
Abstract
There are persistent disparities in the delivery of cancer treatment, with Black patients receiving fewer of the recommended cancer treatment cycles than their White counterparts on average. To enhance racial equity in cancer care, innovative methods that apply antiracist principles to health promotion interventions are needed. The parent study for the current analysis, the Accountability for Cancer Care through Undoing Racism and Equity (ACCURE) intervention, was a system-change intervention that successfully eliminated the Black–White disparity in cancer treatment completion among patients with early-stage breast and lung cancer. The intervention included specially trained nurse navigators who leveraged real-time data to follow-up with patients during their treatment journeys. Community and academic research partners conducted thematic analysis on all clinical notes (n = 3,251) written by ACCURE navigators after each contact with patients in the specialized navigation arm (n = 162). Analysis was informed by transparency and accountability, principles adapted from the antiracist resource Undoing Racism and determined as barriers to treatment completion through prior research that informed ACCURE. We identified six themes in the navigator notes that demonstrated enhanced accountability of the care system to patient needs. Underlying these themes was a process of enhanced data transparency that allowed navigators to provide tailored patient support. Themes include (1) patient-centered advocacy, (2) addressing system barriers to care, (3) connection to resources, (4) re-engaging patients after lapsed treatment, (5) addressing symptoms and side effects, and (6) emotional support. Future interventions should incorporate transparency and accountability mechanisms and examine the impact on racial equity in cancer care.
Background
Racial disparities in cancer outcomes between Black and White patients are persistent. Although cancer mortality rates in the United States have declined overall, Black Americans continue to receive fewer cancer treatment cycles than White Americans (Harrison et al., 2022; Wolf et al., 2019), contributing to higher cancer death rates among Black patients (Jatoi et al., 2022; O’Keefe et al., 2015). Decades of research has demonstrated that Black patients with cancer tend to receive less chemotherapy than White patients and are more likely to discontinue treatment before receiving the recommended dose (Hershman et al., 2005; Wolf et al., 2019). A 2018 meta-analysis found that Black patients with breast cancer were more likely than White patients to experience delays in treatment initiation of 90 days or more (Green et al., 2018). Furthermore, there is evidence that Black breast cancer patients are more likely to receive a suboptimal dose of adjuvant therapies (e.g., radiation, chemotherapy, or hormonal therapy) than White patients, even when controlling for factors such as neighborhood socioeconomic deprivation, age at diagnosis, cancer stage, and tumor size (Cho et al., 2021). Among patients with localized lung cancer, Black patients have lower 5-year survival rates than White patients (Bade & Cruz, 2020). Numerous studies have documented that unequal rates of lung cancer treatment and disparities in treatment delivery among Black and White patients play a role in survival rate differences (Elliott et al., 2022; Evans III et al., 2021; Taioli & Flores, 2017).
Today, there is a need for research that closely examines cancer care systems to better understand how organizational factors contribute to creating and maintaining racial disparities, and, in turn, how system-level interventions could work to improve care quality and reduce treatment disparities. Nurse navigation is a care system approach and an effective strategy to improve the quality of cancer care (Cobran et al., 2017; Kline et al., 2019; Rawther et al., 2018). A central tenant of oncology navigation is to provide patients with tailored support to facilitate care engagement as they undergo cancer treatment (McMullen, 2013). Initially developed by Dr. Harold Freeman in Harlem, New York, in 1990 to address racial disparities in breast cancer screening and biopsy (Freeman & Rodriguez, 2011), navigation has been adopted and implemented in numerous health care systems across the United States, as evidenced by several systematic reviews (Baik et al., 2016; Jojola et al., 2017; Robinson-White et al., 2010). Navigation programs vary across contexts (Cantril & Haylock, 2013), with navigator tasks encompassing a range of support activities such as assisting with treatment plans, care coordination, referral to social services, educating patients about medications and side effects, and providing emotional support (Wells et al., 2018).
Among cancer patients, navigation can lead to more positive care experiences and fewer care-related problems (Kline et al., 2019). Navigation has also been shown to reduce surgery wait times for breast cancer patients (Baliski et al., 2014; Rohsig et al., 2019) and reduce the time from suspicion of cancer on a chest X-ray to treatment initiation among lung cancer patients (Kunos et al., 2015; Shusted et al., 2019). Qualitative research findings show that navigation provides patients with both emotional and logistical support needed to engage with a fragmented and confusing cancer care system (Carroll et al., 2010) and positively impacts patients’ sense of agency and ability to take action on matters related to their health care (Hudson et al., 2019).
