
Abstract
Introduction. Mental Health First Aid (MHFA) was created to teach individuals how to identify, understand, and respond to signs of mental illnesses and substance use disorders. Programs like this may be essential for agricultural communities where suicide rates have increased, and mental health stigma has been a barrier to this population. This study evaluated how effective MHFA and Youth MHFA were for participants from agricultural communities. Methods. Participants completed the MHFA (N = 38) and Youth MHFA (N = 66) programs in 2021–2022, and Extension educators offered both programs as a part of outreach efforts within agricultural contexts. Participants completed pre-, post-, and post-only evaluations as standardized by the National Council for Mental Wellbeing. Results. After completing the MHFA and Youth MHFA training, participants increased their knowledge, confidence, and skills in various mental health topics. This includes early indicators of mental health challenges, the ability to have supportive conversations, and how to provide resources to others. For example, most participants felt they became more knowledgeable about MHFA (69%) and the ability to recognize the signs and symptoms of mental health or substance use challenges (65%). Conclusion. This research has implications for supporting agricultural workers through additional mental health training, managing farm stress, and understanding mental health stigma within this community.
Suicide rates among farmers have increased since 2003 and are up to 2 times higher than the general population (Norrod et al., 2023). Norms and values such as stoicism, independence, and hard work through adversity create barriers for help-seeking among agriculturalists (Baker et al., 2022; Brandth, 2020). Within this context, accessible mental health literacy trainings can help community members improve their knowledge of mental health issues, signs of emerging mental health crises, communication skills, and helpful resources to assist a distressed farmer (Jorm, 2012).
Mental Health First Aid (MHFA) is an evidence-based mental health literacy program originally developed and implemented in Australia; it has since been adopted in 21 other countries worldwide (Kitchener & Jorm, 2002, 2004). MHFA was created to teach individuals how to identify, understand, and respond to signs of mental illnesses and substance use disorders. The training provides individuals with skills and knowledge to provide support, initial help, and how to reach out to someone who may be developing a mental health problem or experiencing a crisis. Youth MHFA (YMHFA), for adults who work with youth, focuses on differences between typical adolescent development and emerging mental health issues. Both MHFA and YMHFA have increased mental health literacy, confidence/self-efficacy, action, continued use of MHFA skills after the training, and reduced stigma, including diverse communities and occupational groups (Banh et al., 2019; Childs et al., 2020; Corona et al., 2020; Hadlaczky et al., 2014; Lee & Tokmic, 2019; Robertson et al., 2021). We aimed to evaluate how effective MHFA and YMHFA were for participants from agricultural communities.
Methods
Programs
MHFA and YMHFA are standardized programs; to ensure applicability to farming and agricultural contexts, roleplaying scenarios in both trainings were adapted to be about people working in agriculture. Extension educators offered both programs as a part of outreach efforts within agricultural contexts. YMHFA was offered from October 2021 to May 2022 in a blended format (i.e., 2 hours of online work and 4.5 hours of instructor-led content), wherein eight instructors taught 66 participants across 10 sessions. MHFA was offered from January to March 2022 in a blended format wherein three instructors taught 38 participants across five sessions. This study was labeled as exempt by the Institutional Review Board of the authors’ university.
Evaluation Surveys
Participants in both trainings were asked to complete pre-, post-, and post-only evaluations as standardized by the National Council for Mental Wellbeing. Surveys asked about confidence, skills, taking action, and knowledge about mental health. Questions varied with four and five-point Likert-type scales, which included do not agree at all (1) to strongly agree (5), not at all likely (1) to extremely likely (5), not at all difficult (1) to extremely difficult (5), and have no knowledge of content (1) to consider myself very knowledgeable (4).
Participants
Participant demographics can be found in Table 1. YMHFA participants were also asked if they identify as a person with lived experience, serious mental illness, or a person in long-term mental health recovery. 86.7% of participants who completed this question indicated that they did not. Participants were also asked if they support a family member with lived experience, and 66.7% stated that they did not.
