
Abstract
People experiencing homelessness balance competing priorities resulting in reduced capacity to meet the care demands of chronic conditions, including Type 2 Diabetes Mellitus (T2DM). Arts-based performances present an avenue to expose others to these challenges. This article describes the process of incorporating qualitative research findings in a community-based participatory theater production to expose audiences to the day-to-day realities of living with T2DM while simultaneously experiencing homelessness. We conducted five focus groups and two individual interviews with people living with T2DM who had experienced homelessness with guidance from a community-engaged research team. We then collaborated with a local theater company to present common themes from these focus groups in a co-created play about the experience of managing T2DM while being homeless. We performed a staged reading of the play and assessed audience members’ perceived stigma through a pre- and post-survey to determine if audience engagement within our theatrical production could reduce stigma toward individuals living with diabetes and/or people experiencing homelessness. This theatrical production is titled “Life Heist: Stealing Hope While Surviving Diabetes and Homelessness.” Our work illustrates the feasibility and effectiveness of using participatory theater to disseminate qualitative research findings.
The dual stress of living with type 2 diabetes (T2DM) and homelessness is associated with premature mortality (Baggett et al., 2013; Roncarati et al., 2018). Previous studies of the impact of diabetes among people experiencing homelessness show similar incidence rates among the populations that are housed and unhoused, but people experiencing homelessness have far worse diabetes outcomes. They often end up hospitalized sooner and dying at younger ages due to diabetes and its complications (Adams et al., 2007; Axon et al., 2016; Baggett et al., 2013; Bernstein et al., 2015). Public perception of homelessness and diabetes also impacts patients’ experiences. Previous studies have shown that people with T2DM report feeling stigmatized based on their disease (Browne et al., 2013; Schabert et al., 2013). Diabetes stigma is compounded by the stigma of homelessness. Perceived stigma of homelessness drives greater psychological distress, poorer physical and mental health, and increased avoidance of services, and is exacerbated among People of Color, especially those with indigenous heritage who disproportionately experience homelessness due to structural racism (Davachi & Ferrari, 2012; Reilly et al., 2022; Weisz & Quinn, 2017).
Community-Based Participatory Research (CBPR) presents a potential solution to engaging people experiencing stigma to discover solutions to lessen the stigma of T2DM and homelessness. CBPR involves collaboration with communities in all steps of the research process to identify problems and create solutions. An important component of CBPR is the accessible dissemination of research findings back to the community.
The conceptual framework guiding this work is the natural synergy between CBPR and the field of Socially Engaged or Applied Theater where the process of making theater (storytelling, trust building, emotion recall) is applied to social issues to support deeper listening, dialogue, understanding, and action (The Center for Applied Theater, n.d.; Cohen-Cruz & Pereira, 2022). CBPR and Applied Theater are both particularly suitable for addressing potentially stigmatizing topics where power differentials exist between people affected by the topics under study and broader society. Applied Theater, like CBPR, is often “community-based,” engaging community members most affected by the issue in the creative process and drawing from real stories of participants (Watermeyer et al., 2021). Applied Theater also encompasses Augusto Boal’s work on the Theater of the Oppressed (Boal, 2000), which is an interactive theater and political technique used to engage audience members and influence their behavior and larger social change (Fredland, 2010). This aligns with the intentions of CBPR and the role of communities to disseminate participatory research findings to wider audiences. Previous studies have used CBPR and theater to address stigma among people experiencing homelessness with chronic health conditions (Reilly et al., 2022; Sullivan, 2019; Watermeyer et al., 2021; Zhuang & Guidry, 2022). One study turned randomized control trial data into a libretto for an opera on veterans experiencing homelessness for a larger audience (Wells et al., 2021).
In this article, we describe our effort to used Applied Theater to disseminate findings from an ongoing research project using CBPR principles to develop a behavioral intervention for people with T2DM who have experienced homelessness. We will: (1) outline the process of developing the theater production based on qualitative research findings; (2) detail how the theater production highlighted our data-driven findings about the day-to-day realities and challenges of living with T2DM while homeless; (3) demonstrate the ability of interactive theater to disseminate qualitative research; and (4) explore the effectiveness of the performance to engage audience members and reduce audience stigma toward people with diabetes who are experiencing homelessness before versus after the performance.
Method
Location
The Life Heist production was a collaboration between zAmya, a local theater group, and Quorum, a community advisory group, both based in Minneapolis, Minnesota. Our previous work reflects a rising prevalence of T2DM to 12% among people experiencing homelessness in Minnesota surpassing the national average (10.5% in 2018; Vickery et al., 2021), making this area an ideal location to conduct these research activities.