Researchers have long argued that, conceptually, nurse navigation is an appropriate strategy to address health care disparities because in the navigation model, patients who might otherwise fall through the cracks of a complex and fragmented health care system received individualized support to remain engaged in treatment (Bone et al., 2013; Moy & Chabner, 2011; Natale-Pereira et al., 2011). In a recent review, Dixit and colleagues (2021, p. 4) described navigators as “a relational bridge, connecting disenfranchised patients to complex networks and processes of cancer care system.” Navigation programs have been effective in reducing racial disparities in rates of cancer screening (Grubbs et al., 2013; Marshall et al., 2016), but there are limited studies evaluating associations between navigation and equitable care across racial identity groups (Cykert et al., 2020). To better understand whether nurse navigation could be an effective strategy to address racial disparities in cancer treatment, research into the specific characteristics of nurse navigation that improve care quality is needed. By examining nurse navigation through an antiracism lens, researchers can identify features of system-wide navigation programs that may have a significant impact on reducing racial disparities in cancer treatment outcomes.
Eliminating Cancer Care Disparities: The ACCURE Intervention
This study examines social support provided by nurse navigators within the context of the Accountability for Cancer Care through Undoing Racism and Equity (ACCURE) intervention. ACCURE was a multicomponent study that successfully eliminated the disparity in treatment completion between Black and White early-stage breast and lung cancer patients at two cancer centers: Cone Health Cancer Center in Greensboro, NC, and University of Pittsburgh Medical Center’s Hillman Cancer Center in Pittsburgh, PA (Cykert et al., 2020). Study enrollment took place from April 2013 to March 2015. Prior to ACCURE, 79.8% of Black patients completed treatment compared with 87.3% of White patients; after implementation of ACCURE, treatment completion increased to 88.4% for Black patients and 89.5% for White patients (Cykert et al., 2020). ACCURE was developed by the Greensboro Health Disparities Collaborative (GHDC), a community-academic-medical center partnership that aims to address racial disparities in health care through applied research. GHDC integrates a community-based participatory research (CBPR) approach, where community partners are equitably involved with decision-making at each phase of the research project (Schaal et al., 2016), with antiracism principles to inform and guide its work (Yonas et al., 2006).
Antiracism Principles Guiding ACCURE
The intervention was the first health services quality improvement effort to operationalize principles from Undoing Racism, an antiracism organizing model. These principles (Table 1) were developed by the People’s Institute for Survival and Beyond, a collective of antiracism organizers and educators based in New Orleans, LA (The People’s Institute for Survival and Beyond, 2018).
Undoing Racism Organizing Principles
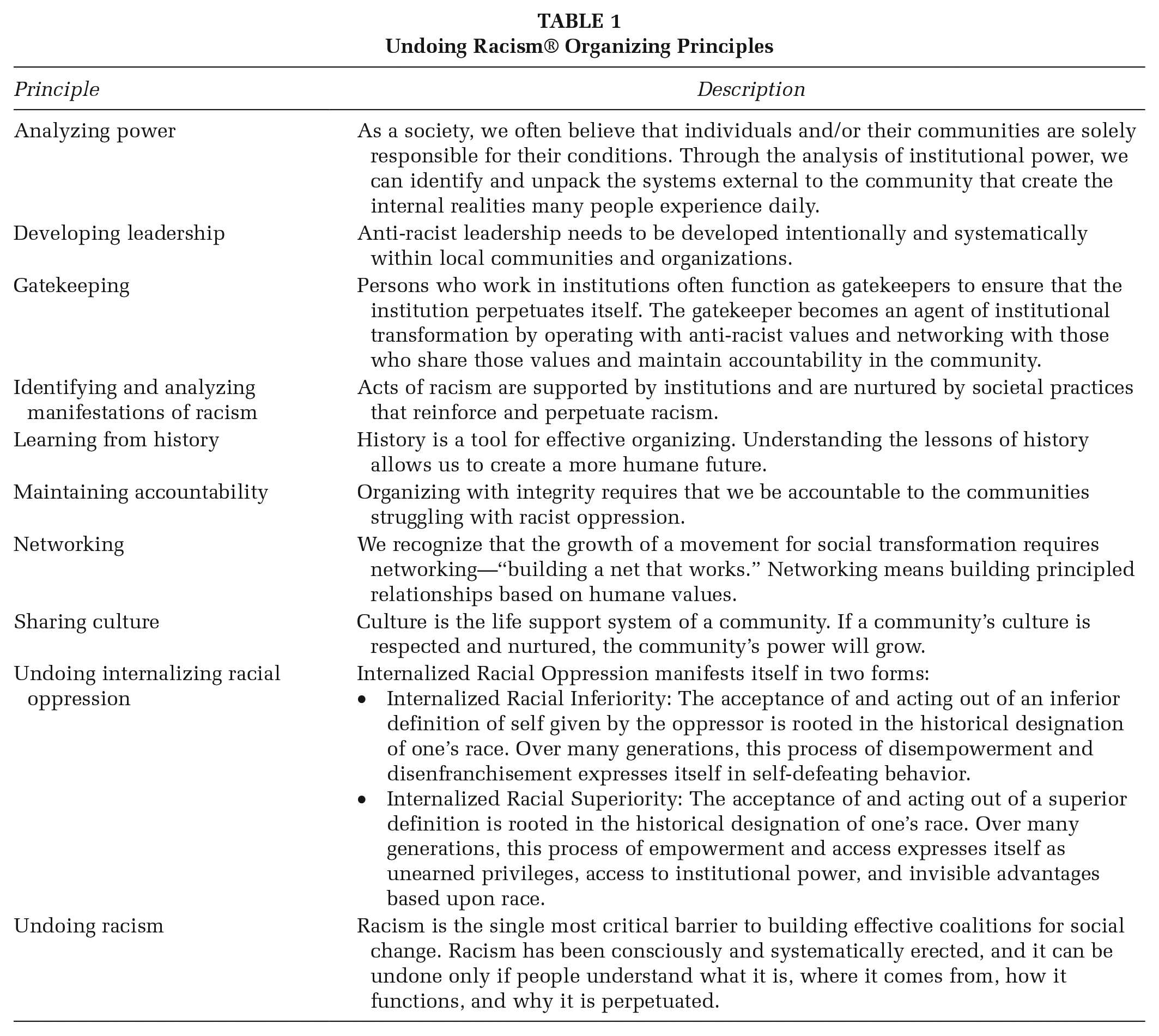
Two key Undoing Racism principles that informed the development of ACCURE were analyzing power and maintaining accountability. ACCURE was developed as a system-level intervention to address (a) lack of transparency in race-based and timely data about cancer treatment outcomes and (b) accountability in equity of cancer care and completion within a cancer center. These priorities were identified through our prior research with Black and White breast cancer survivors, Cancer Care and Racial Equity Study (CCARES) (Yonas et al., 2013).
