
Abstract
University Cooperative Extension, which may be the original rural Implementation Science model, holds great promise for translating research into practice and addressing rural health disparities. As this model not only requires successful collaboration between academic researchers and Extension Educators but also possible implementation adaptation to the context of Cooperative Extension and the environments in which they work, implementation research is critical to effective translation into practice and impact. This study was informed by the RE-AIM (Reach, Effectiveness, Adoption, Implementation, and Maintenance) framework describes Cooperative Extension Educators’ implementation of the virtual Happy Healthy Homes interventions, a nutrition intervention and a children’s environmental health intervention, for rural Family Child Care Home providers. Educators provided feedback on curricula, were trained and conducted the two virtual interventions with providers. Implementation of intervention activities and dose were recorded using REDCap. Virtual, structured interviews were conducted to assess Educators’ intervention adoption, implementation, and maintenance. Transcribed interviews were analyzed for themes by two investigators and confirmed by a third. Results indicated that the majority the intervention curricula and activities were delivered as planned. Adoption themes included topical relevance to the community; toolkit provision and financial resource need; and need for additional marketing materials. Implementation themes included Educator’s content expertise; learning environment distractions; and virtual delivery. Maintenance themes included transferability of content to multiple audiences; mission alignment; and Educator awareness. Overall, the implementation partnership with Extension Educators was successful. Virtual implementation was novel for Educators but considered to be positive and an opportunity for expanding future reach.
Approximately 20% and 32% of the American and Oklahoman population live in rural areas, respectively (United Health Foundation [UHF], 2025). Rural health disparities are well-documented (Miller & Vasan, 2021; Oklahoma State Department of Health [OSDH], 2023; Thomas et al., 2014). Disparities extend to health care access (National Institute of Health [NIH], 2022), child care access (National Advisory Committee on Rural Health and Human Services [NACRHHS], 2023), and opportunities for adult learning and professional development (Spivey, 2016; United States Census Bureau [USCB], 2022). Efforts to address these health disparities and advance rural Americans’ health, require effective dissemination and implementation research to advance the translation of research into and practice (Brownson et al., 2012). The Cooperative Extension system, a nationwide network supported by land-grant universities that provides constituents, often in rural areas, with research-based programming and education (Association of Public & Land-Grant Universities; United States Department of Agriculture [USDA], n.d.). As such, Cooperative Extension may be the original Implementation Science model with a century of health education outreach to rural communities delivered by Family and Consumer Science (FCS) Extension Educators (herein referred to as Educators; Franz & Townson, 2008). Researchers recognize the efficacy and efficiency of working with Extension to improve rural health and health education opportunities using Implementation Science (Buys & Rennekamp, 2020). However, implementation research seeking to understand delivery and partnership processes between Extension and external university partners has been limited.
Prior studies of collaborations between Cooperative Extension, academia, and public/private sectors suggest several key factors that facilitate success. These include goal alignment, relevant Educator background, marketability, and flexibility in planning and problem-solving (Carnes et al., 2019; Dev et al., 2022; Nitzke et al., 2004; Wilson et al., 2024). Implementation frameworks, such as the Reach, Effectiveness, Adoption, Implementation, Maintenance (RE-AIM) framework (Glasgow et al., 1999, 2019), provide structure to evaluate intervention implementation. Their application can be useful for identifying opportunities to enhance Educator and participant experiences and improve future implementation in Cooperative Extension model (Dev et al., 2022; Glasgow et al., 1999, 2019; Wilson et al., 2024).
Family Child Care Homes (FCCH) are small child care programs operated out of a provider’s home (Oklahoma Department of Human Services [OKDHS], 2018). FCCH and less formal ECE contexts may be associated with higher rates of childhood obesity (Swyden et al., 2017). There are more than 200,000 FCCH in the United States, many serving rural communities. FCCH, especially in rural areas, experience unique access barriers to participation in professional development and training (Sisson et al., 2021). Enhancing the environment which young children spend substantial time can have health benefits (Barnes & TFCO, 2010; Jurewicz et al., 2006). Specifically, those FCCH with higher-quality nutrition environments were associated with healthier children’s dietary intake (Benjamin-Neelon et al., 2018). Efforts to retain the critical rural child care work force by offering professional development, social support, and promoting health (Bergevin, 2018) and enhance quality FCCH environment for young children in their care are important steps to improving rural health and child care quality. Happy Healthy Homes (HHH) was a community, randomized control trial (RCT) to enhance quality of FCCH in two areas: (a) improving quality of foods served and nutrition practices (NUT) and (b) increasing knowledge and practices that promote environmental health and quality (ECO; Sisson et al., 2019). The current mixed-methods study, informed by RE-AIM, describes the implementation of the previously described HHH intervention (Sisson et al., 2019) by Educators into rural communities and the Educators’ experience with adoption, implementation, and maintenance (Sisson et al., 2019).
