
Abstract
Health-related social needs (HRSNs), like unstable housing, inability to afford utilities, food insecurity, unreliable transportation, and lack of personal safety, profoundly affect people’s health and well-being. Between 2017 and 2022, awardees of the Accountable Health Communities Model (AHC) addressed the health-related social needs of Medicare and Medicaid beneficiaries through screening, referral, and community navigation services. Using and sharing HRSN data between clinical and community partners was a critical component of these efforts. This article shares findings from focus groups and interviews with 19 AHC awardees and seven of their partners. It explores the following:
1. Whether sharing HRSN data with clinical partners informed clinical care
2. Successes and challenges related to sharing data with community-based organizations (CBOs) and clinical partners
3. How awardees collected and used HRSN data to advance health equity
Half of awardees interviewed documented HRSNs in electronic health records and shared aggregated HRSN data with CBOs. HRSN data enabled some clinicians to adjust patient care, although most were uncertain about how to do so. Participants described how sharing HRSN data with communities informs program and funding priorities to improve equity. However, CBOs noted that they had limited incentive to participate in data-sharing platforms. Our work highlights opportunities to provide guidance to clinicians on how to use HRSN screening results in care, standardize HRSN screening results in electronic health records, and co-create data-sharing initiatives with CBOs and patients to ensure meaningful participation.
Health-related social needs (HRSNs), such as unstable housing, inability to afford utilities, and food insecurity, can profoundly affect people’s ability to access care and their overall health and well-being (Braveman & Gottlieb, 2014). Universal HRSN screening, referral, and community service navigation can help address HRSNs. Navigation involves a care navigator connecting patients to social services. A critical component of referral and navigation is using and sharing HRSN data among clinical and community partners. HRSN data sharing can also advance health equity by illuminating disparities and gaps in community services (Alcaraz et al., 2017, 2020).
This study highlights the HRSN data-sharing experiences of Accountable Health Communities (AHC) awardees. Designed and implemented by Centers for Medicare & Medicaid Services (CMS) Innovation Center, the AHC Model launched in 2017 and concluded in 2023 (Centers for Medicare and Medicaid Services [CMS], 2023). It supported 28 awardees, including health systems, academic institutions, community-based organizations (CBOs), health information exchanges, and health departments, across 21 states to implement universal HRSN screening and referral for Medicare and Medicaid beneficiaries and navigation services for eligible individuals.
The AHC Model required awardees to securely share identifiable, self-reported, patient-level data on the results of HRSN screening and navigation with the CMS Innovation Center. Though the Model did not have specific requirements for sharing HRSN data with clinical or community partners, several awardees elected to use closed-loop referral systems to do so. Closed-loop referral systems link to electronic health records (EHRs), enable health care staff to refer patients to CBOs, and enable CBOs to report whether an individual followed through on referrals and had their HRSNs addressed.
While research is available on barriers and facilitators to CBO involvement in HRSN data sharing, relatively few studies have explored clinicians’ perspectives on data sharing. This study explores (1) whether sharing HRSN data with clinical partners informed clinical care, (2) the successes and challenges related to sharing data with CBOs and clinical partners, including through closed-loop referral systems, and (3) how awardees collected and used HRSN data to advance health equity.
Method
We conducted, recorded, and transcribed six, hour-long focus groups with two to five participants each and three interviews with awardees and their clinical and community partners in March 2022. Participants were recruited via a series of emails sent to all awardees. If participants expressed interest, we asked whether they shared data with their clinical and CBO partners and whether they would provide the names and contact information for partners with whom we could speak. Twenty-six participants agreed to participate, representing 19 of 28 awardees, one health information exchange partner, three clinical partners, and three CBO partners. Questions included whether and how HRSN data were shared with clinical and community partners, used to inform clinical care, or used to advance equity.
We coded and analyzed transcripts using thematic analysis (Braun & Clarke, 2006). Initially, our team of four researchers each reviewed and coded one to two transcripts, identifying how clinicians and CBOs use HRSN data, barriers and facilitators to HRSN data sharing and use for clinicians and CBOs, and uses of HRSN data to advance equity. The team met to discuss identified themes related to these topics and reached consensus on codes to consistently represent concepts. The team then coded all transcripts, with two team members coding each one. We discussed newly emerging themes and resolved discrepancies in applying codes.