Reviewing CCARES findings with our GHDC partners involved in-depth discussions about how power operated in the cancer care system, and in turn, what strategies might disrupt institutional processes that maintained and reinforced inequities in care quality. Findings from CCARES suggested that increasing transparency on multiple levels was essential, for example, increasing data transparency so cancer center providers and administrators were aware of care inequities in real time, and enhancing transparency in treatment protocols so cancer patients had clear information and the opportunity to participate in treatment decisions that impacted their lives. To develop the ACCURE intervention to test these strategies, we expanded GHDC to engage cancer center partners in addition to community and academic researchers (Eng et al., 2017). As part of our formative research in ACCURE, we conducted focus groups with cancer survivors, in Undoing Racism terms “an analysis of power and authority,” to identify “pressure point encounters” in patients’ cancer treatment where they felt discouraged or encouraged to continue their care and identify—from their perspective—ways to increase transparency and accountability in the cancer care system (Black et al., 2021; Eng et al., 2017).
This prior formative work following the Undoing Racism principle of analyzing power led GHDC to focus on transparency as a key principle in its approach to racial equity interventions. With these foundations, ACCURE operationalized transparency and the Undoing Racism concept of maintaining accountability through intervention components at the community, organizational, and interpersonal levels, described in detail elsewhere (Baker et al., 2021, Cykert et al., 2020). For the present analysis, we focused on ACCURE’s nurse navigation which was conceptualized as an accountability intervention component. At the organizational level, a data system called the Real-Time Registry enhanced data transparency around racial inequities in care quality and treatment protocols by connecting providers with real-time data disaggregated by patient race. ACCURE navigators leveraged data transparency to provide interpersonal-level support to patients through a process of two-way communication. ACCURE navigators also enhanced accountability of the care system to patient needs by proactively following up with patients to address barriers to treatment completion. Details of the navigation component are described below.
ACCURE’s Nurse Navigation
One navigator at each study site received training in antiracism and proactive engagement protocols. ACCURE navigators were required to attend a 2-day antiracism training with the Racial Equity Institute (Greensboro, NC) to provide educational grounding in the historically-rooted systems of oppression that continue to have implications for the unequal treatment of people of color today (Largent, 2018). Navigators also completed training modules led by ACCURE research staff. The content of the modules included training on the teach-back method, which involves navigators describing treatment protocols in accessible language and asking the patient to restate the information in their own words to ensure understanding. This method allows navigators to assess patients’ comprehension of the information presented, and then give further clarification and education as needed. It is a simple yet effective strategy that can help mitigate patient-provider communication challenges due to variation in patients’ health literacy (Scott et al., 2019). The ACCURE navigator training also covered Kleinman’s Patient Model which guides providers to develop an understanding of patients’ perspective on their illness by asking eight questions (see Supplemental Content) (Kleinman et al., 1978). Navigators were also given a proactive communication protocol with a schedule for patient follow-up (full protocol provided in Supplemental Content). If a patient missed a scheduled procedure or appointment, navigators were notified through the Real-Time Registry, a digital warning system linked to the electronic health record. Navigators then followed up with patients to assess barriers to continuing treatment and provide support. After each patient contact, navigators logged a note in the study’s digital database, documenting the content of what was discussed with the patient. Nurse navigator notes were downloaded from the database, converted to text files, and deidentified of any patient information. The research team conducted a qualitative analysis on the notes to examine the mechanisms of support provided by ACCURE navigators in the context of an equity-focused quality improvement intervention. Each site’s navigator was certified as key research personnel and study procedures received full board review and were approved by each site’s Institutional Review Board.
