
Abstract
Trust plays an integral part in the effective functioning of public health systems. During the COVID-19 pandemic, distrust of public health fueled vaccine hesitancy and created additional barriers to immunization. Although most Americans have received at least one COVID-19 vaccine, the percentage of fully immunized adults remains suboptimal. To reach vaccine-hesitant communities, it is vital that public health be worthy of trust. As trusted members of their communities, community health workers (CHWs) can serve as ideal messengers and conversation partners for vaccination decision-making. We developed the Be REAL framework and training materials to prepare CHWs to work with vaccine-hesitant communities nationwide. Through the four steps of “Relate,” “Explore,” “Assist,” and “Leave (the door open),” CHWs were taught to prioritize relationship building as a primary goal. In this shift from focusing on adherence to public health recommendations (e.g., get vaccinated) to building relationships, the value of vaccine uptake is secondary to the quality of the relationship being formed. The Be REAL framework facilitates CHWs harnessing the power they already possess. The goal of the Be REAL framework is to foster true partnership between CHWs and community members, which in turn can help increase trust in the broader public health system beyond adherence to a specific recommendation.
Assessment of Need
COVID-19 vaccination rates have slowed. While most adults have received at least one vaccine dose, a substantial proportion of adults remain under-vaccinated, particularly for bivalent boosters (Kaiser Family Foundation, 2023). Notably, vaccine attitudes have become more entrenched over time with adults who remain unvaccinated reporting less openness to vaccination now than at any earlier point in the pandemic (Kaiser Family Foundation, 2023). Many of these same adults report a heightened distrust of health institutions as a result of the pandemic (Pew Research Center, 2022). Distrust in health institutions is particularly problematic in communities disproportionately affected by discrimination and disinvestment, including majority Black, Latinx, and Tribal communities (Allen et al., 2022).
Maintaining herd immunity through vaccination requires an ongoing investment in communities, with an emphasis on bridging gaps in trust. To accomplish this, public health must reorient the way it approaches vaccination, replacing transactional encounters with deeper, sustained community relationships. As trusted members of their communities, community health workers (CHWs) are well positioned with the skills and the orientation this effort will require. We present Be REAL as a novel framework designed to empower CHWs to lead this charge, embracing public health relational practice.
Building Trust Through Relationships
Robust literature supports the importance of trust as a cornerstone of an effective public health system (Gille et al., 2017; Gilson, 2003; Siegrist, 2021). To bridge the gap between trust in individuals and trust in broader institutions, we pull from the work of Giddens and his notion of “facework” commitments (1990). In this conceptualization, individuals form trust in relationships with abstract institutions through encounters with the individuals who serve as “access points” to the larger system (Giddens, 1990). Through face-to-face interactions with the public (described as “facework”), these representatives can sustain trust in the broader (faceless) expert system (Giddens, 1990). Inherent in this conceptualization is the recognition that individual representatives are imbued with the authority and credibility of the broader expert system, forming a reciprocal relationship between individual and institution (Giddens, 1990). Giddens’ work has been “reinvigorated” in recent years, with scholars and practitioners alike recognizing its applications to trust in modern institutions, including community health (Kroeger, 2017).
Description of the Be REAL Approach
The Be REAL framework was developed as part of a project to hire, train, and support CHWs to increase access to COVID-19 vaccination in communities experiencing hesitancy. We selected 14 sites across seven states (AL, AZ, FL, GA, KY, MI, TX), including majority Black communities representing urban and rural populations, as well as Spanish-speaking regions with large immigrant populations. We recruited more than 100 CHWs directly from local community-based organizations.
The framework was a principal feature of the CHW curriculum. Our approach centered on relationship building—and not vaccination—as the primary goal of an encounter. Inherent in this approach was the acknowledgment that trust is both relational and voluntary, a trust relationship cannot be forced (Gilson, 2003). Trust relationships are never static, creating ongoing opportunities for trust to be earned. CHWs can position themselves to establish long-term relationships that allow for repeat opportunities to establish and demonstrate trustworthiness.
To decenter the traditional public health paradigm around individual behavior change, we assembled a large and interdisciplinary team working in and outside of public health. Under the leadership of a pair of professional stakeholder engagement experts and mediators (JB and MDH), our approach incorporated expertise gleaned from years of public policy mediation focused on intentional approaches that have the following cornerstones: careful, empathetic listening; honoring and redistribution of power (as appropriate for each circumstance); collaborative decision-making; and co-creating sustainable solutions that work for a diversity of stakeholders. Additional team members included both practitioners and scholars from a wide array of racial/ethnic, cultural, linguistic, and geographic backgrounds. Many of the team had participated in extensive formative work with vaccine-hesitant communities or had firsthand experience working in health departments during the pandemic (see Schwartz et al., 2023).
