
Abstract
Dental providers play a critical role in public health initiatives, contributing to broader health promotion efforts despite not treating systemic illnesses like HIV directly. Collaboration with nontraditional partners, such as dentists and dental hygienists, is essential for achieving the health promotion goal of ending the HIV epidemic (ETE) by 2030. This study recruited 15 dental providers (seven dentists and eight dental hygienists) from Connecticut via dental associations, academic programs, and social media. Participants completed a semi-structured interview guided by the Social Ecological Model and a brief survey to capture demographics and HIV knowledge. Data were analyzed using the RADar (Rigorous and Accelerated Data Reduction) technique. Participants were predominantly female (66.7%) and White (66.7%) and averaged 48.4 years old. The mean HIV knowledge score was 32 out of 41 (78%). Key themes included (1) continuing education, (2) knowledge of pre-exposure prophylaxis (PrEP) and HIV, (3) communication best practices, (4) care coordination best practices, and (5) the role of dental providers in ETE efforts. This study underscores the need for collaborative efforts between dental providers and health promotion practitioners to address HIV-related knowledge gaps, stigma, and care coordination through targeted training and communication strategies, while also calling for further research into organizational and policy-level changes that can better integrate dental care into HIV initiatives.
Since being declared an epidemic in the 1980s, human immunodeficiency virus (HIV) continues to be an issue of public health significance (Kaiser Family Foundation, 2023). An estimated 29 million people are living with HIV globally, including 37.5 million adults and 1.5 million children (HIV and AIDS Epidemic Global Statistics, 2025). However, significant progress has been made in curbing the epidemic, as the number of people with HIV (PWH) receiving treatment has reached 29.8 million (Kaiser Family Foundation, 2023). Furthermore, new infections of HIV, which can lead to the development of acquired immune deficiency syndrome (AIDS), have declined by 38% since 2010 (HIV and AIDS Epidemic Global Statistics, 2025). Still, the HIV epidemic is far from over, as significant challenges remain that impede the success of existing interventions (Giroir, 2020).
Despite the U.S. government spending $20 billion in annual direct health expenditures for HIV prevention and care, there are concerns of a resurgence attributable to several factors, including HIV-related stigma, trends in injection and other drug use, lack of access to HIV prevention, testing, and treatment; and the lack of awareness that HIV remains a significant threat to public health (HIV and AIDS Epidemic Global Statistics, 2025). According to the Centers for Disease Control and Prevention (CDC), 40% of new HIV infections are transmitted by people who do not know they have the virus. Thus, ensuring access to HIV screening and early diagnosis, particularly among populations at greatest risk, is crucial to curbing the epidemic (HIV and AIDS Epidemic Global Statistics, 2025). With this in mind, a federal initiative known as Ending the Epidemic (ETE) seeks to reduce the number of domestic new HIV infections by 75% by 2025, and then by at least 90% by 2030. These efforts would avert an estimated 250,000 total infections (NIH, 2021).
A potential opportunity to enhance HIV prevention efforts is to harness dental providers’ direct access to patients. The U.S. dental workforce comprises more than 750,000 dental professionals, including dentists, dental hygienists, and other providers (NIH, 2021). There have been calls to expand the scope of practice for dental providers to encompass additional health services, including screenings often seen in primary care settings (Lamster & Eaves, 2011; Riddle, 2020). With an estimated 70% of US adults seeing a dentist in the past year and considering an aging population with health concerns, dental providers can address gaps in general health care by providing services beyond their traditional scope of practice (Lamster & Eaves, 2011). The opportunity to integrate HIV preventive care is also relevant to the dental profession, given that oral manifestations are prominent in PWH (Lomelí-Martínez et al., 2022). Dental care settings are also positioned to offer effective HIV preventive services to patients, such as rapid HIV screening (Pollack et al., 2010). Studies have also documented patients having positive attitudes toward HIV screening being offered at dental sites, although more research is needed to corroborate such findings (VanDevanter et al., 2012). In addition, studies have suggested dental care providers may have access to patients who are at risk for HIV and are unlikely to be tested in other settings (Blackstock et al., 2010; Pollack et al., 2010).
