
Abstract
As the COVID-19 pandemic recedes, SARS-CoV-2 vaccination is crucial for reducing transmission and severity, but vaccine hesitancy remains a challenge. The study explored community actions and initiatives addressing vaccine hesitancy among Somali immigrant communities in cities in the Upper Midwest, USA, and Western Norway, focusing on trust factors and comparing members of the Somali diaspora in two distinct social and cultural contexts. Qualitative collective case studies were conducted, involving 14 semi-structured interviews with key informants from the Upper Midwest and Western Norway knowledgeable about initiatives designed to address SARS-CoV-2 vaccine hesitancy. Data were coded in NVivo 12 and analyzed thematically, guided by the Bergen Model of Collaborative Functioning and the Socioecological Model to identify basic and organizational themes. The findings illustrate critical sociopolitical influences on vaccine hesitancy, like racial tensions following George Floyd’s murder in Minneapolis and mistrust toward the government in Norway. Effective strategies in the Upper Midwest included maintaining long-term community relationships and culturally tailored outreach and communication to reduce hesitancy. Conversely, Western Norway’s less community-centric approach, focusing on translation services without deeper engagement, faced challenges in trust-building. The study highlights the essential role of culturally affirming and community-centric approaches in addressing health challenges in immigrant communities. Trust, fostered through community involvement and understanding sociopolitical contexts, is pivotal in addressing vaccine hesitancy. This research offers insights into designing and implementing effective health promotion strategies tailored to immigrant populations’ unique needs. It emphasizes the necessity of integrating socioecological perspectives and community-specific interventions in health promotion practice and policy.
Keywords
Background
Four years post-COVID-19 onset, with 775 million cases, over 7 million deaths, and 67% of the global population fully vaccinated, reflection on SARS-CoV-2 vaccine distribution and impact is vital to preparing for future pandemics (World Health Organization, 2024). Vaccine hesitancy, a long-standing global health issue, intensified with the SARS-CoV-2 vaccine (Levin & Bradshaw, 2022). Approval, rollout, and mass administration of the vaccine encountered barriers, notably in immigrant communities (Sallam et al., 2022).
Immigrant health faces structural barriers to vaccination access, leading to lower rates and increased vaccine-preventable diseases compared to host populations (Charania et al., 2019). Access challenges and diverse cultural health perspectives exacerbate these issues (Tankwanchi et al., 2021). Somali immigrant communities, in particular, have demonstrated hesitancy toward vaccines like MMR and HPV due to misinformation, cultural beliefs, and mistrust in healthcare systems (Tankwanchi et al., 2021).
Over 836,000 Somali refugees and asylum seekers displaced by civil war are spread worldwide, with large communities notably in Minnesota, USA, and Norway (Sheikh & Healy, 2013; United Nations High Commissioner for Refugees, 2022). Historical vaccine hesitancy, particularly toward the MMR vaccine, led to measles outbreaks in these regions, fueled by targeted disinformation linking the vaccine to autism (Jenness et al., 2021). Importantly, disinformation is false information spread deliberately to deceive, while misinformation is inaccurately spread without malicious intent (Freelon & Wells, 2020).
The introduction of the SARS-CoV-2 vaccine received mixed reactions, offering hope for reducing COVID-19-related morbidity and mortality while also sparking vaccine hesitancy. Acceptance was positively and negatively influenced by factors such as education, governmental trust, and misinformation (Sallam et al., 2022). In Minnesota’s Somali community, cultural concerns, misinformation, and healthcare distrust mirrored past vaccine issues with MMR and HPV (CDC, 2021; Fazal, 2022; Pratt et al., 2019, 2021). Similarly, disparities in vaccination rates have been observed between native populations and Somali immigrants in Norway, highlighting unique barriers such as health literacy and immigration-related concerns, including healthcare navigation and language barriers (Kraft et al., 2022). Both Minnesota and Norway responded with targeted initiatives; the Minneapolis Health Department collaborated with faith-based and community groups (CDC, 2021), while Norway prioritized immigrant-focused health communication to support equitable distribution of information (Le et al., 2021). These efforts underscore the need for tailored, culturally affirming strategies to increase vaccine equity across diverse populations.
In general, prior interventions addressing vaccine hesitancy have proven effective by focusing on under-vaccinated groups, raising awareness, and involving community leaders (Jarrett et al., 2015). Trust in vaccines and healthcare systems also plays a crucial role in vaccine uptake (Larson et al., 2018; Salmon et al., 2015). However, there is a paucity of literature on interventions specifically addressing SARS-CoV-2 vaccine hesitancy in immigrant communities due to the vaccine’s rapid development and distribution.
The existing literature on COVID-19 vaccine hesitancy is primarily comprised of quantitative surveys, with fewer studies offering qualitative insights into interventions (Callaghan et al., 2021; Levin & Bradshaw, 2022). Although some qualitative work exists (Czapka et al., 2023), research specifically exploring trust and hesitancy within Somali communities remains limited (Jarrett et al., 2015; Salmon et al., 2015). This paper addresses these gaps by examining community efforts to counter SARS-CoV-2 vaccine hesitancy among Somali immigrants in a city in Minnesota in the Upper Midwest, USA (UMW-USA) and a city in Western Norway (W-NO). By considering diverse social and political contexts, the study aimed to highlight tailored intervention strategies rather than a universal approach. The study investigated factors influencing Somali immigrants’ trust in healthcare systems and vaccines and aims to understand differences in the approaches implemented in UMW-USA and W-NO to build trust and encourage vaccine uptake. This research contributes insights for future interventions addressing vaccine hesitancy, emphasizing tailored strategies for marginalized groups with distinct cultural and communication needs.
