
Abstract
Alcohol consumption among adolescents is a critical public health concern, leading to numerous adverse health, social, and economic consequences, which underscores the need for effective prevention strategies. This study aimed to conduct a situational analysis and produce a knowledge synthesis in the initial phase of the Prev.Action study, a multicomponent co-produced community intervention aimed at reducing alcohol use among Brazilian adolescents. This mixed-methods study conducted a comprehensive situational analysis to assess adolescent alcohol use in a Brazilian municipality, corresponding to Phase 1 of the Implementation Research Cycle. We employed three types of triangulation: data source, methodological, and investigator. Data were collected from five sources: a school-based survey (1,210 adolescents), focus groups (144 adolescents), semi-structured interviews with stakeholders (26 participants), a community web-based survey (516 participants), and stakeholder workshops (20 participants). Quantitative data were analyzed using descriptive statistics, whereas qualitative data underwent thematic analysis, ensuring a thorough understanding of community needs and intervention barriers. Key findings revealed that 54% of middle school and 73% of high school students had experimented alcohol. In addition, 13% of students reported binge drinking in the last 30 days. The primary methods of alcohol acquisition were self-purchase (30%) or receipt from parents (40%). Priority issues identified by the community, such as easy access to alcohol, cultural acceptance, and inadequate law enforcement, were key in designing a three-arm multicomponent intervention: school-based programs, family programs, and environmental strategies. The Prev.Action study underscores the importance of community involvement and tailored strategies to reduce adolescent alcohol consumption effectively.
Keywords
Excessive alcohol consumption poses a significant public health concern, resulting in numerous adverse consequences for the population (Levesque et al., 2023). It is associated with more than 200 diseases and injuries, including mental and behavioral disorders, cirrhosis, various cancers, and cardiovascular diseases. In addition, alcohol contributes to intentional and unintentional injuries, such as those caused by traffic accidents, violence, and suicides (World Health Organization [WHO], 2024).
In 2024, the WHO reported that 17% of the global population aged 15 and above reported binge drinking in the last month. This rate reached 20.9% in Brazil. With approximately 2.5 billion people currently consuming alcohol, the severity is underscored by the fact that nearly a quarter (22%) of all adolescents aged between 15 and 19 reported having consumed alcohol in the last year (WHO, 2024). Preventing harmful alcohol consumption throughout life is therefore essential to mitigating these challenges.
The most effective strategies for reducing adolescent alcohol use are multicomponent, multisectoral interventions implemented through community-based approaches (Holder, 2002; Komro et al., 2008; Koning et al., 2009; Spoth et al., 2005; Toomey & Lenk, 2011; United Nations Office on Drugs and Crime [UNODC], 2018). These strategies engage communities by reshaping social norms around alcohol consumption through measures such as enforcing alcohol policies (e.g., restricting sales to adolescents), reducing alcohol’s visibility, and offering incentives to promote behavioral change (Bruce et al., 2002; Giesbrecht & Haydon, 2006; McLeroy et al., 2003). Rather than focusing solely on the individual, community-based interventions aim to mobilize key stakeholders—such as policymakers, educators, and regulators—to influence the broader social and regulatory environment in which alcohol use occurs (Stockings et al., 2018; Segrott et al., 2025).
Although some studies have demonstrated the effectiveness of these interventions in the Brazilian context (Garcia-Cerde et al., 2023; Sanchez et al., 2021, 2024), they were often implemented in isolation, without integration with other components or the involvement of local stakeholders in the adaptation and implementation processes. This may have limited their reach and compromised their long-term sustainability (Medeiros et al., 2016; Melo et al., 2022; Murta et al., 2018; Stirman et al., 2012). In this context, implementation research is a critical tool for addressing these challenges by examining how evidence-based interventions can be effectively applied, adapted, and sustained in real-world settings (Theobald et al., 2018).
The Prev.Action was designed precisely to address these limitations by proposing a multicomponent, intersectoral, and evidence-based intervention co-created with local stakeholders. Focused on reducing alcohol use among adolescents, the initiative integrates school, family, and environmental components into a coordinated model tailored to the specific realities of small municipalities. To guide its development and implementation, Prev.Action adopts the WHO’s Implementation Research Cycle (IRC), which provides a structured, four-phase framework for community-based interventions. These phases include (1) identifying evidence-based policies suitable for the local context, (2) adapting and piloting interventions, (3) evaluating implementation, and (4) scaling up. The first phase involves situational analysis and knowledge synthesis, including stakeholder engagement, needs assessment, and evidence review to design context-appropriate strategies (WHO, 2016).
This article focuses on the initial phase of the Prev.Action, while subsequent phases are currently underway. Specifically, it aims to (1) identify key risk factors and patterns of adolescent alcohol use using mixed-methods research, (2) synthesize evidence on effective alcohol prevention interventions for the local context, and (3) collaborate with stakeholders to co-produce actionable strategies tailored to community needs.
Method
Study Design
This mixed-methods study evaluates municipal needs for preventing adolescent drug use in Cordeirópolis, a city 160 km from São Paulo (Brazil), with a population of 24,514 (2022) and an Human Development Index (HDI) of 0.758. In 2021, the city’s Gross Domestic Product (GDP) per capita was ≈ USD 31,453.