While dental providers consider health screenings to be important and aim to incorporate them into their practices (Greenberg et al., 2010), research assessing their attitudes, beliefs, and perceived barriers to integrating HIV screening and other preventive services is limited. A qualitative study involving dental school faculty and students documented high acceptability toward offering routine HIV screening. However, significant barriers—ranging from discomfort communicating about HIV to patients and concerns around patients’ reactions to HIV testing—were highlighted (Hutchinson et al., 2012). Additional studies are needed to identify best practices for dental providers in effectively communicating with PWH.
Communication and coordination among dental providers, primary care providers, and other specialists are essential to ensure that PWH receive integrated care that addresses both their oral and overall health. PWH often have complex medical needs, and their oral health can be affected by both the HIV disease and the antiretroviral therapy (ART) medications used to manage it (Lomelí-Martínez et al., 2022; NIH Office of AIDS Research, 2023). Considering HIV can lead to significant oral health issues such as xerostomia, gingivitis, periodontitis, and oral candidiasis, PWH need consistent and coordinated dental care (NIH, 2024). Dental providers must be aware of the patient’s medication regimen to prevent complications, manage side effects, and avoid drug interactions that could impact oral health. Dental visits can also provide an opportunity to identify signs of systemic health issues related to HIV that the primary care provider may not recognize or require close coordination between the dental provider and the primary care provider (Lomelí-Martínez et al., 2022).
Furthermore, effective communication between primary care providers and dental providers allows the dental team to track changes in patient health status over time and collaborate on preventive strategies to manage and mitigate health risks (Atchison et al., 2018). By maintaining open communication with primary care providers and other specialists, dental providers can develop a deeper understanding of these factors and create a supportive environment for the patient. Challenges in interprofessional communication include significant power differences between providers, the wide range of tasks in primary care, and less teamwork in practice than is ideally expected (Fox et al., 2021). Nevertheless, enhancing communication strategies between primary care providers and dental providers is essential as the U.S. health system shifts toward integrated care models that aim to treat the whole person rather than merely addressing isolated health issues.
Building upon the limited literature, the purpose of this study was to identify the best communication strategies that dental providers may adopt when discussing HIV prevention and care with patients. In addition, this study seeks to explore how dental providers can effectively coordinate with colleagues in primary or specialty care to support HIV prevention efforts and improve patient outcomes, thereby contributing to ETE efforts.
Method
A phenomenological qualitative design was used in this study as we describe the experience of dental providers. Semi-structured interviews with dentists (n = 7) and dental hygienists (n = 8) practicing in Connecticut were used as the primary data source to contextualize the experiences and perspectives of these providers. Our analysis sought to synthesize their experiences as we explored the data to reveal descriptions of their phenomena. This project was approved by the Fairfield University Institutional Review Board (4103-2023).
Eligibility criteria included individuals who are licensed and practicing dentists and dental hygienists in Connecticut. The recruitment process began by compiling a list of universities that offer dental (n = 1) and dental hygiene (n = 5) degrees, hospital dental departments (n = 17), dental residency programs (n = 2), federally qualified health centers (n = 19), regional dental societies (n = 22), and a state dental hygiene association (n =1).
The key contacts of those organizations were sent an introductory email with a request to distribute the study flier to their respective constituency groups. The study flyer was also shared with multiple dental Facebook pages. Interested persons were contacted by the research team via email to be screened to ensure eligibility. If eligible, participants were scheduled for a Zoom interview.
Each interview session lasted for approximately 1 hour. Interviews began with a review of the consent form, obtaining verbal consent, and administration of a demographic survey. The demographic survey collected demographic and professional information from participants and assessed their knowledge of HIV and pre-exposure prophylaxis (PrEP). It included 12 questions on participants’ gender, age, race/ethnicity, education, and experience working with individuals at risk for or living with HIV. The second part of the survey evaluated participants’ understanding of HIV-related topics using a 28-item knowledge assessment on the effectiveness of PrEP, treatment for HIV, and the transmission and prevention of HIV, modeled after a study of pharmacy students (Bunting et al., 2021). We performed descriptive statistics to summarize the survey data.