Descriptive Statistics
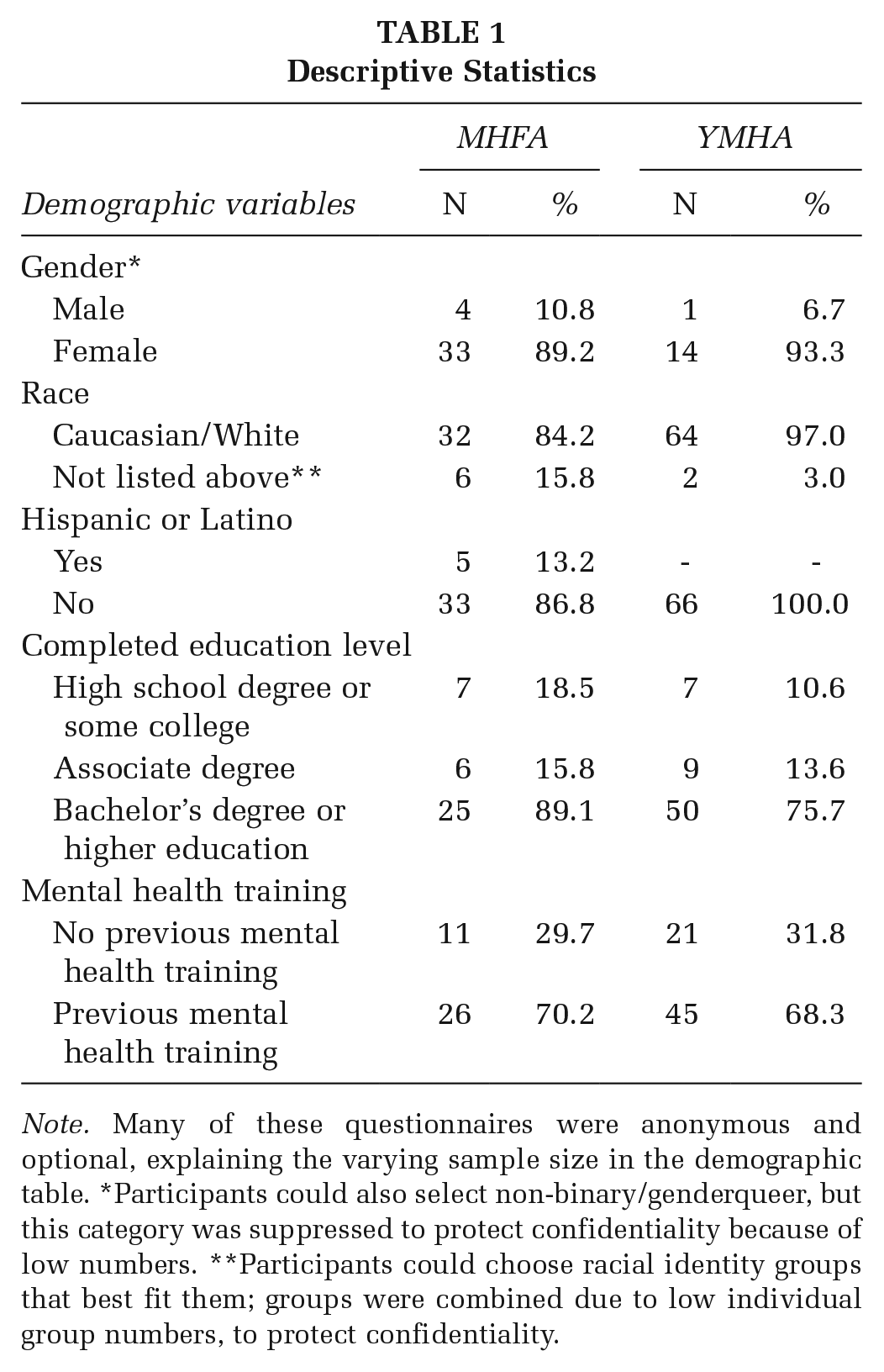
Note. Many of these questionnaires were anonymous and optional, explaining the varying sample size in the demographic table. *Participants could also select non-binary/genderqueer, but this category was suppressed to protect confidentiality because of low numbers. **Participants could choose racial identity groups that best fit them; groups were combined due to low individual group numbers, to protect confidentiality.