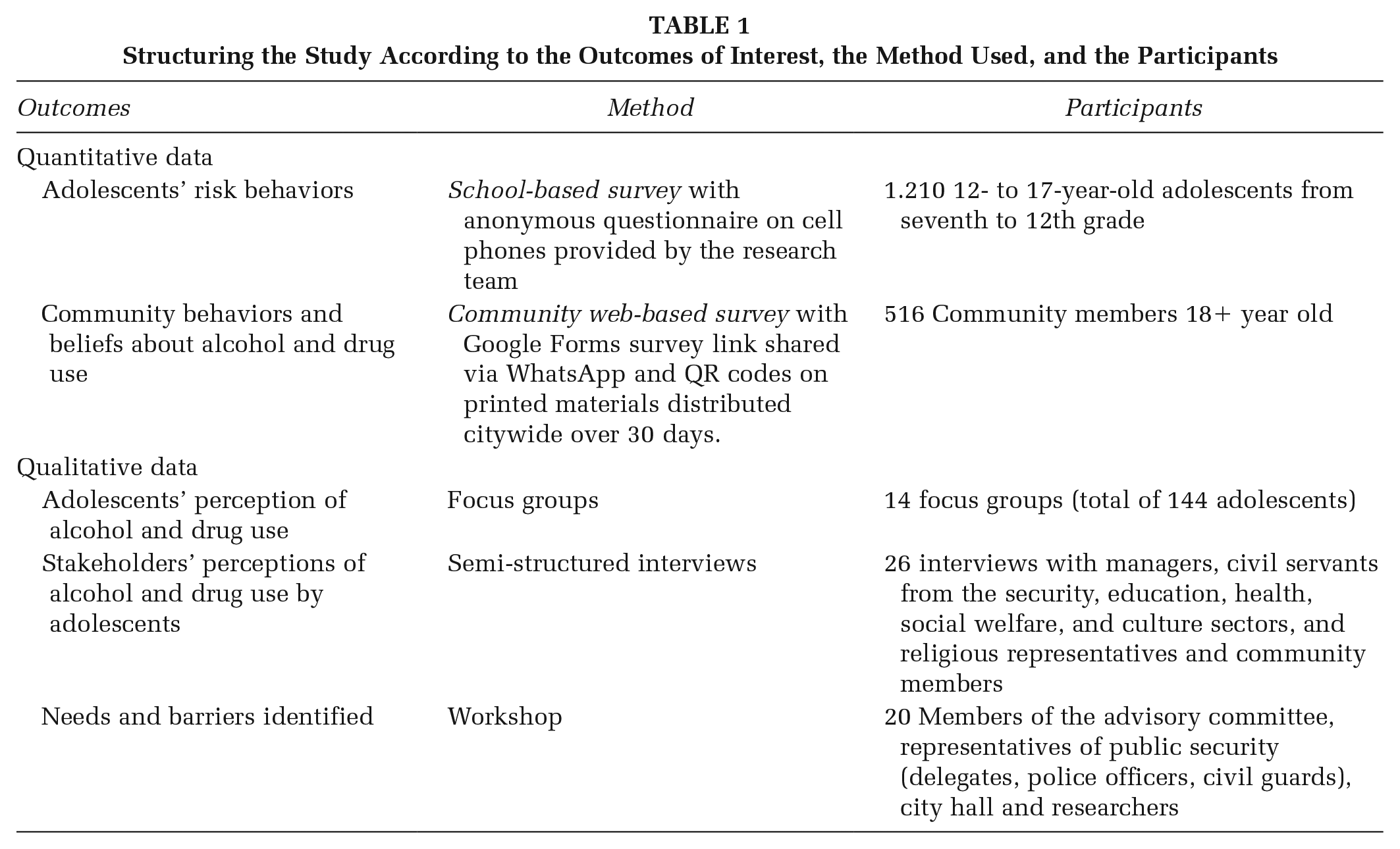
Following Phase 1 of the WHO IRC, the study established an advisory stakeholder committee, conducted a situational analysis, organized knowledge synthesis workshops on evidence-based interventions, and identified strategies to address local barriers. The situational analysis utilized five data sources: school-based survey, focus groups with adolescents, semi-structured stakeholder interviews, community web-based survey, and knowledge synthesis workshops (Table 1). Data were collected from November 2023 to April 2024.
Structuring the Study According to the Outcomes of Interest, the Method Used, and the Participants
Prior to data collection, informed consent was obtained from parents or legal guardians, and assent was secured from adolescents on the day of the survey. These procedures adhered to ethical standards required for research involving minors. The project was approved by the Research Ethics Committee of the Universidade Federal de São Paulo (approval number: 6.598.311).
Quantitative Data
Study Sample and Data Collection
School-based survey
A total of 1,745 students enrolled in seventh to 12th grade across four schools were invited to participate in the Prev.Action survey. The municipality has only five schools—three public and two private. The selection aimed to include all of them: participation from public schools was secured through a formal request issued by the Municipal Department of Education. Private schools were invited directly by the research team, but one declined to participate. Each student was provided with a mobile phone to complete the anonymous questionnaire in the classroom, without the presence of a teacher. Of those invited, 1,335 students completed the survey, resulting in a participation rate of 76.5%. Nonparticipation was due to student absences, refusal to participate, or lack of parental or guardian consent. Since the study focused on underage drinking, students above the age of 18 were excluded. The final sample included 1,210 adolescents aged 12 to 17.
Community web-based survey
The community survey was structured using Google Forms, and the access link was widely publicized and shared via WhatsApp by residents and through printed materials containing QR codes distributed throughout the city over 30 days. Residents and individuals working in the city aged 18 and above were invited to participate. A total of 516 residents or workers in the city participated in the survey.
Instruments and Variables
The school-based survey was adapted from widely used Brazilian instruments, assessing:
Substance Use: Lifetime, past-year, and past-month use of alcohol, tobacco, e-cigarettes, and other drugs (e.g., Did you drink alcohol in the past year?; response options: yes/no); binge drinking (e.g., In the past month, did you consume five or more alcoholic drinks on a single occasion?; response options: yes/no); and ways of accessing alcohol were collected (e.g., How do you usually obtain alcoholic beverages?; response options: purchase, with parents, with friends, etc.; Galvão et al., 2021). Location of alcohol consumption (e.g., What are the main places where young people in your city consume alcohol and other drugs?), parental alcohol and drug use (e.g., Do your parents or guardians drink beer, wine, or spirits?; response options: yes/no), and parental reaction to an intoxicated child (e.g., Suppose you came home drunk one night. How would your parents or guardians react?; response options: my parents would get mad, my parents would hit me, my parents would ignore me) were assessed using the Prevention of Alcohol Use Students (PAS) study instrument (Koning et al., 2009).