Purpose
We aimed to examine how ACCURE’s nurse navigation component contributed to the overall success of the intervention in eliminating the racial disparity between Black and White patients in treatment completion for early-stage breast or lung cancer. We used an antiracism lens to examine how ACCURE’s Real-Time Registry worked in tandem with navigation to enhance transparency and accountability in the care system. The present analysis did not stratify the sample by race, and instead examined navigator support among both racial groups represented in the ACCURE sample. Although a race-based comparison in navigator support is an important topic for future research, the present analysis is focused on first examining the link between specialized navigation, the principles of transparency and accountability, and quality improvement in the delivery of cancer care.
Methods
This study examines clinical notes (n = 3,251) written by ACCURE navigators (one navigator at each site) documenting their interactions with participants randomized to receive ACCURE navigation (n = 162). We engaged in a collaborative analytic process involving GHDC community, academic, and medical research partners.
Eight GHDC community and academic research partners conducted thematic analysis (Clarke et al., 2015) on notes digitally entered by ACCURE navigators after each patient contact. The unit of analysis was each individual note as documented by the navigators. The team coded the text using a codebook of 22 codes developed through collaborative review of the ACCURE navigator notes (Table 2). Most of the codes were developed a priori and covered topics such as barriers to care, means of support, and psychosocial factors such as family hardship—topics anticipated to be addressed by navigators. Several codes were developed during the analysis through iterative review among community, academic, and medical center team members, a process used in ACCURE previously and described elsewhere (Schaal et al., 2016). Once the codebook was finalized, the transcripts were divided among analysts and independently coded. Multiple codes could be applied to each note.
Codebook
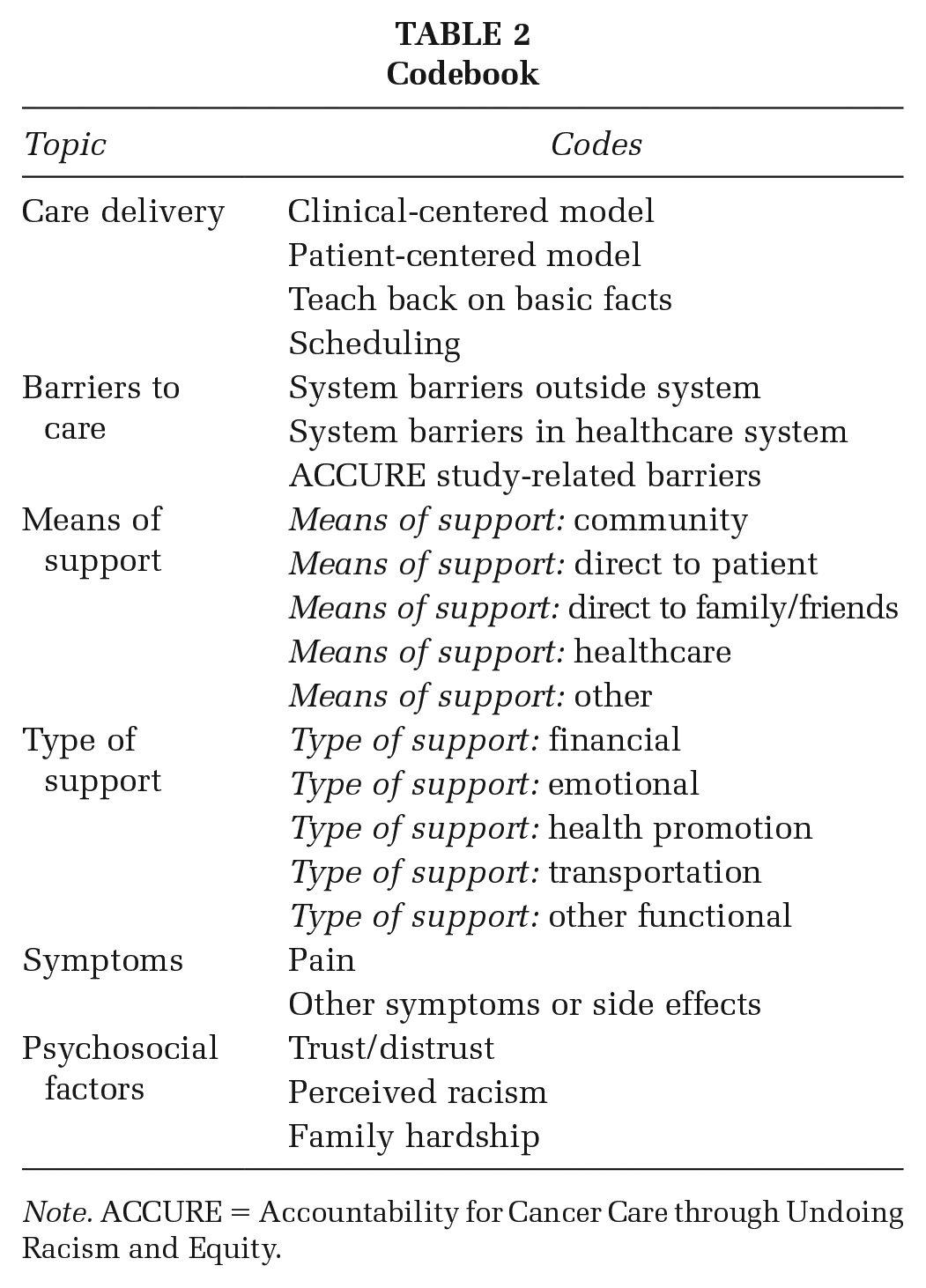
Note. ACCURE = Accountability for Cancer Care through Undoing Racism and Equity.