Results
MHFA
Knowledge
After completing training, 100% of participants knew (a) ALGEE action plan statements (e.g.,
Confidence and Skills
Most participants also experienced a positive change in their confidence surrounding mental health and their ability to take action. For example, 54% of participants increased by at least one level of likelihood when asked if they give information about mental health professionals in the community to any person experiencing a mental health or substance use challenge(s), which may assist in that person getting help. Figure 1 displays additional examples of this change.
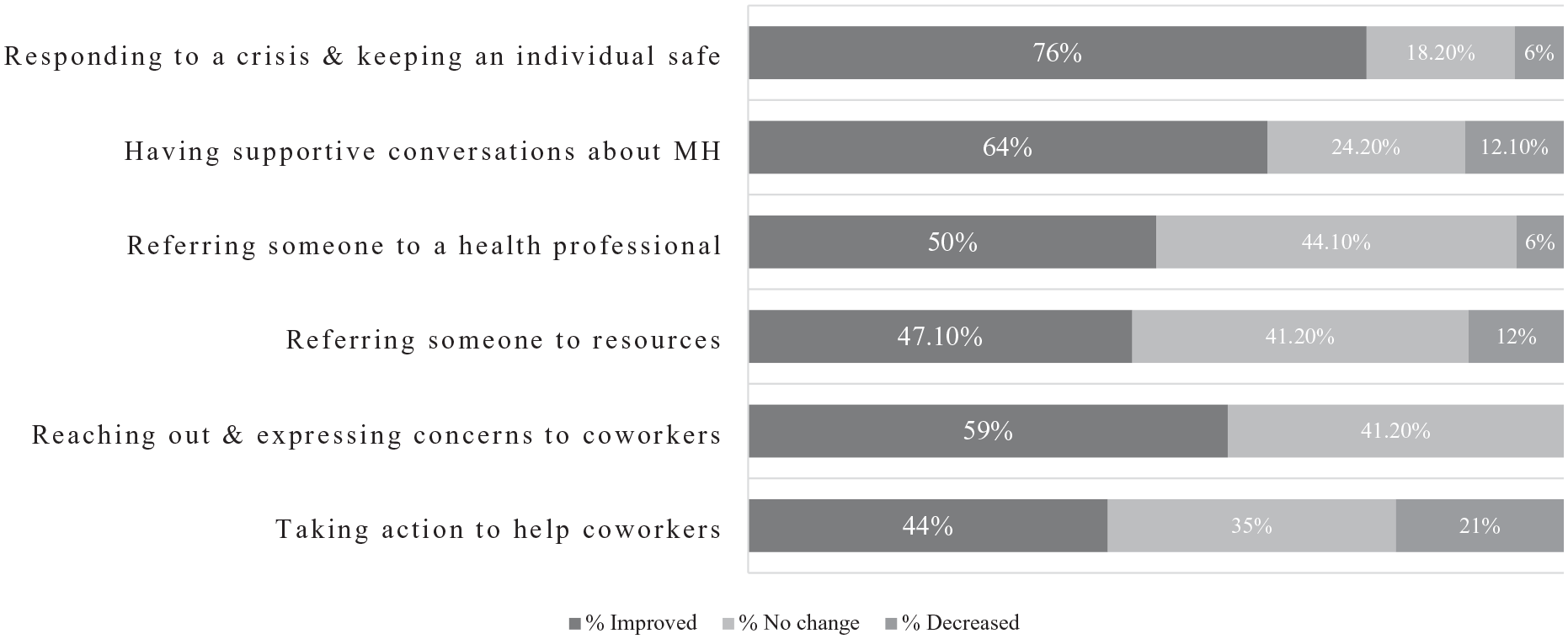
Change Among MHFA Participants
Participants Perceptions
Participants were asked about their knowledge, confidence, and skills before and after the training. Figure 2 displays perceptions from the participants of their abilities, with the most notable change being the use of the ALGEE action plan to assist adults (42.4%–100%).
