
Abstract
This article discusses the importance of building community capacity through collaborative partnerships, especially in rural areas. Community Health Organization Improving Care and Equity (CHOICE) is an accountable community of health piloting the Improving Senior Healthcare Access in Rural Environments (I-SHARE) program. I-SHARE’s goal, to improve health for rural older adults (aged 65 years and older) by increasing their ability to access primary care in-person and through telehealth, led to the collaboration between CHOICE, a federally qualified health center, a community-based organization, and the regional library system. This collaboration strengthened community capacity by more effectively utilizing limited resources, increasing program visibility and reach, and providing a template for future partnerships, all of which are especially important in resource-scarce rural areas. The organizations’ differing backgrounds and expertise enriched the program’s creation and implementation while the strength of the partnership and the organizations’ commitment to serving area older adults propelled the team when faced with implementation barriers. Lessons learned in collaboration include working within recognized social networks and establishing commonalities in shared values and foundational knowledge. Building collaborative partnerships is a vital practice in rural areas to maximize resource utilization and deepen trust between community members and service providers.
Assessment of Need
America is aging. Between 2010 and 2020, the older adult population, aged 65 years and older, grew by 38% compared with a 2% increase for the rest of the population combined (Administration for Community Living, 2022). This is especially visible in rural areas where older adults comprise 19% of the population versus 15% in urban areas (Harrington et al., 2020). Rural residents experience higher rates of mortality and chronic disease, such as heart disease and diabetes, than urban residents, as well as greater health professional shortages and decreased access to care (Harrington et al., 2020). Older adults, likewise, are at higher risk for experiencing one or more chronic conditions, and 32.6% of older adults have a disability versus 13.6% of the total population (Harrington et al., 2020; United States Census Bureau, 2023). Therefore, rural older adults have more health care needs and less access, putting them at greater risk for poor health outcomes. Robust community-based interventions are needed to protect the health of rural older adults; however, rural areas often have limited resources and capacity (Harrington et al., 2020).
Description of Innovation
Community Health Organization Improving Care and Equity (CHOICE, n.d.) is an accountable community of health (ACH) encompassing a seven-county region in central western Washington state, with a mission to help all residents thrive. Based on a comprehensive needs assessment that included key informant interviews with older adults and community agencies that support older adults, CHOICE identified a need to better support this population in accessing care. This led to the creation of the Improving Senior Healthcare Access in Rural Environments (I-SHARE) program. I-SHARE’s goal is to improve health for rural older adults by increasing their ability to access primary care in-person and online. The I-SHARE pilot partners CHOICE with a federally qualified health center (FQHC), a community-based organization (CBO), and a regional library system, in one CHOICE county. See Figure 1 for partnership details.
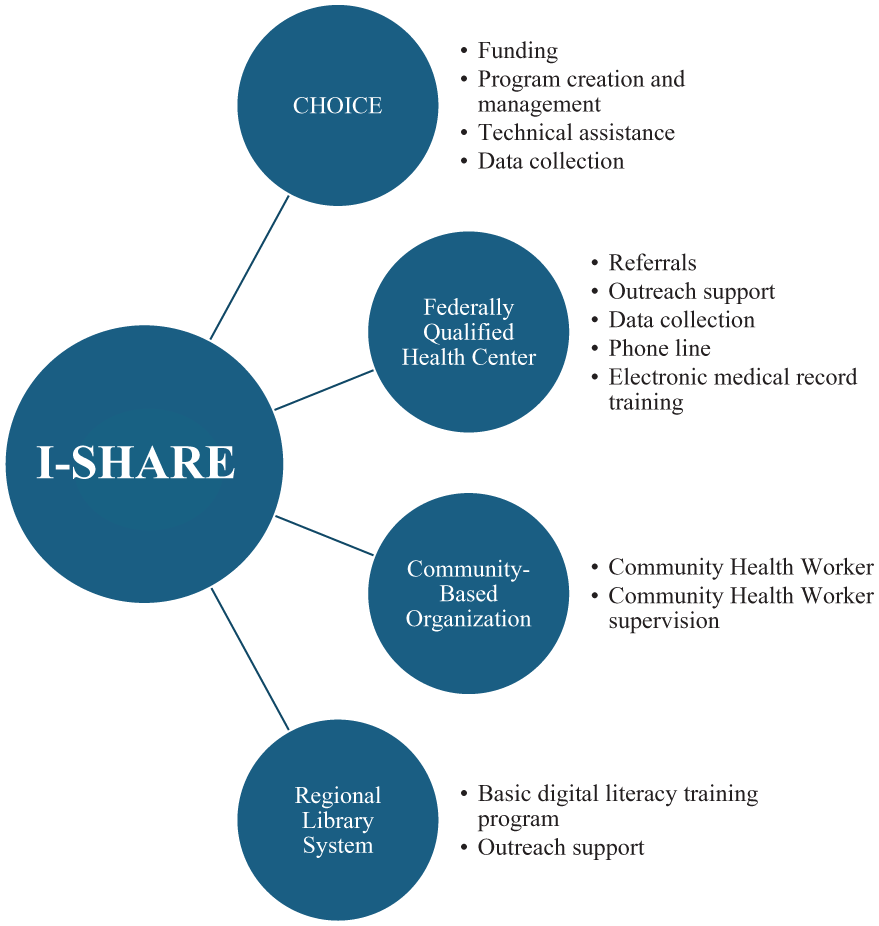
I-SHARE Program Partners and Their Roles
I-SHARE is a twofold strategy in which a community health worker (CHW) from the partner CBO receives referrals from the FQHC and connects patients to resources promoting in-person care access such as third-party transportation and insurance navigation. Online access to care is supported through one-on-one digital training. The CHW provides basic digital training through an online library resource, and telehealth training on the FQHC’s specific patient portal and telehealth appointment platforms. CHOICE’s initial investment of $175,000 supports one full-time equivalent CHW position, CHW supervision, electronic devices for program participants, CHW travel, provides technical assistance and training to program staff, along with CHOICE’s administrative costs for 1 year.