Community and Social Context: Perceived substance availability (e.g., If you wanted to use a drug, how easy would it be for you to get it?; response options: easy, moderate, difficult), community characteristics, and engagement (assessed via the Communities That Care Youth Survey, CTCYS; Arthur et al., 2002).
Socioeconomic status (SES): Students’ socioeconomic class was assessed using the scale of the Brazilian Association of Research Companies (ABEP), which varies from 1 to 100 points and considers the education level of the head of the household and the goods and services used, with categories ranging from A (highest) to D/E (lowest; Associação Brasileira de Empresas de Pesquisa [ABEP], 2021).
The community survey assessed sociodemographics (gender, race, age, education, income), normative beliefs about adolescent alcohol use using the Alcohol Use Norms Scale (Koning et al., 2021), perceived substance availability (CTCYS; Arthur et al., 2002), and barriers to intervention implementation (e.g., What are the main barriers to implementing alcohol and drug prevention initiatives, considering the reality of the municipality?).
Statistical Analysis
A descriptive analysis of all variables collected via the adolescent school-based survey was conducted. Categorical variables were summarized as percentages and absolute numbers, while numerical variables were presented using means and standard deviations.
Qualitative Data
Study Sample
The study involved 144 adolescents from the survey, recruited for focus groups based on school management recommendations to ensure diversity in gender, age, SES, and alcohol use experience. For the semi-structured interviews, 26 key stakeholders were involved, including managers, public officials from the sectors of security, education, health, social assistance, and culture, as well as religious representatives and community members. Initially, advisory stakeholder committee members, previously invited by the city hall, participated voluntarily in the interviews. Others were recruited through snowball sampling when participants nominated additional community members.
Data Collection, Instruments, and Variables
Focus Groups: Fourteen ~40-minute focus groups, each with 10 adolescents, addressing alcohol and drug consumption patterns, access to alcohol, law enforcement, and family, peer, and community influences were conducted.
Stakeholder Interviews: Twenty-six interviews (~50 minutes each) were guided by a semi-structured script similar to the adolescent focus groups, with added topics on barriers to implementation.
All statements were audio-recorded, and a field diary was used to register noteworthy situations.
Knowledge Synthesis Workshops on Potential Evidence-Based Interventions