We developed a 15-item semi-structured questionnaire guided by the Social Ecological Model (SEM; Wold & Mittelmark, 2018). The SEM has been used as a guiding framework to examine the multiple levels of influence on health and behavior, from individual to societal/policy (Dyson et al., 2018; Golden et al., 2015; Wold & Mittelmark, 2018). The SEM has also been used as a guiding framework to examine the multilayered factors, ranging from individual-level stigma and fear to systemic issues like care fragmentation and social determinants of health and understanding of multiple levels of HIV risk, that shape referral behaviors and attitudes toward dental and mental health services among PWH (Baral et al., 2013; Sterrett-Hong et al., 2023). At the individual level, personal knowledge, attitudes, and practices that influence HIV prevention and care decisions, such as continuing education (CE) choices and familiarity with biomedical interventions like PrEP and ART, play a significant role. The interpersonal level focuses on patient communication strategies and coordination with primary and specialty care providers, which can directly impact care coordination and patient outcomes. At the organizational level, dental practice policies and practices, such as whether HIV testing is offered, are crucial in determining the scope of services. At the community level, professional identity, norms, and collective efforts can either foster or hinder involvement in broader health promotion initiatives, such as involvement in professional organization efforts to end the HIV epidemic. Finally, the societal/policy level highlights how external factors, such as provider licensing and regulations, can either support or impede HIV-related coordination and communication. Each question on the semi-structured interview guide explored one or more of these levels, providing an understanding of the complex factors influencing HIV care in the dental setting.
The lead researcher (A.J.S.) conducted all 15 interviews. All interviews were audio-recorded. After the interview, participants were sent a $25 electronic gift card incentive. The audio recordings were forwarded for verbatim transcription by a professional service. Once the written transcripts were returned, the analysis began.
We employed a phenomenological approach within an interpretivist paradigm, using an inductive method involving constant comparison to analyze the data and develop a list of themes (Smith & Fieldsend, 2021). The primary aim of this study was to explore a phenomenon openly and inductively, allowing new insights and themes to emerge directly from the interview data. This approach prevented premature constraint by theoretical frameworks such as the SEM and allowed the findings to naturally shape the direction of the study and