Impact
Currently in its pilot phase, I-SHARE’s creation allows for renewed alignment between the partner organizations, which had limited previous interactions, and increases funding in a resource-scarce environment. Synergistic cooperation supports the sharing of resources and knowledge, expanding the project’s reach and capacity without duplicating services. This intercollaborative approach demonstrates the importance of regional collaboration and shared investment in rural areas, and is foundational to increasing community capacity and sustainability of services regarding older adults’ access to care.
I-SHARE’s alignment of four different types of organizations toward a common goal increases the program’s visibility among their unique audiences. In addition, the partnership enables outreach efforts to extend beyond the typical clinical footprint. Leveraging shared resources, that is, utilization of a digital literacy program provided by the regional library, allows staff to reallocate their time and efforts, increasing program capacity.
I-SHARE also increases the visibility of older adults as a population within the community. Presenting the partner organizations with county-specific data on older adult health disparities brings the issue into greater focus and gives a new platform for advocacy within their networks and throughout the county.
Successes and Challenges
Program buy-in was gained from each partner by presenting quantitative and qualitative data concerning health outcomes of the region’s older adult population. The strength of this buy-in supported the partnership when confronted with implementation challenges. Each organization brought a nuanced understanding of their communities, constructing a rich context from which the program could be created. CHOICE’s experience administering a regional CHW network also lent valuable expertise in developing the programmatic structure. Providing electronic devices to participants in need increased older adults’ ability to access digital care.
Challenges also arose. Two organizations utilized different electronic health record systems necessitating additional training and technical assistance to ensure partners’ needs were met. Each organization had different operational experiences with CHW programs which required the establishment of standard protocols, while staff turnover led to the loss of program champions which affected progress. Broadband limitations in certain areas, despite use of a hotspot, created barriers to training and access.
Lessons Learned
Assessing adjacent sectors to identify potential collaborating organizations may increase resources, capacity, and approaches. Finding commonalities in organizational missions, and leveraging shared values and existing relationships, can lead to greater community buy-in. Harnessing informal networks can also effectively establish partnerships in rural communities.
During the initial phases of collaboration, time should be taken to ensure consistency of partners’ understanding and expectations for the project. When feasible, establish early successes that build momentum. Begin with simple activities and increase in complexity as understanding of the program evolves. Flexibility and willingness to consider suggestions are essential.
When more than one documentation platform may be in use, consider each partner’s documentation needs versus their wants. Also, ensure that partners understand the scope of practice for the CHW or staff completing the documentation. Depending on the position’s requirements, some staff may not have had the training necessary for certain types of documentation.
Implications for Practice
Promoting collaboration across health care and community sectors continues to be vital to improving population health (McClellan et al., 2025). Not only are patients better supported in clinical spaces, but also in their communities where they spend most of their time. As workforce capacity and resources become scarcer in the face of escalating needs, building community capacity and collaboration also allows for better human and nonhuman resource management and allocation. It promotes the broadening of perspectives, teaches individuals to share their lived experiences to better advocate for their needs, and deepens trust between community members and service providers.
Footnotes
Authors’ Note:
Authors S. Joyce Heck and Katherine Willet are employed by CHOICE, the funding organization. Author Daniel Hannawalt-Morales was employed by CHOICE at the time of project implementation, but is currently employed at Kaiser Permanente, This program was funded by CHOICE.