
Abstract
Colorectal cancer (CRC) disparities continue to persist in the four corners region (states of New Mexico, Arizona, Utah, and Colorado) of the United States. The Comprehensive Cancer Control (CCC) state plans provide a policy and practice snapshot on how a state identifies and addresses its cancer burden. This study critically examines the four state plans to identify gaps and opportunities for cancer prevention and control. Using a conventional content analysis approach, we reviewed the CCC plans for CRC screening-related information, culminating in a conceptual framework that highlights three themes. First, states reported their cancer burden using national data from American Cancer Society, Centers for Disease Control and Prevention, or the NCI’s Surveillance, Epidemiology, and End Results. Although these data informed specific goals and objectives, not all plans reported state-level data on CRC differences by specific social determinants of health and other characteristics. Second, it was not clear whether the interventions chosen to address state plan objectives were evidence-based and whether or not clearly described criteria were used for the selection of the interventions. Third, very limited information was provided in terms of state-specific contextual challenges and practical implementation of interventions. Study findings highlight opportunities to improve state-level cancer prevention and control efforts: first, by promoting the selection and adaptation of contextually relevant evidence-based interventions for this unique region; and second, through multidirectional engagement with communities, researchers, and policy and practice stakeholders. Such synergies in research and policies are vital for a coordinated and integrated approach to cancer prevention and control.
Keywords
Cancer disparities persist in the four corners region of the United States, which consists of New Mexico (NM), Arizona (AZ), Utah (UT), and Colorado (CO). Compared with the national profile, the four corners region is home to larger Hispanic and American Indian (AI) communities, and smaller Black and Asian communities (see Table 1; https://statecancerprofiles.cancer.gov/). For