Method
The Norwegian Center for Research Data (NSD) approved personal data collection, use, and storage for this study. IRB review was sought in Minnesota but deemed unnecessary due to NSD’s prior authorization.
Theoretical Framework
The Bergen Model of Collaborative Functioning (BMCF), as seen in Figure 1, offers a structured framework for analyzing collaboration by examining inputs (partner skills, mission, and financial resources), throughputs (communication, leadership, and tasks), and outputs, which range from additive to synergistic or antagonistic outcomes. This model helps identify pathways that influence community engagement and health promotion efforts (Corbin et al., 2013, 2016). In this study, the BMCF was used to understand how collaboration dynamics shaped COVID-19 vaccination efforts, especially in marginalized communities, while highlighting the importance of effective partnerships in overcoming barriers.
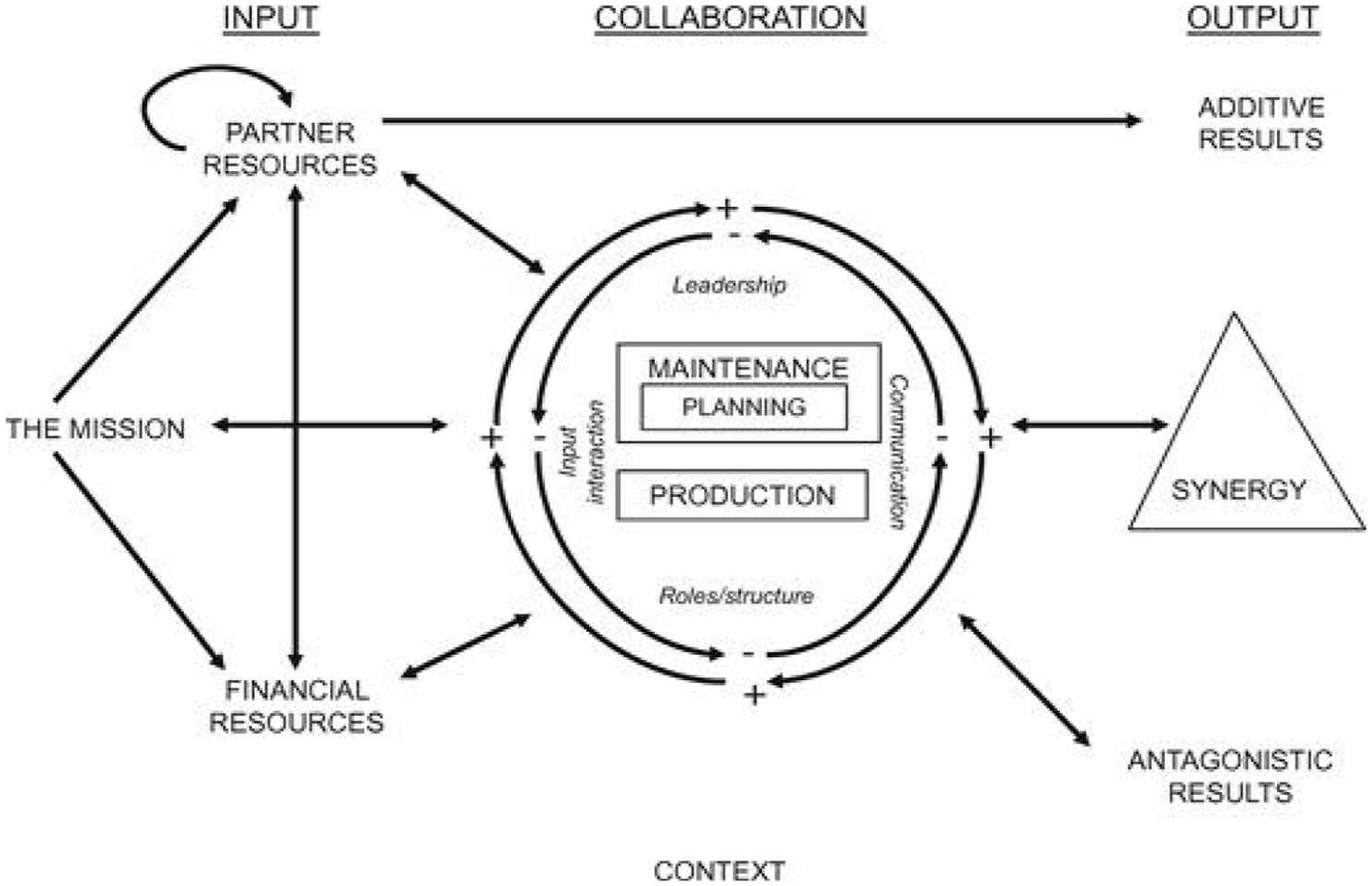
Bergen Model of Collaborative Functioning (Corbin et al., 2016)
However, it became clear during data collection and analysis that broader contextual factors—such as individual, community, and policy-level influences—were also essential to understanding collaboration outcomes. To capture these layers, the Socioecological Model (SEM) was incorporated to explore how different levels (individual, interpersonal, community, organizational, and policy) influenced health behaviors and collaboration efforts (Bronfenbrenner, 1979). This dual-framework approach allowed for a comprehensive understanding of both the collaborative processes and the external factors that shaped them.
Participants
This study focused on Somali immigrant populations in cities in UMW-USA and W-NO. Key informants engaged in community initiatives addressing SARS-CoV-2 vaccine hesitancy were selected based on their (1) active engagement with the Somali community in UMW-USA or W-NO, (2) knowledge of local vaccination efforts, and (3) willingness to be interviewed in either English or Norwegian. Recruitment utilized gatekeepers in cultural and community centers, universities, and health institutions. In UMW-USA, prior collaboration with a local university department facilitated access to informants, while in W-NO, connections were established through the Norwegian Institute of Public Health, a local university’s Pandemic Center, and a regional mosque. Snowball sampling continued until no new themes or insights emerged, indicating saturation had been reached.
