
Abstract
Barriers to behavioral health care, increasing deaths by suicide, and provider shortages represent critical global public health challenges. The World Health Organization (WHO) calls for upstream mental health strategies that go beyond clinical approaches; however, culturally responsive, community-engaged mental health promotion efforts remain limited in the United States. This research brief presents evaluation results of Mental Health Matters of Washington’s Peer Mental Health Navigator (PMHN) program, which trains lay community members to provide peer mental health support, education, and resource navigation. Researchers used a non-controlled pre- and post-design with a 12-month follow-up survey across seven cohorts of Spanish and English-speaking peer navigators (n = 141) over 3 years. The 6-week bilingual training applied socio-ecological and critical theory frameworks to address mental health holistically, covering stigma, systemic factors, cultural perspectives, communication skills, stress management, suicide prevention, and resource navigation.
Pre- and post-surveys measured knowledge, stigma-related attitudes, self-efficacy, and intentions. Twelve-month follow-up evaluated sustained application of training, mental health conversations initiated, and referrals made. Results showed significant improvements across all measures, with the largest effect sizes for self-efficacy (d = 0.70–0.96) and knowledge (Year 1: d = 0.94; Year 2: d = 0.63; Year 3: d = 0.55). Qualitative analysis revealed high satisfaction, with participants valuing comprehensive resources, skilled facilitation, and culturally responsive content. Twelve-month follow-up showed sustained engagement (97% applied training in their daily lives, 94% had three or more mental health conversations, 77% made two or more referrals). Findings demonstrate the promise of lay health models for expanding community-level mental health promotion and investment in community-driven strategies that go beyond clinical interventions.
Background
Mental health disparities in the United States represent a significant public health challenge. Provider shortages persist, with only one mental health provider per 340 people in the United States (Reinert et al., 2024). Rural areas face greater gaps: 33% lack licensed providers compared to 4.6% urban (Andrilla et al., 2022). Two-thirds of adults with mental illness receive no treatment, particularly pronounced among marginalized communities facing structural barriers including racism, poverty, and inadequate infrastructure (Substance Abuse and Mental Health Services Administration [SAMHSA], 2023). The Health Resources and Services Administration’s (2024) State of the Behavioral Health Workforce Report projects widening gaps for licensed behavioral health providers, consistent with global trends. In response, the World Health Organization (WHO) calls for community-driven approaches providing more upstream strategies that are culturally responsive and extend beyond traditional clinical models (World Health Organization, 2022). A growing body of evidence demonstrates how early intervention for those exhibiting signs of mental illness can significantly mitigate negative outcomes (Balaji et al., 2012; Fuhr et al., 2019; Patel et al., 2011, 2023).
Creating more comprehensive and accessible mental health systems requires cross-sector integration spanning health care, education, social services, and technology (WHO, 2022). Equipping non-specialists, or “lay health” promoters, such as community health workers, peers with lived experience, and/or community members with foundational mental health literacy, to deliver evidence-based interventions may help to extend reach and impact (Patel et al., 2011; WHO, 2022). Their specific application to mental health promotion within a U.S. context requires further exploration.
The Intervention
Mental Health Matters of Washington (MHMWA) is a community-based program that emerged from the co-founders’ experiences navigating loved ones’ acute mental health diagnoses during the COVID-19 pandemic. Despite combined decades of health care and public health expertise, both experienced fear, frustration, and confusion navigating a complex, strained system impacted by service gaps, lack of tailored resources, and stigma. These experiences underscored the need for frontline support strategies that strengthen communities and complement secondary and tertiary care.
MHMWA trains Peer Mental Health Navigators (PMHNs) to promote mental health within their communities through conversations and by connecting individuals, families, and caregivers to resources and care. The program challenges deficit-based narratives by conceptualizing mental health not merely as absence of illness, but as encompassing joy, purpose, and capacity for self-actualization.
Using a strengths-based approach, the program centers groups most impacted by historical, structural, and systemic injustices who experience greater behavioral health disparities. Grounded in critical pedagogy (Freire, 1970), the curriculum recognizes community wisdom in creating strategies that reduce stigma and increase collective dialogue. Through health education and engagement, participants may experience critical consciousness—awareness of how structural and social factors shape mental health at individual, community, and societal levels and motivate one to take action (Freire, 1970). PMHNs may also gain self-efficacy while building skills to support their own mental health and serve as resources to others.