Three 5-hour workshops were held with ~20 advisory committee members to review the findings, discuss evidence-based prevention programs, identify barriers, and co-create strategies for implementing multicomponent interventions. Activities included problem identification, reviewing proven programs, and proposing localized actions. The groups’ presentations were audio recorded in all activities, and poster presentations were photographed.
Data Analysis
All audio recordings were transcribed using Whisper AI and reviewed for accuracy. Data were analyzed using Thematic Analysis (Braun & Clarke, 2021), with categories constructed deductively from the semi-structured guide (Bingham & Witkowsky, 2021). Five researchers conducted floating readings, created codes, and grouped them into broader categories. Final categories addressed adolescent alcohol consumption patterns, access, beliefs, enforcement actions, family roles, solutions, barriers, and implementation strategies. Participant statements were anonymized with identification codes (e.g., STK01 for stakeholders; FG01, focus groups; W1, workshops).
We applied a triangulation approach to ensure the robustness of our findings (Patton, 2002). We used data source, methodological, and investigator triangulation (Supplemental Table S1). This triangulation approach improves our study’s reliability, validity, and overall quality, ensuring a more accurate understanding of the community’s needs. However, some themes in this study are presented using only qualitative data due to the unavailability of corresponding quantitative measures. This is the case for the section on Law Enforcement and Alcohol Sales, for which no quantitative data were collected.
Results
Characterization of Participants
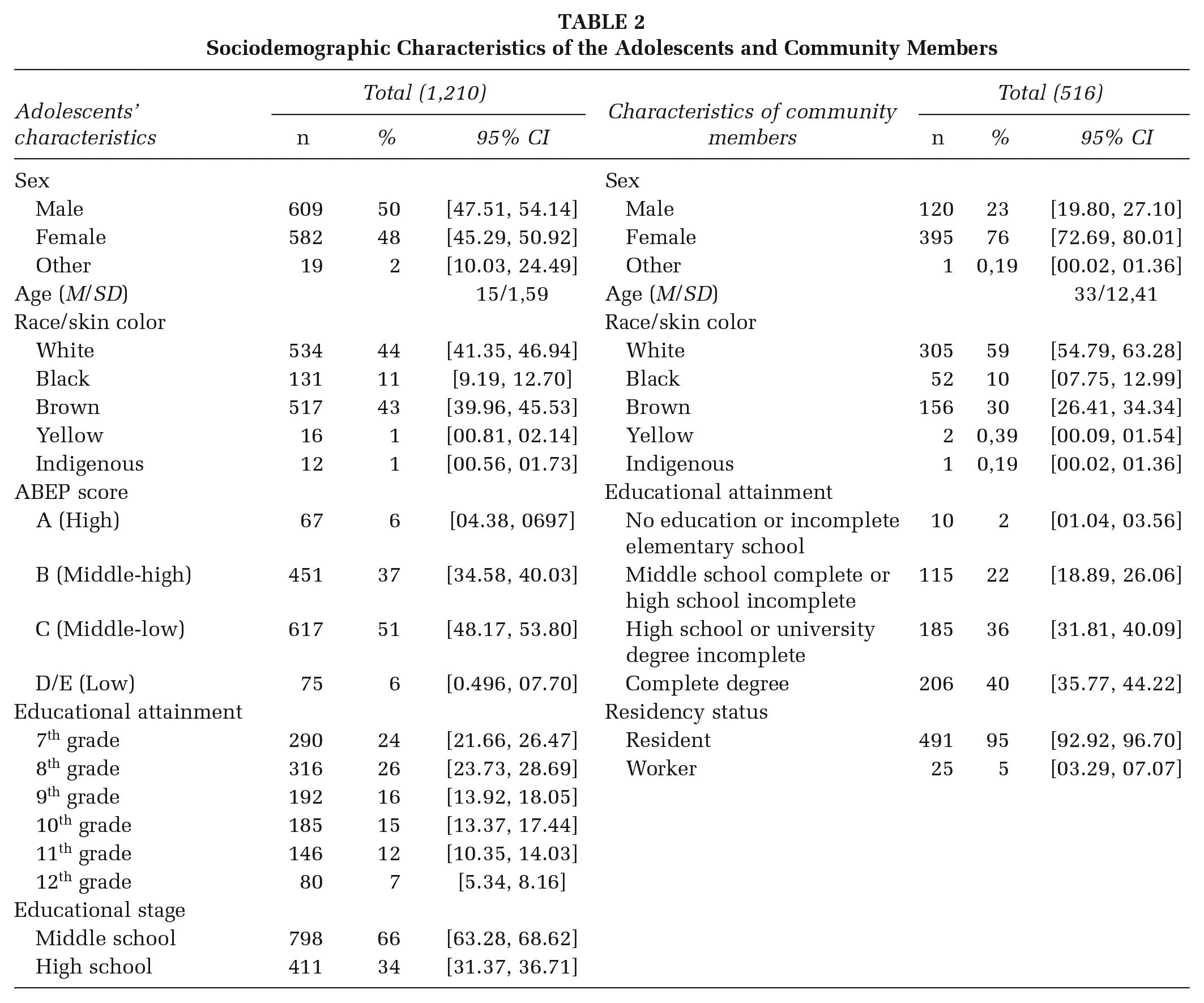
Most adolescents from the school-based survey were enrolled in middle school (66%), with 8th-grade students representing the largest group (36%). The average age was 15 years, and the sample was well distributed in terms of gender. In addition, 44% declared themselves white, and 51% belonged to lower-middle SES. Among the community members from the community web-based survey, the majority were female (76%), white (59%), had completed a degree (40%), and lived in the municipality (95%). The average age was 33 (Table 2).
Sociodemographic Characteristics of the Adolescents and Community Members
Consumption Patterns
The majority of students reported lifetime alcohol use (60%), with 54% among middle school students and 73% among high school students. The average age of first alcohol use was 13 years; 13% reported binge drinking in the past 30 days. Lifetime use of e-cigarettes was 25% in middle school and 33% in high school, while cannabis use was 10% and 19%, respectively (Table 3).
Student Drug Use (Lifetime, Past Year, Past Month) and Current Alcohol Consumption Patterns
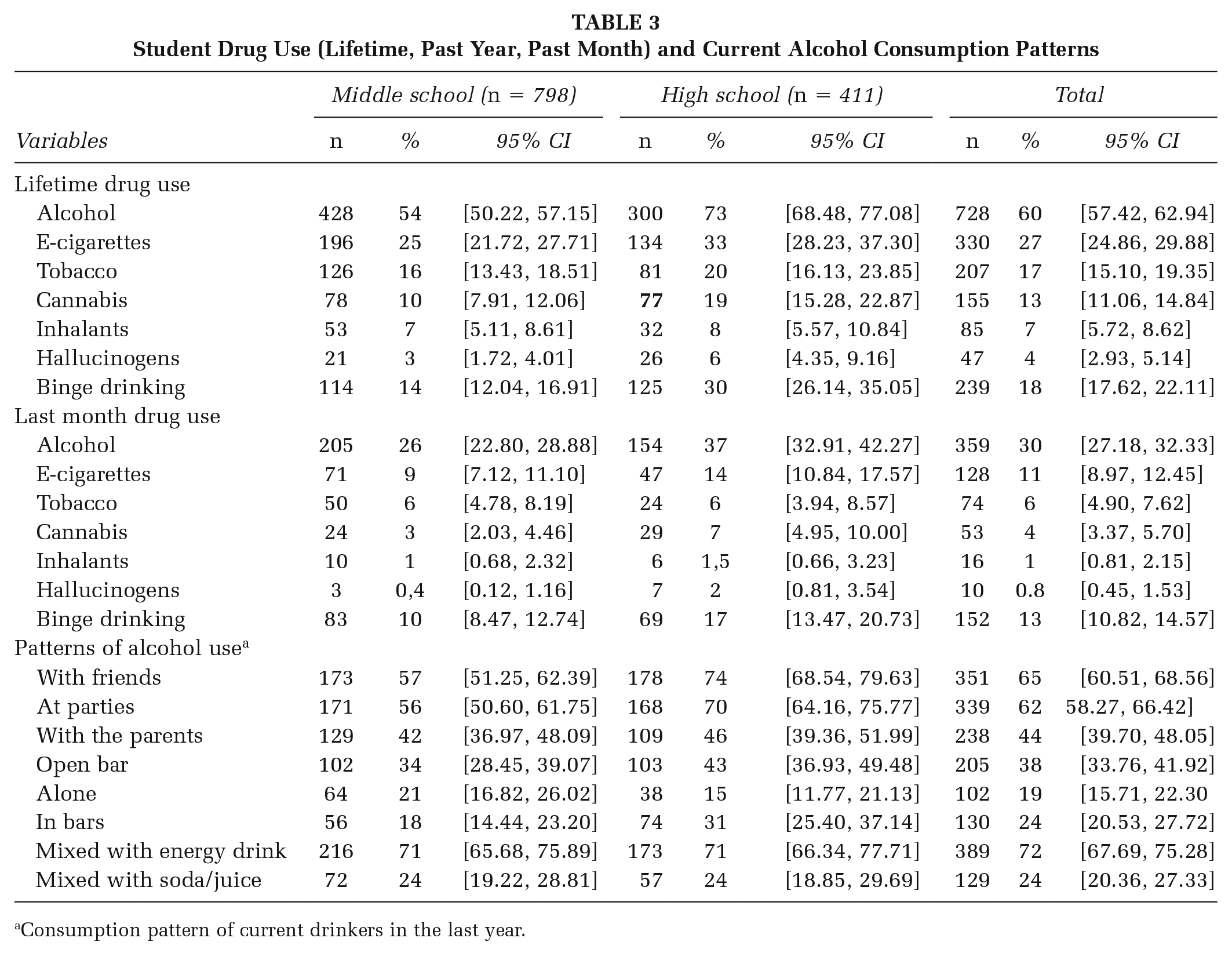
Consumption pattern of current drinkers in the last year.