Initial Inspiration
The collaboration between zAmya and Quorum began when the Quorum group attended a zAmya performance (zAmya Theater Project 2019) and saw synergy in the participatory nature of the performance and the subject matter of homelessness. Inspired to learn more, the team met with zAmya’s artistic director. The team acknowledged mutual interest in using theater to disseminate community-engaged research findings. We undertook a collaborative grant-writing process for a university grant about health equity research using innovative dissemination strategies. Both organizations co-wrote the grant, developed a collaborative budget, and reviewed the project timeline and deliverables. This grant supported the production and impact measurements we describe here.
Partnership Development
zAmya began in 2004 when a group of housed people committed to examining homelessness came together to find a solution. They chose theater as their container for this work because of its unique ability to center personal narratives, shift culture, and build interdependence. zAmya contracted a troupe of 12 actors, writers, makers, and activists, most of whom have lived experience of homelessness, who guide the direction of the company. zAmya is situated in the field of Socially Engaged/Applied Theater. Professional artists and community partners collaborate with the Troupe on performances that activate compassion and inspire communities to work for housing justice. The aesthetic of zAyma is informed by Augusto Boal and the Theater of the Oppressed, which uses theater to “rehearse the revolution” and “Community-Based” models such as Roadside Theater and Cornerstone Theater that use real stories to uplift and strengthen communities as well as the Los Angeles Poverty Department that has been using art to build community in Skid Row, Los Angeles since 1970 (ImaginAction, n.d.). The zAmya troupe finds ongoing engagement with the homeless community in the Twin Cities and Greater MN through residencies in libraries, shelters, and transitional housing facilities.
The Quorum was founded in 2015 to “reimagine health and wellness through community connection.” The team met monthly to co-define research priorities which included: (1) the “pile up” of (multiple) chronic conditions, especially diabetes and behavioral health, (2) unstable housing and its impact on health, (3) support from community health workers/lay health coaches, and (4) patient and family-centered health care. Quorum members included people with lived experience of T2DM and/or homelessness and unstable housing; clinical staff from the local Health Care for the Homeless program, people from local community organizations, research staff and the PI, and a community engagement facilitator.
The Quorum members supported the principal investigator (PI, KDV) in developing a research proposal to develop and pilot test a behavioral intervention to support diabetes self-management tailored to the needs of adults living with T2DM who had experienced homelessness (K23DK118117). The input from Quorum helped guide all phases of this ongoing research. The qualitative research took place from October 2019 to March 2020 when the research team completed five small group and two individual interviews in urban community settings in Minneapolis. Twenty-six people participated in an interviews. Each interview lasted approximately 1 hr. Questions explored barriers and enablers to diabetes care management among people experiencing homelessness, values and beliefs about medications, the impact of unstable housing, and diabetes treatment preferences.
The research staff analyzed the resulting transcripts from these conversations and used a framework matrix approach (a deductive analytic approach used to inform our behavioral intervention development) to produce summaries and illustrative quotes of key themes (Gale et al., 2013). Research findings can be found elsewhere (Turcotte Manser et al., 2023, Vickery et al., 2023).
Production Development
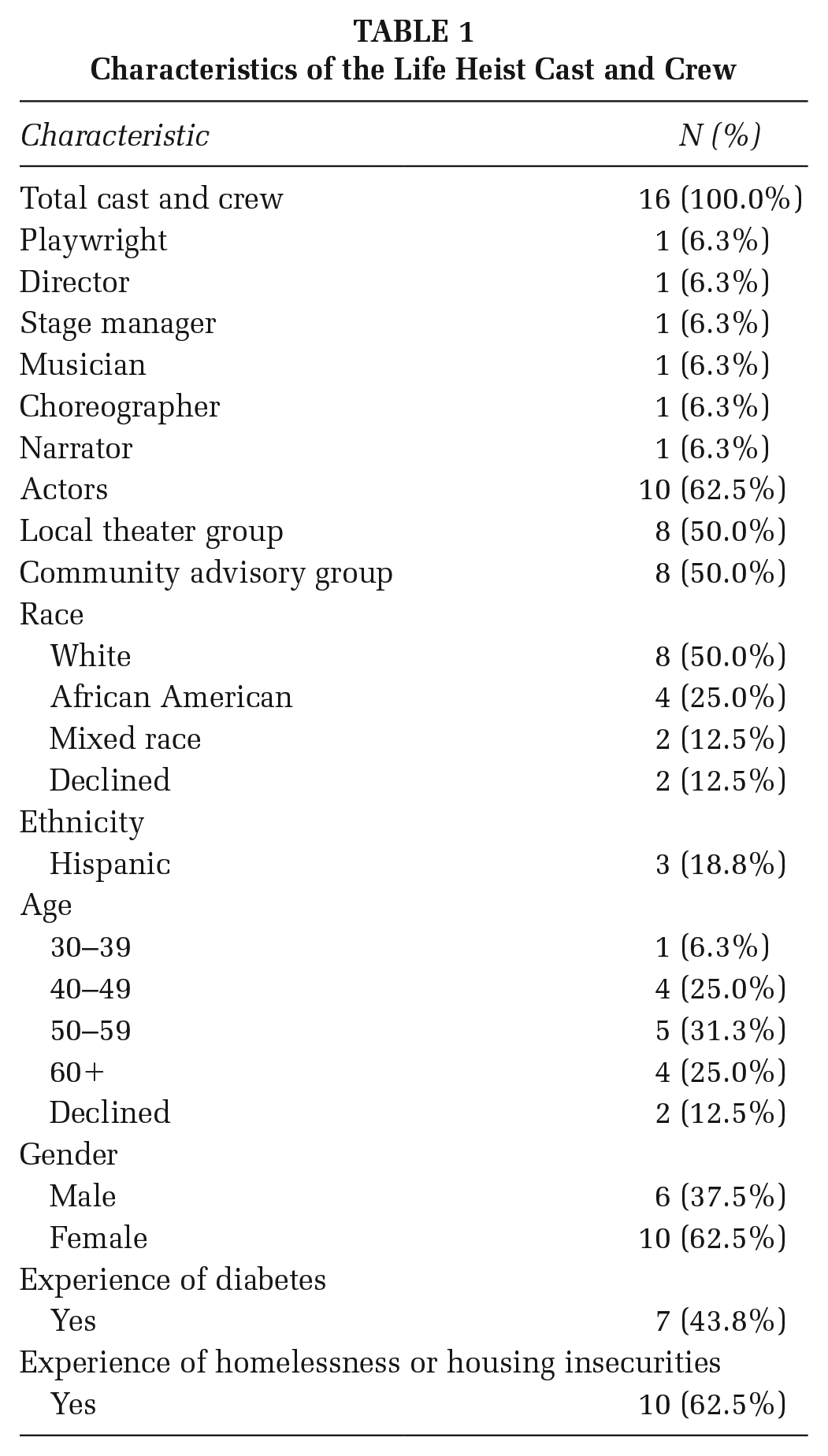
