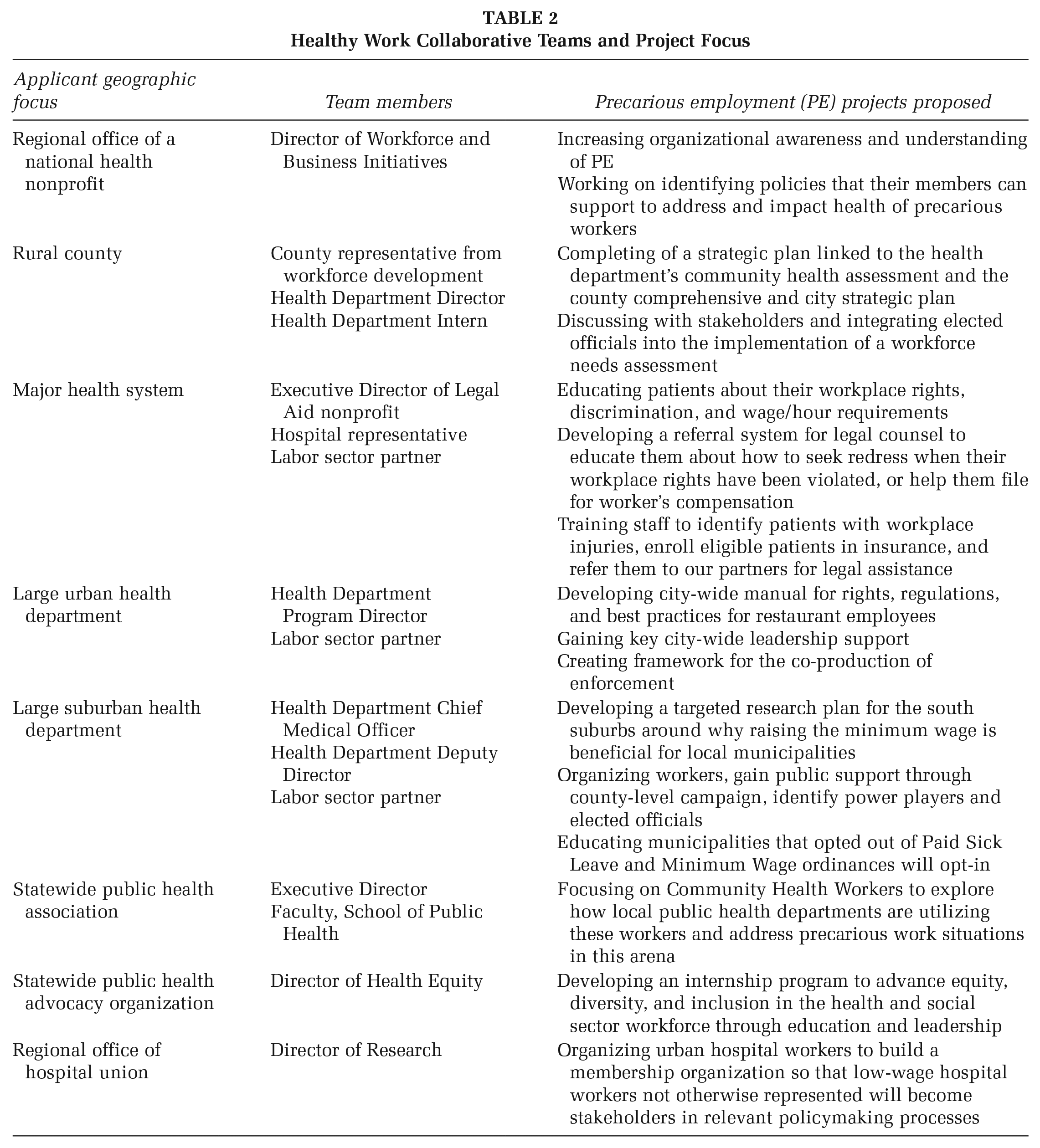
Eight teams with health and/or labor sector members participated in HWC from urban, suburban, rural, and statewide organizations within Illinois. Mini-grants of $1250 to $5250 were provided to the teams. University staff, faculty, and labor partners provided TA and skill building. Table 2 outlines HWC participant team membership and project areas. The purpose of this paper is to present evaluation findings and lessons learned from the HWC as one of the first health/labor collaborations addressing PE. Results report on whether and how HWC helped the participants build knowledge, skills, and abilities to address PE through PSE change.