Method
Intervention
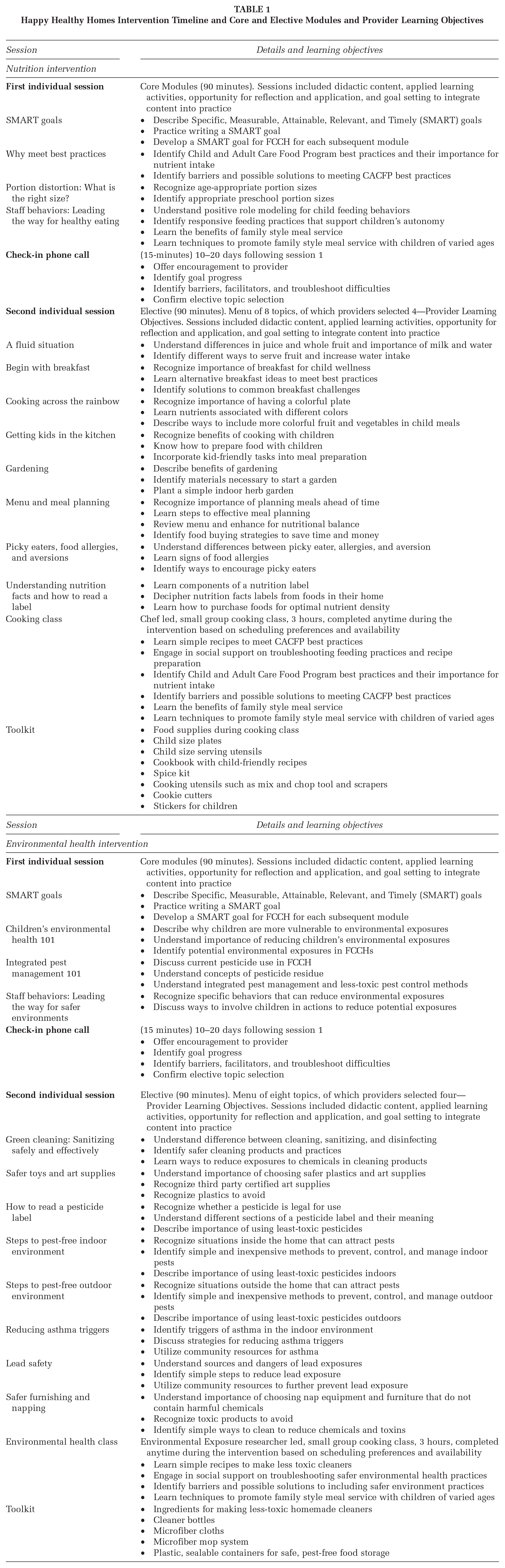
HHH rationale and procedures (Sisson et al., 2019) are briefly summarized herein and in Table 1. HHH was based on Social Ecological Model (Sallis et al., 2008), Social Cognitive Theory (Bandura, 1986), Social Support (Heaney & Israel, 2002), Self-Determination Theory (Ryan & Deci, 2000), and Adult learning Principles (Committee on Developments in the Science of Learning, Committee on Learning Research and Educational Practice, & National Research Council., 2000). Goals of the NUT arm were to enhance the quality of foods provided and the provider’s nutrition-related behaviors (Sisson et al., 2019). Goals of the ECO arm were to increase providers environmental health literacy and use of less toxic cleaners and pest management practices (Sisson et al., 2019). The intervention included six contact hours via Zoom including two 90-minute individual, interactive education sessions with their assigned Educator and a 3-hour small group class. Each module concluded with goal setting. Toolkits valued at $250 were provided to promote behavioral goals (Table 1). All providers received a 15- to 20-minute check-in phone call a couple weeks following the first individual session to provide encouragement, troubleshooting, and progress toward goal attainment. The second individual session included eight modules of which FCCH selected four with content to reinforce desired behavior changes.
Happy Healthy Homes Intervention Timeline and Core and Elective Modules and Provider Learning Objectives
Process of Integrating Intervention With Extension
Educators in six Oklahoma counties were invited to participate in the HHH project and 100% agreed in spring 2018. The Educators were all women and 7 to 28 years of experience. Ten percent of each Educator’s salary was provided. In spring through fall 2018, Educators were invited to offer comments, suggestions, and modifications to the curricula. In response, minor modifications for literacy were made. Educators attended a 2-day implementation training in fall 2019.
Recruitment and enrollment for HHH, originally planned to take place in-person, began in January 2020 to all FCCH providers in the six targeted counties. While several providers were enrolled and started in-person delivery with Educators, as a result of the COVID-19 pandemic, in March 2020, Educators and researchers modified HHH for virtual delivery and opened recruitment statewide focusing in rural areas. Those providers who started with in-person delivery and shifted to virtual delivery were excluded from the research, but were allowed to complete content, receive toolkits, and CEC. Figure 1 shows HHH FCCH statewide, virtual recruitment and enrollment. Three Educators opted to teach the NUT curriculum, and three Educators opted to teach the ECO curriculum. FCCH providers were randomly assigned to one of the groups then randomly assigned to an Educator. Toolkit supplies were shipped, and gift cards were provided for perishable supplies (e.g., groceries needed for the cooking class) so that providers could purchase them. Additional meetings were held with Educators to provide revised implementation plans and procedures.