A team emerged led by zAmya director (MW), stage manager (EO), playwright (JMC), PI (KDV), community engagement facilitator (SG), and research staff (MF). The final team included 14 cast and crew members including troupe members from zAmya and members of the Quorum. Many people had lived experienced of T2DM and homelessness (Table 1).
Characteristics of the Life Heist Cast and Crew
In the summer of 2020, we began the process of relationship-building between Quorum members and zAmya leadership. We introduced the theater production as a way of sharing our research findings with the broader community. The playwright and director used research summaries of the themes and illustrative quotes from the qualitative data without personal identifiers to begin script development and to plan workshops with the larger team. The team met twice a week for 2 hr over 4 weeks for structured “script workshops,” where the playwright and director led conversation and writing prompts along with improvisation games and exercises designed to generate material and explore content. One example was “Machine,” an exercise adapted from Boal where participants make a repetitive sound and motion that is associated with, in this case, living with diabetes (Boal, 2002). Participants built a machine for taking diabetes medications (the primary target of the behavioral intervention research). Some participants’ sound/motion emphasized side effects of medications (e.g., stomach upset), while others focused on cost barriers and others on their feelings about being told to take their medications. We held in-person and video meetings given the pandemic, and despite our best efforts to overcome barriers, participation was impacted for some team members. The playwright and director participated in these workshop activities and used the time between workshops to write the script integrating emerging workshop content with research themes and quotes. The team began rehearsing the script while it was still being finalized, and the script was edited continually as we practiced reading lines and made casting decisions. For example, the cast was encouraged to edit their lines to sound natural and fit with the profile of their character. The enthusiasm and creativity of the team also led to the creation of musical numbers and choreography to accompany the script. These numbers emphasized healthy eating, staying active, and the social support essential for successful diabetes self-management. See Production (below) for details on the resultant script. From July 20 to August 31, we held 15 rehearsals in-person and via Zoom to prepare for the performance, a public staged reading.
Measurement of the Impact of the Performance
To measure the impact of the performance, we obtained IRB approval from the University of Minnesota to invite audience members to complete a paper survey before and after the performance.
Recruitment was conducted as participants entered the theater; interested participants were introduced to the project and instructed how to participate. Audience members could view the play and decline to participate in the survey.
Before the performance, we asked audience members for relevant sociodemographic data, housing status, prior experience with homelessness, and knowledge of and previous experience with diabetes. After the play, to assess the level of audience engagement with the play, we asked them to complete the Narrative Engagement scale, a 12-item survey using Likert-type-like response scales from 1 to 7 (See Supplemental Materials). This scale assesses four aspects of engagement each with three questions: narrative understanding (audience making sense of the narrative), attentional focus (how distracted audience members are when watching the performance), narrative presence (feeling involved in the story), and emotional engagement (emotions toward characters; Busselle & Bilandzic, 2009). The lower end of the scale denotes less agreement with the statement and higher numbers indicate more agreement with the statement. The narrative understanding and attentional focus questions were reverse-coded. To score the scale, we summed the Likert-type score for each aspect of engagement.