Healthy Work Collaborative Teams and Project Focus
Method
HCHW conducted a mixed-methods evaluation of the HWC using the Kirkpatrick model to shape the evaluation design. The Kirkpatrick model presents four levels for evaluating training that increase in scope and impact of participants’ outcomes including reaction, learning, behavior, and results beyond the individual (Kirkpatrick & Kirkpatrick, 2006). Evaluation questions aligned with Kirkpatrick levels as follows: (K1) What were the experiences of participants in the HWC and how satisfied were participants with HWC curriculum and its delivery; (K2) What was learned: (a) How did participant perceptions about PE shift as a result of the HWC; (b) How useful were the tools provided; and (c) How have networks, relationships, connectivity, and communications changed, if at all, as a result of the process; (K3) How have participants applied lessons learned during the HWC; and (K4) How has the application of lessons learned influenced impact at the organizational level? This project was deemed exempt research by the Institutional Review Board of the University of Illinois Chicago (#2018-0370).
Survey Data
Participants were asked to complete a post-only close-ended questionnaire (Attachment A) with Likert-type response options to address questions of participant satisfaction (e.g., rated from strongly agree to strongly disagree) alongside their perceived usefulness of the HWC tools presented in each phase (e.g., rated each tool for knowledge of its existence, helpfulness in addressing the problem, application to work, request for more information, or not useful).
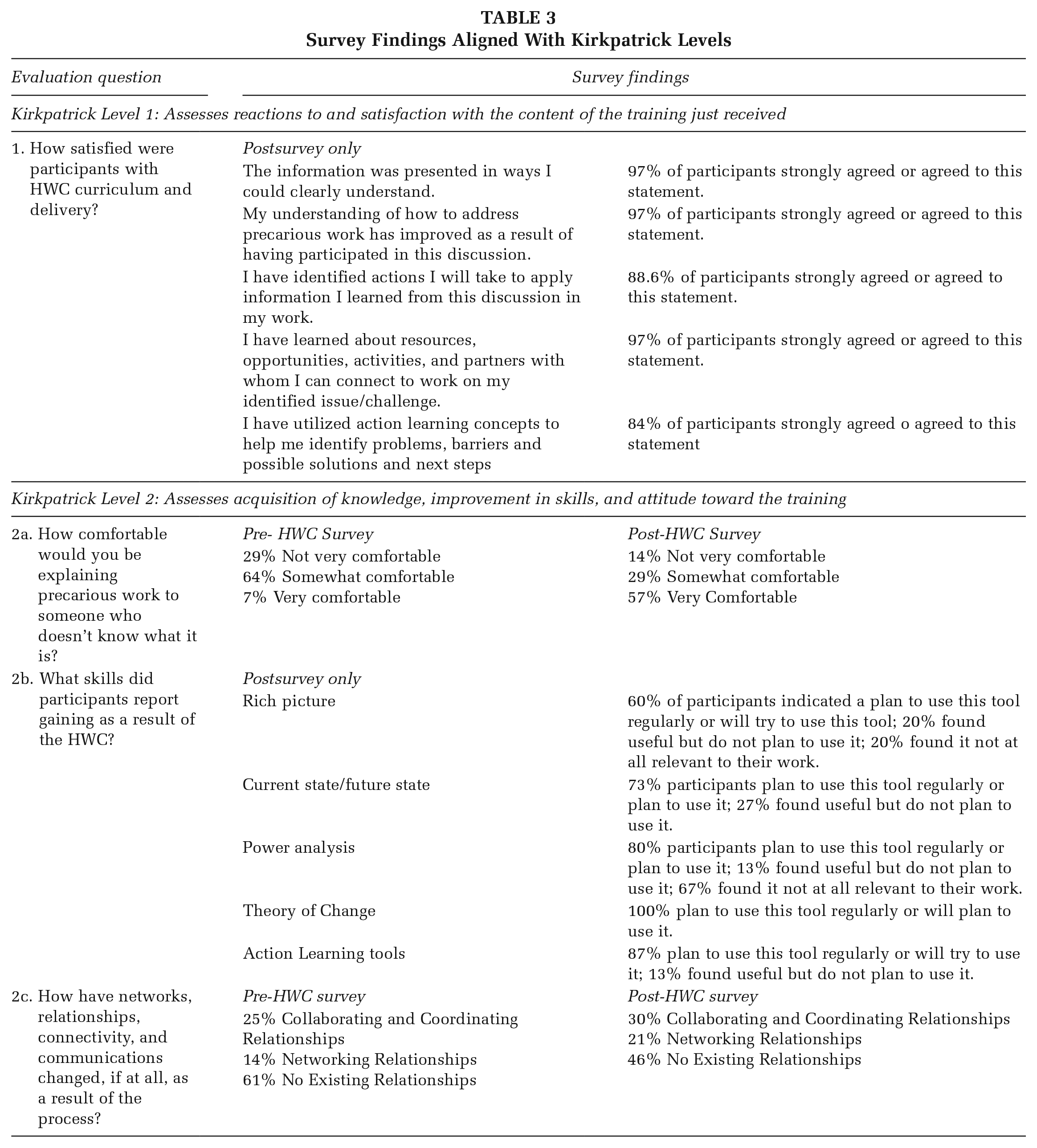
Participants also completed a pre–post survey immediately before and after the HWC’s first and last sessions, respectively, to assess how their perceptions of PE had shifted as a result of HWC (e.g., high familiarity, some familiarity, or no familiarity) and to explore how networks, relationships, connectivity, and communication (e.g., changes in strength of partnerships) may have changed as a result of HWC (Attachments B and C, respectively). Survey data were analyzed descriptively to address Kirkpatrick Levels 1 to 2 (Table 3) and inform the qualitative inquiry which informed all four Kirkpatrick levels (Table 4).
Survey Findings Aligned With Kirkpatrick Levels
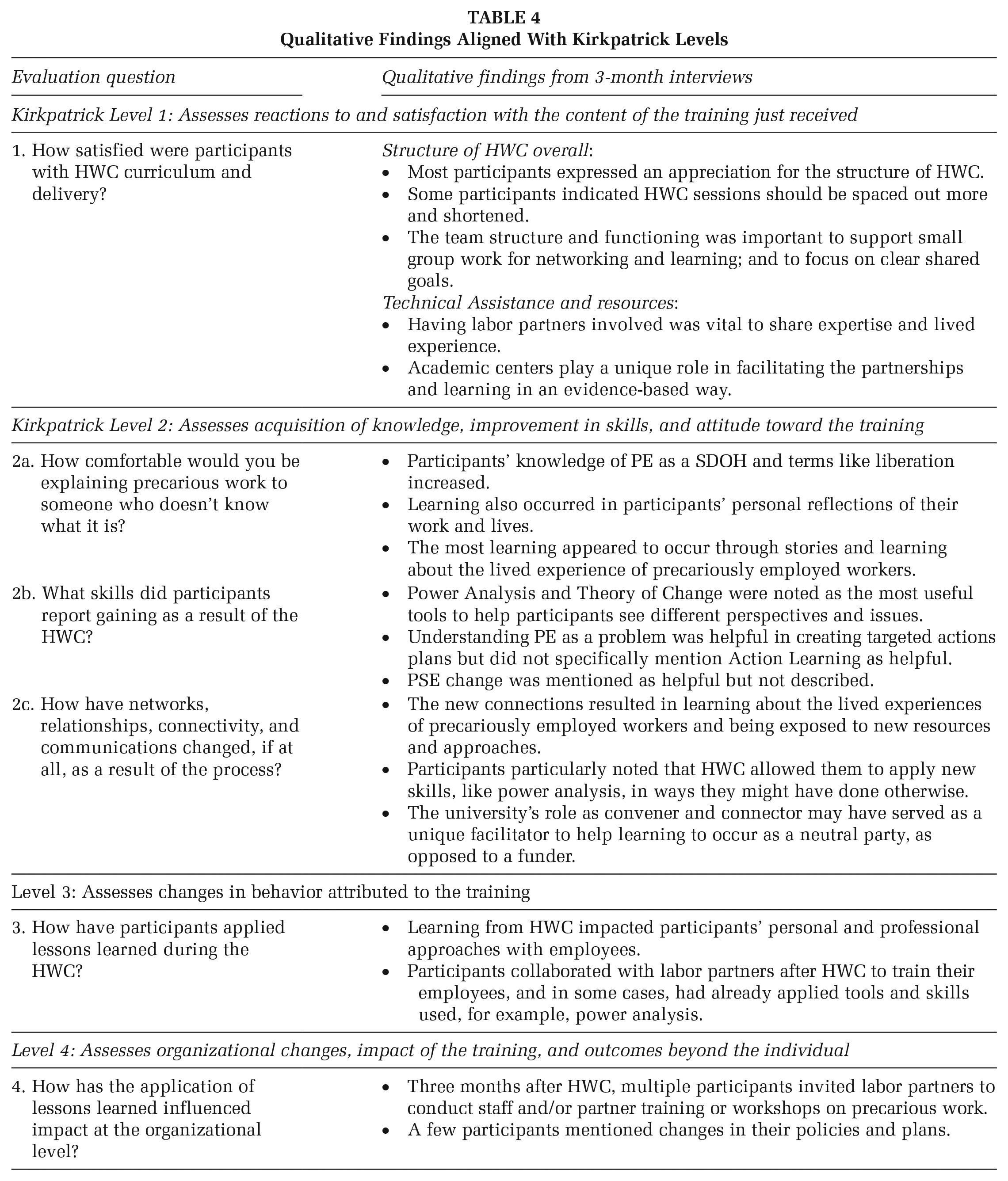
Qualitative Findings Aligned With Kirkpatrick Levels
Qualitative Data
Approximately 3 months after the completion of the HWC, participants were invited to participate in qualitative telephone interviews to assess evaluation Questions 1 to 4 (Attachment D). In addition, one TA labor partner who joined a participant team was also asked to participate in a qualitative telephone interview. Telephone versus in-person interviews were offered to increase participation rates due to resource limitations including time and travel costs. Interviews were recorded with permission and lasted an average 60 minutes.
The university team conducted thematic analysis using a “hybrid” approach, combining deductive with inductive (grounded) approaches to coding (Brixey et al., 2007; Fereday & Muir-Cochrane, 2006). A codebook was developed based on the constructs identified from the literature that informed the development of HWC, including effective PSE factors such as change readiness and implementation (Kegler et al., 2015; Welter et al., 2019), action learning (Marquardt et al., 2009), partnership development (Freudenberg et al., 2015), and Kirkpatrick levels (Kirkpatrick & Kirkpatrick, 2006) plus emerging themes from the transcripts. Pairs of university team members hand-coded five similar transcripts for coding agreement, reaching 80% agreement after discussion about code interpretation. No changes to the codebook were made; however, additional examples of intended meaning were provided with examples of interview data. Next, one team member entered coded transcripts into Dedoose software (Version 8.0.35, Los Angeles, CA, 2018) for further analysis. The university team reviewed the coded text and collaboratively identified themes for each evaluation question based on coded segments and co-occurring codes.