interpretation of results (Creswell, 2014). To facilitate this process, we used the RADaR (Rigorous and Accelerated Data Reduction) technique, a validated method for analyzing textual data (Watkins, 2017). All four team members independently organized the raw transcript data into an Excel table, developed codes, and identified which codes appeared most frequently across all coders. From these frequently used codes, we collaboratively selected those most relevant and reduced the data to generate key themes, which were unanimously agreed upon. Representative quotes were then selected to support each theme.
Results
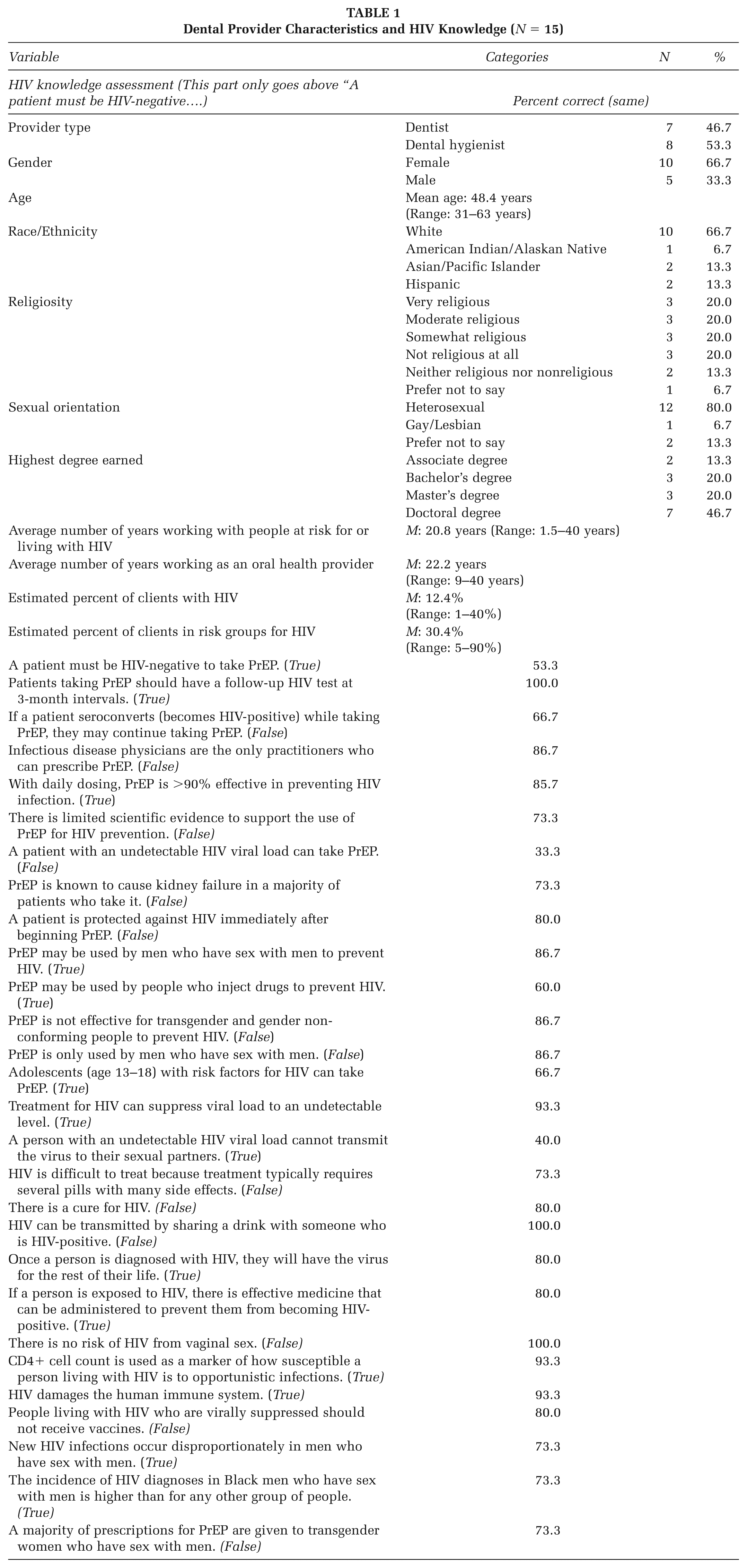
As shown in Table 1, participants were mostly female (66.7%), White (66.7%), and heterosexual (80%), with an average age of 48.4 years (range = 31–63 years). On average, the participants had been working as a provider for 22.2 years (range = 9–40 years) and had been working with people at risk for or living with HIV for 20.8 years (range = 1.5–40 years). HIV knowledge questions that were answered correctly by less than half of the participants included: “A patient with an undetectable HIV viral load can take PrEP” (33%) and “A person with an undetectable HIV viral load cannot transmit the virus to their sexual partners” (40%).
Dental Provider Characteristics and HIV Knowledge (N = 15)
Key themes included CE, knowledge of PrEP and HIV, HIV testing, communication best practices, care coordination best practices, and the role of dental providers in ending the HIV epidemic.
Continuing Education
Many participants in our study highlighted the importance of CE in their respective fields. When selecting CE courses, dentists often prioritize content based on their interests, which helps them stay informed on the latest dental practices and understand patient requirements. As one participant shared, “I’m really looking for topics that keep me up to date in the various areas of pathology and clinical pathology that I’m interested in,” highlighting the importance of relevance and professional alignment in course selection. In addition, participants noted the absence of HIV-specific CE opportunities, with most noting they encountered this topic only within broader infection control or disease prevention training. One dentist explained, “Not directly HIV related. It was an infectious disease seminar given by pathologists at Salt Lake City around a month ago,” illustrating how HIV-related content is typically embedded within larger seminars rather than offered as a stand-alone topic. These reflections from both dentists and dental hygienists underscore how CE is integral to the success and effectiveness of dental providers, enabling them to stay current, deliver high-quality care, and contribute to the overall advancement of the field.