The next phase of analysis involved the first author, who was not involved in the initial coding process, reviewing the coded transcripts and organizing the codes into themes. Theme development was guided by the antiracism principles of transparency and accountability. The first author applied these principles to the analysis by grouping codes into themes that pertained to transparency in care protocols and treatment decisions and accountability of the care system to patient needs. The fourth author (who was also independent from the initial coding process) reviewed the coded navigator notes data and contributed to theme formation at this stage. The final phase of analysis involved collaborative review of the themes by the first, second, third, and last authors, the latter three of whom were ACCURE Principal and Co-Investigators.
Results
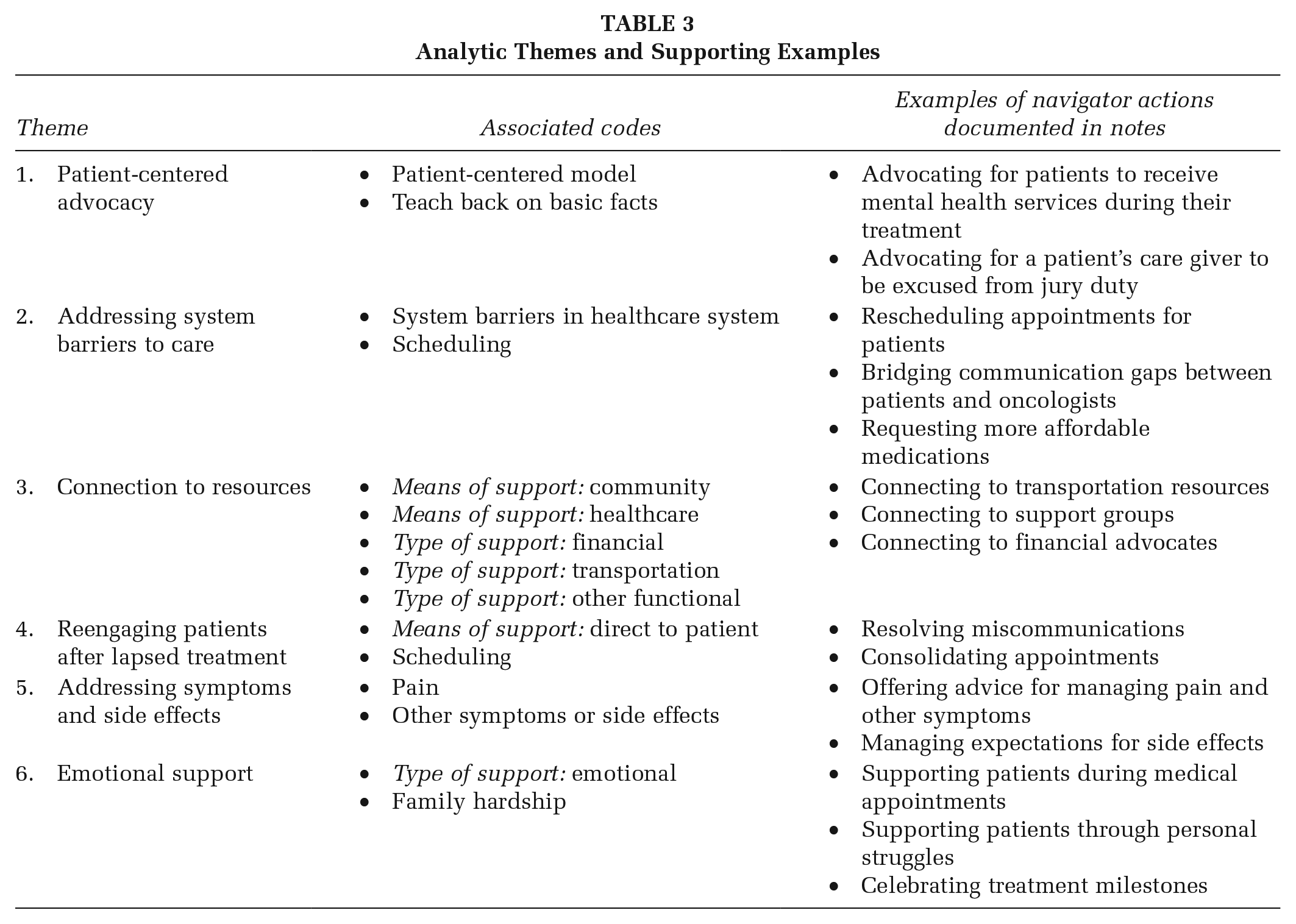
Codes were grouped into six themes. Themes were initially categorized as pertaining to either transparency or accountability. Further discussion with senior members of the study team led to a more nuanced interpretation of the role of transparency and accountability in the ACCURE navigation component. Transparency was identified as an underlying mechanism that was operationalized through ACCURE’s Real-Time Registry, which was integral to ACCURE’s navigation program. The Registry created data transparency by flagging deviations from standards of care and funneling that information to navigators, who could then provide tailored follow-up to support patients in their treatment journeys. The Real-Time Registry was a system-level intervention component, which directly influenced the navigators’ interpersonal-level patient support. The navigation component of ACCURE enhanced accountability of the care system to patient needs. This accountability was made possible by patient-specific data from the Real-Time Registry. The six themes identified in our analysis describe the specific ways in which ACCURE navigators enhanced accountability in the cancer care system. The themes include (1) Patient-centered advocacy, (2) Addressing system-level barriers to care, (3) Connection to resources, (4) Reengaging patients after lapsed treatment, (5) Addressing symptoms and side effects, and (6) Emotional support. The themes, associated codes, and examples from the navigator notes are presented in Table 3. Each theme is discussed below with supporting quotations from the notes.
