
Abstract
Background
Diabetes affects millions of people in the United States and poses significant health and economic challenges, but it can be prevented or managed through health behavior changes. Such changes might be aided by voice-activated personal assistants (VAPAs), which offer interactive and real-time assistance through features such as reminders, or obtaining health information. However, there are little data on interest and acceptability of integrating VAPAs into programs such as the National Diabetes Prevention Program (National DPP) or diabetes, self-management, education, and support (DSMES) services.
Methods
We conducted individual and small-group semi-structured interviews of National DPP and DSMES staff and program participants. We used rapid-turnaround qualitative thematic analysis to identify emerging themes using an adapted version of the Consolidated Framework for Implementation Research (CFIR).
Results
Nearly all program participants and staff had prior experience with VAPAs, but not in the context of these programs. Most program participants felt confident in their ability to use VAPAs but were concerned about their privacy and security. Program staff were optimistic about the feasibility of integrating VAPAs into existing programs given their ability to support healthy habit formation, but staff were less optimistic about using VAPAs to share health information. Program staff also felt that additional resources to support VAPA use would help ensure that VAPAs would not create an extra burden on staff and program participants.
Implications
Integrating VAPAs as a resource to enhance mobile applications already in use shows potential to support health behavior change. Future research should include how this technology could be further optimized to enhance utility.
Keywords
Diabetes affects more than 37 million people in the United States (Centers for Disease Control and Prevention, 2022b) and is costly to control (American Diabetes Association, 2018). However, it can be prevented or managed through the adoption of healthy behaviors (Centers for Disease Control and Prevention, 2022c). Making behavior change easier can help people form healthy habits to prevent and manage chronic diseases (Service et al., 2014). In this context, voice-activated personal assistants (VAPAs) are gaining attention for their potential to help people make lifestyle changes through features such as offering interactive and real-time support or information, and facilitating use of mobile applications or features for individuals with lower literacy or disabilities (Bérubé et al., 2021).
VAPAs are digital assistants that use voice recognition, language-processing algorithms, and voice synthesis to receive specific commands and offer relevant information or perform specific functions as requested (Hoy, 2018). Examples of VAPAs include Google’s Assistant, Apple’s Siri, and Amazon’s Alexa. VAPAs can be accessed through a variety of platforms, including smart speaker or display devices, or through built-in voice assistants on smartphones, smartwatches, and tablets. VAPA use is common. In 2022, 62% of American adults reported using VAPAs on any device (Edison Research, 2022). Recent studies underscore the potential of VAPAs in health-related contexts. For instance, one study conducted among older adults in the United Kingdom found VAPAs to be acceptable and utilized for activities such as medication reminders and management of diet and exercise (Balasubramanian et al., 2021). A separate study highlighted the usability of VAPAs for pain management among older adults (Shade et al., 2020). Two prior reviews have demonstrated how behavioral health and chronic disease management interventions using VAPAs have high feasibility, usability, and acceptability and can support self-management and promote healthy lifestyle behaviors (Bérubé et al., 2021; Sezgin et al., 2020).
Despite this growing body of research and common usage of such devices, there is a notable gap in the literature regarding the specific application of VAPAs to support people in making healthy behavior changes as part of chronic disease prevention or management programs—such as the National Diabetes Prevention Program (National DPP) lifestyle change program or diabetes self-management education and support (DSMES) services. The National DPP lifestyle change program is a structured, evidence-based, yearlong program that focuses on modest behavior changes, like healthy eating and physical activity, to help people prevent or delay type 2 diabetes (Centers for Disease Control and Prevention, 2022a). DSMES services include teaching personalized, ongoing strategies to help participants manage their diabetes (Beck et al., 2017). Moreover, it is also unclear as to whether VAPA usage would be feasible or as accessible in communities that are historically underserved and may have more limited access to such devices.
The goal of this Centers for Disease Control and Prevention (CDC)-funded study was to understand how VAPAs could be incorporated into the National DPP and DSMES services to support lifestyle change for people with diabetes or at risk for type 2 diabetes.
Method
Guiding Framework for Data Collection
We used an adapted version of the Consolidated Framework for Implementation Research (CFIR; Rojas Smith et al., 2014) to develop formative evaluation questions and data collection instruments (Figure 1).