Knowledge of PrEP and HIV
Dental providers in our study overwhelmingly expressed a willingness to learn about PrEP and HIV treatment medications. It was noted by a few participants that dental treatment is not impacted by taking medications for HIV prevention or treatment. One dentist explained, “So, as far as dental treatment goes, it doesn’t really affect our—I don’t feel like it really affects our field in any different way.” Another dentist expressed enthusiasm for learning about PrEP and HIV through the interview process noting “Honestly, not much. I think that I can stand to learn a lot more about it. So, I’m excited to have our discussion today, and that might be illuminating for me.” Overall, many participants expressed openness to learning more about PrEP and HIV-related medications, particularly in the context of providing supportive, informed care and working collaboratively with other health professionals.
HIV Testing
Participants expressed mixed views about the role of HIV testing in dental settings. While many acknowledged that offering rapid HIV testing is feasible in the dental setting, a few raised concerns about the logistical challenges, operational constraints, and potential stigma associated with providing such services. A dental hygienist participant explained,
So, I think, where I work, yes, it’s feasible. . . . I would worry though because not everybody treats people well, I guess. Same thing with COVID. Like ‘Oh, my gosh. My rapid. . .’ Imagine something as sensitive as this. I think it may further stigmatize. It depends on people’s comfort level and education and personal bias.
Several participants also noted that the ability to implement HIV testing varies depending on local regulations and state-specific scope of practice. Some participants also pointed out that broader acceptance would likely require stronger evidence of feasibility and impact. A dentist stated, “I think a multi-central study that demonstrates the acceptance and efficacy, much in the same as dentists who are recruited to administer COVID vaccine at the heart of the pandemic [would be needed].”
Communications Best Practices
All participants noted the importance of effective provider-patient communication as foundational to delivering high-quality, patient-centered care. For instance, most participants emphasized the value of incorporating motivational interviewing (MI) strategies—such as openness, empathy, and active listening—into their interactions with patients. One dentist said,
The motivational interviewing piece comes into place, and then following up with the patients, I think is the critical, most important thing. As you know now the providers are very busy, right? So, maybe the follow-up with the patients I feel like in that area of the communication gap, I mean, it’s not the communication gap, but the gap in care falls when we don’t follow up with the patients and help them understand that it’s very important to follow up for care.
Other participants expressed uncertainty around how to approach conversations about HIV or PrEP, citing a lack of formal training or guidance from regulatory bodies and professional associations. One dentist shared,
I just don’t think we have those conversations in general . . . I know of patients that have had HIV and I’ve talked to them and we talk about where they are in their medication regimen, just because I don’t know anything about it and I’m learning from them. But I just don’t think that that’s what dentists get. I don’t think that’s in our wheelhouse at all, really.
Care Coordination Best Practices
All participants expressed the need for increased collaboration and coordination between dental care and primary care providers around HIV prevention and treatment. In particular, some expressed a strong desire for universal electronic health records to facilitate interagency collaboration. A dentist noted,
Being outside of this prior to this role, I will say that it is a lot more challenging, unless you are really well connected with your internal medicine docs or the medical community. Unfortunately, I don’t see this integration as much. It has a lot of potential, but I just don’t think dentistry and medicine are integrated in a way that they really need to be, but I’m hopeful that there’s a lot of push toward this integration in the next five, 10 years.
On the other hand, a dental hygienist stated, “So, education, pamphlets, referrals. I’m quite limited on what I can do, but I always want to put the patient in contact or in touch with somebody that can actually help more.”
Role of Dental Providers in Ending the HIV Epidemic
Most participants acknowledged that dental providers are uniquely positioned to contribute to efforts to end the HIV epidemic, particularly through patient education and increasing awareness around HIV prevention and treatment. Given their regular contact with patients—including those who may not otherwise access traditional medical care—dental professionals have an opportunity to play a more active role in HIV-related outreach and screening. A dental hygienist noted,
But the whole dental team starting from reception, what’s on the walls in the waiting area, what’s on the TV screens, I think that this is a group effort. It’s not only the providers. So, I think that in order to help patients and make this stigma go away, I think that everybody in the dental office should be on board. There’s a lot of continuing education courses for dentists and hygienists, but there’s nothing really for assistants or receptionists.