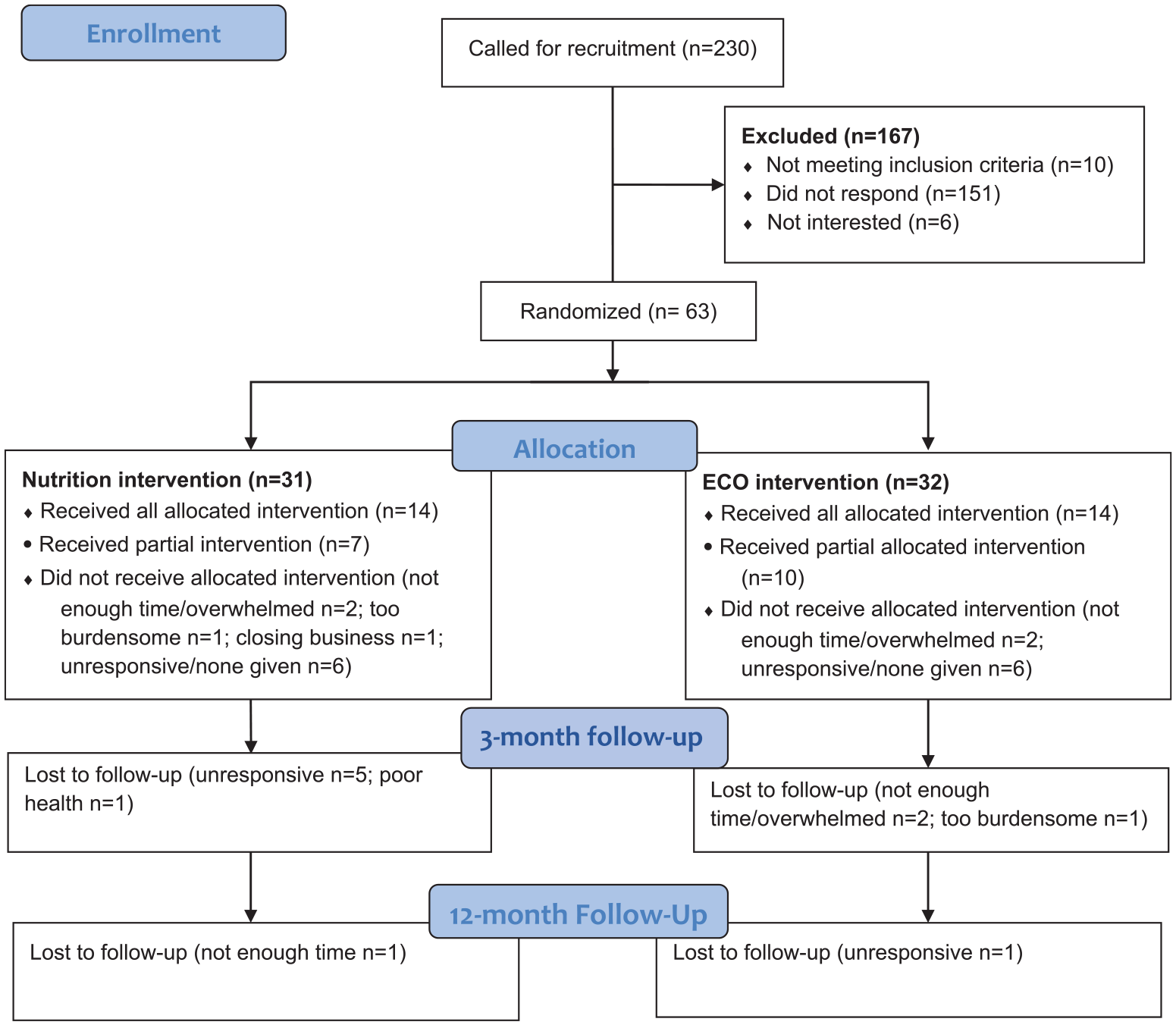
CONSORT 2010 Flow Diagram HHH Virtual Implementation
Process Evaluation
The RE-AIM (Borrelli et al., 2005; Glasgow et al., 1999, 2001, 2019) Framework, specifically “implementation” guided the process evaluation. Educators recorded their delivery experiences within 2 to 3 days after the session. Items consisted of “activity completion (yes/no)” (i.e., dose delivered for each planned activity for all three sessions), “total dose delivered” (average percent of all planned activities that were delivered), completion of the session, and duration of each session. Educators reported their perception of provider interest for each of the three sessions. Interest was not reported for specific topics. Data were entered into REDCap and analyzed using Excel.
FCS Extension Educators Experiences
In fall 2021, a qualitative investigation was conducted virtually, via audio-recorded Zoom sessions (Version 5.12.2) using structured one-on-one interviews with all Educators (N = 6) who implemented HHH. The primary interviewer was a senior faculty (DH) member with experience in qualitative methods and with 18 years’ experience as an Extension Specialist and Implementation Science. The secondary interviewer, or note-taker, was a second-year graduate student trained in qualitative methods (BR). Interviews were recorded for automated transcription within Zoom. The protocol was reviewed and approved by the Oklahoma State University Institutional Review Board. Educators provide consent prior to interviews.
Interview Guide
Structured questions were developed using the RE-AIM framework and focused on the constructs of adoption (three questions), implementation (five questions), and maintenance (three questions; Glasgow et al., 1999, 2019). Reach and effectiveness are being disseminated elsewhere. Educators were also asked about their experiences working with academic researchers.