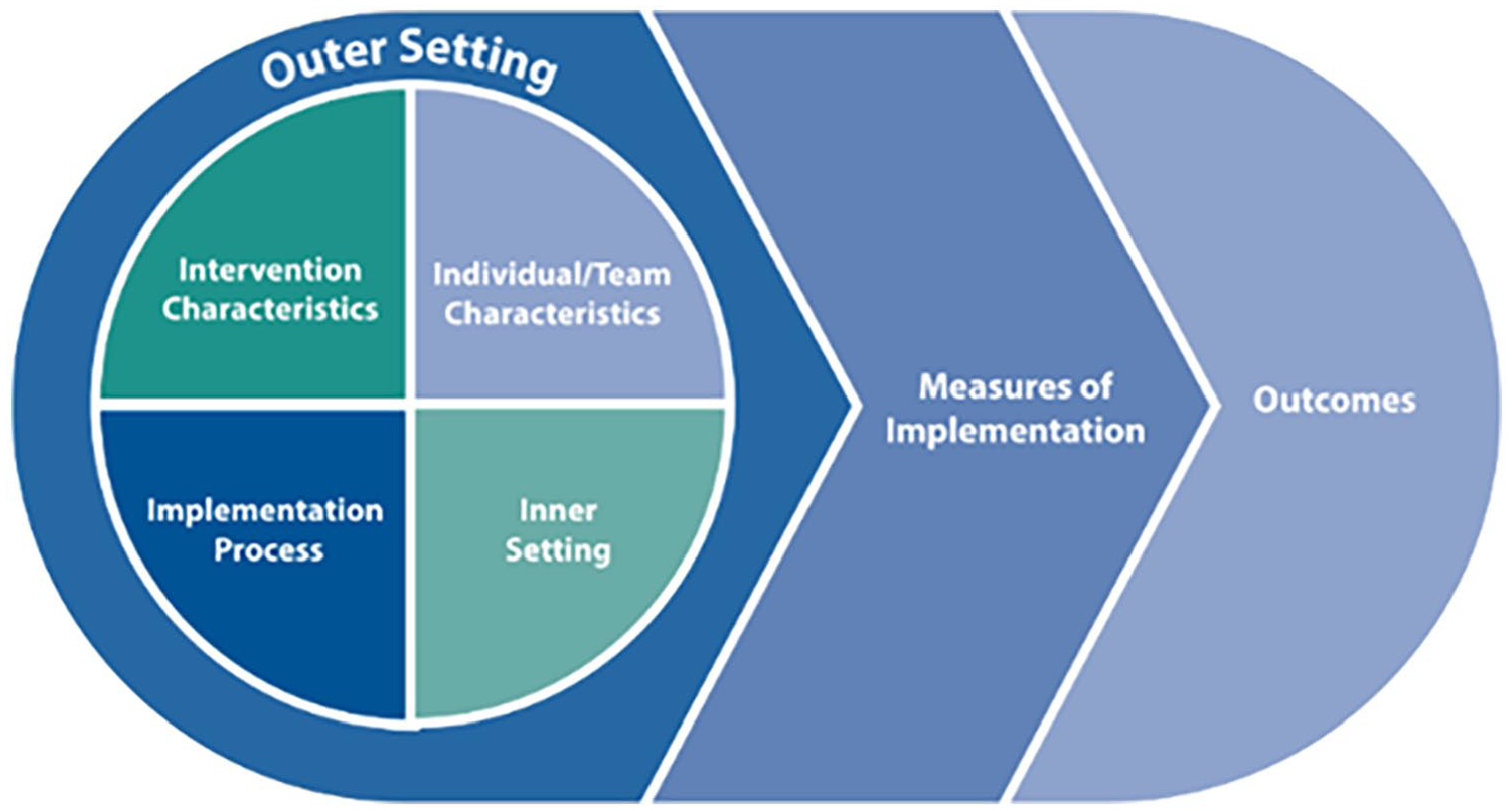
Adapted Consolidated Framework for Implementation Research (CFIR) to Inform Technical Approach (Rojas Smith et al., 2014)
CFIR consists of five domains: inner setting, outer setting, intervention characteristics, characteristics of individuals involved, and implementation process (Damschroder et al., 2009). The adapted CFIR adds outcome constructs to the original framework, including measures of implementation and any outcomes related to the intervention itself (Rojas Smith et al., 2014). By following the adapted framework, we considered the relevant community factors, organizational characteristics, and barriers and facilitators that might affect the use of VAPAs (Table 1).
Study Evaluation Questions Mapped to Relevant Adapted CFIR Domains and Constructs
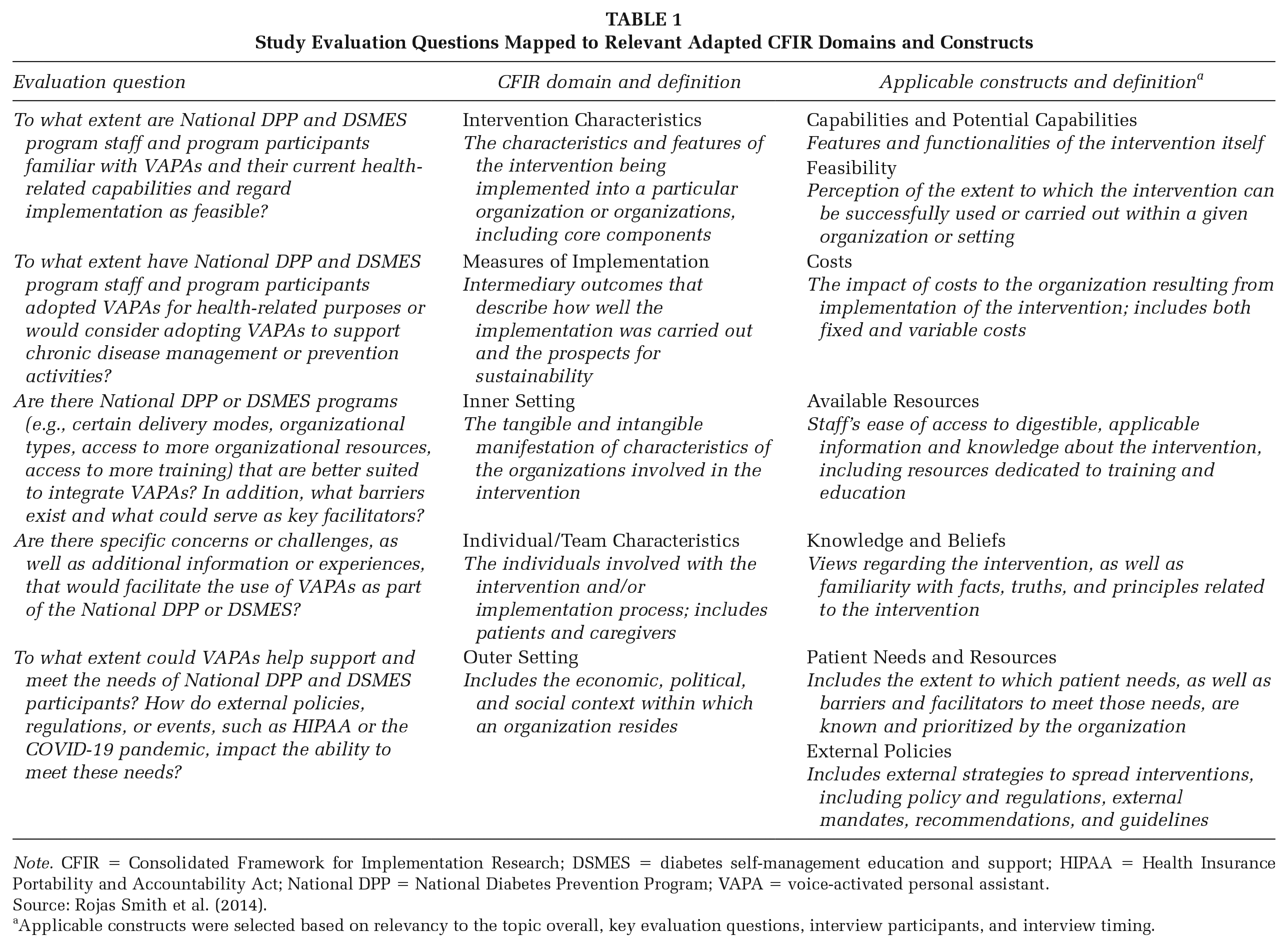
Note. CFIR = Consolidated Framework for Implementation Research; DSMES = diabetes self-management education and support; HIPAA = Health Insurance Portability and Accountability Act; National DPP = National Diabetes Prevention Program; VAPA = voice-activated personal assistant.
Source: Rojas Smith et al. (2014).
Applicable constructs were selected based on relevancy to the topic overall, key evaluation questions, interview participants, and interview timing.
Site Selection and Data Collection
We worked with CDC staff to identify National DPP and DSMES programs. We prioritized programs that work with historically marginalized populations, meaning individuals disadvantaged by their social or economic status, geographic location, and environment (Healthy People 2030, n.d.) to understand the potential for exacerbating health inequities by using VAPAs in these programs. We selected programs that were diverse in terms of the geographic location (e.g., urban and rural), organizational type (e.g., a mix of federally qualified health centers, health systems or clinics, community-based organizations), and delivery mode of services (e.g., online, in-person, or mixed). In addition, all recruited programs worked primarily with either historically marginalized racial groups, individuals served by uninsured, Medicare, and/or Medicaid insurance status, or individuals with lower educational attainment. We recruited programs via email and asked administrative staff and Lifestyle Coaches (National DPP) and diabetes care and education specialists (DSMES) who support program delivery to participate in 60-minute virtual interviews. Before the interview, all program staff and participants received a brief document describing VAPAs, the most common brands of VAPAs, and VAPA capabilities. Neither program staff nor participants needed to be familiar with VAPAs to participate in the interviews.