This study included 14 key informants: eight from UMW-USA and six from W-NO. UMW-USA participants included a mix of Somali community members and individuals from diverse backgrounds involved in health-related initiatives. In contrast, the W-NO sample consisted of predominantly Somali community members. The demographic characteristics, roles, and relevant backgrounds of these participants are detailed in Table 1.
Demographic and Professional Profiles of Study Participants
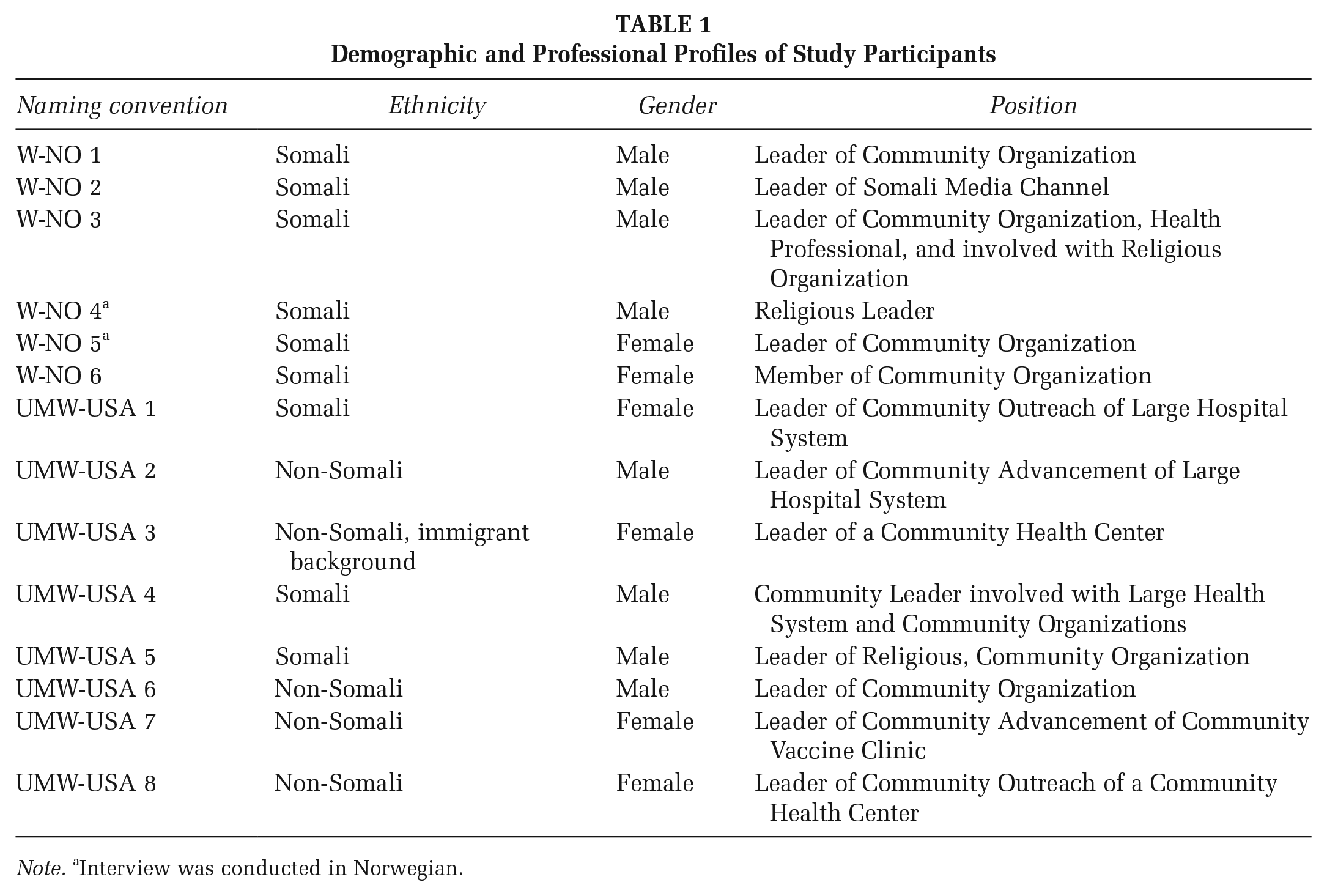
Note. aInterview was conducted in Norwegian.
Data Collection
A semi-structured interview guide was developed based on the BMCF to examine collaboration through inputs, throughputs, output, and contextual factors. Questions such as “Can you tell me about any organizations [insert organization] has collaborated with?” and “Do you feel there are enough financial resources to do what is needed?” explored inputs, while questions like “Can you tell me about any challenges related to these initiatives?” examined throughputs. Outputs were assessed through questions like “What do you think has been helpful related to COVID vaccination in this community?” This guide ensured a comprehensive exploration of collaboration dynamics in addressing vaccine hesitancy, using the BMCF framework to understand key elements shaping community engagement. The questions covered in the interview guide can be viewed online as supplementary materials.
Procedures
The study conducted semi-structured interviews between January and March 2023, to gather in-depth insights from the participants. The interviews were held in-person or remotely via video conferencing, adapting to post-pandemic conditions. Each interview lasted from 20 to 40 minutes and allowed flexibility for participant narratives. Written, informed consent was obtained, and the interviews were conducted in English or Norwegian based on participant preference. Redacting identifiers anonymized the recordings, and participants were assigned unique IDs known only to CP. A colleague reviewed anonymized Norwegian transcripts for linguistic accuracy and contextual understanding.