To explore possible stigma about diabetes and/or homelessness and if/how this was impacted by viewing the performance, we asked audience members to complete two instruments before and after the play: The Diabetes Causal Attributions Scale and the Competence and Warmth scale adapted to focus on people experiencing homelessness (See Supplemental Materials). We modified the Diabetes Causal Attributions Scale from Persky et al. (2021) to assess the degree to which the audience believed that diabetes was affected by food choices, physical activity, genetics, access to health care, and access to healthy foods (Persky et al., 2021). The instrument used a Likert-type scale ranging from 1 to 7, where 1 denoted strongly disagree and 7 denoted strongly agree. The second scale, Competence and Warmth, is derived from Cuddy and Fiske (Cuddy et al., 2008). We used this scale to measure audience stigma by their perceptions of competence and warmth of people experiencing homelessness. This instrument uses a Likert-type scale ranging from 1 to 5 to respond to the extent people experiencing homelessness have various attributes, where 1 denotes “not at all” and 5 denotes they “very much.” We calculated a mean for competence and warmth across relevant items as the authors have done in previous work (Fiske et al., 2002). Paper surveys were entered twice into a REDCap digital database. Discrepancies were resolved by a senior research staff member. Audience characteristics and narrative engagement scores were summarized using appropriate univariate statistics in R. Changes in before and after performance survey results were analyzed with a two-tailed paired sample t test.
Results
Production
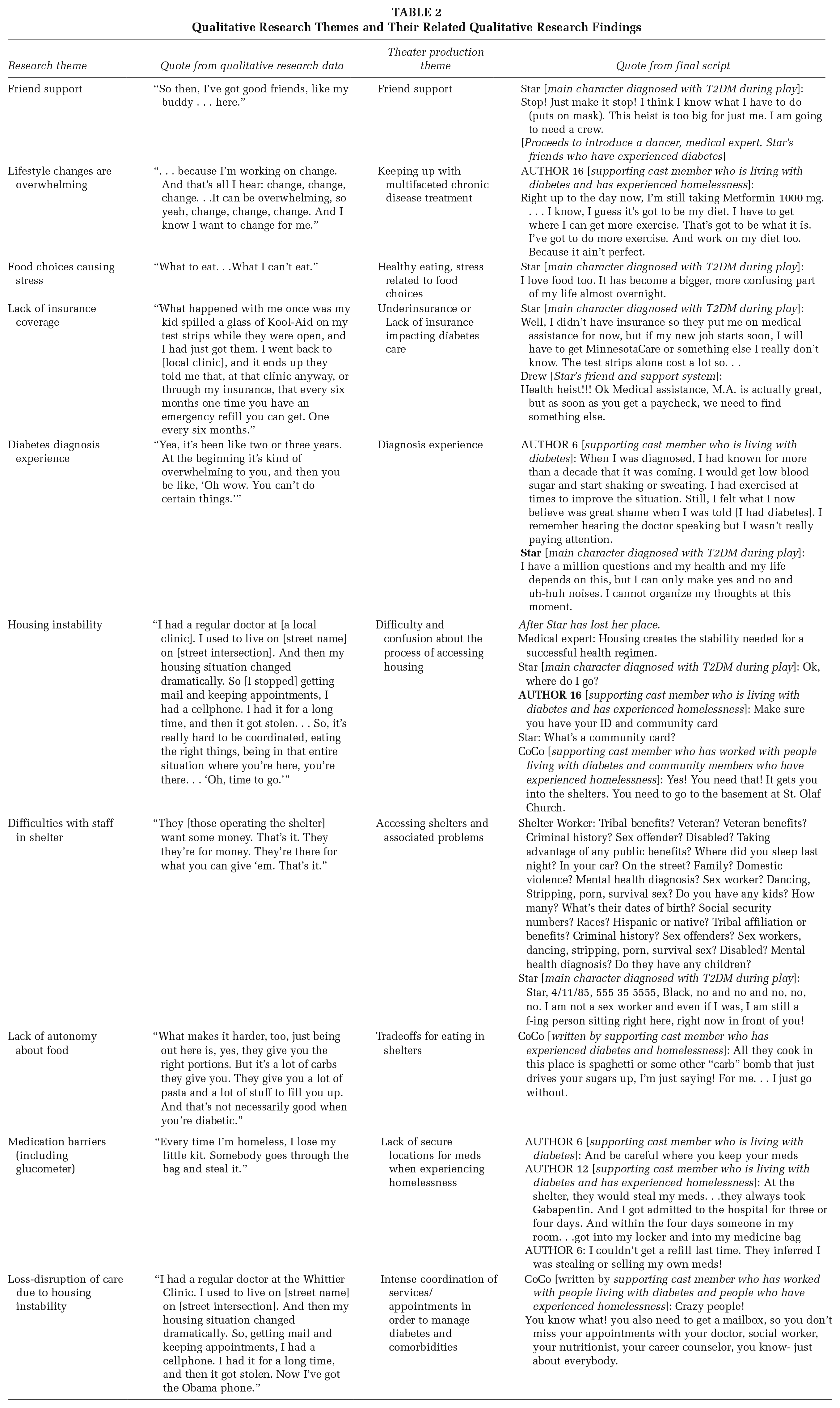
The play was derived from themes from our team’s qualitative research about diabetes and homelessness. The resulting script was titled “Life Heist: Stealing Hope While Surviving Diabetes and Homelessness.” The play hinges on the main character, Star. She has been recently diagnosed with diabetes and the play focuses on the interplay of diabetes and unstable housing that makes it difficult to care for her diabetes. Star navigates barriers such as the difficulty of making lifestyle changes, limited food choices, lack of insurance coverage, difficulty managing diabetes in shelter settings, and medication barriers. The play uses the trope of a bank heist to illustrate the increasingly complicated and creative strategies Star employs to overcome these barriers. Her character also shows some of the facilitators of diabetes care when experiencing homelessness. For example, through her interaction with her friend and confidant, Drew, she underscored the importance of friend and family support, a recurring theme in our research data.