We conducted virtual individual interviews of program staff, although on several occasions, multiple staff from the same organization were interviewed together. Following the interview, program staff identified and introduced the research team to program participants who were eligible and could be recruited to participate in 90-minute virtual small-group interviews. Program participants were interviewed in groups of two or three. All participants were at least 18 years old and spoke English. Given our selection of specifically historically marginalized programs, we did not collect participant demographic information to minimize any potential discomfort that might deter participation. Program participants had to be currently enrolled in their respective program or have completed their program within a year of the interview. Program staff and participants each received a $50 gift card as an incentive.
In addition, we used an online poll conducted through Mentimeter during the small-group interviews to help guide the discussion. We obtained verbal consent from each respondent before each interview. Interviews were audio recorded and transcribed verbatim for analysis. Research Triangle Institute (RTI) International’s Institutional Review Board approved the study in November 2022.
Analysis
We used rapid-turnaround qualitative analysis (Hamilton, 2020) to examine the data, which is ideally suited in instances where interested parties must quickly obtain insights needed to make timely decisions regarding strategy and practice (Hamilton, 2020). This involved first developing a template to condense the qualitative data and document key findings. The research team then developed matrices to identify emergent themes by CFIR construct. The matrices included separate worksheets for each interview type. As a final step, we assigned domains to co-authors to review and analyze across participant and program types. We categorized themes as applying to a few interview participants (0%–19%), some participants (20%–39%), about half of participants (40%–59%), most participants (60%–99%), and all participants (100%). For the poll questions, we conducted descriptive analyses, and the responses are reported in aggregate below.