Public health communication often follows a deficit model, assuming individuals lack the information to make informed decisions (Simis et al., 2016). However, the COVID-19 pandemic exposed the many flaws of this assumption. As our team set about to develop a novel framework, we decided to flip the deficits model on its head. Instead of designing a traditional public health communication campaign and adapting it for CHWs, we turned instead to our team of experienced mediators to develop the initial outline of a framework that focused on relationship building (the R, E, and L portions of the model) and then incorporated health communication as a small portion of that framework (the A portion of the model). The four stages emerged organically team members attempted to translate discipline-specific expertise into lay language; mediators focused on relationship building, public health researchers on informational content, and practitioners on the community context. We utilized an iterative process to develop the final materials, with extensive internal pre-testing, practice sessions, and team feedback. Finally, we also refined training materials to meet CHW requests and respond to feedback, particularly around self-professed skill deficits and community concerns.
The Framework
Be REAL consists of four stages: “Relate,” “Explore,” “Assist,” and “Leave (the door open).” Stages are meant to be engaged sequentially, and build upon each other, with relationship building as the foundation of the encounter (Figure 1).
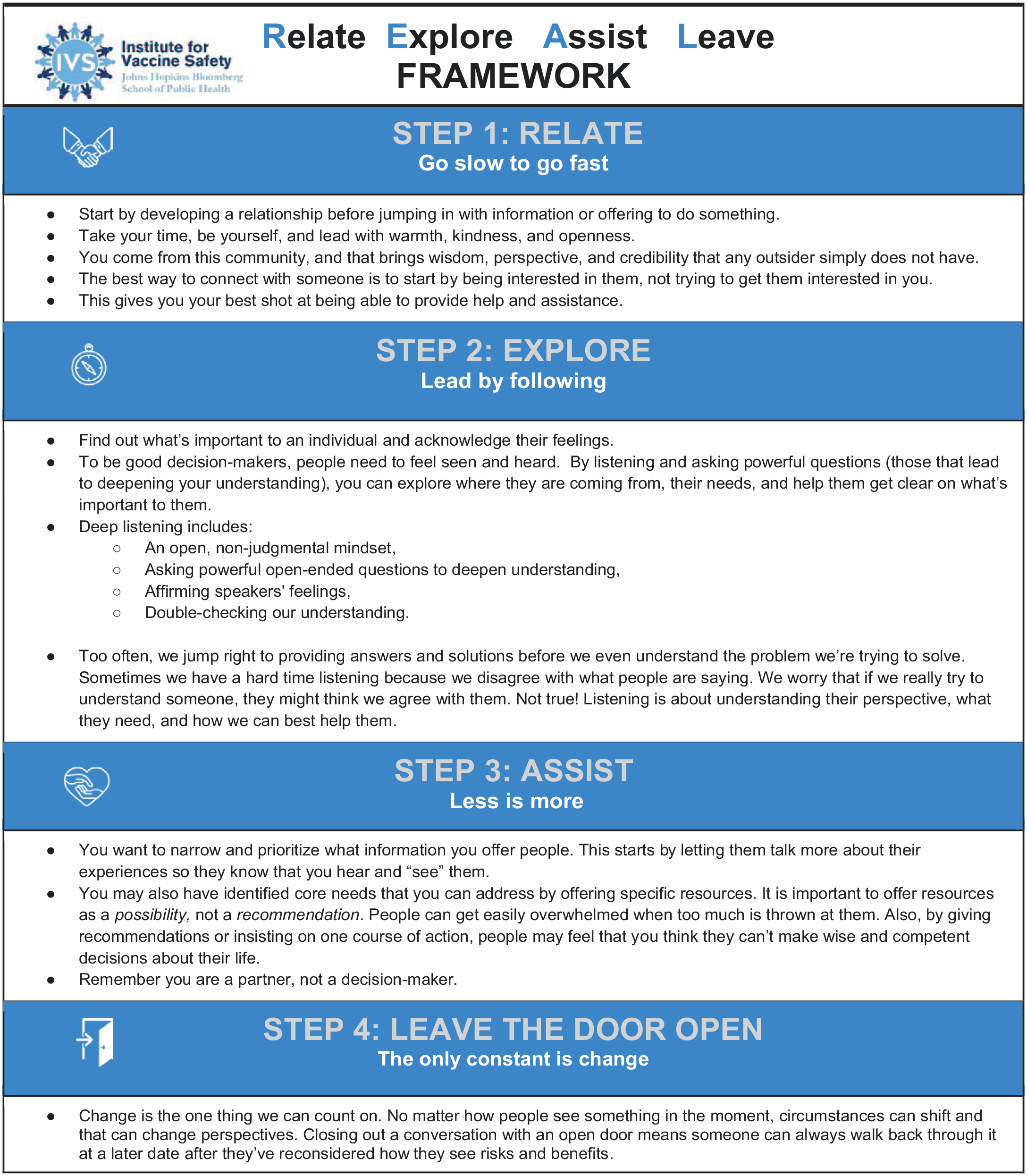
The Be Real Framework
Relate: The success of any CHW encounter hinges on establishing a relationship with community members. Accordingly, we encouraged CHWs to start by establishing common ground before broaching the subject of vaccines.