Results
Tables 3 and 4 highlight survey and qualitative results, respectively. Sample characteristics and evaluation participation numbers can be found in Table 5. No HWC participant dropped out of the initiative; however, some participants did not participate in some aspects of the evaluation. Fifteen participants (71%) completed both pre- and postsurveys and 13 participants (59%), including one labor TA member who continued to engage with the health sector, completed the 3-month follow-up interview. Reasons reported for not finishing evaluation instruments included lack of time to participate in the evaluation process due to other urgent priorities. Notably, at least one representative of each project team completed a 3-month follow-up interview.
HWC Sample Characteristics and Participation in HWC Evaluation
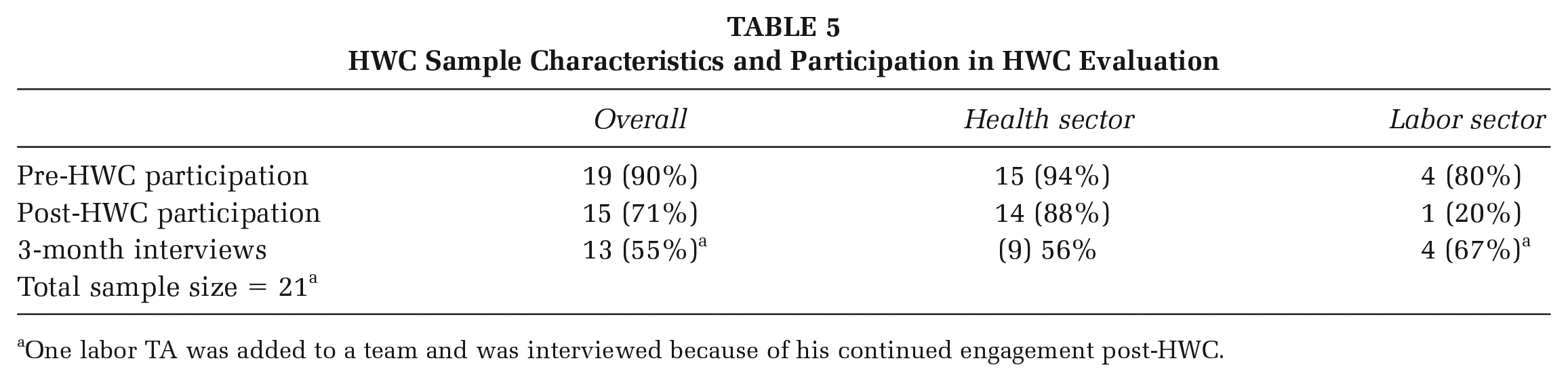
One labor TA was added to a team and was interviewed because of his continued engagement post-HWC.
What Were the Experiences and Reactions of Participants in the HWC?
Overall, HWC participants reported a high level of satisfaction with the HWC curriculum and its delivery. Ninety-seven percent of participants indicated they strongly agreed or agreed with satisfaction questions around clarity of the information, improvements in understanding PE, identifying actions to apply based on discussions, and learning resources from HWC. A slightly smaller percentage (84%) agreed that they used action learning concepts to identify problems, barriers, possible solutions, and next steps.
Three-month interviews revealed three aspects of HWC structure and design for improvement: operational structure, team structure and functioning, and the role of TA. Participant response regarding the operational structure (e.g., time/day of HWC, length of sessions, resources provided) was overwhelmingly positive with an appreciation for how HWC sessions were held over a 10-week timeframe with 2 to 3 weeks in-between sessions. Interestingly, some interviewees noted that while funds to participate were not substantial, it helped to justify their involvement.
Participants reported that team structure and functioning were important to the success of HWC. First, small group work allowed for intimate networking and learning about diverse perspectives. Second, having clear goals and a project to work on together helped focus collaboration efforts: “I think the importance of bringing people together from different sectors [is] to collaborate and work on projects with common goals.” Third, time together to dialogue helped to build trust and accountability with one another, which helped teams progress toward project goals. Participants noted that having additional time for dialogue (as opposed to other activities) would have been valuable.