instance, NM has 12 times the number of AIs as the national average, while one sixth the number of Black Americans. Similarly, poverty rates in the four corners region tend to outpace the national average, particularly in NM and AZ. Such communities often have disparate access to cancer screening modalities and manifest disproportionate cancer burden.
Population Characteristics in the Four Corners Region of the United States, as Percentages of Total Population
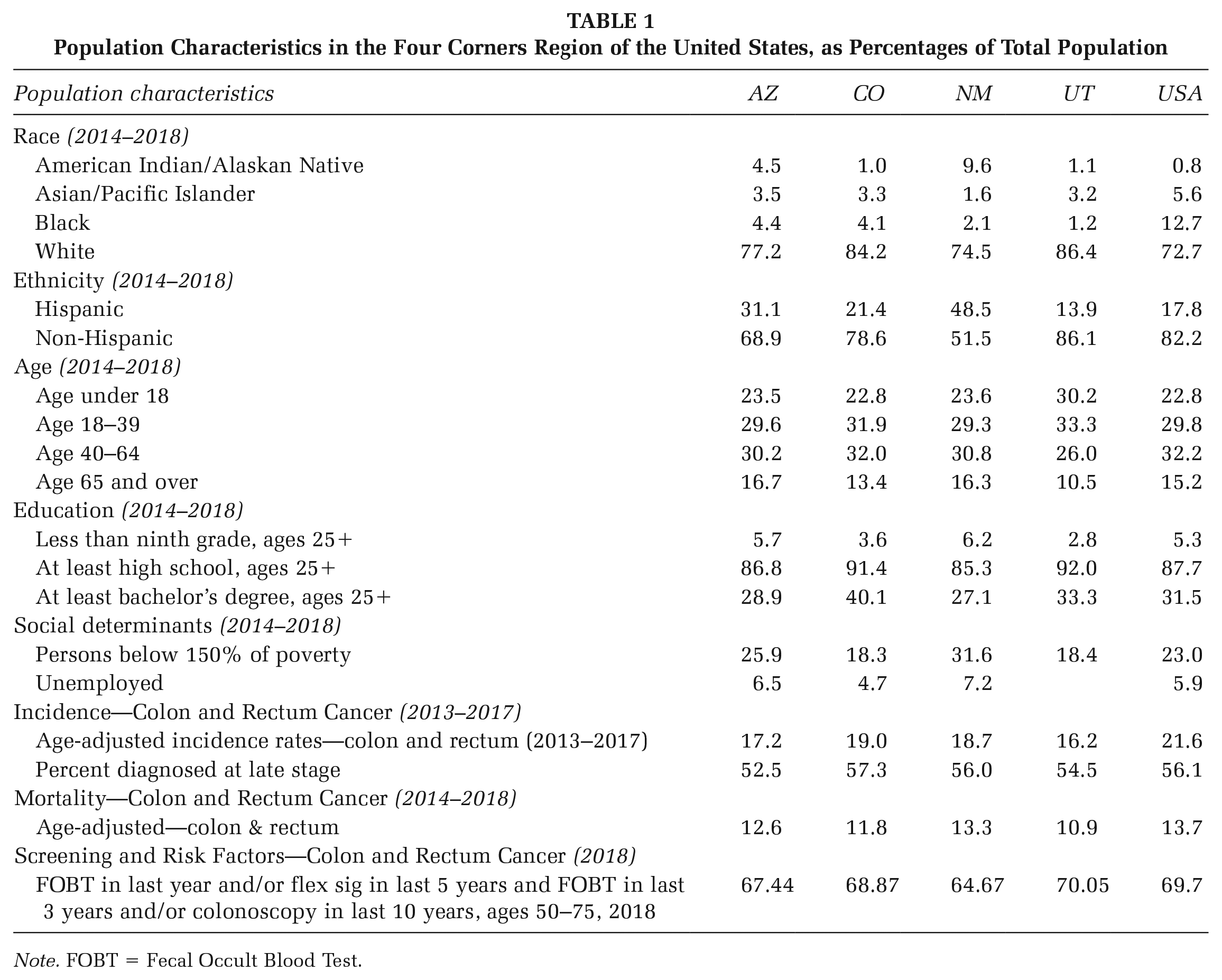
Note. FOBT = Fecal Occult Blood Test.
For colorectal cancer (CRC), these disparities are stark. Hispanics and AIs are often less likely to be screened for CRC and, as a result, tend to be diagnosed at later stages and have lower survival rates than non-Hispanic Whites (Gonzales et al., 2012). Specifically, AI populations have the lowest survival rates for nearly all types of cancer of any subpopulation in the United States, with cancers often detected at later stages (Gonzales et al., 2012). Compared with non-Hispanic Whites, Hispanics are also more likely to be diagnosed with advanced stages of disease and experience poor quality of life following a cancer diagnosis (Yanez et al., 2016). The intersection with rural residence (Zahnd et al., 2021), socioeconomic status (Aloysius et al., 2021), and health care delivery access (Adjei et al., 2021) can further exacerbate these disparities.
Supported by the Centers for Disease Control and Prevention (CDC), Comprehensive Cancer Control (CCC) state plans provide an important policy strategy for how a state identifies and addresses its cancer burden. It reflects the breadth of cancer prevention and control activities undertaken in a state along with set goals and objectives, which can serve as crucial means to coordinate and prioritize efforts. For the past decade, CDC has funded state-level cancer coalitions to develop these plans every 5 years and encouraged the use of evidence-based interventions (EBIs) and programs to address the cancer burden, in addition to information on how to implement EBIs. The purpose of this article was to critically examine the four corners state plans specific to CRC prevention and control.