Data Analysis
Thematic analysis, guided by Braun and Clark’s (2006) method, was used to identify key themes within the qualitative data. The analysis was initially guided by the BMCF to explore the dynamics of collaboration, including inputs, throughputs, and outputs (Corbin et al., 2013). However, as the data revealed significant contextual influences on collaboration—particularly cultural, social, and policy-level factors—the SEM was integrated into the analysis to further explore these broader layers (Bronfenbrenner, 1979).
This two-step process involved analyzing the UMW-USA and W-NO datasets individually to capture context-specific insights, followed by a comparison to identify overarching themes across both datasets. The analysis remained flexible to allow inductive themes to surface while using the BMCF and SEM deductively to structure the findings. Interviews conducted in Norwegian were transcribed and coded in their original language, then translated into English following Esfehani and Walters’ (2018) process to capture the participants’ nuanced perspectives accurately. CP and JHC collaboratively coded and discussed the data to ensure a well-rounded analysis. Triangulation ensured credibility by comparing multiple sources, including key informants, coding perspectives, and probing questions. Dependability was ensured through systematic thematic analysis and accurate transcription. The final report underwent review by FGO and RP.
Positionality
The primary investigator, a young White woman from Minnesota, previously an immigrant in Norway and married to a Muslim man from Morocco, considered her positionality throughout the research process. She used reflexivity strategies and adhered to cultural customs to mitigate biases, level power dynamics, and demonstrate respect for participants’ identities, while also acknowledging her role as an outsider studying the Somali community. She aimed for accuracy and sensitivity in representing participant identities and research findings, striving to minimize personal identity influence on data collection. In addition, the broader research team, with members from diverse nationalities and sociopolitical contexts, further enriched the research by bringing varied perspectives, ensuring findings were represented accurately and sensitively while minimizing personal identity influence on data collection and analysis.
Results
This section presents findings from 14 interviews, structured around three overarching themes and nine sub-sections guided by the BMCF. It explores the varied experiences of Somali communities in different geographic locations, highlighting both similarities and differences between these populations.
Contextual Influences on Vaccine Hesitancy
Sociopolitical Context and Cultural Clashes
The study exposed the sociopolitical context’s profound impact on vaccine hesitancy in UMW-USA and W-NO’s Somali communities, as detailed in Table 2. In UMW-USA, the racial tensions post-George Floyd’s murder and the COVID-19 pandemic intertwined to heighten mistrust, particularly toward healthcare systems perceived as culturally insensitive. Participants noted how the significant clash between healthcare systems’ individualistic approach and Somali communities’ communal decision-making, deepened mistrust as families felt excluded from critical health decisions.
Impact of Contextual Factors on Vaccine Hesitancy
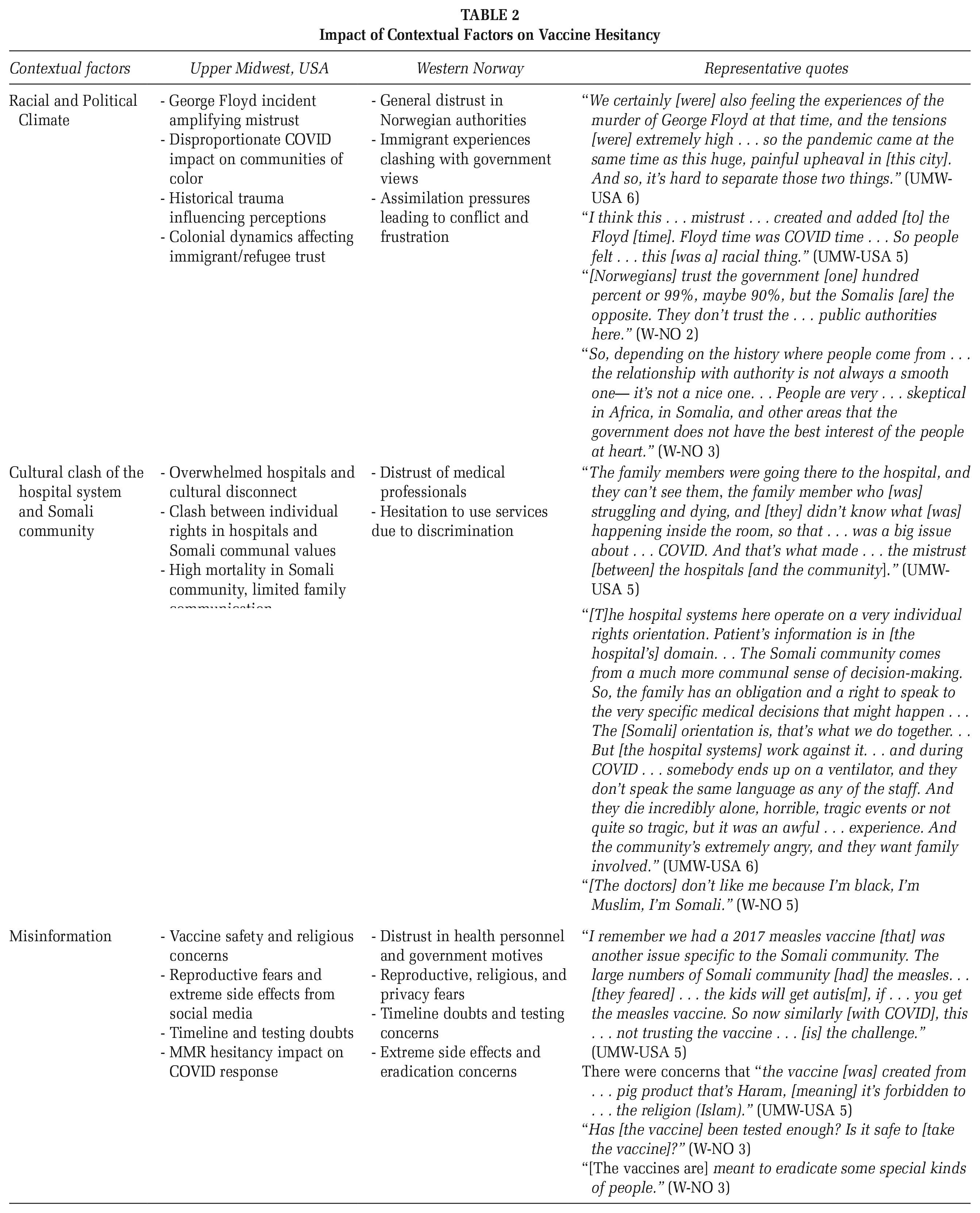
In W-NO, distrust stemmed mainly from pervasive skepticism toward public authorities and governmental decisions, intensified by a racial and political climate that alienated Somali immigrants. Past experiences and cultural backgrounds compounded this distrust, leading to hesitancy toward public health initiatives. Pressures to assimilate worsened conflicts and frustration. This was highlighted by the Somali community’s marked reluctance to engage with medical services, fearing discrimination and misunderstanding. These complex dynamics highlight the challenge of bridging the gap between healthcare systems and the Somali community’s unique needs and perspectives.