Provision of both labor and university TA facilitated participant learning. Having labor sector TA partners with experience in organizing for policy change and direct involvement with workers in PE was vital. One participant noted, “It was also particularly helpful to get to know and see all of the resources that are sort of marshaled in this area . . . all the different, the technical assistance and all their different sort of worker centers.” Participants noted that the university’s role was also important because it facilitated the cross-sectoral relationships through the evidence-based design of HWC.
What Was Learned in the HWC?
Perceptions of PE
Most participants reported a shift in perception about PE. Participants were asked in the pre- and post-HWC survey about their comfort explaining PE to someone unfamiliar. Of the 15 complete pre–post survey responses, 50% reported an improvement in their ability to explain PE.
Three-month interviews also revealed that participants had increased knowledge and understanding of PE with an emphasis on improved understanding about the lived experience of workers. Some participants noted that they had not really thought about PE before: I had an absolute light bulb moment well like, “Of course work is a social determinant of health.” It was not something that I had really honestly considered that deeply and I was slightly embarrassed to feel like I was having a light bulb moment.
These reflections impacted the participants’ perceptions of their own work: I think the biggest thing that changed for me was remembering that precarious work disproportionately affects low wage workers, but to also not forget that so many other people are in precarious work situations too. I think that’s what I meant about being introspective to my own organization. How to make sure that I am not creating a precarious work environment here within my department, but also within the rural county.
Understanding the lived experience and impact on workers appeared to be one of the most impactful approaches to promote improved understanding of PE, such as a participatory theater exercise facilitated by worker-actors during the HWC.
Usefulness of HWC Tools
Most but not all participants found HWC tools useful. Postsurvey data asked about the usefulness of five tools explicitly shared during the HWC. For each tool, more participants indicated that the tool was more useful than not, with intentional plans to use it. Rich Picture was ranked the lowest for its usefulness, whereas Theory of Change was ranked highest.
Participants’ opinions of the most useful tools were consistent with the survey data. Power Analysis and Theory of Change tools appeared to help participants see different perspectives, partnerships, and issues more clearly and lay out causal aspects of the problem. One participant noted, So, I’d like to add [Theory of Change] into my strategic planning process when I go forward with different organizations. Mission, vision and values are historic pieces of strategic planning, but I hadn’t ever really thought about including a theory of change and getting a group to subscribe to that Theory of Change.
Changes in Network, Relationships, Connectivity, and Communication
HWC resulted in some increased and strengthened relationships. Participants were asked to rate their relationship with each participating organization as “no relationship,” a “networking relationship,” or as a “coordinating/collaborating relationship” in accordance with Himmelman’s relationship definitions (Himmelman, 2002). Participants reported a 53% increase in “networking” relationships and a 21% increase in “collaboration/coordination” relationships at the end of the HWC.
In 3-month interviews, many participants reported learning from the labor sector because their expertise was so different from their own. One participant said that sitting down and discussing those concepts with people around the room or in my group, that have expertise in areas that I do not have, where they are community organizers, and work day to day with immigrant workers or underemployed workers and things like that, that to me was what was the most useful.
Participants also noted learning about new approaches and resources to address PE in practice rather than theory: It’s not anything I wasn’t, haven’t been taught before, in a school setting, but I think the actual practice of thinking about the power analysis, and really trying to think through those stakeholders and what that means for your strategy.
How Have They Applied Lessons Learned During the Collaborative (K3)?
Participants noted personal and professional changes in their behavior after participating in HWC. Multiple participants noted that HWC helped them reflect on ways in which they employed and worked with people in their own lives. For example, one participant indicated, “I think that it made me a little bit more sensitive on a personal level around the people that I hire and support. My babysitters, the woman that cleans my house.”
This thinking applied to the workplace as well, as some participants reflected on their approaches at work: “. . . I took away some ideas for some of my own management and leadership style practices to make sure that I’m not creating a precarious work environment for my own employees.” This included new management approaches and acknowledging one’s power in the organization: I think there’s a lot to learn about just how to interact with employees and work on those power dynamics. Because I hold so much power here and sometimes when I open my mouth I need to remember that that goes along with it.