However, several participants identified significant barriers that limit this involvement, including lack of time, professional burnout, low interest in public health topics, and a tendency to adhere to more traditional dental roles. A dentist added,
The landscape of dentistry is changing so rapidly and in a direction that’s so frightening because I don’t think it promotes really good care for the dental patient . . . I think that we are inundated with we’re just trying to survive the day, and so I don’t think that dentist can necessarily take on one more thing . . . So, quite honestly, we’re struggling so much financially with insurance cutbacks and rising costs of our payrolls that—and a shortage of ancillary help that we I think to take on something that, and it’s so sad, but that isn’t necessarily going to produce a revenue stream it is going to be ignored by the majority of dentists.
Discussion
The results of the interviews conducted as part of this study emphasize the influential role of CE for dental providers, particularly as an avenue for HIV and PrEP education. Dentists licensed to practice in Connecticut must obtain at least 25 contact hours of qualifying CE every 2 years (Connecticut Department of Public Health, n.d.-b). While infection control is listed among the 10 mandatory topics for CE activities, HIV prevention is not explicitly mentioned (Connecticut Department of Public Health, n.d.-b). Although state and local health departments may offer and approve qualifying CE activities, it is important to note that the Connecticut Department of Public Health currently does not. Qualifying CE activities may also be approved by several governing bodies, such as the American Dental Association (ADA) or state, district, or local dental associations associated with the ADA. Hospitals or other health care institutions, dental schools, and many other agencies recognized by the Council on Dental Accreditation, among many others, may also offer or approve qualifying CE activities (Connecticut Department of Public Health, n.d.-b).
Dental hygienists are also mandated to earn CE hours, as those licensed in Connecticut are required to obtain a minimum of 16 hours of CE over 2 years. As with CE requirements for dentists, dental hygienists must also obtain infection control-related training or education (Connecticut Department of Public Health, n.d.-a). To ensure both HIV and PrEP education are included as part of CE, the ADA, and other professional societies and governing bodies, responsible for approving CE opportunities, need to play a more active role. To overcome concerns around time constraints to HIV prevention in the dental setting, as some of this study’s participants raised, additional studies are needed to further explore innovative approaches to assessing patients’ risk for HIV before their arrival to receive care, such as the use of computer-based risk assessments (Silapaswan et al., 2017).
Prior studies have not only supported the possibility of providing HIV screening in dental settings (Pollack et al., 2014; Riddle, 2020; Santella et al., 2013) but have also documented dental providers’ willingness to provide it (Pollack et al., 2014). While some studies have raised patient acceptance as a potential challenge to implementing HIV screening in dental settings (Patel et al., 2015), a growing number of studies have documented positive attitudes, beliefs, and acceptance, further supporting efforts to offer such services (Chung et al., 2020; VanDevanter et al., 2012). In addition, patients, particularly PWH, are often concerned with experiencing HIV-related stigma and shame. Such stigma is also associated with reduced health-seeking behaviors (Carr & Gramling, 2004; Fortenberry et al., 2002).
Dental providers need to obtain education about HIV prevention, as studies suggest a lack of PrEP knowledge is a barrier to provider engagement in patient-centered discussions (Wilson et al., 2021). The CDC estimates that 1.2 million people in the U.S. could benefit from PrEP (CDC, 2023). The medication was first approved for HIV prevention in 2012 and is attributed as a factor in recent decreases in new HIV infections (CDC, 2023). There is currently a shortage in the number of health care specialists available to meet the growing demand for providers trained to provide PrEP (Silapaswan et al., 2017). The low results of the HIV knowledge test administered as part of this study underscore the need for PrEP education for dental providers. Studies have suggested that PrEP education among providers is associated with its prescription, suggesting education to be a key component of the medication’s implementation (Blumenthal et al., 2015). In addition, studies have shown that health care providers who are more knowledgeable about CDC guidelines for PrEP delivery demonstrated greater odds of prescribing PrEP to adolescents (Price et al., 2023). Thus, increasing dental providers’ knowledge of PrEP may contribute to an increase in prescribing PrEP and a decline in the prevalence of new HIV infections.