The information cited above is detailed by data from interviews and focus groups with participants, who highlighted that consumption in the municipality is considered high.
I see that today in the city [alcohol consumption] is very serious. From my point of view, I find the issue of the use of alcohol and other drugs by adolescents to be serious and worrying. (STK01)
Alcohol Access
Regarding access to alcohol, it was found that self-purchasing and receiving alcohol from parents were the main ways of acquisition among adolescents. In middle school, 30% of students reported acquiring alcohol through self-purchase and 40% by receiving it from their parents, while in high school, these percentages were 49% and 34%, respectively. Students perceived alcohol as the most accessible substance (67%; Figure 1). Data from the community web-based survey are also aligned with this issue, as 76% reported that it is very easy for an adolescent to access alcohol.
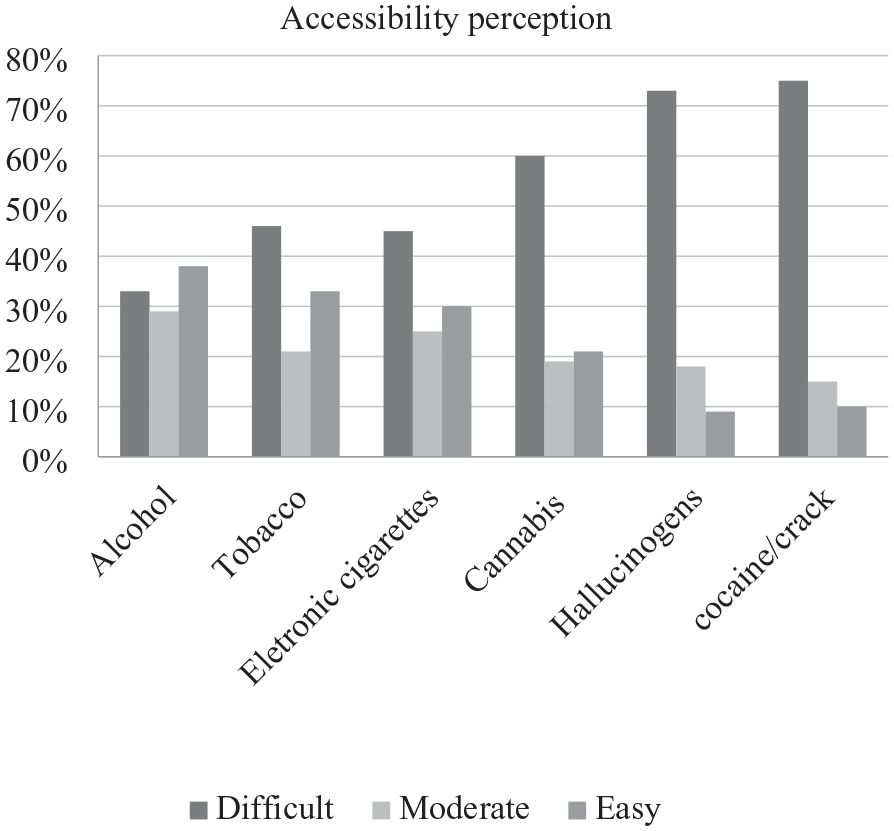
Adolescents’ Perception of Accessibility to Drugs
In interviews and focus groups, many participants noted adolescents obtain alcohol through establishments, family, friends, or at home:
There are always older friends who go there and buy and give it to them. (STK14) Even in their own home, with their parents who have the drink on display, even decorating their home. (STK16)
Normative Beliefs and Alcoholic Culture
The community largely disapproved of underage drinking (81%), yet 42% of middle schoolers and 46% of high schoolers reported drinking with parental permission (Table 3). Peer pressure and social norms were key influences:
To belong and to be accepted in the group, you have to drink. (STK20; FG07)
Participants also highlighted the normalization of underage drinking:
At the same time that the population sees it as a problem, it accepts consumption among young people. (STK22) I think many people normalize, even the authorities. (STK12)
The participants pointed out that drinking is generally associated with a way to cope with emotional, personal, and family problems.
. . . [it is motivated] mainly by the issue of problems, because the person always tries to do something to escape the problems, so the person ends up consuming alcohol. (FG07)
It is worth noting that, from the stakeholders’ perspective, certain elements, such as participation in extracurricular activities and religious practice, may serve a protective role.
And I think it is always terrific . . . because most [sports or leisure] activities will encourage them not to consume alcohol or other substances. (STK11) Religiosity can help many people. I believe that those young people who are in church, whatever their religion, are less likely to get involved with alcohol and drugs. (STK13)
Law Enforcement and Alcohol Sales
Participants highlighted that inadequate enforcement and fragmented laws could facilitate adolescents’ access to alcoholic beverages. Reports indicate that while some establishments commonly require identification, wineries and bars are less strict about verifying age.
[They buy alcoholic beverages] in bars, pubs, wineries, places like that. (STK12) It depends on the establishment. At the supermarket, they ask for [the identity document]. (FG03)
Adolescents report that, although there is a consistent police presence in the city to enforce the law, police actions aimed at preventing adolescent alcohol consumption are perceived as ineffective and not prioritized. However, stakeholders expressed significant concern about law enforcement and monitoring of alcohol consumption.