Analytic Themes and Supporting Examples
Theme 1. Patient-Centered Advocacy
The patient-centered advocacy theme encompassed notes that documented navigators enhancing two-way communication and intervening in the care system on behalf of patients’ needs. One note documented the navigator advocating for a patient’s preference for a female mental health care provider: “Her [primary care provider] made an appt with a counselor, but he is male and she said she requested a female. I told her I would cancel that appt and attempt to schedule with a female counselor prior to her surgery.” This note exemplifies enhanced accountability as the navigator clarified and advocated for the patient’s preference.
In other instances, navigators advocated for patients by supporting needs related to factors outside the care system. One note documented the navigator helping a patient obtain a doctor’s note to give to her employer when requesting a modified work schedule. Another note documented the navigator advocating for a patient’s primary support person to be excused from jury duty: “Patient called and shared that her husband has been summoned for [jury duty]. She is dependent on him for all transportation to her appointments and procedures and she requested that I send a letter stating that she is under our care and requesting that he be excused . . .” A later note stated that the patient called to let the navigator know that the request was received and her husband had been excused. Nurse navigation allowed for the care system to support patients’ needs regarding external factors affecting their treatment.
Theme 2. Addressing System-Level Barriers to Care
Navigators routinely assisted patients in handling systemic issues that presented barriers to their care. One form of this support was when navigators assisted patients with scheduling treatment appointments. Navigators checked in with patients about scheduling or rescheduling appointments and incorporated their scheduling needs into the system. One note stated, “[Patient] expressed frustration that she had tried to call to change her appointment and has not been able to speak to someone. I told her that I would send a request to reschedule her appointment.” Here, the navigator addressed a scheduling barrier experienced by the patient and alleviated some of her burden.
Navigators also addressed system barriers to care by closing gaps in communication to ensure that patients’ health information was up to date with various providers. For example, in one note the navigator wrote, “Patient called stating that the [primary care provider] that manages her care has not received results of the latest bloodwork that she had drawn at our facility. Requested that I fax those results—successfully completed.” Navigators also addressed cost barriers by requesting more affordable medications be prescribed to patients when they heard from patients that cost was an issue. A note stated, “Patient called because she heard from her pharmacy that her newly prescribed Aromasin will cost ~US$400. She asked if there was anything more cost effective. I discussed with [doctor] who will prescribe Letrozole . . .” The navigator communicated with the provider on the patient’s behalf, demonstrating enhanced accountability of the care system to patient needs.
Theme 3. Connection to Resources
For patients struggling due to lack of basic needs, the navigator connected them to resources such as support groups and financial assistance. Navigators also documented linking patients to local transportation resources, for example, a navigator wrote, “I gave her information on [a local transportation service] for assistance to come to her appointments.” Other notes described navigators’ efforts to connect patients with resources to alleviate the financial burden of treatment. For example, one note stated, “Patient has started a new job and there has been a lapse in her insurance premium payments, and she requested assistance to pay her premium. I discussed with the financial advocate who will call patient with instructions.” Navigators linked patients with financial advocates and assisted with applications for financial assistance. These examples demonstrate enhanced accountability in the care system by connecting patients with resources to help them remain engaged in care.
Theme 4. Reengaging Patients After Lapsed Treatment
Navigators, who received alerts for missed appointments from the Real-Time Registry, reached out to patients to understand the reason for lapsed treatment and to help troubleshoot barriers to care engagement. For example, one note described a miscommunication between a patient and the care provider that the navigator helped resolve: “I called patient to check in and [follow-up] on missed appointment with [her doctor]. Patient thought her appointment was for the same day as her scheduled mammogram. I . . . spoke to [a nurse] who will call patient to reschedule her appointment.”