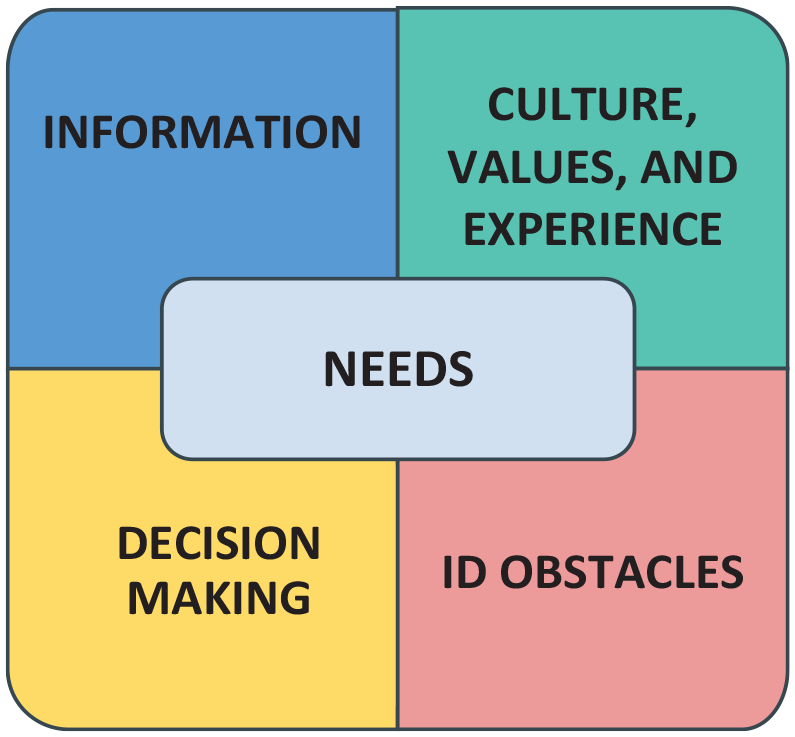
Explore: Rather than assume an individual’s concern, enter an exchange with curiosity. Listen first, then probe with “deep” questions. We introduced a “Needs Assessment Matrix” which divides information seeking into four quadrants—Information, Culture/Experiences, Identifying Barriers (to action), or Supporting Decision-making—for CHWs to probe the root cause of someone’s concerns or needs (Figure 2).
Assist: In an environment of pervasive vaccine information (both good and bad), it is essential that a CHW narrowly prioritizes the specific type of assistance individuals need. Narrowly targeting information will reduce the potential to overwhelm while increasing the potential for positive impact.
Needs Assessment Tool
CHWs can approach these encounters as “partners in decision-making” offering resources as a possibility, not a recommendation. The choice of whether to vaccinate is always up to the individual, and CHWs must respect individuals as fully capable decision-makers. If mutually agreed upon, CHWs can take active steps to connect individuals to resources.
4. Leave (the door open): Circumstances and perspectives change, closing with an “open door” means people can feel comfortable to return after they have fully considered their decision. We emphasized this is only the start of a relationship.
Power relationships were a central theme of the training. Frank conversations about the types of power wielded by different actors made clear the contrast between the formal power of authority figures and the informal—but incredibly valuable—power that CHWs possess within their communities. We asked CHWs to think of this as a “superpower” that made them uniquely prepared for their roles.
The Training
We held two weeklong training sessions over Zoom in June 2022. Be REAL was presented on Day 1, Session 1, to set the tone for the entire training. While later sessions incorporated clinically focused materials, each day closed with a return to the Be REAL principles. We designed these Zoom sessions to be highly interactive, with frequent breakout sessions and one-on-one practice time, supplemented with downloadable files and rich media clips. Professional engagement specialists (JB and MDH) mediated all Zoom sessions, with support from a team of bilingual cultural specialists (AC, AFo, AFu, RR, MEM, YT). The training materials were also made into brief animation videos, which we now host on the Institute for Vaccine Safety at the Johns Hopkins Bloomberg School of Public Health YouTube channel (Institute for Vaccine Safety: YouTube Channel, 2023).