A few participants had already applied some of the skills learned: “We’ve used [power analysis] at State public health organization since [HWC], too.” Others indicated an intent to apply the skills, such as including a Theory of Change, in the next organizational strategic planning process.
How Has the Application of Lessons Learned Influenced Impact at the Organizational Level (K4)?
The long-term goal of HWC was for the health and labor sectors to partner together to advance PSE approaches in their organizations and communities that address PE. Three months after HWC, multiple participants invited labor partners to conduct staff and/or partner training or workshops on PE. Beyond training and education, one HWC team noted that “So this whole process allowed us to network and to even expand the project that we were doing [with a new Worker Center] and I think that came through because [of the Worker Center Director].”
A few participants mentioned changes in their policies and plans, such as revising an internship policy to be paid with widespread recruiting instead of only referral-based recruiting, changing the workforce development plan to address concepts learned in HWC, and applying for a grant to address PE. One project piloted a legal referral system to help workers to realize their rights.
Discussion
Evaluation data demonstrated that the HWC improved knowledge and shifted perceptions, introduced skills, and resulted in the application of learned PSE change tools to address PE. Findings suggest the HWC may be a model process for building knowledge, skills, and abilities to address the SDOH and serve as an example of how public health agencies and their partners can collaborate to address the structural and social determinants of health (DeSalvo et al., 2017; Freudenberg et al., 2015). We note several key findings that should be emphasized in future health promotion capacity building endeavors:
1) HWC participants frequently mentioned that learning about workers’ lived experiences through conversation and interactive exercises brought home PE’s impact on real lives. Others have documented that conveying the connections between lived experience and health is vital to community and systems health promotion approaches (Freudenberg et al., 2015; Smedley, 2012). Inclusion of the voices of communities experiencing PE or other structural determinants of health should be an important element in future health promotion initiatives addressing health equity.
2) Structured learning groups with a shared vision and project helped to focus the new partnerships toward cross-sector collaboration. In addition, having the time for reflection, dialogue, and ongoing application of the skills in real time to accomplish project goals appeared to improve learning and foster deeper partnerships. Most training in public health remains largely focused on knowledge building and technical problems. Others have called for more capacity building strategies to address systems change that support ongoing group learning over a defined period, such as action learning (Welter, Bekemeier, & McKeever, 2020).
3) TA and training about resources and community organizing approaches helped to visualize possible pathways for PSE change. While TA is well known for social service implementation (Le et al., 2016), there were few examples of TA from other sectors such as the labor sector and/or TA to promote PSE change before the HWC (Bonney et al., 2020).
Limitations
HWC participants represented a purposive sample of pre-existing partnerships whose involvement launched this collaborative and cross-sectoral project (Welter, Jarpe-Ratner, et al., 2020). Evaluation results may be skewed due to their above-average readiness to learn and address PE. In addition, there were incomplete data for several of the participants, primarily from labor partners who noted a lack of time to participate in data collection and need to focus on critical worker–centered policy campaigns. Furthermore, at least one labor partner opted out of the evaluation due to concerns over sharing organizing approaches more publicly.
Implications for Policy and Practice
There are several important lessons learned from HWC that health promotion experts and public health practitioners might consider in their efforts to address SDOH. First, HWC participants noted the importance of hearing from those with lived experience to understand the impact on health inequities on their lives. COVID-19 has illuminated this finding and the importance of understanding firsthand experiences and the impact of COVID-19 on precariously employed workers and their families. Worker voices highlight opportunities for public health agencies to intervene in ways that would have otherwise been unseen (e.g., paid-sick leave, lack of health and safety precautions, or wage violations). Second, many public health interventions focus on short-term individual skill building and behavior change. Addressing SDOH is a long-term endeavor; facilitating learning over time to apply skills, address real time challenges, and use action learning to promote dialogue, reflection, and learning may be a more impactful and long-lasting capacity building strategy. Third, public health is also somewhat new to addressing many SDOH using PSE—TA from sectors other than public health (e.g., labor sector) with more experience may be needed. Finally, PSE change takes time. HWC teams continued beyond the initial 10 weeks and at the time of this article continued to support PSE PE change and adapted their efforts to respond to COVID-19. In conclusion, this evaluation suggests that the HWC may provide health promotion practitioners an evidence-based framework to address SDOH like PE through PSE change.