Another note described a reengagement process where a patient expressed a need for appointments to be consolidated, which the navigator communicated back to the care team: “Patient did not show for her chemotherapy treatment. I called patient and she said that she just couldn’t get here this morning . . . We talked about the importance of rescheduling her chemotherapy appointment and she requested that it be scheduled so that her chemo and radiation therapy appointments follow each other because she cannot tolerate being out for long periods of time due to her respiratory limitations. I discussed with [nurse] who notified [the] scheduling [office] to reschedule her treatment.” Navigators following up with patients after missed appointments created more accountability in the system to patients’ needs, making it easier for patients to reengage with care.
Theme 5. Addressing Symptoms and Side Effects
Navigators supported patients by offering advice in pain and symptom management. For example, one note regarding a patient stated: “[Patient] is experiencing some fatigue. We talked about increasing her activity to increase her energy level. We reviewed what to expect with radiation therapy.” Navigators also provided patients with information to help them manage expectations around medication side effects and reiterated the purpose of the medication, as documented in this note, “. . . Patient called because she had her prescription for Arimidex filled and had read the possible side effects and is afraid to start the medication . . . We discussed the most common side effects and that many patients experience no side effects. We discussed that her physician will monitor her side effects. We also talked about why she was prescribed Arimidex and how it is important to help prevent a recurrence of breast cancer.” These findings are consistent with evidence from prior research documenting the importance of enhanced accountability in symptom management and education within the cancer care system (Samuel et al., 2018).
Theme 6. Emotional Support
Navigators were available to talk and listen to patients during moments of emotional distress due to concerns about their treatment or from other hardships affecting their care. One note describes the navigator providing emotional support to a patient during a medical appointment: “. . . met [patient] upon arrival for [medical oncology] visit . . . [patient] quietly cried, [doctor] and I consoled her, validated her emotions and inquired on thoughts/questions.” Navigators also provided emotional support to patients during moments of celebration in their cancer journey. One cancer center in the study has a tradition of inviting patients to ring a bell after their last chemotherapy or radiation treatment. The navigator wrote about supporting a patient during this ritual: “Patient at [cancer center] for final radiation therapy treatment, accompanied by her sister. I met with patient to celebrate with her as she rang the bell.” These notes exemplify the unique role these nurses played in being accountable to patients and offering tailored support through the challenges and celebrations in their treatment journeys.
Discussion
The ACCURE intervention implemented specially trained nurse navigators who provided patient support and advocacy through targeted follow-up informed by a real-time digital alert system. The Real-Time Registry also gave ACCURE navigators access to treatment data that were disaggregated by patient race. By implementing the Real-Time Registry and linking it to patient navigation, ACCURE transformed systems of care at the two intervention sites. Navigators were able to track patients’ treatment progress, remain attuned to discrepancies in care engagement by patient race, and proactively engage both patients and providers to ensure all patients received timely and appropriate care. Without the system-level component of a real-time alert system to enhance data transparency, something as seemingly simple as a scheduling error can disrupt a patient’s life and make it more difficult for them get the care they need. In ACCURE, the Real-Time Registry enhanced data transparency and gave navigators access to the information they needed to track gaps in treatment and follow-up with patients to facilitate care engagement.
Navigators also enhanced care-system accountability to patients by connecting them with useful resources and addressing their concerns regarding symptoms and side effects. For example, navigators helped patients understand what to expect when taking hormone therapy medications, provided them with education around their treatment team’s rationale for using certain treatments, and supported them in managing side effects. In addition, navigators connected with patients on a personal level by offering emotional support throughout their treatment journeys. These support strategies bolstered two-way communication between patients and the care system, and enhanced accountability of the care system to patient needs. ACCURE operationalized the Undoing Racism principle of maintaining accountability to communities by implementing data-informed navigation. As a whole, the ACCURE intervention worked to disrupt status-quo processes that reproduce racial inequities, creating a system that succeeded in eliminating the Black–White racial disparity in care completion. ACCURE is one example in a growing literature that documents and advocates for community-engaged strategies to effectively leverage health informatics to advance health equity (Brewer et al., 2020; Carney & Kong, 2017; Oh et al., 2016).
While grant funding for ACCURE has ended, the intervention transformed the two cancer centers involved with the study in several ways. One site has committed a budget and information technology personnel to extend ACCURE’s Real-Time Registry to other cancers. After learning from ACCURE that electronic health record data on patient race and ethnicity were sometimes missing or not always correct, Senior Vice President for the health system mandated new training for all in-take personnel on how to ask each patient, respectfully, to indicate their race and ethnicity. In addition, all cancer navigators are now required to complete antiracism training. Breast cancer navigators now remain with the same patient until they complete chemotherapy, whereas before ACCURE, breast cancer navigators stopped contacting patients when they began chemotherapy. The other study site has hired additional nurse navigators in several areas and has implemented diversity, equity and inclusion mandated education for oncology providers. They have also hired additional Black staff including two ambassadors and a clinical research coordinator. This has resulted in increased clinical trial participation among Black patients and has improved patient satisfaction. ACCURE created a foundation of antiracist care practices at system and interpersonal levels, which in turn prompted transformation in the cancer centers that extend beyond the initial study’s intervention components.