Results
Overall, we interviewed nine staff members from eight National DPP programs, nine staff members from seven DSMES programs, eight National DPP participants, and nine DSMES participants. The National DPP organizations included one Federally Qualified Health Center, four community health centers, and three community-based agencies/organizations. Three DSMES sites were located within independent health care clinics, and four were affiliated with academic medical institutions.
The eight National DPP participants were from four different programs. Seven participants were female, and one was male. Each of the nine DSMES participants was from a different program. Four of the participants were male, and five were female. We present the results of our analysis of all interviews by CFIR domain below, in addition to displaying the emerging themes in Table 2.
Overview of Emergent Themes by CFIR Domain
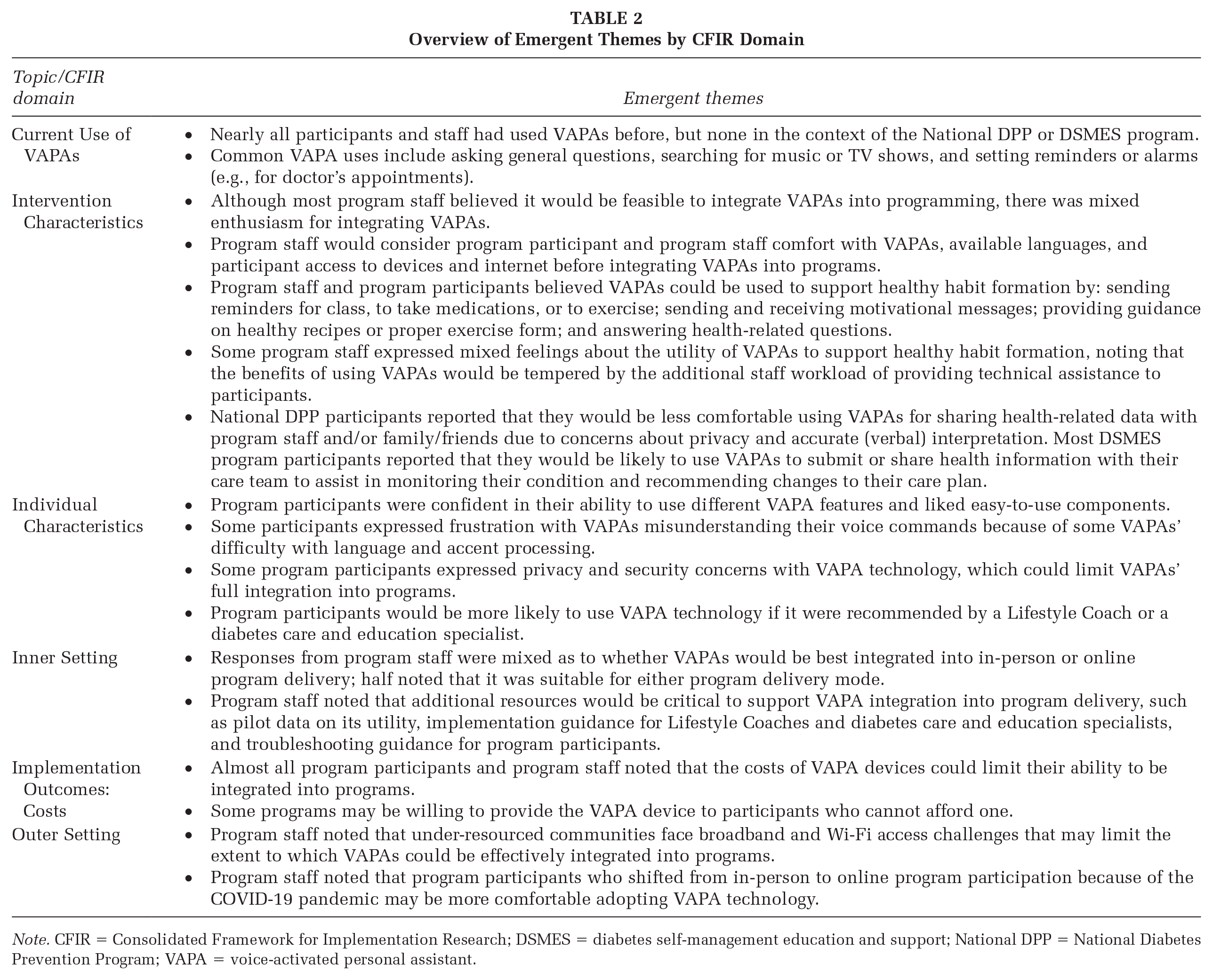
Note. CFIR = Consolidated Framework for Implementation Research; DSMES = diabetes self-management education and support; National DPP = National Diabetes Prevention Program; VAPA = voice-activated personal assistant.
Current Use of VAPAs
Most program staff reported that they currently used VAPAs at home, and about half had used VAPAs at work in some capacity. No program staff had ever used VAPAs in the context of delivering the National DPP or DSMES program. Smartphones were the devices used most often to access VAPAs in both settings, although about half of the staff also mentioned using smartwatches at home.
All DSMES program participants and most National DPP program participants had used VAPAs before. Table 3 summarizes the specific VAPA type by program participant type.