Results
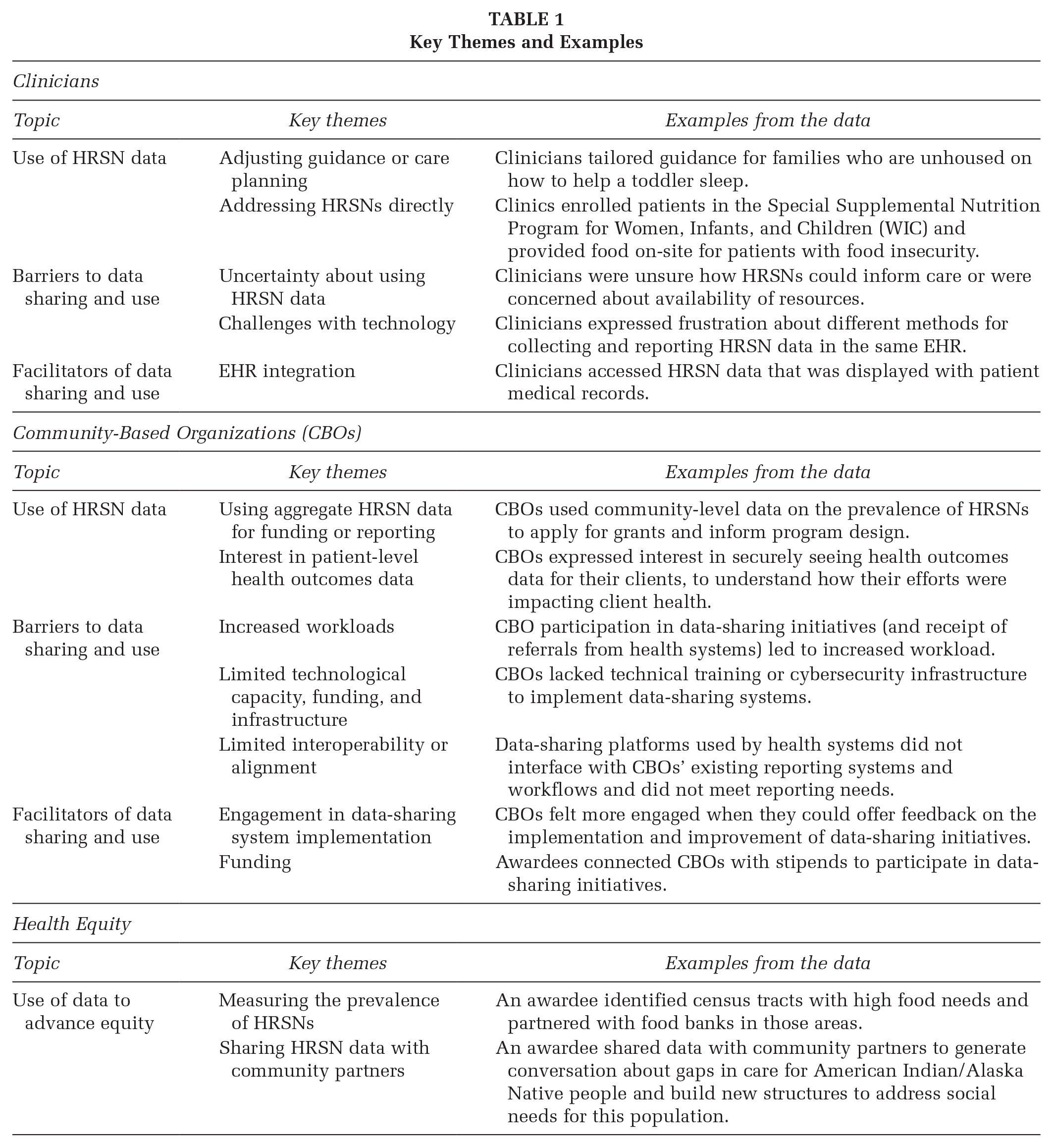
Of the 19 awardees, 11 reported that some or all clinical partners had access to HRSN screening results through EHRs, and 12 shared HRSN data with CBOs. Nine awardees used a closed-loop referral platform. Below we describe how clinicians and CBOs used HRSN data, barriers to and facilitators of HRSN data sharing and use, and opportunities to support equity with HRSN data. Table 1 summarizes key themes related to these topics.