Interview Data Analysis
Two researchers (BR and DH) independently read the transcripts and compared the field notes. Thematic analysis was used to group the phrases into themes (Kiger & Varpio, 2020). The two researchers met to compare the independent analyses and resolve discrepancies and subsequently met with a third researcher (SS) to review and discuss themes and supporting data. Following thematic analysis, member checking was conducted with one Educator who confirmed the identified themes.
Results
Process Evaluation
A process evaluation was conducted to document the degree to which the intervention activities were delivered as intended. Table 2 details participation across all intervention activities. The sample size decreased throughout the study as participants withdrew for a variety of reasons (Figure 1). Even with withdraw, most providers who remained in the project completed most intervention activities and with a high degree of interest and participation, as determined by the educator (Table 2). The virtual, individual sessions lasted 93.6 minutes and 85.8 minutes, respectively, with the check-in phone call lasting 10.3 minutes. Check-in phone calls did experience some interruptions. However, any omitted activities were completed in visit 2. The average class duration was 161.3 minutes and out of the nine virtual small group classes conducted, educators perceived providers interest in the topics.
Happy Healthy Homes Virtual Family Child Care Home Intervention Activities, Completion Rates, and Implementation
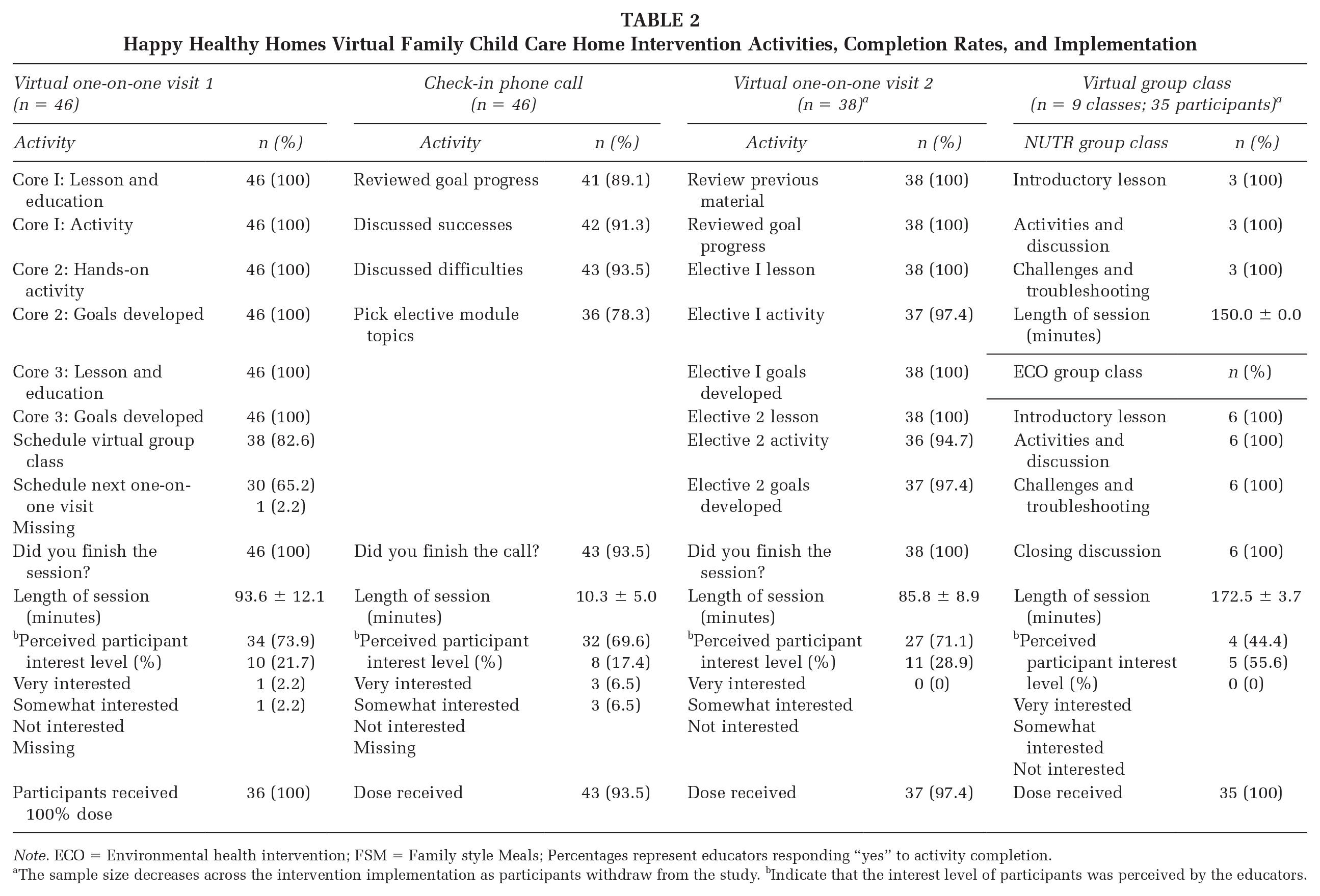
Note. ECO = Environmental health intervention; FSM = Family style Meals; Percentages represent educators responding “yes” to activity completion.
The sample size decreases across the intervention implementation as participants withdraw from the study. bIndicate that the interest level of participants was perceived by the educators.
Educators reported some challenges to the delivery of individual sessions including technology-related issues and presence of children being a source of distraction (Table 3). For the small group classes, reported challenges included technology issues, difficulty translating activities to virtual delivery platform (cooking demonstrations and making cleaning solutions), and difficulty engaging providers.