Current Use of VAPAs Among Program Participants
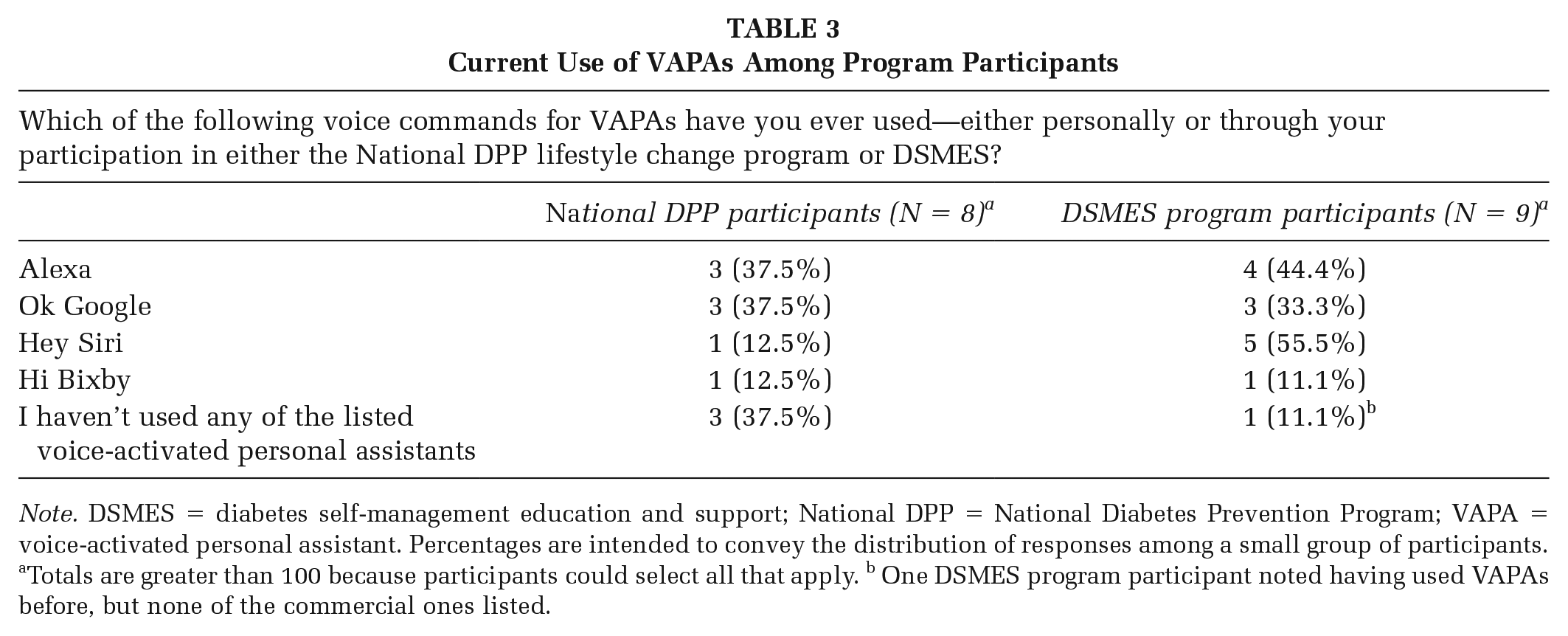
Note. DSMES = diabetes self-management education and support; National DPP = National Diabetes Prevention Program; VAPA = voice-activated personal assistant. Percentages are intended to convey the distribution of responses among a small group of participants.
Totals are greater than 100 because participants could select all that apply. b One DSMES program participant noted having used VAPAs before, but none of the commercial ones listed.
Most program participants reported using VAPAs for general purposes, such as asking for directions or the weather forecast, or searching for music. The frequency of using VAPAs among program participants varied; a few reported using VAPAs several times a week to several times a day, whereas several participants said they used VAPAs a few times per month. Approximately half of participants had used VAPAs for health-related reasons. For example, some participants said they currently use VAPAs to set reminders to attend workout classes or upcoming doctor’s appointments. One participant reported using VAPAs to search for healthy recipes and information on diabetes symptoms.
Intervention Characteristics
Feasibility
Most program staff said it would be feasible to integrate VAPAs into National DPP and DSMES programs. However, several factors would need to be considered: (a) program participants’ comfort and skill level with VAPAs; (b) VAPAs’ ability to operate in multiple languages; (c) VAPA hardware (device) availability among participants; (d) the need for high-speed internet access, especially for participants in rural areas and/or for those using a smart device that needs an internet connection; (e) program staff familiarity and comfort with VAPAs; and (f) gradual introduction of VAPAs into classes/sessions.
Some program staff expressed great enthusiasm around the idea of integrating VAPAs, reporting that most of their program participants have access to a smartphone. One staff member also stated that if a familiar and trusted source of information discussed the use of VAPAs with participants—“like you’re talking to family or a friend”—then it would be feasible. One staff member said that it would not be feasible to integrate VAPAs into the current program; they could envision this only if an implementation toolkit was developed and presented to staff “on a silver platter.”
VAPA Capabilities
Overall, program staff and participants believed that VAPAs could be used to support healthy habit formation. Regarding reminders, all DSMES participants rated themselves as “very likely” or “somewhat likely” to use VAPAs to set reminders, and most but not all National DPP participants noted they were “very likely” or “somewhat likely” to use VAPAs for this purpose (Table 4). One DSMES participant said that as they have aged, it has become helpful to have VAPAs remind them to complete tasks such as taking medication, whereas one National DPP participant expressed dislike of speaking to a device. Overall, participants said that knowing their data were secure would make them “very likely” or “somewhat likely” to use VAPAs to set reminders.