Key Themes and Examples
Clinicians’ Perspectives
Clinicians’ Use of HRSN Data
Participants provided mixed input on whether and how clinicians use HRSN data. Some clinicians used HRSN data to inform care plans and adjust guidance to patients’ needs, such as tailoring advice on helping toddlers sleep for families who were unhoused. Three awardees also shared that some clinicians address social needs directly, for example, by providing free food on site to patients with food insecurity or working with staff to enroll patients in federal assistance programs for food and nutrition.
Barriers to Data Sharing and Use
Awardees reported being unsure whether clinicians used or viewed the screening data to which they had access. Although some clinicians were aware that their patients had HRSNs, they were uncertain how this could inform care. One participant noted that care navigators have a critical role in helping clinicians understand how to use HRSN data to impact care. However, managing communication between care navigators and clinicians was a challenge, particularly when staff worked remotely. Some clinicians felt that asking patients about HRSNs was not helpful if resources were not available to address them.
In addition, participants faced challenges with technology, including lack of interoperability across the EHR systems used by different clinical partners, or even when sharing data using the same EHR. For example, one clinical partner noted that each department used different methods for collecting and reporting HRSN data in the EHR.
Facilitators of Data Sharing and Use
Despite the challenges, integrating screening tools into EHR systems enabled data sharing with clinicians. Awardees noted that clinicians were more likely to review patient-level HRSN data if they were in the EHR, and some participants mentioned that they were working toward EHR integration of screening information.
CBOs’ Perspectives
CBOs’ Use of HRSN Data
Awardees typically shared aggregate data with CBOs, such as rates of identified HRSNs across clinical partners. Although CBO partners used aggregate data to apply for grants and inform program design, two CBO partners emphasized a desire to also receive patient-specific and identifiable data on HRSNs and health outcomes. Patient-level data would enable CBOs to see which HRSNs their clients reported, track people who are at risk of negative health outcomes, and study whether their interventions affected their clients’ health. CBOs also valued patient-level data for funding and reporting. One CBO shared that funders often consider health system data more valid than self-reported health data.
Barriers to Data Sharing and Use
When asked about challenges and barriers with closed-loop referral systems, CBOs and awardees said that these systems often did not interface with their existing data collection systems, nor align with their workflows or reporting needs. Although CBO partners recognized the benefits of closed-loop referral systems for clinical-community communication, two CBO partners largely saw the closed-loop referral system they accessed through the AHC Model as simply another way to receive a referral rather than a data-sharing mechanism.
In addition, technical capacity and infrastructure challenges were common across CBOs. Awardees noted that CBOs had challenges training staff on new systems, difficulty maintaining access because of volunteer turnover, and barriers to implementing the cybersecurity infrastructure necessary to protect information in a closed-loop referral system.
Facilitators of Data Sharing and Use
Two CBO partners emphasized the importance of meaningfully and equitably engaging CBOs and communities in data-sharing initiatives. Asking CBOs to provide feedback on data-sharing systems supported their engagement with and use of those systems. They shared that, with encouragement from awardees, they felt comfortable providing candid feedback on the type of data that would be most useful to their organization and the communities they served.
Funding is another factor that supported CBO engagement with data-sharing systems. Although the AHC Model did not allow awardees to pay for community services using CMS Innovation Center funds, awardees described efforts to connect their CBOs with other sources of funding. One awardee identified funding to provide CBOs with stipends to participate in data-sharing initiatives, and another helped CBOs identify philanthropic grants. Awardees underscored the importance of allocating funding to CBOs to support their overall capacity and ability to devote more staff time to HRSN data-sharing initiatives.