Educator-Reported Challenges to One-on-One Visit and Group Class Delivery
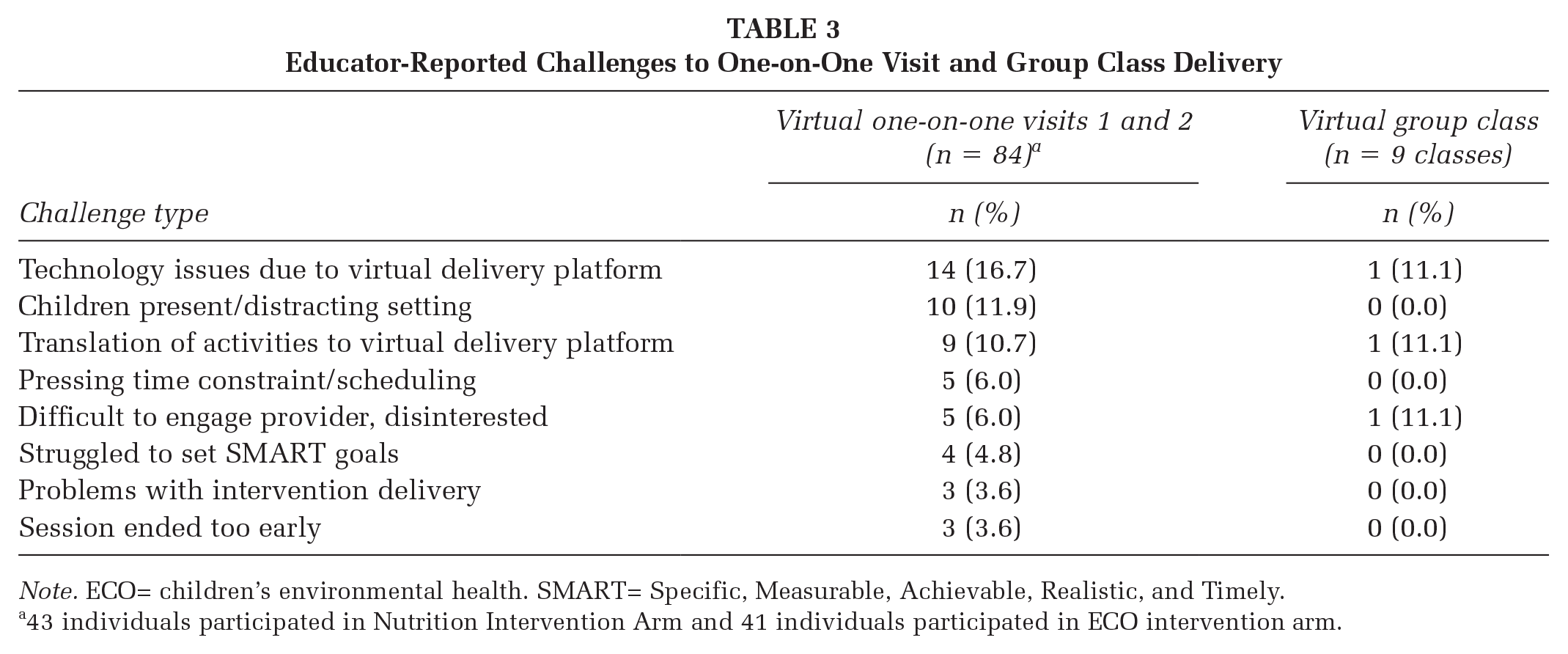
Note. ECO= children’s environmental health. SMART= Specific, Measurable, Achievable, Realistic, and Timely.
43 individuals participated in Nutrition Intervention Arm and 41 individuals participated in ECO intervention arm.
Exploration of FCS Extension Educators Experiences
All supporting quotes are in Table 4.