Method
This study implemented conventional content analysis of publicly available (https://www.cdc.gov/cancer/ncccp/ccc_plans.htm) CCC plans for each of the four corner states (AZ, 2014–2018; CO, 2016–2020; NM, 2012–2017; UT, 2012–2017). Content analysis is an inductive coding approach to qualitative analysis that allows researchers to describe phenomena (Hsieh & Shannon, 2005). We began by conducting key word searches for relevant terms, including “colorectal,” “colon,” “colonoscopy,” “FIT,” “fecal immunochemical test,” “FOBT,” “fecal occult blood test,” “sigmoidoscopy,” and “polyp.” Following this, relevant text adjacent to these key words was extracted to NVivo (qualitative analysis software) to provide context for their usage. The Cancer Plan Index (CPI) served as an initial reference in the development of the coding guide (Rochester et al., 2011), as it has been used by state officials to create CCC plans. Two team members trained in qualitative analysis coded each of these selections from one state plan independently to identify additional or specific concepts. The team members met to discuss these concepts and operationalize the coding guide (see Online Supplement). Relying on the coding guide, one team member (J.R.) coded the remaining two state plans and a second team member (P.A.) independently reviewed approximately 20% of the excerpts to check for alignment. The two analysts resolved coding disagreements in one-on-one meetings, with changes made to operational definitions in the coding guide, if needed. Both analysts reviewed the coded excerpts together in one-on-one meetings and summarized the key findings and relationships within codes while referencing the coding guide. This collective and reflective process led to distinguishing three key conceptual themes that emerged from these data and are presented below.
Results
Each state plan ranked CRC as the fourth most common cancer by incidence rate for their respective state and second or third in terms of mortality.
Limited Data Presented in Terms of the Influence of Social Determinants of Health on CRC and Health Services Data Regarding CRC Screening
States provided differing details beyond the benchmark statistics of incidence and mortality. NM and AZ provided differences by gender (i.e., men and women) in CRC incidence and mortality rates. In AZ, CRC was the fourth most commonly diagnosed cancer among women and the third most common cause of cancer death among men. The NM plan did not provide specific statistics for CRC, but rather offered rankings of cancer deaths in the state for men and women. CO highlighted differences among racial/ethnic groups. UT provided no additional CRC data for specific population subgroups. All four state plans cited CRC data from their respective cancer registries (AZ Cancer Registry, CO Central Cancer Registry and Vital Statistics, UT Cancer Registry, and NM Tumor Registry).
Each of the four state plans we reviewed provided some CRC screening data. Three states (CO, NM, and UT) collected these data from a common source, the Behavioral Risk Factor Surveillance System (BRFSS), whereas the fourth state, AZ, provided screening statistics from the Arizona Department of Health Services that was specific to their state’s clinics and programs. With regard to disparities, two of the four state plans reviewed, CO and UT, presented statistics detailing screening rates among population subgroups distinguished by socioeconomic status, rural residence, education level, and race and ethnicity. The NM and AZ plans published no such information. The NM plan noted that the BRFSS screening data were compiled in collaboration with the NM Department of Health.
Information Regarding the Selection, Adaptation, and Implementation of EBIs Was Missing From State Plans
All four state plans included goals and objectives specifically related to CRC. The AZ plan included seven discrete CRC objectives, whereas NM included three. The CO and UT plans did not include CRC in any objective statement; rather, each addressed CRC in “strategies” (CO) or “action steps” (UT) to achieve more general cancer prevention and control goals. Three of four state plans (AZ, CO, and UT) included specific EBIs, activities, or strategies that relate to CRC. NM was the only plan that did not include such specifics.
Although three states (AZ, CO, and UT) selectively stated specific EBIs, activities, and strategies to achieve goals and objectives, they did not always provide the original source or how they were selected by the state. AZ cited the Evaluation of Genomic Applications in Practice and Prevention recommendations to support its objective to increase genetic counseling and testing when appropriate for CRC at-risk individuals. The AZ plan also cited CDC guidelines in reference to its objective to decrease the time from abnormal detection to definitive diagnosis of CRC. The CO plan cited the National Colorectal Cancer Roundtable’s efforts to standardize family history data collection in electronic health records (EHRs) to support its objective to do the same. The UT plan explicitly aligned its goal to “increase the number of Utahns who receive recommended cancer screenings” to the CDC’s 2013 document “Increasing Colorectal Cancer Screening: An Action Guide for Working With Health Systems.”