Likelihood, Interest, and Confidence in Using VAPAs by Program Participants
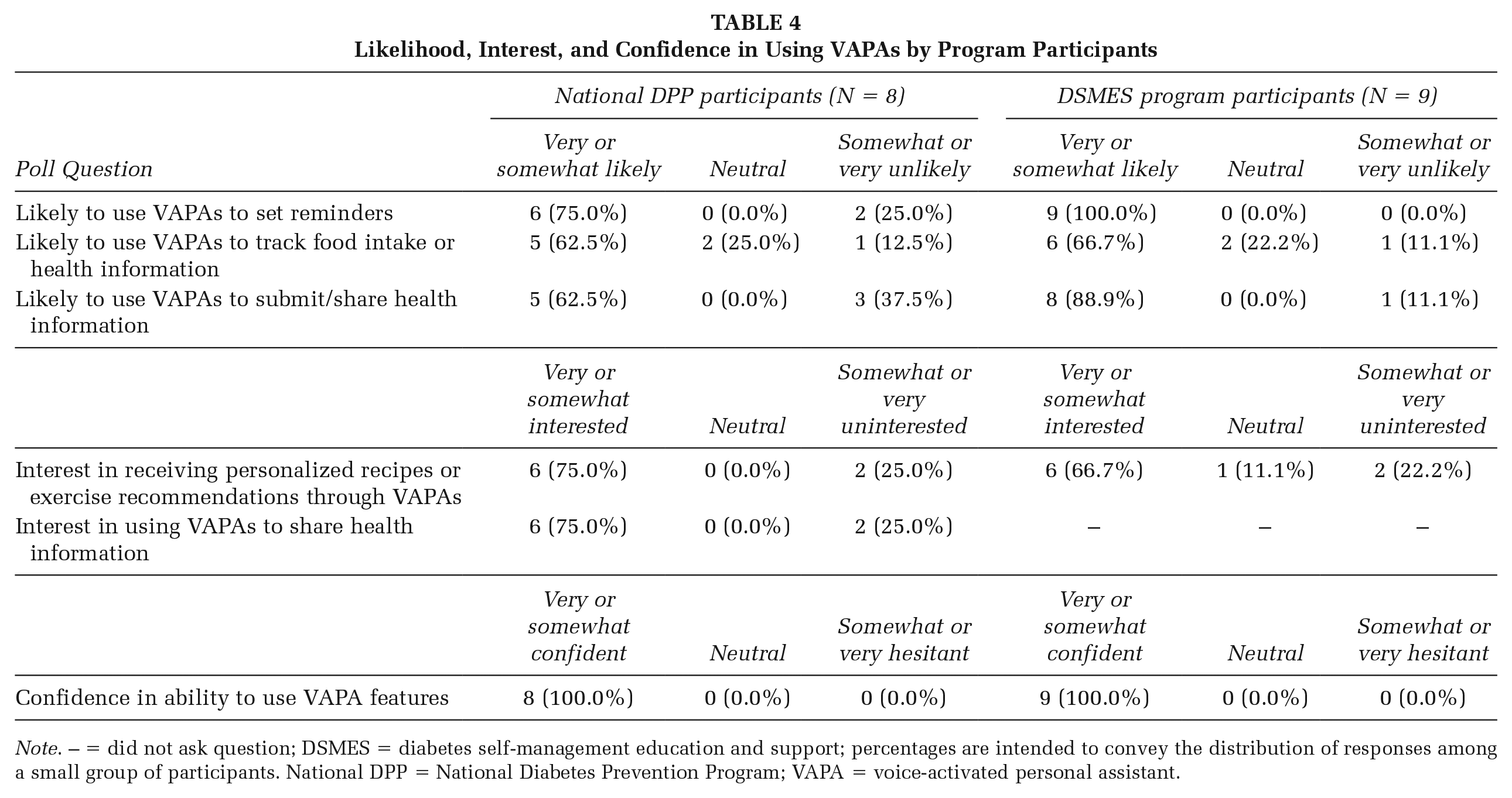
Note. – = did not ask question; DSMES = diabetes self-management education and support; percentages are intended to convey the distribution of responses among a small group of participants. National DPP = National Diabetes Prevention Program; VAPA = voice-activated personal assistant.
Some program staff also thought VAPAs could provide motivational messages to participants, such as telling them to keep up the good work; providing guidance on new skills (e.g., ingredient substitution during meal prep, proper exercise form); and/or answering questions about health, nutrition, healthy recipes, and physical activity. Some program participants rated themselves as “very likely” to use VAPAs to track food intake (National DPP participants) or health information (DSMES participants). One participant noted that they were “very likely” to track food intake using VAPAs because it helps to hear the nutrition information aloud in addition to reading it. One participant said they were only “somewhat likely” to use VAPAs to track their food because some devices that have VAPAs do not have the ability to show or take pictures, and they felt that taking and sharing pictures of food increased accountability with their social support network.
Some staff members expressed mixed feelings about using VAPAs to support healthy habit formation. They said it might help participants achieve their goals, but those benefits would be tempered by the additional staff workload of providing technical assistance to participants. Another staff member was doubtful VAPAs would work at all, except for a small percentage of participants. They said that VAPAs would become an annoyance to participants because there are other resources to help with tasks mentioned above (e.g., medication reminders, text messaging with program staff, internet searches).