For example, sometimes police officers waste time on less relevant things. . . they give more importance to something that no one cares about and end up not paying as much attention to what matters, like adolescents drinking in the square. (FG10) I believe there is a big concern because there is always supervision and policing. For example if an adolescent wants to buy drinks, someone will always be supervising; supervision is very serious. (STK21)
Role of the Family in Alcohol Consumption
Families played a dual role in adolescent alcohol use. Although 95% of the community viewed families as protective, adolescents reported permissive behaviors such as parents allowing drinking at home (12% middle school, 33% high school). Participants emphasized family influence:
They often say “look now my son is 14 years old, he is going to have a beer with me.” (STK15) There are parents who prefer their children to drink in front of them rather than in secret or with other people. (FG08)
Others highlighted family members modeling drinking behaviors, which could either discourage or encourage alcohol use:
I guess it depends. If you see your father being an addict, you probably will not want to get involved with it. However, if you are in an environment where drinking is more liberated, and people do not seem addicted, you might want to try it. (FG06)
Proposed Solutions for Alcohol Prevention
Stakeholders identified major issues, including alcohol availability, cultural normalization, and family influence. Suggested strategies included enhancing parenting skills, school prevention programs, stricter enforcement, and community engagement:
One of the problems is the easy access to alcohol and other drugs, in addition to the naturalization and consent of the family regarding consumption among adolescents. (W1)
Barriers included a lack of professional training and political support, with solutions proposed:
Our biggest difficulty is teacher training. One strategy to deal with this difficulty is to request a hybrid or completely online format . . . (W2)
During the discussion on environmental actions for the municipality, stakeholders proposed strategies such as disseminating informational materials through various media outlets, organizing workshops for adolescents, and training merchants to verify the age of buyers. They also suggested establishing a municipal protocol for events, incorporating wristbands to identify adolescents, thus facilitating enforcement and preventing the sale of alcohol to minors.
We will focus on disseminating materials (posters, videos) through social media, the platforms most accessed by adolescents. We will also use schools, radio, podcasts, and workshops to engage young people and disseminate information. (W3)
Deliberative Actions From Workshops
The workshop deliberations resulted in a multicomponent intervention plan with three arms, including the only evidence-based prevention programs with proven effectiveness among the Brazilian population:
School Programs: #TamoJunto 2.0 (Brazilian version of Unplugged for adolescents aged 12 to 14) and Elos (Good Behavior Game for children aged 8 to 10).
Family Programs: Famílias Fortes program (Strengthening Families) in social assistance or health settings.
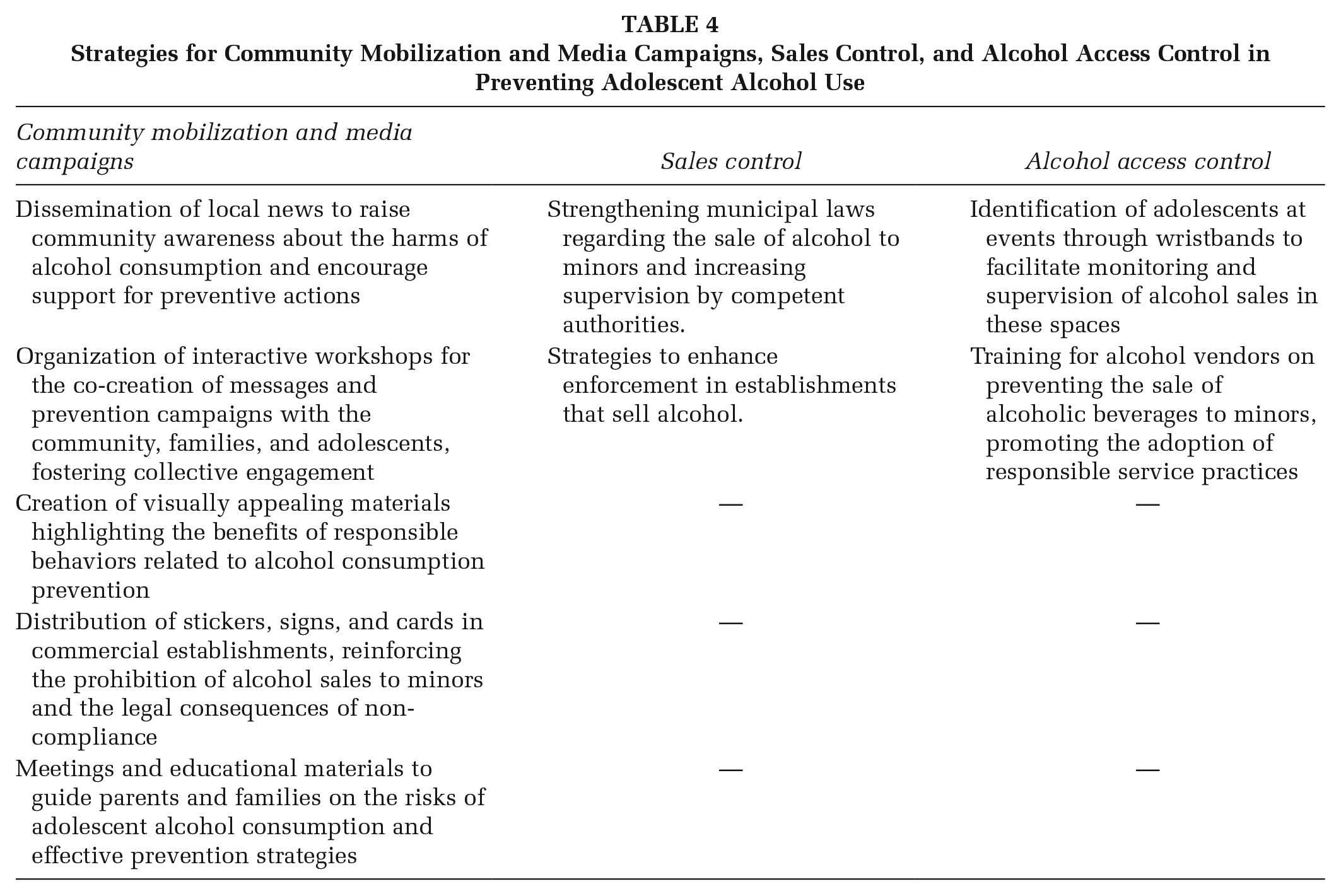
Environmental Strategies: Community Mobilization and Media Campaigns, stricter sales enforcement, and alcohol access control (Table 4).