As Star progresses through the play, she relies on Drew’s support to navigate many barriers. Table 2 shows examples of the collaborative translation of qualitative research findings into excerpts from the play’s script.
Qualitative Research Themes and Their Related Qualitative Research Findings
To use the performance as a means of exploring and affecting audience members’ perspectives on homelessness, we engaged them by using techniques from Boal’s Theater of the Oppressed such as breaking the fourth wall and encouraging audience members to interact with the play. At times cast members would ask the audience for their input. For example, at the beginning of the play, Drew, Star’s friend, asks the audience to list all that they know about diabetes and the possible challenges Star might face. Similar call-and-response activities, dancing, and original music compositions were interspersed throughout the performance and were aimed at increasing audience engagement.
To increase the accessibility of the staged reading, we chose a newly renovated theater located in a primarily Black/African American neighborhood that has been harmed by housing discrimination and other disparities. In an effort to reduce financial barriers to attendance, admission was free. The non-profit theater venue is a cornerstone of the neighborhood and is utilized for community building, youth outreach, and education.
Measurement of the Impact of the Play
Audience Recruitment and Demographics
Audience recruitment was done via an email invitation, flyers, and a radio show to the larger community and occurred through zAmya and on the research lab’s social media platforms. We specifically targeted invitations within the local community by outreach at the local community health center and other area organizations and businesses using flyers and written invitations. We also advertised via an interview on a local radio station focused on Communities of Color in this region (KMOJ) and invited all listeners to attend the upcoming performance. We also specifically targeted those who work in the housing and health care sector, including health care workers, social workers, and shelter staff. In total, 72 people attended and 34 audience members completed a survey (response rate 47%). Sociodemographic information is recorded in Table 3. The average age in our audience was 52 (SD = 15 years). The majority of our audience identified as female (68%) and the audience was largely white (79%). While most of our audience was currently stably housed, 24% had experienced homelessness sometime in their lives. Nearly three-fourths of our audience (74%) had diabetes or knew someone close to them with diabetes. Audience members were also given the chance to provide free-hand comments as part of the survey to give feedback on their performance. One audience member wrote, “Thank you for creating this space and narrative. It helped me put challenges of chronic disease in homelessness feel more real/put to a story/face” and another said “This was an amazing show! Very well put together. My family and I enjoyed every minute. I learned new things and enjoyed the interactive moments. Great Performances!!”