Notably, the majority of DSMES program participants reported being “very likely” or “somewhat likely” to use VAPAs to share their health information with doctors or diabetes educators, whereas fewer National DPP participants said the same. For instance, one National DPP participant said that sometimes VAPAs do not understand their pronunciation of different health readings, so the data input will be incorrect, thereby limiting trust in VAPAs for sharing important health information.
Individual Characteristics
Personal Experiences
All program participants felt very confident in their ability to use various features of VAPAs, and about half of participants said they liked that VAPAs were convenient and allowed hands-free use while multitasking. Participants felt that using voice commands to log health-related data (e.g., body weight, minutes of physical activity) or search for information was more convenient than typing into a mobile application or search bar. Most participants noted that they liked and often used specific features of VAPAs, including setting reminders, playing songs, logging notes while “on the go,” making a hands-free phone call, using timers for cooking, or monitoring goal progress. For example, one participant noted that it can be a useful tool to monitor progress on daily goals such as meeting a certain step count or drinking a target amount of water; the participant also perceived it as encouraging when goal accomplishments are verbalized.
Personal Beliefs
When asked what they disliked about VAPAs, some participants expressed frustration in communicating with VAPAs, which was caused by either language barriers (e.g., the VAPA did not understand commands spoken in Spanish) or misunderstood voice commands. VAPAs’ misunderstanding of voice commands was attributed to accents or speaking while exercising and out of breath.
Some participants also voiced privacy concerns, such as how and where their data would be stored and used, as well as the possibility that VAPAs are constantly listening (“eavesdropping”) in the background. A few participants expressed discomfort with using VAPAs in public spaces for fear of others hearing their personal information. In addition, a few participants mentioned being selective about the type of information they shared with VAPAs. For example, some would share only information that they would be comfortable with others knowing, and others would use VAPAs only for tasks that they did not perceive as privacy or security related, such as setting reminders, creating recipe lists, or guiding physical activity.
About half of participants said that they would be more likely to use a VAPA if it were recommended by a Lifestyle Coach or diabetes educator. Participants said they trusted that recommendations made by their Lifestyle Coach were vetted and appropriate for enacting lifestyle change.
Inner Setting
Program Features
Overall, most program staff said they would be likely to recommend the use of VAPAs to their program participants. About half of staff felt that VAPAs could be integrated into either in-person or online program settings. Some staff said that in-person programs would be a better match for VAPAs because staff could provide in-person technical assistance with multiple participants at once. In-person programs could also allow participants to help each other, thereby reducing the staff burden. Conversely, several staff members preferred the online setting for VAPAs, because VAPAs could supplement skills useful for making lifestyle changes at-home uses such as reading nutrition labels or exercise demonstrations.
DSMES program staff were more likely than National DPP staff to report that they would incorporate VAPAs into their work. For example, some DSMES staff said they would use VAPAs to dictate patient or clinic notes into charts. National DPP staff generally did not note potential VAPA use for delivering the National DPP lifestyle change program.
Required Resources and Support
All program staff mentioned the need for additional resources and support to facilitate the integration of VAPAs into programs. Program staff frequently mentioned needing evidence on the effectiveness of VAPAs as a resource. Specifically, staff wanted pilot data on VAPA’s usefulness in DSMES and National DPP programs to understand how it aids program retention and may help participants achieve health goals. Staff cited the need for device comparisons, mobile applications that work with VAPAs, and detailed documentation of challenges encountered and potential solutions. Most importantly, such assessments should include people who are from historically marginalized populations (e.g., rural, non-English speaking, uninsured) to ensure that this technology could benefit them.
Program staff noted that they would also need resources to support program participants’ use of VAPAs. Resources should be tailored for those with lower literacy, use plain language, and include guidance on troubleshooting. All materials should be available in multiple languages. Finally, staff stressed the importance of VAPAs as an optional tool for participants rather than a requirement. Some participants may not have a VAPA device, and others may not be comfortable using VAPAs because of the privacy and language concerns previously described.
Implementation Outcomes
Nearly all program participants and staff noted that costs would factor into their decision to use VAPAs. Some participants said that many VAPAs, such as a smart speaker, carry high price tags and therefore are low on the household budget priority list. One DSMES participant noted that since diabetes is expensive to manage, they would not want to pay for a VAPA. When participants were asked whether they would use a smart speaker if it were free, most said that they would; however, a few DSMES participants said that even then they would not want to use it. One participant said that they would not want a separate VAPA-enabled device, such as smart speaker, given that they already have a cell phone and a continuous glucose monitor to keep track of. In addition, a few program participants noted that if VAPAs were incorporated into a free mobile application, they would be more interested in using them, as it would not require purchasing or managing a separate device.
Some program staff mentioned that their organizations may possibly support VAPA access for participants who could not afford it. Given the costs associated with standalone VAPAs, such as a smart speaker, one staff member noted that it might be more feasible to recommend specific mobile applications with a VAPA component, as most participants already own smartphones.
Outer Setting
Many program staff noted that some program participants who live and work in rural areas, and communities with limited Wi-Fi access, may face barriers using VAPAs. Other program staff, however, mentioned that many phone plans include internet access, and VAPA capabilities are built into smartphone devices.