State Cancer Plans Acknowledged Partnerships and Policies Critical to Their Plan’s Development or Implementation, Yet Provided Limited Details About Contextual Challenges and Practical Implementation of Interventions
All four state plans cited collaboration with a CRC “work group,” “roundtable,” or “task force” in some capacity for the development of the CCC plan. There was no mention of academic partnerships in the CO, NM, or UT plans as they related to CRC content, with AZ as an exception. In this case, the Survivorship and QoL (Quality of Life) Action Team collaborated with the University of North Carolina to adapt the national survivorship care plan survey to AZ. Three of four state plans did not reference public–private partnerships with regard to CRC. The exception was UT’s plan, which cited the work the Huntsman Cancer Institute (HCI) and Intermountain Healthcare (a regional nonprofit health care system) have done to institute tumor screening protocols to assess for Lynch syndrome in all colon cancers.
There was limited discussion of contextual challenges and facilitators related to CRC screening in the four state plans. Three of the four state plans (AZ, NM, and UT) included some relevant content. The AZ plan cited lack of federal funding for CRC screening as a challenge. The NM plan cited the lack of access to CRC screening stool cards among providers in AI communities. The UT plan highlighted three points regarding CRC that serve as contextual challenges: (a) those living in frontier areas have lower rates of CRC screening than those living in other areas of the state; (b) CRC screening rates are significantly higher among those with higher income and education levels; and (c) Pacific Islanders, Hispanics, Asians, and AI in UT have lower rates of CRC screening compared with the others in the state. The UT plan provided statistics to underscore such disparities in the state. The CO plan included no discussion of contextual challenges and facilitators related to CRC. Three of the four state plans (AZ, CO, and UT) made no specific mention of CRC in their implementation plans.
Discussion and Implications
These data collectively contribute to the conceptualization of how state plans inform the policy and practice around cancer prevention and control in the state. Guided by the gaps identified in this article, we highlight in Figure 1 the opportunities for future policy, research, and practice (shown in italics) within each critical aspect of cancer prevention and control planning and implementation.
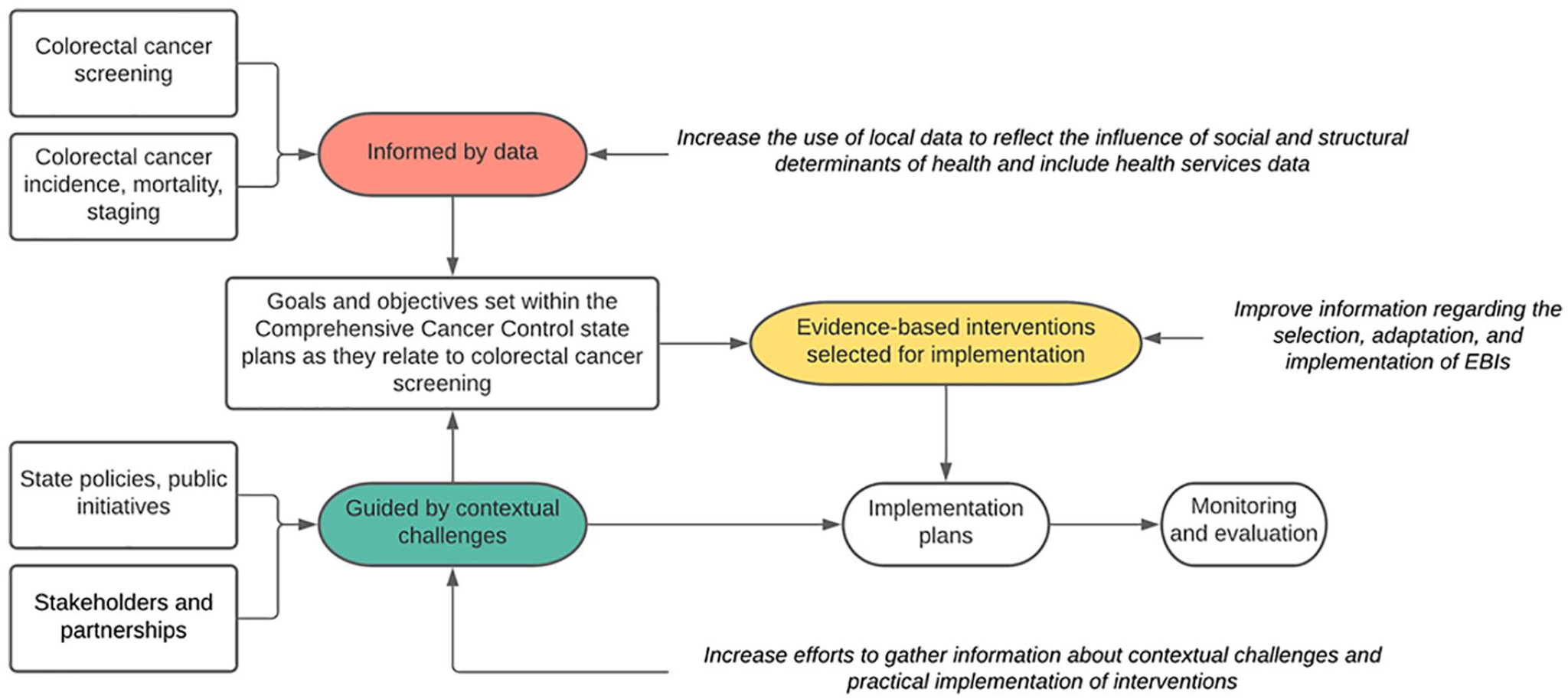
Highlighted Opportunities for Improving Cancer Prevention and Control Through State-Level Cancer Plans
Our review indicates limited data on population-level disparities both in terms of CRC statistics and screening-specific data within the CCC plans. Specifically, they did not provide CRC incidence, mortality, and screening data by socioeconomic status, race/ethnicity, gender, and other characteristics. We believe these data to be critical to highlight specific disparities among and between population subgroups to describe needs that can be addressed by goals and objectives outlined in the plan. As such, CCC plans should incorporate data from relevant sources such as the Uniform Data Systems by the Health Resources and Services Administration, Health Information National Trends Survey, and the National Health Interview Survey, for specific information regarding population-level screening outcomes.