Audience Survey Results
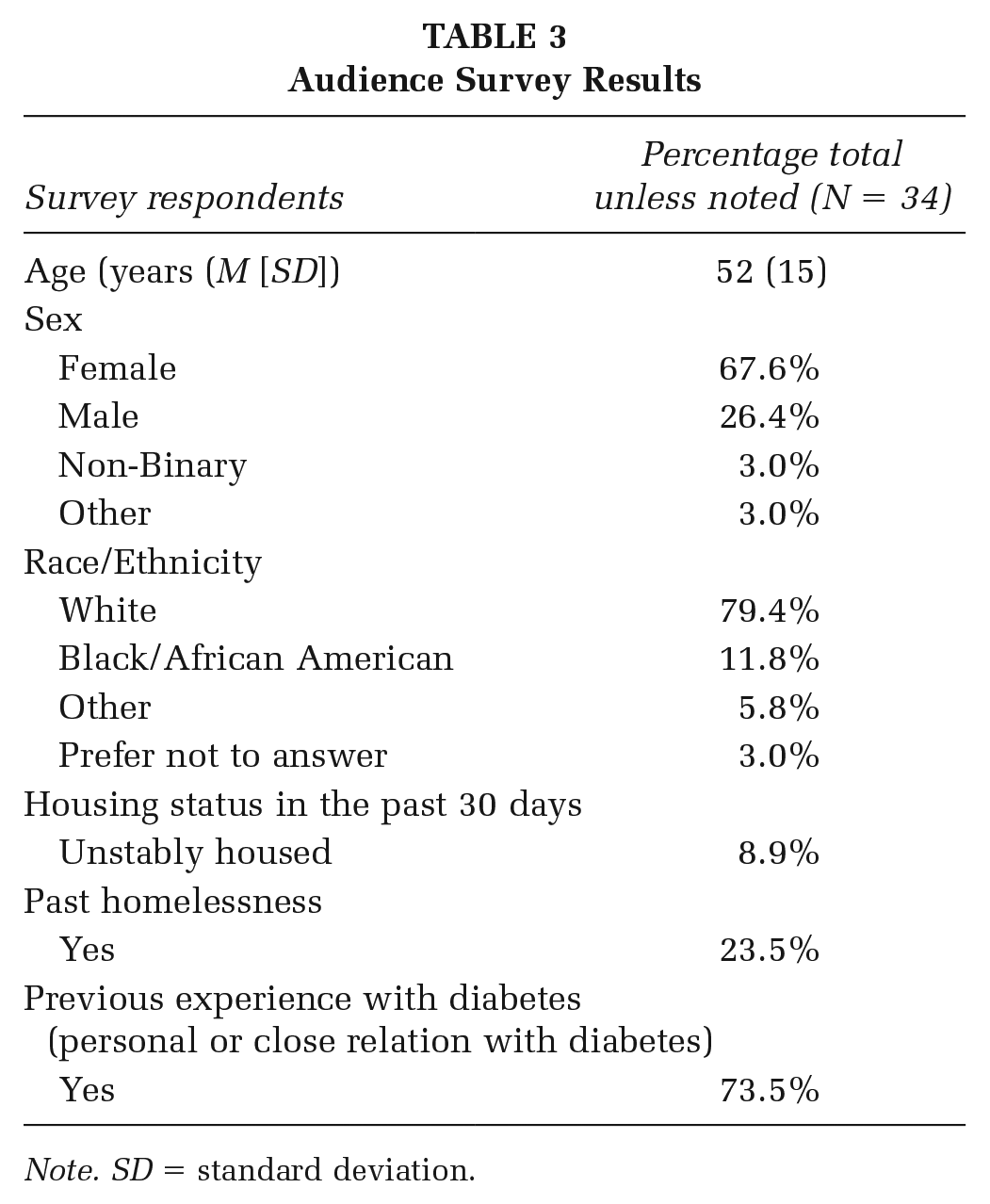
Note. SD = standard deviation.
Audience Survey
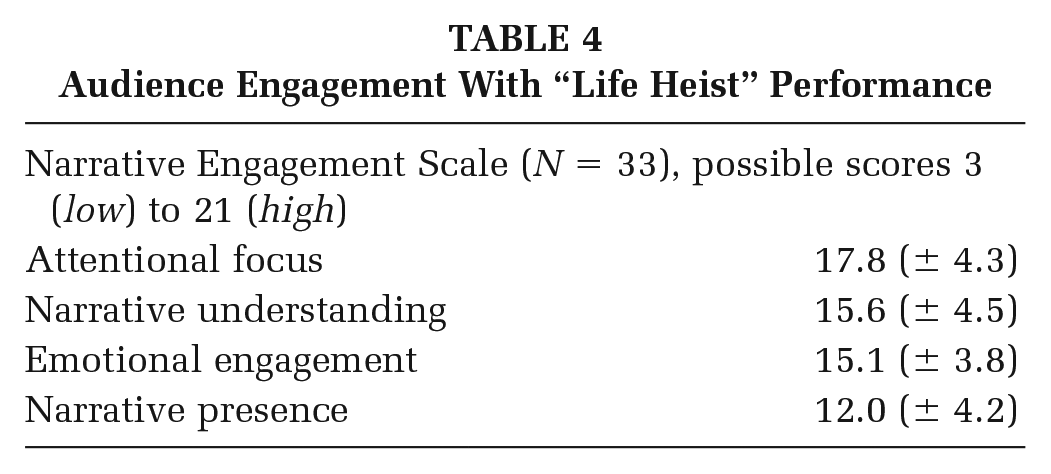
The narrative engagement scale is reported across the domains of engagement, each with a possible score ranging from 3 (low) to 21 (high). The audience had moderately high scores across all the domains. Attentional focus had the highest score (M = 17.8, SD = 4.3). Emotional engagement (M = 15.1, SD = 3.8) and narrative understanding (M = 15.6, SD = 4.5) had similar scores. The narrative presence a lower score (M = 12.0, SD = 4.2; Table 4).