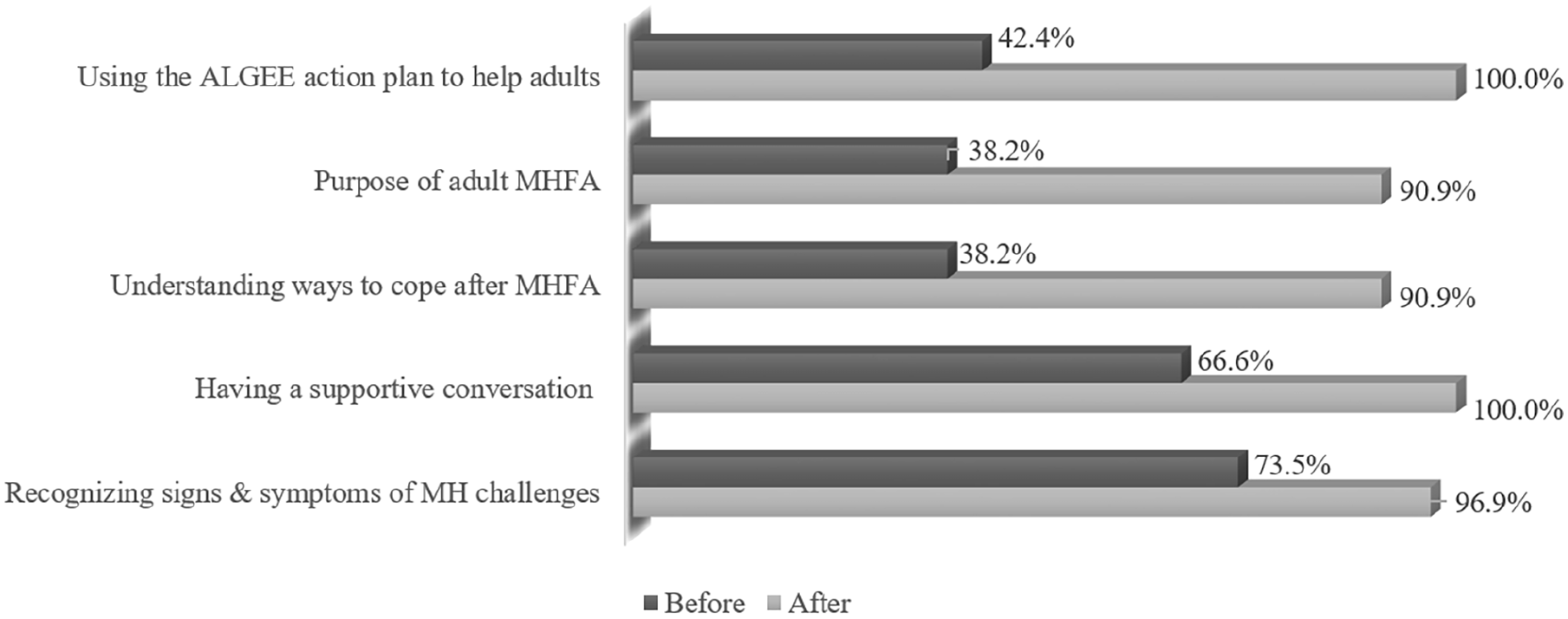
Participants’ Perceptions of Skill (Before and After MHFA Training)
Minimal Change
There were also a few questions in which participants did not have a change in score. For example, 82% of participants did not change their agreement level when asked if they should listen without expressing their judgment to anyone they suspected of experiencing a mental health or substance use challenge(s). This may be due to the initial agreement level, as most participants (90%) agreed with this statement before the training. After training, 96% of participants agreed. There were also mixed results when asked if participants were confident in asking individuals whether they are considering killing themselves: 20% had no change, 26% increased by one level of confidence, and 14% decreased by one level of confidence.
YMHFA
Knowledge
After completing the YMHFA training, 100% of participants knew (a) ALGEE action plan statements, (b) the most common protective factor for youth resilience, (c) actions within the scope of a First Aider, and (d) how to cope with feelings of discomfort or frustration associated with providing YMHFA. Most participants felt that they became more knowledgeable about YMHFA and the role of the First Aider (69%), the ability to recognize the signs and symptoms of mental health or substance use challenges that may impact youth (64%), explain the impact of traumatic experiences and the role of resilience on adolescent development (60%), have a supportive conversation with youth experiencing signs and symptom(s) of a mental health or substance use challenge (60%), and use the ALGEE action plan to assist youth experiencing a mental health or substance use challenges to appropriate resources (70%).