Misinformation and Its Impact
Misinformation was crucial in shaping vaccine hesitancy in UMW-USA and W-NO, as illustrated in Table 2. Concerns about the vaccine’s safety, religious compatibility, and side effects were widespread, fueled by rapid vaccine development and rumors. In UMW-USA, this was further complicated by historical trauma related to medical mistreatment, particularly in communities of color. In W-NO, misinformation was exacerbated by a lack of trust in the motives of healthcare providers and government authorities, fueling conspiracy theories and skepticism.
Strategic Approaches to Vaccine Hesitancy
Inputs: Trust-Building and Community Engagement
As seen in Table 3, UMW-USA city’s approach was characterized by its focus on building trust through extensive community engagement and responsiveness. Efforts centered on understanding and addressing the specific needs and concerns of the Somali community, involving community leaders in decision-making to foster ownership and relevance among community members. Conversely, W-NO’s strategy revolved around translating and disseminating government-provided information, with less emphasis on community dialogue and more on information access. While informative, this approach lacked the personal touch and trust-building elements of UMW-USA’s strategy.
Strategic Approaches in the Upper Midwest, USA and Western Norway
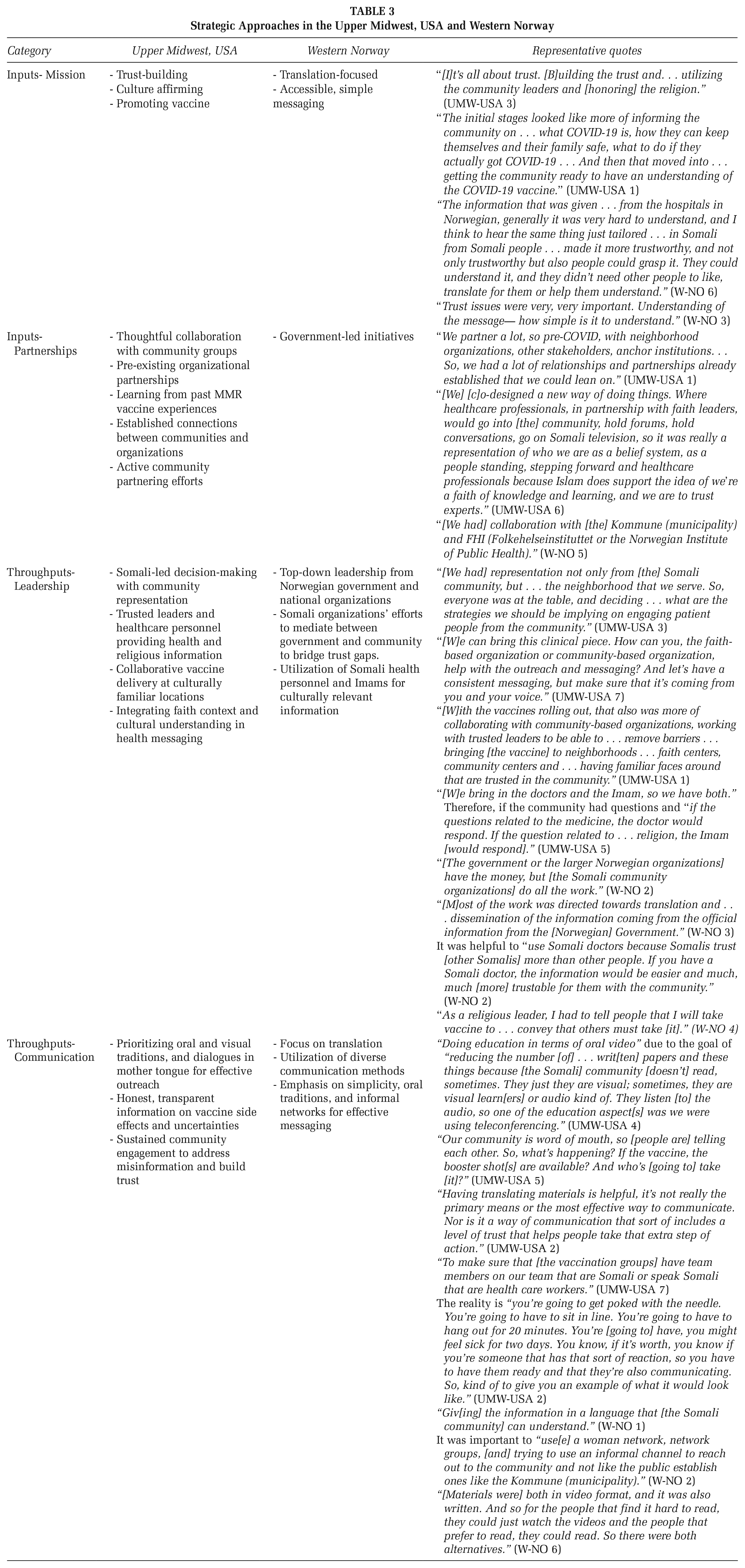
Throughputs: Leadership and Communication Styles
In the UMW-USA, the leadership model was heavily community-based, with a significant role for Somali leaders in shaping the vaccination campaign, highlighted in Table 3. This approach ensured respect for cultural and religious nuances, enhancing effectiveness. Communication methods, such as WhatsApp and live video events, were tailored to community preferences for broader reach. Conversely, the city in W-NO’s approach was more top-down, led by government authorities and large Norwegian organizations. Communication primarily involved translating existing materials rather than crafting culturally specific messages.