However, it is also critical to identify and select EBIs that support the specified goals and objectives in CCC plans. In our review, state plans inconsistently cited the source of the selected EBIs or how they were selected or identified as important for achieving the goals and objectives related to CRC. Growing number of repositories like the Evidence-Based Cancer Control Programs and Community Guide, among others, can support the selection of EBIs and thereby, the science of adaptations (Alvidrez et al., 2019) and selection of implementation strategies (Powell et al., 2019) which can inform implementation at the state level. Similar to data and EBI gaps described above, the limited information around challenges and facilitators to implementation, disconnects identification of the problem from selection of the proposed solution. Describing and addressing contextual challenges in state plans through the use of implementation theories, methods, and measures can promote the integration of research into routine clinical and community practice. Furthermore, collaborative synergies in research and policies are vital for a coordinated and integrated approach to cancer prevention and control (Hayes et al., 2018).
We acknowledge the limitations of this work in that only four state plans were reviewed and that some of the states may have revised these goals and objectives in more recent state plans since our analysis began. However, we believe that even with a limited sample, the critical examination of CCC plans helped us identify crucial opportunities for cancer prevention and control that are relevant across the United States. Foremost, they highlight opportunities for scientists engaged in public health, cancer prevention, and implementation science to work together and leverage the coordinated and far-reaching platform that these plans provide.
Supplemental Material
sj-docx-1-hpp-10.1177_15248399211073803 – Supplemental material for Improving Comprehensive Cancer Control State Plans for Colorectal Cancer Screening in the Four Corners Region of the United States
Supplemental material, sj-docx-1-hpp-10.1177_15248399211073803 for Improving Comprehensive Cancer Control State Plans for Colorectal Cancer Screening in the Four Corners Region of the United States by Joseph Rodman, Shiraz I. Mishra and Prajakta Adsul in Health Promotion Practice
Footnotes
Authors’ Note:
This research was partially supported by (1) grant from the New Mexico Department of Health: FY21UNM 021102 and FY22UNM 021102, and (2) UNM Comprehensive Cancer Center Support Grant NCI P30CA118100 and the services of the Behavioral Measurement and Population Sciences (BMPS) Shared Resource. All authors declare no conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.