Interview Questions, Items, Overarching Themes and Sample Quotes
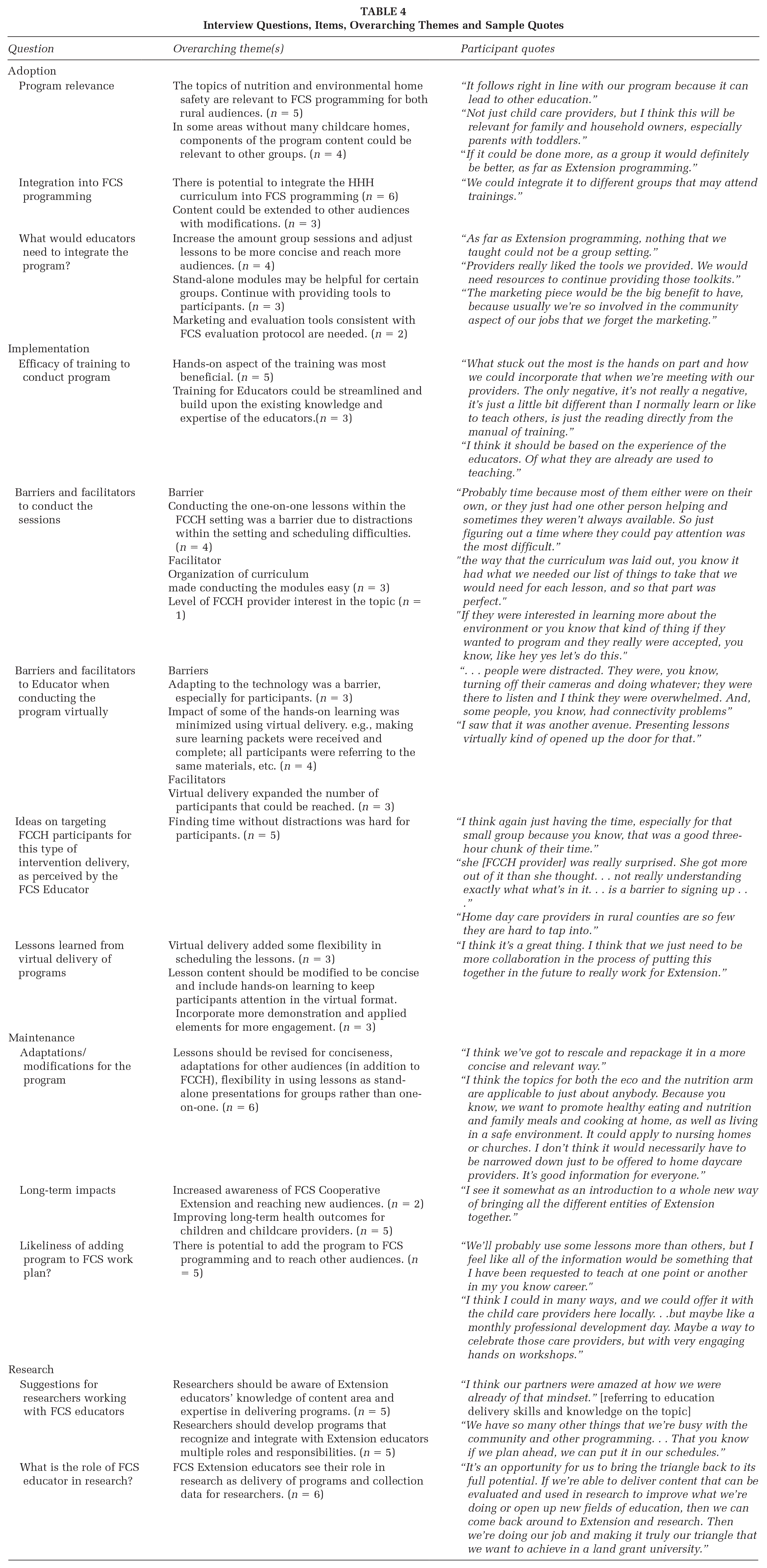
Adoption
Adoption refers to factors that influence the Educator’s ability to adopt and integrate HHH into Extension practice (Glasgow et al., 1999, 2019). The Educators believed the topics of childhood nutrition and environmental home safety were relevant and applicable in rural settings. Educators believed that there is an opportunity to integrate HHH content into programming for general audiences. However, to efficiently integrate interventions into county level programming, some modifications from HHH delivery were recommended, such as modifying one-on-one lessons into group lessons and making content more concise. Another suggested modification for sustainability would be the ability for Educators to implement pieces of a curriculum (i.e., a’la carte) in response to a specific community need, rather than the entire curriculum. For example, if a community member or organization requests education on a specific single topic from the curriculum (i.e., using less toxic cleaners in the home) the Educators would like the opportunity to be able to adapt and share only that component of the curriculum.
Educators indicated they felt the toolkits were well received by FCCH providers. However, additional financial resources would be needed to continue to provide behavioral supports (i.e., toolkits). Educators also suggested that additional promotional materials such as marketing flyers and sample social media posts would be useful for future efforts. This recommendation supports program adoption and maintenance.
Implementation
Implementation refers to factors that influence Extension’s ability to adopt and integrate HHH into practice (Glasgow et al., 1999, 2019). Educators reported the hands-on training was beneficial to reinforcing module content. When designing train-the-trainer sessions, the Educators advised that researchers should make sure to consider their existing content knowledge and teaching expertise. For example, working with Educators to understand their familiarity and comfort on a specific topic prior to training. However, some challenges were reported. During the implementation, Educators found the level of distraction in the learning environment, the FCCH, to be a barrier. Sessions were delivered in FCCH provider’s home (pre COVID-19 in person and post COVID-19 via Zoom) at a time that was most convenient to providers, this often ended up being during working hours when children were present. Efforts were made to schedule sessions during nap times or when other staff may be available to assist with the children’s needs, nonetheless, schedule conflicts persisted with a 90-minute individual session and 3-hour small group class.
In March 2020 all programming switched to virtual delivery due to the COVID-19 pandemic. Initially, the adaptation presented technology and delivery of learning tool challenges to both Educators and FCCH providers, many of whom were new to using the Zoom online videoconferencing. Once the challenges were addressed, Educators reported virtual delivery of the program to be a facilitator of program implementation. Virtual delivery afforded the opportunity to offer HHH to FCCH outside of the Educators’ assigned counties, added flexibility in scheduling, and created opportunities for Educator collaboration across counties. To better adapt the HHH to virtual delivery, Educators suggested keeping content concise, retain but modify hands-on learning for virtual delivery, and offering group classes rather than providing one-on-one lessons. It is also important to ensure Educators have ready access to all materials electronically vs. paper copies to demonstrate and show materials and handouts to providers via Zoom.