Outcomes of Vaccine Hesitancy Initiatives
Antagony and Synergy in Cities in the UMW-USA and Western Norway
In UMW-USA, existing mistrust, worsened by racial tensions and cultural clashes within healthcare, was alleviated through pre-existing, sustained community relationships. These relationships, built before the pandemic during the 2017 measles outbreak, fostered synergy and facilitated vaccine acceptance initiatives. Engaging trusted community leaders and organizations, who had established credibility through past collaborations, proved crucial in overcoming barriers and increasing vaccine uptake, as detailed in Table 4.
Outcomes of Vaccine Hesitancy Initiatives
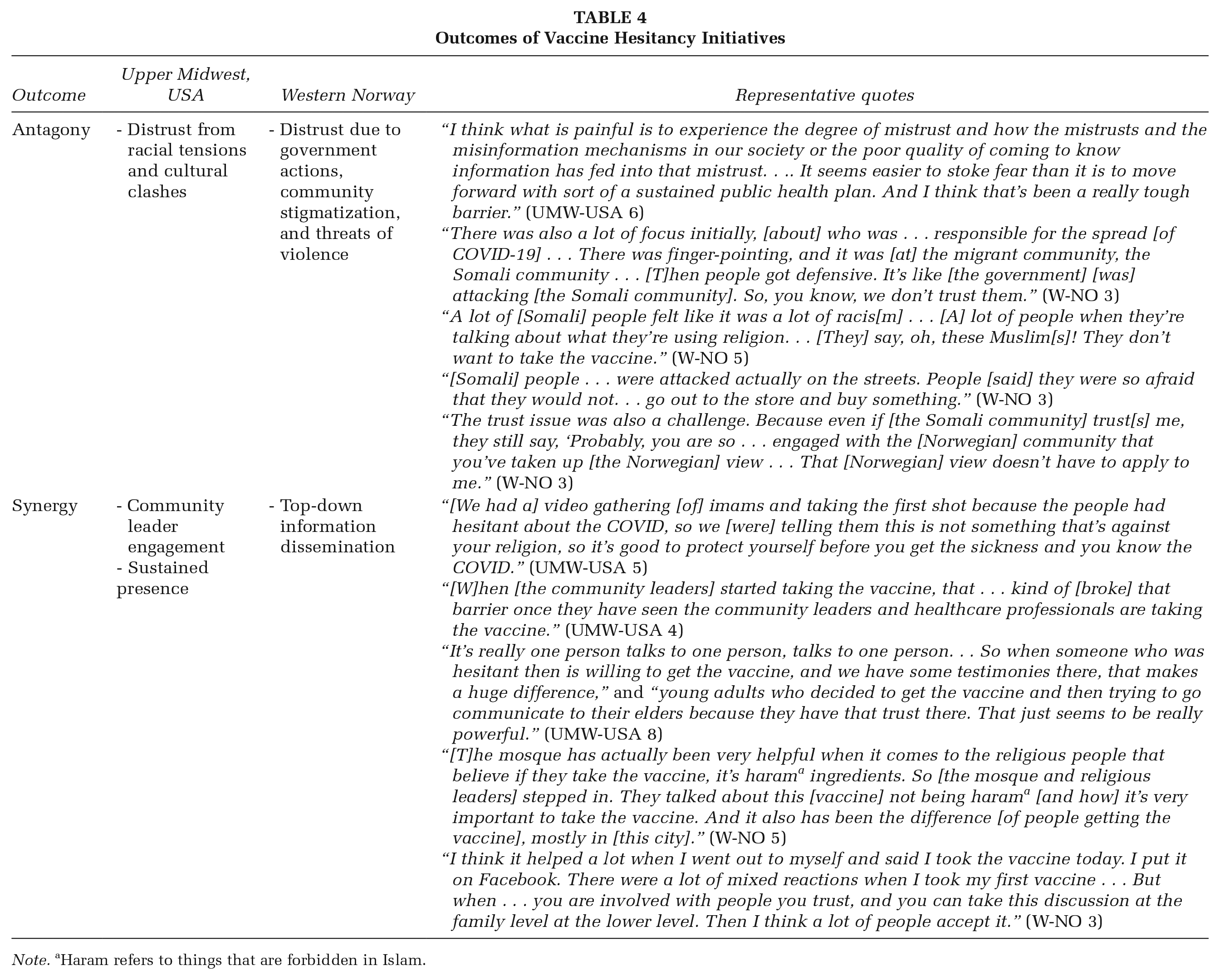
Note. aHaram refers to things that are forbidden in Islam.