The free PMHN training is offered across six counties in Washington State in hybrid format. The 6-week training combines asynchronous online, mobile-friendly modules with weekly live virtual sessions facilitated by licensed mental health providers and the MHMWA team. Training covers cultural perspectives on mental health, common diagnoses and terms, stigma, stress management, burnout, resource navigation, and suicide prevention. All materials are available in English and Spanish at or below the seventh-grade reading level, accessible via computer and smartphone with hard copies available if needed. Participants receive certificates of completion, a modest stipend (Visa gift card of $150), and a graduation celebration.
The program integrates four theoretical frameworks: socio-ecological model of health (McLeroy et al., 1988) framing mental health as influenced by individual through policy-level factors; critical theory (Freire, 1970) emphasizing critical consciousness and community dialogue; social cognitive theory (Bandura, 2001) explaining peer influence through self-efficacy and modeling; and theory of planned behavior (Ajzen, 1991) describing pathways from attitudes to behavioral intentions and actions.
Research Questions
This study addressed the following questions:
Method
Study Design
This study utilized a non-controlled pre- and post-design with a 12-month follow-up across seven cohorts. The design addressed pragmatic constraints and established feasibility for future longitudinal and controlled designs. The university Institutional Review Board (IRB) approved the study.
Setting and Time Period
The program served six north Puget Sound counties (Snohomish, Skagit, Whatcom, San Juan, Island, and King). Data represent seven cohorts between January 2022 and December 2024.
Participants
A total of 141 PMHNs completed the training and the pre- and post-surveys. Participants were predominantly Latine/Hispanic/Chicano/a/x (62.8%) and female (83.9%), cisgender (91%), and ages 13–70 years (mean of 40). Most (58%) spoke Spanish only, 21% spoke only English, and 21% were bilingual (English-plus another language). Most participants had at least a high school diploma (33%), and only 12% had less than that. More (44%) had some college training, and 11% had a graduate degree.
Measures
Pre- and post-surveys measured knowledge, attitudes, self-efficacy, and intentions using 4- and 5-point Likert-type scales. Constructs were selected based on curriculum objectives and behavior change theories. Items aligned with content and were adapted from established instruments: General Self-Efficacy Scale (Schwarzer & Jerusalem, 1995) and Internalized Stigma of Mental Illness Scale (Boyd Ritsher et al., 2003).
Knowledge was assessed using four items evaluating mental health concepts, distress signs, and resources (α = 0.74). Items were scored as correct (1) or incorrect (0) and summed to create total scores ranging from 0 to 4, with higher scores indicating greater knowledge. Attitudes were measured with seven items assessing stigma-related beliefs and comfort discussing mental health (α = 0.81). Self-efficacy was evaluated through two items assessing confidence initiating conversations and connecting to resources (α = 0.88, scale changed from four-point Year 1 to five-point Years 2–3). Intentions were assessed using two items evaluating likelihood of facilitating conversations about mental health and referring others (α = 0.79, scale changed from Year 1 to Years 2–3). Attitude, self-efficacy, and intention items used Likert-type scales and were summed to create composite scores for each construct, with higher scores indicating more positive attitudes, greater self-efficacy, and stronger intentions. Mean scores for each construct were compared pre-post using Wilcoxon signed-rank tests (Year 1) and paired t-tests (Years 2–3). Open-response questions asked what participants to describe program strengths and areas for improvement or development.
An electronic follow-up survey was distributed to all program graduates 1 year after training completion. Nearly half completed the 12-month follow-up survey (n = 69/141). Variables measured included continuing engagement with MHMWA; ways PMHNs applied training to daily lives; number of mental health conversations initiated; number of referrals made; self-efficacy; and reflective insights or suggestions.
Data Analyses
Researchers used R software for quantitative data analyses. Due to sample size and distribution differences, Wilcoxon signed-rank tests were used for Year 1, while paired t-tests were used for Years 2–3. Qualitative, open-ended survey responses were analyzed using Braun and Clarke’s (2019) reflexive thematic analysis approach, which emphasizes researcher reflexivity and the active role of interpretation in theme development. Two team members independently coded a subset of responses to establish inter-rater reliability (κ = 0.90). The full dataset was then analyzed through iterative coding and collaborative theme development, with ongoing discussion to refine themes and ensure analytical rigor. Dedoose 10 verified themes and identified additional patterns.