Maintenance
Maintenance refers to factors that influence Extension’s ability to sustainably integrate HHH into practice (Glasgow et al., 1999, 2019) and the culture and context of Extension over the long term. Educators recommended the lessons be adaptable to other population segments, such as homeowners, parents of young children, and the general community, rather than exclusively focusing on FCCH providers. This would expand reach and community interest which would support maintenance.
Educators did perceive the program to have long-term impacts such as increasing awareness of Extension and reaching new audiences potentially improving health outcomes, such as dietary intake and exposure to toxins, for both children and FCCH providers. An important consideration for researchers to be mindful of when translating research into public health programming using the Extension model is the numerous responsibilities and services provided by Educators. Educators are seldom in the office and may have limited time for detailed processing or noting during intervention trials. Similarly, software used in research, such as REDCap, may be unfamiliar to Educators. Seasonally, Educators have various responsibilities that are largely demanding of their time, such as county and state fair season and could likely prevent research engagement during those times.
Discussion
This paper describes the pilot adaptation and implementation of a virtual health intervention for FCCH providers into the Extension model. Researchers collaborated with Educators on the adaptation of the curriculum for the Extension context, but retained the literature-informed, theoretically driven delivery format of two individual sessions and one small group class, and one phone call check-in. Process evaluation indicated that Educators delivered nearly all intervention components as designed. However, Educators reported some challenges during virtual delivery with the technology, provider engagement, and distractions. Few studies have examined the integration of Educators into health dissemination research, specifically around early care and education providers. Overall, the Educators reported the HHH program was relevant to Extension programming; thus, having aligned goals with the researchers is important to successful collaboration. Key considerations for researchers were identified to build upon Educator strengths and expertise and the diversity and demands of their ongoing Extension responsibilities more seamlessly.
Leadership support, champions, and alignment of research goals and priorities with community needs, and Educator priorities for the research need to be optimally integrated within the Extension model and enjoyed by Educators for long-term program success (Carnes et al., 2019; Wilson et al., 2024). Our findings indicate that the Educators found HHH fit within their community’s identified needs, similar to Dev et al. (2022) and Wilson et al. (2024). Educators in the current study identified that HHH content may be relevant to a general audiences and a larger community interest would be important for sustained integration into programming. In Nebraska, Educators delivered a 16-week intervention to FCCH providers and served as one-on-one “coaches” to enhance responsive feeding practices during mealtimes. In Georgia, Educators delivered the Diabetes Prevention Program series of 22 classes including healthy eating to cohort groups of adults (Wilson et al., 2024). Like Wilson et al. (2024), costs to deliver the intervention, such as toolkit materials, were raised as sustainability and maintenance concerns. Financial support is key to project sustainability and emphasizes the important role of partnership and support from Extension leadership.
In Oklahoma, as with other states, a requirement for employment as an Educator is a master’s degree in a general or focused area under the FCS umbrella. In addition, Educators often have multiple roles within their counties. While it is important for researchers to partner with Educators who have relevant backgrounds (Carnes et al., 2019; Dev et al., 2022; Wilson et al., 2024), as was the case in this project. Educators recommend researchers be cognizant of the level and area of expertise and multiple roles held by the Educators and build on existing strengths. This research emphasized the need for concise materials. Findings from Dev et al. (2022) indicated that Educators were, at times, overwhelmed with the content and rigor of the study and Wilson et al. (2024) indicated that program complexity and time were implementation and adoption barriers. While the HHH Educators did not use the language of overwhelm in this study, the comments to make the content more concise and simpler to deliver amid competing demands is similar. While the intervention was designed with some duplication of content that aligns with pedagogical principles (Batt, 2023) to enhance learning, especially in distracted environments, clearly a balance can be reached that includes necessary level of duplication while maintaining brevity.
Inclusion of Educators in the development or adaption of research interventions will be necessary for the intervention to integrate within the Educator’s competing time demands and the style of training which Educators prefer and are skilled (Dev et al., 2022). While the HHH research team invited the Educators to offer guidance and feedback on intervention adaptation, limited feedback was received which may reflect time constraints. It is important to note that opportunity for review and feedback was conducted in advance of any opportunity for Educators to deliver the intervention. It would be recommended for future partnerships that Educators can learn and familiarize themselves with the intervention and have opportunity to pilot delivery one or two classes to offer more experiential feedback for the intervention.
FCS programs are primarily, if not always, conducted as a single class with groups of adults and/or youth in community settings, whereas HHH included two individual lessons and one small group class with FCCH providers. Utilizing group lessons instead of individual lessons increases the number of people who can be reached, which is consistent with the concept of existing public health education approaches. However, formative work for this research study indicated that FCCH providers indicate they are often unable to attend in-person group classes due to restrictive work and personal schedules (Sisson et al., 2021). Rural and remote FCCH providers may experience this concern to a greater degree than urban providers given the travel distance for class participation. However, offering in-person, virtual, or hybrid-style small group classes in rural counties could increase reach for multiple FCCH providers, decrease the distance needed to travel for group training, and establishing social support and observational learning (Bandura, 1998).