In contrast, synergy in W-NO was limited due to a top-down approach emphasizing translation over deeper community engagement and trust-building. The government’s actions inadvertently led to stigmatization and worsened mistrust, hindering progress. This lack of engagement, which prompted a defensive stance from the Somali community, underscored the challenges of addressing vaccine hesitancy without foundational trust built through direct community involvement.
Discussion
Using the BMCF and SEM to examine vaccine hesitancy in Somali immigrant communities in UMW-USA and W-NO reveals the complexities of public health interventions. The study highlights the importance of contextual understanding, trust, and collaboration in tackling health challenges, especially in immigrant communities.
Trust and Collaboration in Vaccine Hesitancy Initiatives
Trust was crucial in overcoming vaccine hesitancy. In the UMW-USA city, successful initiatives were largely due to established trust through community engagement. By leveraging existing relationships and addressing specific community needs, effective vaccine uptake was achieved (O’Mara-Eves et al., 2015; Quinn & Andrasik, 2021). These UMW-USA community-based, Somali-led, and healthcare organizations utilized Somali oral traditions, health personnel, and religious leaders in effective strategies previously proven to address MMR vaccination challenges (Stinchfield, 2021) SARS-CoV-2 efforts built on the trust and relationships established during the UMW-USA city’s MMR campaigns, aligning with literature emphasizing the importance of community engagement in marginalized groups (O’Mara-Eves et al., 2015; Quinn & Andrasik, 2021).
The findings from UMW-USA indicate that health system changes can create synergy by partnering with community organizations and incorporating their feedback. The literature emphasizes the importance of listening to community suggestions to build trust between marginalized populations and institutions (Bagasra et al., 2021). Continued investment in these relationships is vital for emergencies like the COVID-19 pandemic (Corbin et al., 2021). However, the question remains of how to preserve this knowledge, especially considering the high turnover of public health professionals during the pandemic (Leider et al., 2023).
Despite good intentions, W-NO’s top-down approach of translating government messages into Somali revealed shortcomings in building trust and meaningful engagement. It failed to account for literacy differences or include trusted community figures, creating communication gaps. W-NO’s experience emphasizes the need for reciprocal collaboration and empowerment in public health. Trust and understanding thrive with community-centric strategies that engage communities as active partners and affirm their culture (Quinn & Andrasik, 2021). These methods ensure that interventions deeply resonate, shifting from passive dissemination to active, participatory engagement (Quinn & Andrasik, 2021).
The literature supports the need for multidimensional communication strategies that consider cultural backgrounds, language proficiency, and literacy levels while involving community members to promote inclusivity and empowerment (Demeke et al., 2022; Finset et al., 2020). Community-engaged leadership, proven effective in UMW-USA, emphasizes the value of involving community members in decision-making to align interventions with community needs and cultural practices (O’Mara-Eves et al., 2015; Quinn & Andrasik, 2021).
Furthermore, partner resources are traditionally seen as assets (Corbin et al., 2013). However, challenges in W-NO reveal that partners can also bring negative traits like bias, assumptions, and arrogance, which can affect collaboration. Recognizing both positive and negative aspects of partner resources offers a more nuanced understanding of collaborative dynamics, especially in multicultural settings. Adopting a more inclusive, participatory approach in health communication and intervention models is essential for tackling public health issues like vaccine hesitancy.
Contextual and Cultural Considerations in Vaccine Hesitancy
Exploring actions and initiatives related to vaccine hesitancy in Somali communities in cities in UMW-USA and W-NO revealed significant contextual and cultural considerations. UMW-USA approach, shaped by the convergence of the COVID-19 pandemic and heightened racial tensions after George Floyd’s murder, highlighted how historical trauma and perceived insensitivity in healthcare can deepen distrust. This period exposed a clash between Western healthcare’s individualism and the Somali community’s communal decision-making, emphasizing the need for culturally affirming interventions. UMW-USA strategies transcended simple message translation by employing culturally tailored communication, embracing Somali oral traditions, and harnessing the credibility of community and religious leaders alongside Somali health personnel. These methods cultivated ownership, relevance, and trust in the community, illustrating the importance of community participation and feedback in creating effective interventions (O’Mara-Eves et al., 2015; Quinn & Andrasik, 2021). UMW-USA’s success underscores the critical role of understanding sociopolitical and cultural contexts, demonstrating that addressing vaccine hesitancy requires more than information dissemination—it demands collaborative, empowering, and trust-building efforts that resonate with the community’s values and experiences.
In contrast, W-NO’s experience highlighted a general distrust of public authorities and governmental decisions. This skepticism, rooted in the Somali community’s historical experiences with authority, was exacerbated by the global backdrop of the COVID-19 pandemic, where fear, racism, xenophobia, and even acts of violence often intensified the stigmatization of immigrant communities (Diaz et al., 2021; Teixeira da Silva, 2020). The reliance on translation, without addressing the community’s cultural, linguistic, and literacy nuances, failed to foster engagement or trust and further impeded efforts to address vaccine hesitancy effectively. Relying on translation only can create power dynamics that marginalize certain groups, highlighting the need for more inclusive communication methods (Demeke et al., 2022). Further, the literature shows that incorporating the community’s perspectives and values is more effective than solely focusing on translation to promote health behavior change among immigrant communities (Finset et al., 2020). These findings underscore the critical need for nuanced, culturally affirming engagement strategies that prioritize genuine understanding and inclusion over mere translation to address public health challenges within immigrant communities.