Confidence and Skills
Most participants also experienced a positive change in their confidence surrounding mental health and their ability to take action. 67% of participants showed increased confidence by at least one level of confidence when asked if they could have a supportive conversation with anyone about mental health or substance use challenges, if they could respond to a substance use crisis, and know what to do to keep an individual safe (62%), and if they can ask anyone directly whether they are considering killing themselves (62%). In addition, 60% of participants increased by at least one level of likelihood when asked if they express concerns to any person about mental health signs and symptoms that they are experiencing, which may help that person seek timely support.
Participants Perceptions
After completing the training, participants were asked about their knowledge, confidence, and skills. Some participants felt knowledgeable of each of these areas before the training: using the ALGEE Action Plan (46%), the purpose of YMHFA (44.9%), having supportive conversations (70%), recognizing signs and symptoms (78%), and understanding trauma and resilience in youth development (60%). However, after the training, participants (100%) felt more knowledgeable in each of these areas.
Minimal Change
Similar to MHFA, there were a few questions where participants did not have a change in score. For example, 68% of participants did not change their agreement level when asked if they should take action to help the youth they work with to address their mental health or substance use challenge(s). 52% of participants did not change their level of agreement when asked if they should reach out and express their concerns to the youth they work with that might be experiencing a mental health or substance use challenge(s), which may be due to pretraining agreement levels. Before the training, when asked if they should take action, 80% of participants generally agreed that they should, and when asked if they should express their concerns, 71% generally agreed that they should reach out and express their concerns.
In addition, 92% of participants did not change their agreement level when asked if they should listen without expressing their judgment to the youth they suspect of experiencing a mental health or substance use challenge(s). Similar to the above findings before the training, 98% of participants generally agreed that they should listen without expressing judgment. There were also several questions surrounding resources and referring youth to health professionals. While there was minimal change, participants generally felt less difficulty referring youth to resources and health professionals after the training.
Discussion
Similar to other findings (Banh et al., 2019; Childs et al., 2020; Corona et al., 2020; Hadlaczky et al., 2014; Lee & Tokmic, 2019; Robertson et al., 2021), many of the current study’s participants experienced increased knowledge, confidence, and agreement when asked about mental health topics and working with either adults or youth. Some participants may feel comfortable providing knowledge to adults; however, we found that some conversations (e.g., suicide) might be uncomfortable for some, even after completing this training. These results highlight the continued need to discuss mental health with adults and youth, even if the conversations may be challenging; this is especially true given the prevalence of mental health problems. Discussions can help empower youth and future generations to assist and understand mental health within their communities. Even for items that experienced minimal change, we found a positive increase in participants’ confidence, ability to take action, and support others (e.g., resources and referring).
There are limitations to this study that should be addressed. The sample was not diverse in terms of race, gender, and levels of education. More diverse contexts and participants should be examined in the future, especially since there are ethnic and racial differences in mental health. These differences may be due to racial discrimination, stressful life events, resource access, and unfair treatment (Williams, 2018). In addition, future research needs to examine how these findings change over time and how they may affect the aid recipients.
Implications for Practice and/or Policy and Research
These results highlight the continued need to discuss mental health and empower people to get the help they need, including focused suicide prevention trainings. MHFA and YMHFA are efficacious programs to improve mental health literacy for adults in agricultural communities. Cooperative Extension is an effective mechanism to deliver trainings as Extension has offices in most counties across the United States. Some areas with minimal or no improvement may be indicative of stigma related to mental health generally or within agricultural communities, specifically (Baker et al., 2022). Practitioners must consider how agricultural communities think of stress, mental health, and suicide and tailor programs to be responsive to community concerns and reduce stigma. Tailored programs could include agriculture-specific coded language about suicide to improve awareness of how those working in the agricultural industry indicate they might be experiencing suicidal ideation.