Supplemental Material
sj-docx-1-hpp-10.1177_15248399211069099 – Supplemental material for Evaluation Results From the Healthy Work Collaborative: A Cross-Sectoral Capacity Building Partnership to Address Precarious Employment
Supplemental material, sj-docx-1-hpp-10.1177_15248399211069099 for Evaluation Results From the Healthy Work Collaborative: A Cross-Sectoral Capacity Building Partnership to Address Precarious Employment by Christina Welter, Elizabeth Jarpe-Ratner, Tessa Bonney, Eve Pinsker, Elizabeth Fisher, Nandini Deb, Anna Yankelev, Devangna Kapadia, Marsha Love and Joseph Zanoni in Health Promotion Practice
Supplemental Material
sj-docx-2-hpp-10.1177_15248399211069099 – Supplemental material for Evaluation Results From the Healthy Work Collaborative: A Cross-Sectoral Capacity Building Partnership to Address Precarious Employment
Supplemental material, sj-docx-2-hpp-10.1177_15248399211069099 for Evaluation Results From the Healthy Work Collaborative: A Cross-Sectoral Capacity Building Partnership to Address Precarious Employment by Christina Welter, Elizabeth Jarpe-Ratner, Tessa Bonney, Eve Pinsker, Elizabeth Fisher, Nandini Deb, Anna Yankelev, Devangna Kapadia, Marsha Love and Joseph Zanoni in Health Promotion Practice
Supplemental Material
sj-docx-3-hpp-10.1177_15248399211069099 – Supplemental material for Evaluation Results From the Healthy Work Collaborative: A Cross-Sectoral Capacity Building Partnership to Address Precarious Employment
Supplemental material, sj-docx-3-hpp-10.1177_15248399211069099 for Evaluation Results From the Healthy Work Collaborative: A Cross-Sectoral Capacity Building Partnership to Address Precarious Employment by Christina Welter, Elizabeth Jarpe-Ratner, Tessa Bonney, Eve Pinsker, Elizabeth Fisher, Nandini Deb, Anna Yankelev, Devangna Kapadia, Marsha Love and Joseph Zanoni in Health Promotion Practice
Supplemental Material
sj-docx-4-hpp-10.1177_15248399211069099 – Supplemental material for Evaluation Results From the Healthy Work Collaborative: A Cross-Sectoral Capacity Building Partnership to Address Precarious Employment
Supplemental material, sj-docx-4-hpp-10.1177_15248399211069099 for Evaluation Results From the Healthy Work Collaborative: A Cross-Sectoral Capacity Building Partnership to Address Precarious Employment by Christina Welter, Elizabeth Jarpe-Ratner, Tessa Bonney, Eve Pinsker, Elizabeth Fisher, Nandini Deb, Anna Yankelev, Devangna Kapadia, Marsha Love and Joseph Zanoni in Health Promotion Practice
Footnotes
Authors’ Note:
The authors wish to acknowledge the study participants and participants of the Healthy Work Collaborative for their contributions to this article and its impact. Funding for this project was through the University of Illinois at Chicago (UIC) Center for Healthy Work, a National Institute for Occupational Safety and Health Center of Excellence for Total Worker Health® (Grant: U19OH010154). The views expressed in written materials do not necessarily reflect the official policies of the Department of Health and Human Services, nor does the mention of trade names, commercial practices, or organizations imply endorsement by the U.S. Government. Total Worker Health is a registered trademark of the U.S. Department of Health and Human Services (HHS). Participation by the UIC Center for Healthy Work does not imply endorsement by HHS, the Centers for Disease Control and Prevention, or the National Institute for Occupational Safety and Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.