Results
Quantitative
All measures improved across cohorts, with variation in significance across years. Table 1 shows Year 1 median scores were significantly greater post-training, with effect sizes ranging from medium (0.45; Attitudes) to large (0.94; Knowledge). Years 2–3 showed consistent improvement patterns (Table 2). Knowledge increased significantly (Year 2: p < .001, d = .63; Year 3: p < .001, d = .55).
Wilcoxon Signed-Rank Tests Comparing Pre- and Post-Surveys for Year 1 (n = 28)
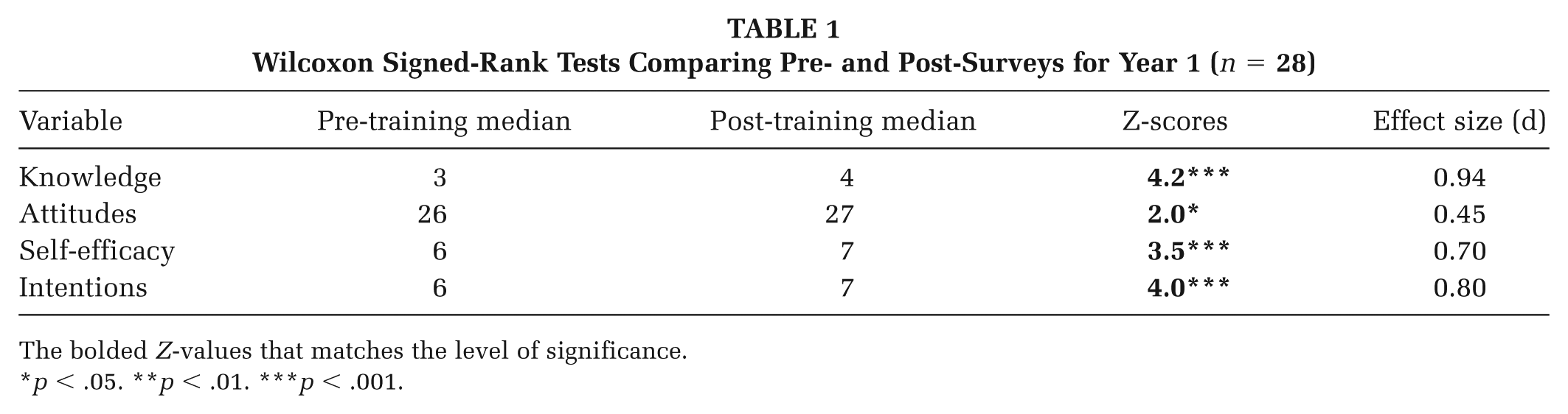
The bolded Z-values that matches the level of significance.
p < .05. **p < .01. ***p < .001.
Paired Sample t-Test Results of Pre- and Post-Training Surveys for Years 2 and 3
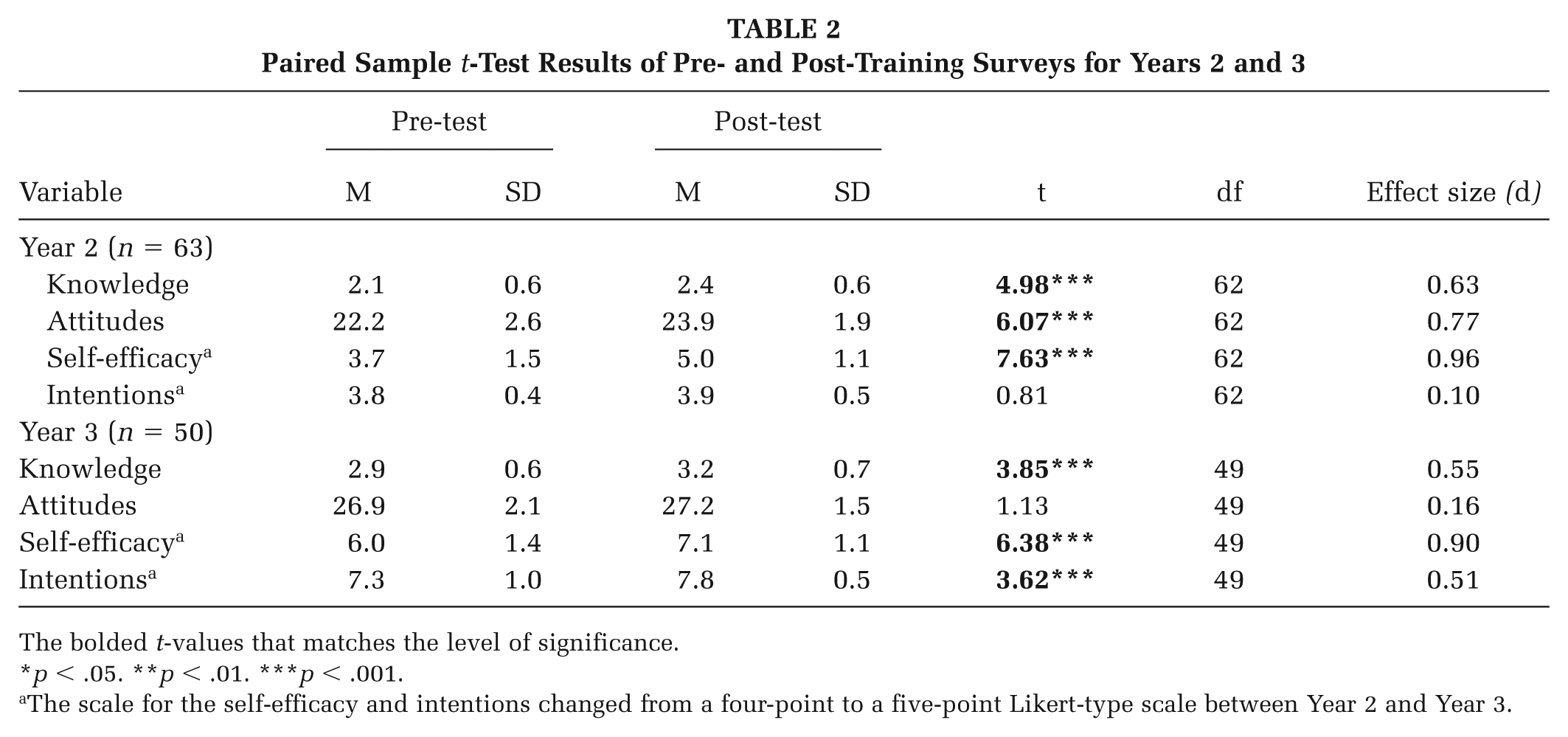
The bolded t-values that matches the level of significance.
p < .05. **p < .01. ***p < .001.
The scale for the self-efficacy and intentions changed from a four-point to a five-point Likert-type scale between Year 2 and Year 3.
Self-efficacy showed the most substantial gains with large effect sizes across all years (Year 1: p < .001, d = .70; Year 2: p < .001, d = .96; Year 3: p < .001, d = .90), indicating substantial confidence improvements. Statistical significance for attitudes and intentions varied between years, likely due to ceiling effects—many participants entered with relatively positive attitudes and strong intentions.