Several program staff noted that the COVID-19 pandemic was initially perceived to be a barrier for in-person program participation and instruction. However, program staff noted that the pandemic actually served as a catalyst for participants to acquire added knowledge and resources. For instance, online and distance learning programs required participants to use mobile devices and web conferencing services, which provided a good foundation for acceptance of VAPAs.
Discussion
To our knowledge, this study is the first to examine the feasibility and perceived value of integrating VAPAs into existing chronic disease prevention or management programs. Overall, both staff and participants see integration as feasible and beneficial. Nearly all staff stated they would be willing to recommend the use of this technology to their participants, and participants had the greatest interest in using features that promote healthy habits including setting reminders to attend workout classes, take medications, or attend doctor’s appointments; sending motivational messages from a Lifestyle Coach or diabetes care and education specialist to support healthy behaviors; and providing nutritional and physical activity information, such as listing nutritional facts or reading healthy recipes aloud. VAPA use could simplify behavior change and support improved health outcomes, as the use of technology as part of diabetes self-management services has been shown to be associated with improved clinical outcomes (American Diabetes Association, 2021). However, program staff stressed the importance of integrating VAPAs as an optional tool rather than a programmatic requirement.
However, participants would need additional guidance on how to use and engage with VAPA for health-related purposes within their programs. Given nearly all participants reported they currently use VAPAs in some context, programs have an opportunity to teach them health-specific applications. For example, programs could consider emphasizing to participants how to utilize the voice-activated features they may already be familiar with to support healthy behavior, such as setting reminders specifically for medication or physical activity, and consider how voice-activated features could add value to mobile applications that are already promoted and widely used in these programs, such as mobile applications that support the logging and tracking of food.
Nevertheless, it is important to note enthusiasm was tempered by concerns and challenges with using VAPAs. The biggest concerns expressed by program staff and participants were related to privacy and security, resulting in participants having less interest in the features of VAPAs that would share personal health information. However, DSMES participants were more likely than National DPP participants to be willing to use VAPAs to share health information. One potential explanation for this may be that DSMES participants are actively managing diabetes; sharing health information with their care team to help monitor their condition may be more applicable to their needs.
It is important to acknowledge that people from historically marginalized communities face well-documented barriers to participating in chronic disease prevention and management programs, such as financial and transportation challenges and language and literacy barriers (Canedo et al., 2018; Morgan et al., 2018; Hill-Briggs et al., 2020; Powers et al., 2020). Our interviews with program staff and participants from historically marginalized communities affirmed these barriers persist when considering the feasibility of integrating new digital technology, specifically posed by costs, digital literacy, internet access, and language barriers. To ensure the adoption of new digital technologies like VAPAs does not inadvertently widen existing health inequities (Yao et al., 2022) but rather contributes to more equitable and accessible chronic disease prevention and management services, programs must continue prioritizing evidence-based strategies that effectively reach people from historically marginalized communities. For example, financial support to provide VAPAs to some participants could eliminate a cost barrier to the technology; VAPA developers could work to recognize specific accents and languages better, and educational materials related to digital literacy could be useful for staff and participants who intend to use this technology. Although incorporating VAPAs may be feasible into chronic disease prevention and management programs, their integration should be approached with a critical assessment of the unique needs and preferences of the specific participant population.
Limitations
This was an exploratory qualitative study with several limitations. The study was conducted with a few programs, so findings may not be generalizable to all National DPP or DSMES programs. We did not collect demographic data from participants (e.g., age, ethnicity), although most participants were recruited from programs that are held in historically marginalized areas. In addition, because we collected data from small groups, participants’ responses may not reflect broader opinions regarding the use of VAPAs.
Implications for Practice
This study’s findings can help inform future efforts to promote VAPAs as a tool to enhance program engagement and support health outcomes by identifying the types of devices and functionality with the greatest potential to be integrated into chronic disease prevention and management programs. Health promotion practitioners should consider the findings in the broader context of rapid advancements of digital technology, including the emergence of large language models (LLMs) such as Chat GPT version 4 (OpenAI, 2023). These technologies have similar features to VAPAs in terms of mobile accessibility and voice interaction, while also introducing other advanced features like image recognition (Haleem et al., 2022). LLMs have already demonstrated applications in chronic disease clinical support, for example, in one study utilized to extract oncologic phenotypes from free-text computed tomography (CT) reports on lung cancer (Fink et al., 2023). The potential integration of LLM features into VAPAs could improve their utility and overall effectiveness in the future.
Implications for Research
Prior research has documented the accuracy, comprehensiveness, and reliability of VAPAs to provide health-related information as variable, depending on the type of device (e.g., smartphone, smart speaker) and software (e.g., Google Assistant, Bixby) used (Chia et al., 2023). Therefore, future research should consider exploring the specific health-related contexts in which VAPAs may be most reliable, accurate, and effective. In addition, given the role of health educators in the chronic disease prevention and management programs in facilitating lifestyle change interventions, future research should investigate which strategies for uptake and implementation of VAPAs may be most effective.
Footnotes
Authors’ Note:
The authors thank staff at CDC and our selected National DPP and DSMES programs for their assistance in recruitment as well as for their participation. This work would not have been possible without their expertise and dedication, and we are deeply thankful for their contributions. This work was supported by funding from the Centers for Disease Control and Prevention, Contract # 200-2013-M-53964B.
Disclaimers
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of Health and Human Services. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.