Strategies for Community Mobilization and Media Campaigns, Sales Control, and Alcohol Access Control in Preventing Adolescent Alcohol Use
Discussion
This article describes the first phase of the Prev.Action study, which began with a situational analysis and knowledge synthesis involving a whole city. By identifying key issues such as the prevalence of drug consumption, ways of accessing alcohol, cultural normalization of consumption, and family and peer influence as the most important and changing mechanisms that can influence the onset of adolescent drinking, it was possible to focus precisely on priority areas for intervention, such as school programs, family programs, and environmental strategies.
The study revealed that 60% of the students had tried alcohol throughout their lives. Surveys carried out at the national level in Brazil, such as the Brazilian Study of Cardiovascular Risks in Adolescents (ERICA), indicate that the prevalence of alcohol consumption ranged from 35.3% (Ferreira et al., 2019) to 63.3% according to the National School Health Survey (PeNSE; IBGE, 2022). In a global trend analysis that included more than 135,000 adolescents aged 12 to 15 in 22 countries, it was observed that 14.1% reported having consumed alcohol (Smith et al., 2024). In this study, 13% of adolescents reported having consumed excessive alcohol in the last 30 days, while PeNSE (IBGE, 2022) indicated that 6.9% reported excessive alcohol consumption in the previous month. Despite the relatively modest sample size, specific factors may be increasing the risk of alcohol consumption among the adolescents studied, underlining the importance of targeted community interventions. These results indicate that there is a local need for preventive interventions to reduce alcohol consumption.
The present article reveals that the Cordeirópolis community views alcohol consumption as a normalized practice, a phenomenon widely corroborated by the literature, which highlights the permissiveness of alcohol consumption by adolescents (Jones et al., 2017; Rowland et al., 2018). This normalization may be one of the main factors behind adolescent drinking (Prabhughate et al., 2020), especially when this perception is reinforced by peer acceptance (Buvik et al., 2022). A study covering data from 36 countries revealed that in contexts where drinking is seen as normal, adolescents are less likely to identify the risks associated with this practice (Sznitman et al., 2013). Cultural attitudes that treat alcohol consumption as a social norm constitute significant barriers to changing perceptions about alcohol use in the community. Therefore, it is essential to implement practical actions aimed at changing these perceptions to promote broad community support for prevention policies (McLeroy et al., 1988; Perry et al., 2002) since reducing the normalization of alcohol use among adolescents can contribute to reducing binge drinking in this group (Ball et al., 2020; Scheffels et al., 2020).
Data from this research highlights how the family context emerges as both a risk and protective factor in alcohol consumption among adolescents. Social and family perspectives on alcohol consumption directly influence how adolescents interpret the possibility of substance use (Rowland et al., 2018; Rowland, Kremer, et al., 2022). Although 95% of the Cordeirópolis community believes that families should play a protective role, the study also shows that a significant proportion of adolescents were allowed to drink by their parents. Longitudinal analyses show that giving alcohol to children increases the risk of problems and excessive consumption among adolescents (Clare et al., 2020). In addition, adolescents in our study reported that their parents get drunk frequently (20%). These data also reinforce the need for family and community interventions that address changes in attitudes and behaviors concerning alcohol since parents who drink abusively may have a decreased ability to monitor their children, increasing the risk of alcohol consumption among adolescents (Valente et al., 2024).
To change social norms about adolescents’ alcohol consumption, the use of communication and media is a widely employed strategy to direct or amplify public health messages (Casswell et al., 1989). These efforts aim to shift communities’ alcohol beliefs by challenging and modifying the cultural acceptance of alcohol. Specifically for alcohol use, environmental interventions that use informational messages as prevention strategies are often used in community-based studies (Holder et al., 1997; Perry et al., 1993; Rowland et al., 2013; Treno et al., 2007; Wagenaar et al., 2000). Given the context of Cordeirópolis, it is necessary to offer new paths for engagement and education in alcohol use prevention. Social marketing through Community Mobilization can be an avenue that plays a fundamental role in establishing informative and warning messages and seeking greater possibilities for behavior change concerning norms, laws, and perspectives on the harms of alcohol consumption (Flynn et al., 2006; Holder, 2000; Treno & Holder, 1997).
Accessibility to alcohol emerged as one of the most challenging mechanisms that influence adolescents’ alcohol consumption, with self-purchasing being one of the most prevalent methods through which adolescents obtain alcohol. In addition, the enforcement of laws and policies in Cordeirópolis is reported as inconsistent. Expanding or enforcing measures aimed at preventing alcohol consumption by minors is widely used through targeted environmental actions (Duch et al., 2020; Grube, 1997; Wagenaar et al., 2006). This approach would significantly contribute to limiting the access or consumption of alcohol by adolescents in the municipality. Furthermore, evidence of gaps in the enforcement of legal restrictions on alcohol consumption by adolescents also stands out, showing the presence of establishments that are less rigorous in age verification and frequently provide alcohol to adolescents. This type of behavior by beverage merchants is not exclusive to this study; many prevention projects over time are designed to make this behavior less frequent, limiting adolescents’ access to alcohol (Flewelling et al., 2013; Rehnman et al., 2005; Rowland et al., 2018). Strategies such as Rewards & Reminders, which involve visits to alcohol sales establishments to test identity verification, effectively promote Responsible Beverage Services. In the case of compliance with the laws, the employees are congratulated; in the case of a sale to a decoy, the employee is reminded of the laws prohibiting sales to minors (Moore et al., 2012; Rowland et al., 2013; Van Ryzin et al., 2019).
Other studies have also carried out a situational analysis to identify local specificities (Koning et al., 2021; Rowland, Kelly, et al., 2022; Suiter, 2017), and this phase of Prev.Action managed to identify the demands and needs of the local community regarding adolescent alcohol prevention. This allowed the high level of community involvement and the personalized approach to dealing with cultural norms to help us develop strategies with the community to increase the chances of effectively achieving the expected results. In this sense, this first phase of the study was important for guiding the initial development of a multicomponent prevention intervention designed to operate synergistically, in which each component strengthens the others, potentially maximizing the impact of the actions to be implemented.