Misinformation significantly influenced vaccine hesitancy across both cities in UMW-USA and W-NO, with concerns spanning vaccine safety, religious beliefs, and conspiracy theories circulating on social media. In W-NO, skepticism toward healthcare initiatives and government directives revealed deeper mistrust. Yet, in both contexts, religious leaders emerged as pivotal figures in bridging the divide by dispelling myths and aligning vaccination efforts with Islamic teachings prioritizing life preservation and preventive health measures. The engagement of religious leaders illustrates how faith-based approaches, validated by literature, effectively counter misinformation and integrate cultural and spiritual values into public health strategies (Alsuwaidi et al., 2023). This approach highlights the need for culturally aware and community-supported health interventions that leverage assets like religious influence to address vaccine hesitancy and effectively navigate public health complexities.
Challenges and Efforts in Rebuilding Trust
Efforts to rebuild trust in UMW-USA underscored the critical role of cultural affirming practices and acknowledging the historical trauma that influences community perceptions of healthcare systems. Historical trauma also shapes trust concerns within minority communities, manifesting as reluctance to engage with healthcare providers or skepticism about public health initiatives due to deep-seated distrust of institutions perpetuating colonial power dynamics (Bagasra et al., 2021). UMW-USA’s success in overcoming hesitancy through culturally and religiously attuned engagement, drawing on past collaborations, and recognizing historical and community leadership values, underscores the importance of a nuanced, community-integrated public health approach that fosters genuine partnership. UMW-USA’s success showcases the effectiveness of culturally congruent strategies, highlighting how deep trust and cooperation between healthcare providers and communities address specific concerns and needs, as supported by literature (Diaz et al., 2021). Establishing and maintaining relationships with the Somali community is crucial in rebuilding the trust lost during the pandemic. In contrast, the less collaborative approach in W-NO resulted in a trust deficit, underscoring the importance of incorporating community voices and respecting sociocultural nuances.
Limitations
The study encountered limitations in its recruitment strategy, particularly in UMW-USA, where a single gatekeeper was relied upon. This reliance could limit the diversity of viewpoints captured, though the gatekeeper’s strong trust within the community likely enriched data quality by encouraging honest and open participation. In W-NO, the sample was only from the Somali community, lacking broader perspectives from health professionals or other groups. Efforts were made to address these issues by seeking diverse viewpoints within available networks. The interviewer (CP), an outsider, may have influenced responses, given her background and positionality. To mitigate potential bias, reflexivity strategies and adherence to cultural customs were employed, promoting openness and minimizing power dynamics. Despite these efforts, the exclusive focus on Somali immigrant communities limits the applicability of findings to other groups, calling for careful interpretation of the results. Further, we did not account for the duration of each key informant’s involvement in their initiatives to address vaccine hesitancy, which may have influenced their perspectives as community attitudes evolved over the course of the pandemic. Future research should broaden its approach to include more diverse perspectives, ensuring a deeper understanding of health challenges across different populations.
Implications for Practice
This research underscores the complex interplay of sociopolitical events, cultural nuances, and the critical role of context in shaping health interventions for immigrant communities. For practitioners, the findings emphasize the necessity of deep community engagement that extends beyond mere participation to active collaboration and co-creation of health initiatives. Engaging with communities through trusted leaders, acknowledging historical traumas, and addressing systemic inequalities are pivotal for building trust. Specifically, the use of culturally tailored communication strategies that resonate with community values and traditions, as evidenced in UMW-USA’s successful interventions, illustrates the effectiveness of such approaches.
In addressing vaccine hesitancy, this study advocates for the use of a Social Ecological Model (SEM) to frame health behaviors within broader systemic contexts, rather than focusing solely on individual factors. Vaccine hesitancy, often framed in stigmatizing individualistic terms, should be understood through multiple layers, including interpersonal, community, organizational, and policy influences. Shifting to this socioecological perspective helps to avoid victim-blaming and recognizes the social determinants that influence health behaviors in immigrant communities. Policymakers should empower communities, promote culturally affirming healthcare, and ensure equitable access to health information and services. Supporting community organizations in developing tailored health promotion strategies and dismantling barriers rooted in historical and systemic disparities is critical for creating an inclusive healthcare system.
Future research should explore the long-term impact of community engagement and trust-building on health outcomes and vaccine hesitancy, along with the influence of sociopolitical factors on health policy. While the BMCF was effective in illustrating partnership dynamics, incorporating a socioecological perspective into future public health strategies may promote health equity and social justice. Refining the BMCF to better account for contextual and systemic factors can enhance its effectiveness in diverse health settings, ensuring that health interventions are both collaborative and responsive to community needs.
Conclusion
The research provides a nuanced understanding of the factors influencing vaccine hesitancy in Somali immigrant communities in cities in UMW-USA and W-NO. The findings highlight the importance of trust, context sensitivity, and socioecological considerations in public health interventions. Community-centered, culturally affirming approaches emerge as crucial for effectively addressing vaccine hesitancy.
This study enriches the ongoing dialogue on crafting public health strategies tailored to immigrant populations, shedding light on the complex interactions between cultural identity, social determinants, and health behaviors. By focusing on the dynamic interplay of these elements, the research underscores the essential steps toward fostering equitable health outcomes and advancing the understanding of health promotion practice in multicultural contexts.
Supplemental Material
sj-docx-1-hpp-10.1177_15248399241308547 – Supplemental material for Critical Insights Into Public Health Interventions: Partnership, Cultural and Racial Tensions, and Vaccine Hesitancy Within Somali Communities in the Upper Midwest, USA, and Western Norway
Supplemental material, sj-docx-1-hpp-10.1177_15248399241308547 for Critical Insights Into Public Health Interventions: Partnership, Cultural and Racial Tensions, and Vaccine Hesitancy Within Somali Communities in the Upper Midwest, USA, and Western Norway by Claire A. Pernat, Rebekah Pratt, Fungisai Gwanzura Ottemöller and J. Hope Corbin in Health Promotion Practice
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.