Audience Engagement With “Life Heist” Performance
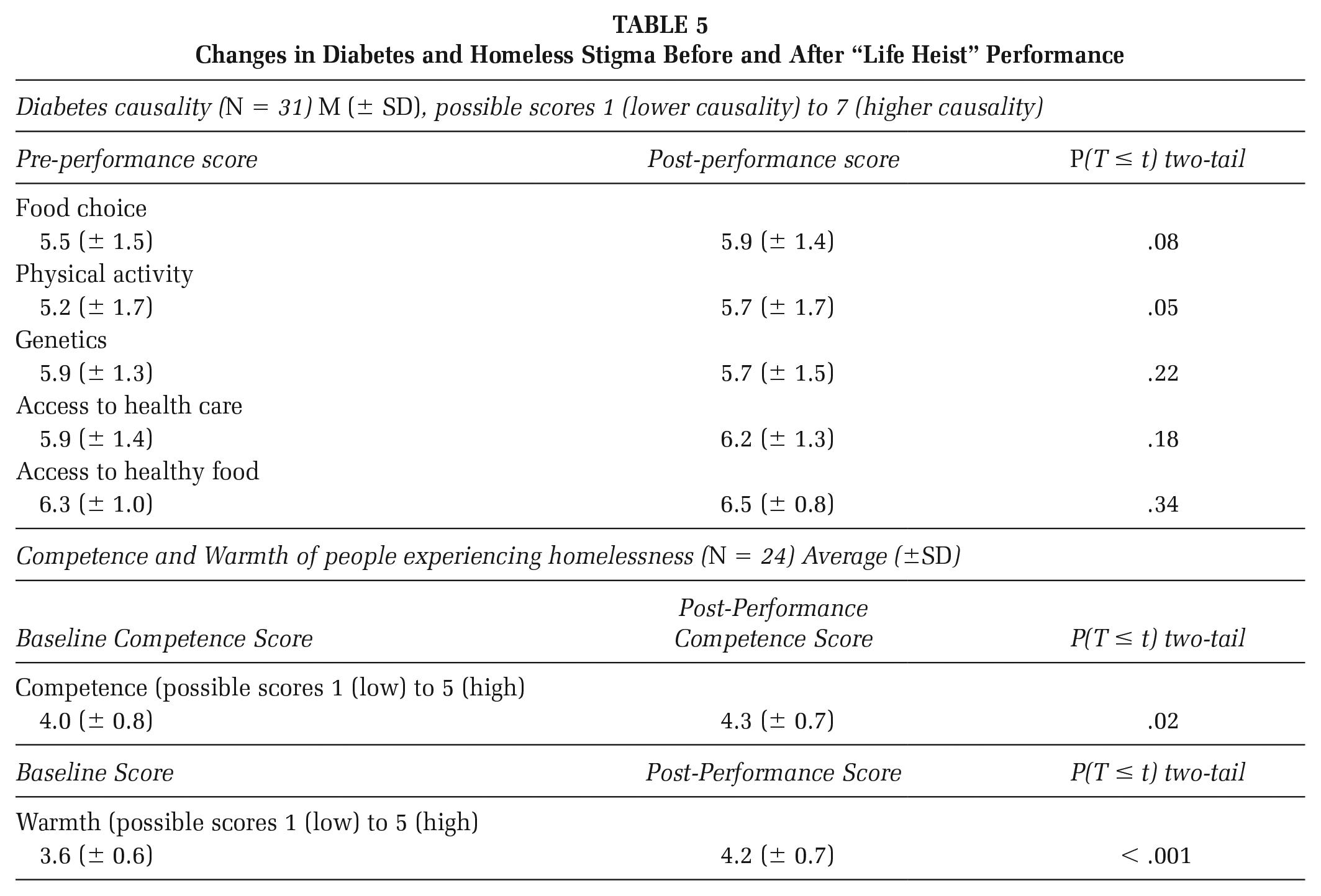
Our exploratory analyses to measure stigma using the Diabetes Causal Attribution Scale demonstrated an increase from before to after the play in the audience members’ perception of diabetes being impacted by food choices and physical activity (Table 5). However, the other aspects of our scale: genetics, access to health care, and healthy foods, did not change. Changes in the Competence and Warmth scale show an increase in audience members’ perception of people experiencing homelessness as competent (Δ0.3, p = .02) and warm (Δ0.6, p < .001) from before compared to after the play.
Changes in Diabetes and Homeless Stigma Before and After “Life Heist” Performance
Discussion
Our theater production effectively transformed research data into accessible stories that led to measurable engagement by an audience that included a substantial number of community members with personal experiences of diabetes and homelessness. We found substantial synergy between the Quorum approach to CBPR and Community-Based Theater production of zAmya. This underscores the potential of participatory theater as a promising dissemination medium for participatory research findings in the future. This is especially true when related to complex topics such as diabetes and homelessness.