A total of 115 CHWs and four regional CHW coordinators attended the training sessions. While a few were experienced CHW workers with more than 10+ years in the field, the majority were novices with less than 1 month of CHW job experience. The race/ethnicity of CHWs reflected the selected communities, with 63% identifying as Latinx, 33% identifying as Black, and 4% identifying as White.
Looking Ahead: Impact and Sustainability
We designed Be REAL to prioritize community engagement in the long term. As we continue to adapt and expand our CHW programming, we are actively collecting data from the field supervisors and soliciting direct feedback from CHWs. While a full evaluation of the overall program is forthcoming, early feedback specific to the training has been positive with the majority of participants reporting the training provided adequate preparation for their roles. In an informal post-training survey, all participants (n = 27) indicated that they would recommend the training to others in their position (including local health department workers, health educators, CHWs, and other NGO workers). Qualitatively, participants told us either that the materials were new and valuable—“I found answers here!!” and “this is gold!.” Or that the materials reflected things they intuitively knew but had never been formally presented (e.g., “This is not a new approach, but is helpful to be reminded how to do this . . .”).
However, the true success of the Be REAL approach may be difficult to assess in the short term. This challenge is twofold, first, unlike vaccine uptake which is clearly measurable with standardized metrics, assessing the quality of relationships—particularly at scale—poses a major challenge. Second, we recognize that metrics like vaccine uptake may obscure aspects of relationship building, particularly in preliminary stages of a relationship. For instance, if a participant initially refuses a booster but feels that the CHW supported and respected them through that decision, vaccination rates remain unchanged, but a relationship has begun. Furthermore, we recognize that current public health funding mechanisms can make it difficult to sustain long-term engagements, particularly without hard evaluation data to report progress. Indeed, as the COVID-19 public health emergency ends, will there still be funding to sustain CHW vaccine advocates? For these reasons and more, we encourage the field to consider and explore novel approaches and metrics to assess success around relationships. We believe that novel measures of both relationship quantity (e.g., number of engagements, length of engagement) and relationship quality (e.g., perceived trust, reciprocity, increased sense of belonging) can provide a more comprehensive evaluation.
In addition, a CHW can become a trusted source for future health information on a range of topics beyond vaccination. As implemented, Be REAL focused on COVID-19 vaccine hesitancy in minority communities, but the general nature of the framework makes it widely adaptable for a range of public health issues and the focus on relationship building is appropriate for all communities. A sustainable future for public health includes embracing community-centered care and CHWs can play a valuable role. Participants also expressed interest in further tailoring the REAL framework for general health promotion topics (e.g., diabetes education), targeting specific communities (e.g., migrant communities, LGBTQ) and for specific community concerns (e.g., opioid use, gun violence).
In the immediate term as vaccination rates continue to lag, we echo the sentiment shared in a recent report, “vaccination moves at the speed of public trust” (Brunson et al., 2021). Building quality relationships is a crucial step toward increasing public trust, which, in turn, may motivate vaccination. While widespread vaccination remains vital to curb the COVID-19 pandemic (and other vaccine-preventable illnesses), the Be REAL framework and results from our trainings suggest that public health practitioners can benefit from a long-term view. It is time to focus on relationship building and not “shots in arms” as our metric of success. We designed the Be REAL framework to support CHWs as they form relationships in communities because we believe that by prioritizing quality relationships public health can better serve its public.
Footnotes
Authors’ Note:
This research was supported by CDC through The Task Force for Global Health (Project ID: 02-6045-04 [RVD-CDCGHC3]; SARS-CoV2 Vaccines Information Equity and Demand Creation [COVIED] Project) and HRSA (Statutory Authority: American Rescue Plan Act of 2021, Section 2302. Award Number: U3UHS45470-01-00; Community-Based Workforce to Build COVID-19 Vaccine Confidence; CGHI project title: Vaccine Access and Training [VAT] Project).
Author Contributions
A.M. Jamison wrote the article. J. Brewer and M.H. Davis led framework design. A. Forr, R. Roberts, and A.M. Jamison assisted in framework design. A. Carey, A. Fugal, M.E. Mankel, and Y. Tovar provided critical feedback to the framework. J. Brewer and M.D. Hamlin led CHW training sessions. A. Carey, A. Forr, A. Fugal, A.M. Jamison, M.E. Mankel, R. Roberts, and Y. Tovar facilitated breakout sections of training sessions. K. Shapcott provided project management and organized CHW training sessions. S. Adams and D. Salmon conceptualized the project, secured funding, and oversaw all aspects of the project. All authors contributed to reviewing and editing the final draft.