The knowledge synthesis from workshop deliberations resulted in the definition of a multicomponent community intervention with three arms: school programs, family programs, and environmental strategies. Integrating programs with positive evidence in Brazil into our study will be a differential: Elos and #Tamojunto 2.0 (school programs) and Famílias Fortes (family involvement). The Elos program, aimed at children aged 6 to 10, promoted modest/robust improvements in children’s pro-social skills and concentration and decreased disruptive behavior (Caetano et al., 2024). #Tamojunto 2.0, aimed at adolescents aged 12 to 14, showed that students exposed to the program were less likely to start using alcohol (Sanchez et al., 2021), in addition to being indirectly effective in preventing bullying and increasing knowledge about normative beliefs regarding alcohol and drug use (Garcia-Cerde et al., 2023). Famílias Fortes, aimed at families with adolescents aged 10 to 14, reduced the chance of parents and legal guardians being classified as negligent by 60%, increased caregivers’ use of nonviolent discipline, and decreased the chance of adults exposing adolescents to their episodes of drunkenness by 80% (Sanchez et al., 2024).
The planning of environmental strategies is also integrated into our study, such as Community Mobilization, which involves organizing community coalitions and local working groups to develop alcohol prevention activities, investing in public awareness focused on problems related to alcohol consumption by adolescents, and engaging the community in the implementation of interventions. In addition, Alcohol Sales Control can involve restrictions on sale hours and warnings to establishments that facilitate access to alcohol for minors (Holder et al., 1997).
The Prev.Action implementation phase faces challenges, including limited resources, political instability, and a need for ongoing professional training. These barriers align with findings from implementation research (Belizan et al., 2019; Mootz et al., 2022). Therefore, ensuring the continuity of these programs despite changes in government or local management is essential for their sustainability (Cannon et al., 2019; Cooper et al., 2021).
This study had several limitations, including potential biases in self-reported data. The sample size and the specific sociocultural context of the study location may also limit the generalizability of the results. In addition, the fact that it is a study involving a community intervention that was widely publicized in the local context may have slightly biased the participants’ responses regarding alcohol consumption and other factors. Future research should address these limitations by employing more diverse samples and expanding the study setting. We suggest that conducting a longitudinal assessment of these indicators is fundamental.
Despite these limitations, the study presents key strengths and novel contributions. It corresponds to the first phase of a broader implementation science initiative—the Prev.Action study—designed to reduce adolescent alcohol use through a co-produced, multicomponent, and community-based approach. The use of mixed methods and multiple triangulation strategies (data source, methodological, and investigator) enhanced the reliability and depth of the situational analysis. Importantly, the study engaged local stakeholders throughout the research process, fostering co-ownership and ensuring that proposed strategies were context-sensitive and feasible. These elements contribute valuable knowledge to the field by illustrating how participatory, implementation-oriented frameworks can be operationalized in small municipalities. The insights gained not only inform the subsequent phases of the Prev.Action study but also offer practical guidance for scaling similar interventions in low- and middle-income settings
Implications for Practice
Mixed-methods approaches were critical to tailoring the intervention to the local context, as outlined in the first phase of the WHO IRC. For example, combining qualitative insights with survey data allowed us to identify priority areas for action and co-develop community-informed strategies. Practical adaptations, such as distributing QR codes in public spaces, proved effective in overcoming barriers to data collection and engaging hard-to-reach populations. These findings reinforce the value of context-specific and adaptive public health interventions.
Beyond practice, our results carry implications for policy and research. Policymakers should consider supporting multicomponent prevention strategies that integrate school, family, and environmental components and that are co-produced with local stakeholders. For researchers, the study underscores the need to further investigate implementation processes in small municipalities, including how community engagement and intersectoral coordination affect sustainability and scalability.
Conclusion
The situational analysis revealed significant gaps in alcohol control, with social permissiveness, peer pressure, and weak enforcement facilitating consumption. Interventions targeting access, cultural norms, and family dynamics are vital to reducing adolescent alcohol use. These findings offer a framework for addressing local challenges and developing sustainable, community-based public health strategies.
Supplemental Material
sj-docx-1-hpp-10.1177_15248399251366355 – Supplemental material for Situational Analysis and Planning of a Community-Based Multicomponent Intervention to Prevent Adolescent Alcohol Use: The Prev.Action Study
Supplemental material, sj-docx-1-hpp-10.1177_15248399251366355 for Situational Analysis and Planning of a Community-Based Multicomponent Intervention to Prevent Adolescent Alcohol Use: The Prev.Action Study by Luís Eduardo Soares-Santos, Matheus de Carlos Silva Oliveira, Marília M. Mendes-Sousa, Sheila C. Caetano, Juliana Y. Valente and Zila M. Sanchez in Health Promotion Practice
Footnotes
Authors’ Note:
All the individuals who participated in this study and the community of Cordeirópolis. This study was supported by grants nº 2022/03145-9 (ZMS), nº 2023/16702-6 (LESS, Ph.D), nº 2024/05810-5 (MMMS) and nº 2023/14565-1 (MCSO), São Paulo Research Foundation (FAPESP). The opinions, hypotheses and conclusions or recommendations expressed in this material are the responsibility of the author(s) and do not necessarily reflect the views of FAPESP.
Author Contributions
LES-S was responsible for designing the study, collecting and analyzing the data and writing the first version of the manuscript. MCSO and MMM-S collected the data, worked in data analysis and revised the manuscript. SCC and JYV contributed to designing the study, interpreting data and revising the manuscript. ZMS is the PI responsible for the grant, conceived and designed the study, supervised data collection and analysis, and approved the final version of the manuscript. All the authors approved the final version of the text.
Ethics Approval and Consent to Participate
The Research Ethics Committee approved the study protocol of the Universidade Federal de São Paulo (# 6.598.311).
ORCID iDs
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.