Furthermore, stigma and discrimination are significant barriers to medical and dental care access for PWH. These attitudes often exacerbate the challenges faced by PWH, leading to delays in seeking care, poor mental health, and reduced treatment adherence. Stigma within health care settings can also erode patient–provider trust, further marginalizing PWH, who are already disadvantaged in many areas of society (Yuvaraj et al., 2020). It has been observed that dentists continue to stigmatize PWH, largely due to persistent negative attitudes, which manifest in avoidance or hesitation to treat such patients. This is further fueled by fears of transmission, misconceptions about HIV, discomfort with treating PWH, and the belief that they are at higher risk for opportunistic infections. The stigma is further compounded by a lack of knowledge or awareness about the chronic nature of HIV and the effectiveness of modern treatments (Giuliani et al., 2023; Patel et al., 2015). Considering the pervasive role of stigma in health care settings, particularly around HIV care, ongoing efforts are needed to mitigate its adverse impact. In particular, interventions at the individual (e.g., increasing awareness of what stigma is conceptually and the benefits of its reduction), environmental (e.g., educational programs around HIV transmission), and policy (e.g., addressing discrimination toward patients with HIV) level in health care settings, including dental care settings, ought to be considered (Nyblade et al., 2009).
This study has some limitations that should be noted. First, the study was limited to dentists and dental hygienists in Connecticut who may not represent the larger dental workforce in other parts of the country, particularly those with greater incidences of HIV. In addition, the participants may also not represent the views of the dental workforce, especially those outside of academic medical centers and community clinics, so these results should not be generalized. Moreover, several of the participants were recruited by word-of-mouth despite the recruitment efforts noted in the methods section.
Overall, this study provides health promotion practitioners, health system leaders, and other decision-makers with valuable insights into dental providers’ knowledge and attitudes toward ETE efforts, with a focus on the role of communication and coordination. By emphasizing health promotion in dental settings and investing in workforce development, these findings can support more effective interventions and contribute to better population health outcomes.
Implications for Practice
Our findings highlight an opportunity that would require the collaboration of both dental providers and health promotion practitioners in their broader efforts toward ETE efforts. In particular, our interviews with dental providers suggest existing gaps in HIV and PrEP-related knowledge, stigma, and care coordination within the dental setting. Considering the SEM, dental providers would benefit from targeted CE that not only builds upon their foundational knowledge of HIV prevention strategies (i.e., PrEP) but also fosters their confidence in initiating patient-centered conversations (individual level). Health promotion practitioners can support such efforts through their ability to design and offer tailored interventions (e.g., CE training and workshops) to mitigate existing knowledge gaps among dental providers.
Concerning the interpersonal and organizational levels, there is a need for communication strategies that foster trusting patient-provider relationships, while also reducing the existing stigma when it comes to caring for PWH. This is another implication for health promotion practitioners who can offer culturally responsive MI techniques and strengthen existing referral navigation through case-based simulation or peer learning. They can also develop training sessions for primary care and dental providers on the bidirectional relationships between oral health and systemic conditions while also creating culturally competent patient education materials that emphasize the impact of oral health on overall well-being and the importance of regular dental and medical visits.
Finally, professional organizations and health departments have a key role in legitimizing the dental workforce’s role in the ETE efforts (community and societal/policy level). Such efforts include advocating for CE requirements that explicitly address HIV screening and raise PrEP knowledge and may also encompass revising existing evidence-based guidelines to better incorporate HIV testing and referral pathways in dental care.
Implications for Research
In our study, communication and coordination between dental and medical providers and re-imagining the role of practice guidelines to better integrate the dental-medical connection emerged as areas needing further investigation. Future research could explore the SEM organizational level by focusing on referrals and care coordination and examining the effectiveness of simulation-based training. For example, such research could evaluate how such training influences dental providers’ ability to manage referrals to primary and specialty care. A key component of this research would involve identifying structural and workflow barriers to integrating HIV-related referrals into routine dental care. Furthermore, at the SEM policy level, another study could examine the role of professional accreditation and licensing bodies in advancing HIV prevention. For instance, a study involving interprofessional and intersectoral stakeholders could identify barriers and facilitators to practice guideline recommendations for dental CE integration.