Strengths and Limitations
The strengths of this study include ACCURE’s community-based participatory approach, which created accountability in the research process to community members who are directly impacted by racial disparities in the cancer care system. Community input strengthened this research by ensuring antiracism was centered throughout the analytic process. Another strength is the novel application of the antiracism principles of transparency and accountability to a qualitative analysis of navigator support. This analysis draws from GHDC’s previous work identifying transparency and accountability as key mechanisms to disrupt institutional racism (Black et al., 2021; Eng et al., 2017). However, we recognize that the focus on these two principles may have constrained the analytic approach. Future research should examine other Undoing Racism principles that could bolster system-change efforts in to enhance equity in health care. Another limitation of this study is that it does not provide a race-based analysis of ACCURE navigator notes to examine differences in support for Black and White patients that may have contributed to the overall intervention’s success in eliminating care completion disparities (Cykert et al., 2020). The results presented provide initial evidence for specialized navigation as an avenue to enhance transparency and accountability in the care system and improve care quality.
Implications for Research and Practice
ACCURE demonstrated the transformative potential of multilevel intervention strategies involving (a) data systems that enhance transparency around care quality metrics, disaggregated by patient race, and (b) navigators who leverage data transparency to enhance care system accountability to patients through tailored support. Future research should apply these intervention strategies in other settings, develop metrics (quantitative or qualitative) to measure transparency and accountability in health promotion interventions, and examine links between transparency and accountability measures and improvements in racial equity in care outcomes. Future research should also continue to explore how Undoing Racism principles can be operationalized in health services research to advance racial equity in health care.
Supplemental Material
sj-docx-1-hpp-10.1177_15248399221136534 – Supplemental material for Examining ACCURE’s Nurse Navigation Through an Antiracist Lens: Transparency and Accountability in Cancer Care
Supplemental material, sj-docx-1-hpp-10.1177_15248399221136534 for Examining ACCURE’s Nurse Navigation Through an Antiracist Lens: Transparency and Accountability in Cancer Care by Ida Griesemer, Alexandra F. Lightfoot, Eugenia Eng, Claire Bosire, Fatima Guerrab, Amanda Kotey, Kimberly M. Alexander, Stephanie Baker, Kristin Z. Black, Crystal Dixon, Katrina R. Ellis, Karen Foley, Christina Goettsch, Antionette Moore, Cleo A. Ryals, Beth Smith, Christina Yongue, Samuel Cykert and Linda B. Robertson in Health Promotion Practice
Supplemental Material
sj-docx-2-hpp-10.1177_15248399221136534 – Supplemental material for Examining ACCURE’s Nurse Navigation Through an Antiracist Lens: Transparency and Accountability in Cancer Care
Supplemental material, sj-docx-2-hpp-10.1177_15248399221136534 for Examining ACCURE’s Nurse Navigation Through an Antiracist Lens: Transparency and Accountability in Cancer Care by Ida Griesemer, Alexandra F. Lightfoot, Eugenia Eng, Claire Bosire, Fatima Guerrab, Amanda Kotey, Kimberly M. Alexander, Stephanie Baker, Kristin Z. Black, Crystal Dixon, Katrina R. Ellis, Karen Foley, Christina Goettsch, Antionette Moore, Cleo A. Ryals, Beth Smith, Christina Yongue, Samuel Cykert and Linda B. Robertson in Health Promotion Practice
Footnotes
Authors’ Note:
Fatima Guerrab is now affiliated to Community- Campus Partnerships for Health, Raleigh, NC, USA. Antionette Moore is now affiliated to Bethune-Cookman University, Daytona Beach, FL, USA. Cleo A. Ryals is also affiliated to Flatiron Health, New York, NY, USA. This research was supported by the National Cancer Institute (Grant Nos. 1R01CA150980-01A1 [PIs S. Cykert and E. Eng] and 1K01CA218473-01A1 [for C.A. Ryals]), the Cancer Health Disparities Training Grant from the National Cancer Institute (Grant No. T32-CA128582 [for C. Bosire]), and a National Research Service Award Pre-Doctoral Traineeship from the Agency for Health care Research and Quality sponsored by The Cecil G. Sheps Center for Health Services Research, The University of North Carolina at Chapel Hill (Grant No. T32-HS000032 [for I. Griesemer]). Writing of this manuscript was also supported by the Department of Veterans Affairs Office of Academic Affiliations Advanced Fellowship Program in Health Services Research, the Center for Health care Organization and Implementation Research (CHOIR), Boston, MA (for I. Griesemer). Conflict of Interest: The authors have no conflicts of interest to disclose.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.