While pivoting the program for virtual delivery was preemptively addressed by researchers and Educators, actual implementation had its challenges both in technology, adjusting the program to fit the virtual delivery, engaging providers virtually with children present around them, and logistics and shipping issues surrounding the delivery and procurement of supplies for the intervention, toolkits, and small group classes. However, Educators thought there might be some positive aspects to virtual delivery in expanding reach to audiences outside of their county and providing flexibility in scheduling. Other research studies have observed that transition from in-person to virtual educational instruction has led to overall positive outcomes when technological support for online learning is available (Carnes et al., 2019; Lemay et al., 2021).
The study has several strengths. Educators not only work in the community but are also a part of the community. As members of the community, Educators understand needs and disparities. Educators were invited to participate in the research, their time was supported, and they were included in curriculum modification and adaptation prior to in-person delivery and during the pivot to virtual delivery due to COVID-19. However, Educators did not receive financial benefit for their time supported in the project and the state retained the salary savings. For future research to be successful, the state may have financial incentive in Educator salary savings to participate in research, but Educators could also be incentivized with salary offset benefits or in other ways (Wilson et al., 2024) to further promote research partnerships in the Extension model. Study development was guided by the RE-AIM Framework to understand actual implementation, adaptation, and sustainable maintenance of research interventions in the Extension context. Process evaluation measures were detailed and self-reported by Educators. Qualitative data were collected from Educators who conducted the HHH intervention in different areas of rural Oklahoma which allowed for multiple perspectives. Probing questions used during the interviews helped achieve saturation. One Educator was able to review findings to ensure accuracy. In addition, the HHH principal investigator reviewed the interview questions prior to the interviews as well as the units of dialogue, thematic analysis, and findings. All of which contribute to the trustworthiness of the findings.
Limitations included the lack of objective process-evaluation observations and the amount of time between the program conclusion and when the interviews occurred. Interviews took place in the fall of 2021 and the program ended November 2020. This is a small study with only six Educators participating and focused on mostly the rural areas of Oklahoma and excluded urban areas.
Implications for Practice
Numerous implications for practice have emerged from this study, for researchers and for Educators. Adaptable and flexible partnerships that honor the Educator’s background, Extension context, and the researchers’ needs for rigor in implementation and evaluation are ideal. First and foremost, the experience and community-perspective of the Educator needs to be a priority for researchers to understand and collaborate to develop or adapt interventions for the local community with Educators’ program delivery expertise and firsthand knowledge of their population and community. Educators are familiar with program evaluation; however, can also be aware of the more detailed types of data necessary for research trials. Advance opportunity to pilot intervention content and utilize research-related software can promote intervention adaptation and smooth implementation and reporting.
Organizational leadership support and buy-in is essential for the Educators to have support and ability to implement these research-based interventions. Both sides can work to develop relationships so that research can be used to support community problems observed by Educators. Educators prefer intervention programs that can be delivered in a group and to a variety of audiences, thus provision of materials in a manner that can be adapted for various audiences may be helpful to Educators. This may or may not be feasible for the context of conducting research on target populations. Educator awareness of possible limited flexibility in controlled research designs may be helpful to promote understanding of the rigors of research design. Educators prefer interventions that are concise and can be delivered in an hour or less and include numerous interactive and hands-on elements. Inclusion of Educators serving as key informants in the intervention development and adaptation can promote conversation on intervention delivery that meets both the researcher and Educator needs, capacity, and preferences.
The application of a virtual intervention was novel in the Extension context and while challenges arose, the flexibility and reach of a virtual intervention was favorable. Provision of all materials electronically as well has hard-copy for Educators and participants would enhance the virtual learning environment. Technology issues identified by Educators including internet connectivity, device compatibility, and the nascent use of Zoom in the early days of the COVID-19 pandemic. Educators and researchers can consider provision of hot spots and trainings/practice connecting to support connectivity to the virtual platform.
Conclusion
Study results have implications for informing researchers seeking to design programming and collaborate with Cooperative Extension in rural communities. Taken together with previous research (Dev et al., 2022; Wilson et al., 2024), these studies indicate that interventions and research that work with early childhood health, and specifically nutrition, may be salient targets and integrate with Educator expertise and community needs. Educators were able to successfully deliver the individual-level intervention using virtual technology. Extension has the opportunity to expand service and integrate with researchers to deliver dissemination and implementation research trials. However, this integration and process must first include Educators in the process and align with their community priorities and other programmatic demands.
Footnotes
Authors’ Note:
We acknowledge the support and contributions of our community partners and food program sponsors, who all worked diligently to ensure successful recruitment efforts and enhance quality of data collection and processing for the intervention. We appreciate and acknowledge the support of the Cooperative Extension Educators in their dual roles of delivering the intervention and volunteering to offer feedback as a participant in this study. We appreciate the Happy Healthy Homes research team members for support in data collection and management. We are deeply grateful to the child care providers who allow us into their homes and who wish to create healthier spaces for young children. This study is supported by Agriculture and Food Research Initiative grant no. 2017-68001-26355 from the United States Department of Agriculture National Institute of Food and Agriculture and the National Institute of General Medical Sciences of the National Institutes of Health under award number U54GM104938. Any opinions, findings, conclusions, or recommendations expressed in this publication are those of the authors and do not necessarily reflect the views of the US Department of Agriculture or the National Institutes of Health.