Our data support our conclusions that the audience was engaged and impacted by our performance. The audience’s scores on the engagement scales specifically demonstrate high levels of attentional focus, emotional engagement, and narrative understanding. The audience’s energy and positive comments after the show also underscore these data. This suggests that theater appears to be an effective means to engage an audience about the difficult topics of diabetes and homelessness. We suspect that the lower scores on narrative presence relate to the multiple characters and many complex themes addressed in the play. While exploratory, our data suggest a possible increased understanding of the impact of lifestyle choices (food choices, physical activity) on diabetes after the performance. We suspect high baseline scores contribute to the lack of change in topics of genetics and health care and healthy food access. Changes in warmth and competency scores align with previous measures done by Cuddy and Fiske who have shown that people who are poor, homeless, or receive welfare are typically regarded as low on competence (Mean of 1.97 out of 5.0) and warmth (Mean of 2.42 out of 5.0; Fiske et al., 2002). Changes in scores seen before and after our performance suggest possible decreased stigma against people experiencing homelessness among audience members after attending the production. More research is needed with larger audience sizes and additional survey instruments to more robustly assess the ability of theater as a dissemination strategy to reduce stigma toward people experiencing homelessness.
We must note several limitations impacting our work. Our overall attendance and the survey response rate were limited by the COVID-19 pandemic. Low sample size limits our ability to make conclusions about the findings we see in this data which is why our questions and analyses remain exploratory, especially related to changes in stigma among audience members. Survey respondents are likely biased toward those with strong opinions to share. Respondents were largely white females demonstrating likely hesitancy among BIPOC audience members to participate in research, a finding reinforced in the literature (Flores et al., 2021; Scharff et al., 2010). Finally, our one-time cross-sectional survey cannot measure if audience engagement or shifts in stigma are long-lasting or transient effects, either because of social desirability or salience of production.
Our work fits into ongoing arts-based strategies to disseminate research findings in an accessible manner to a broad community. We find particular synergy between arts-based dissemination approaches and participatory research as they express the rich nature of participatory, and especially qualitative, research while also highlighting the lived experiences of the research team. Our work can be compared with other arts-based approaches used by others to make research accessible beyond academia and to encourage deeper thought and discussion among audience members (Colantonio et al., 2008; Levin et al., 2007). This includes other health research on homelessness which has used a variety of different artistic media ranging from opera to photovoice (Wang et al., 2000; Wells et al., 2021). These studies note that these arts-based strategies allowed the participants an avenue to creatively express their concerns and build relationships within their artistic communities. These approaches are directly aligned with the principles of participatory research. Engaging in these creative processes and the pedagogical theater approach, similarly, empowered people experiencing homelessness and diabetes to bring up their concerns and inform researchers about their day-to-day concerns while also giving them a platform to educate their community.
Implications for Practice and Future Research
CBPR approaches inherently question power relationships and urge everyone who engages in research to consider who the research is serving. Our work details the rich process of using theater to disseminate qualitative research findings from a participatory research project into the larger community. We learned a lot about the synergy between Applied Theater and participatory research. We found the workshop, script development, rehearsal, and production process strengthened our team and energized us about the research. We also learned how to sustain our work despite pandemic-related challenges and how to balance considerations of safety and inclusion. Our production and survey data fit into the growing body of research bridging participatory and qualitative research with community-based participatory theater and other arts-based approaches. We suggest that this model of qualitative research to arts-based dissemination is feasible and enriching for both the multidisciplinary CBPR team and the community engaging with the resulting productions. Future work can build upon our data to assess the potential of these interventions to reduce stigma and influence public opinion.
Supplemental Material
sj-docx-1-hpp-10.1177_15248399231221731 – Supplemental material for Disseminating Community-Engaged Research Involving People Experiencing Homelessness and Diabetes Using Participatory Theater
Supplemental material, sj-docx-1-hpp-10.1177_15248399231221731 for Disseminating Community-Engaged Research Involving People Experiencing Homelessness and Diabetes Using Participatory Theater by Preethiya Sekar, Maren Ward, Susan Gust, Becky R. Ford, Moncies Franco, Edward Adair, Annette Bryant, Denita Ngwu, Jonathan M. Cole, Lelis Brito, Marcia Barnes, Tahiti Robinson, Ali ‘Cia Anderson-Campbell, Joel Gray, Esther Ouray, Alphonse Carr and Katherine Diaz Vickery in Health Promotion Practice
Footnotes
Authors’ Note:
We list academic degrees per publication conventions for some of our team members. However, our team believes knowledge holders come from many backgrounds not fully captured in academic degrees. Research reported was supported by the University of Minnesota Program in Health Disparities Research (PHDR) Health Disparities Pilot Grants award HD20CHI01. This award is administered by the UMN PHDR and funded by the Office for Business & Community Economic Development (OBCED) Community Health Initiative (CHI), University of Minnesota. The content is solely the responsibility of the authors and does not necessarily represent the official views of the University of Minnesota. K. Vickery and M. Franco’s time on this publication was supported by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health under Award Number K23DK118117. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.