HRSN data and equity
Awardees used HRSN data to understand health inequities and measure the prevalence of HRSNs in populations throughout their community. For example, one awardee used aggregate data to identify census tracts with greater food needs and encouraged food banks to send mobile food bank trucks to those areas. Awardees also shared aggregate data with community partners to guide conversations about how to allocate resources. One organization used HRSN data to show that American Indian/Alaska Native (AI/AN) populations were experiencing higher rates of social needs, which generated conversation about gaps in care outside of reservations and led to structures to provide social services tailored for AI/AN people in urban areas. Participants were also concerned about patients’ privacy and safety when handling sensitive information and emphasized the importance of ensuring that data sharing ultimately benefits patients.
Implications for Practice
Screening for HRSNs is becoming part of standard care, evidenced in part by the Center for Medicare and Medicaid Services (CMS)’s recent adoption of quality measures to promote screening among hospitals (CMS, 2022b). Our work reveals important considerations for ensuring that HRSN screening results are used and shared across sectors to support patients, including (1) supporting clinicians with using HRSN data to inform care, (2) engaging CBOs and patients in the design and implementation of data-sharing systems, and (3) strengthening CBO participation.
While having HRSN screening data available in EHRs drew clinicians’ attention to the data, clinicians were sometimes unsure what to do with the results. Implementing EHR systems to facilitate dialogue across care teams (e.g., by enabling care navigators to flag HRSNs that may affect care plans) could support clinicians. Sharing guidance within the EHR on how to adjust care to accommodate social factors affecting patients or identifying a common method for displaying HRSN results across the health care system could encourage cross-disciplinary coordination (Cantor & Thorpe, 2018; Chen et al., 2020; United States Department of Health and Human Services, Assistant Secretary for Planning and Evaluation, Office of Health Policy 2018).
Our research affirms a lack of coordination between health systems and CBOs, with some CBOs asked to participate in multiple referral platforms that do not align with their existing systems (Trenton Health Team, 2021). Convening CBOs and health systems to select a common platform helps to address this challenge (CMS, 2022a). Participants also emphasized the importance of addressing equity when developing and implementing data-sharing systems, including balancing power and decision-making across health systems, CBOs, and patients, and ensuring that data-sharing initiatives prioritize patients’ privacy, security, and well-being. Although some participants in our study gathered CBOs’ feedback on data systems, few co-created data-sharing initiatives among participants. Community information exchange (CIE) models, which couple information sharing and interoperability with community governance, present a promising strategy for co-designing data-sharing initiatives between health care systems, public health, and patients or community members (Center for Health Care Strategies, 2023; Grounds & Johnson, 2021). More practice-focused research detailing the CIE design and implementation process could support organizations in initiating these systems or in increasing the equity focus of existing data-sharing initiatives.
Consistent with prior research, participants in our study noted the importance of funding CBOs to build internal capacity as well as nonmonetary incentives for CBO participation in HRSN data-sharing initiatives (Cartier et al., 2020; Trenton Health Team, 2021). Specifically, CBOs were interested in accessing their clients’ health outcomes data (with appropriate permissions and safeguards) to better understand client and community needs and demonstrate their impact on HRSNs and health outcomes to funders. Currently, the Agency for Healthcare Research and Quality (AHRQ) encourages primary care organizations to use secure data dashboards to monitor performance on quality metrics related to health outcomes and social needs (Agency for Healthcare Research and Quality [AHRQ], 2015). As organizations develop dashboards for clinical care, they could consider engaging CBOs in selecting HRSN-related metrics to monitor and sharing relevant dashboard components with them.
Conclusion
Although closed-loop referral systems and data-sharing technology can support efforts to address HRSNs and advance health equity, there are gaps in implementing these technologies. Our work revealed clinician uncertainty about using screening results, limited incentive for CBO participation, and a lack of patient input into system design. These gaps demonstrate the importance of coupling data-sharing technology with relationships between health systems, CBOs, and patients to ensure that technology supports all stakeholders’ needs and that data-sharing initiatives serve communities.
Footnotes
Authors’ Note:
We would like to thank the AHC Model awardees and their partners who shared their experiences with us. We would also like to thank the many CMS and Mathematica staff who reviewed and provided input on this manuscript. Funding provided by Centers for Medicare & Medicaid Services, Contract [HHSM-500-2014-00034I].