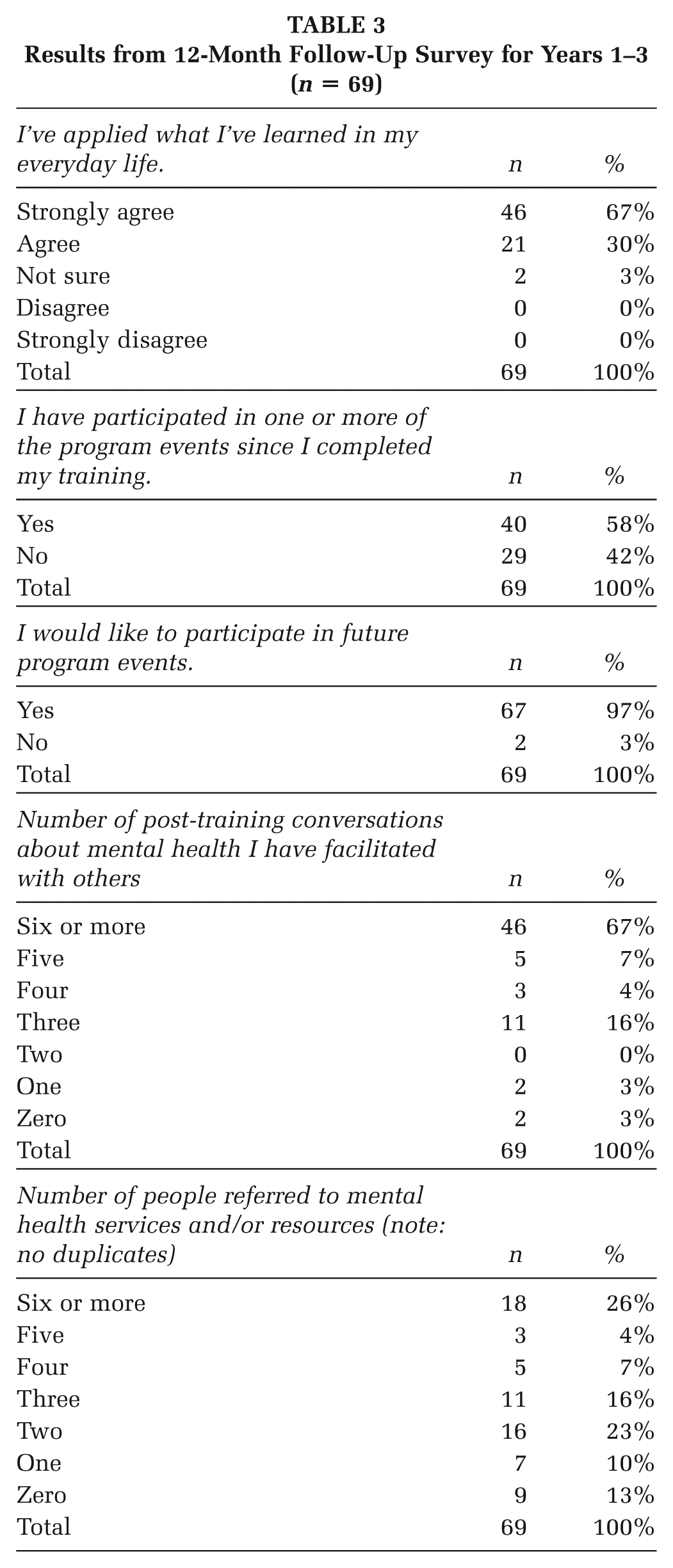
The 12-month follow-up survey (n = 69) demonstrated sustained program engagement and application of training (Table 3). Nearly all peer navigators (97%) reported they applied training in their daily lives. Community engagement exceeded program goals: 94% had three or more distinct mental health conversations with different people (goal was 80%), and 77% made two or more referrals (goal: 80%). Most conversations occurred with family (89%), friends (76%), co-workers (43%), and community members (38%). High satisfaction persisted, with 97% expressing continued interest in program involvement.
Results from 12-Month Follow-Up Survey for Years 1–3 (n = 69)
Qualitative
Two researchers (CG and JS) used Braun and Clarke’s (2019) six-phase approach to analyze 114 qualitative responses to open-ended post-survey questions (70% English, 30% Spanish). Two categories consisting of program strengths and challenges emerged.
Five themes within the program strengths category included:
Accessible comprehensive content: Participants appreciated clear delivery and resource breadth. Spanish-speakers particularly valued primary-language training, often their first opportunity for mental health education in Spanish.
Hybrid design and mobile-friendly format: Participants appreciated both synchronous and asynchronous aspects. Remote, live weekly trainings reduced barriers to access, travel, and child care needs. The asynchronous modules allowed self-paced learning and extra time when needed.
Skilled facilitation: Participants valued the expertise and skill of facilitators, particularly the bilingual, licensed providers.
Peer connection and dialogue: Live breakout sessions enabled meaningful discussion and interaction despite the remote format.
Cultural responsiveness: Content acknowledged diverse perspectives and lived experiences. Discussion of structural determinants and historical events contextualized experiences within systemic factors rather than individual deficits.
Program challenges and development themes included:
Time constraints for completing modules: some felt rushed to complete material within a week.
Spanish dialectal differences: Spanish-speaking participants noted dialectal variations across print and video materials.
Requests for greater coverage of certain topics: Participants requested more information on neurodiversity, LGBTQIA2S+ mental health, mental health and disability justice, and child mental health.
More contemporary and culturally responsive Spanish videos: Participants requested more high-quality contemporary Spanish video content involving storytelling.
Technical difficulties: Some participants struggled to log into the online learning platform during the first week.
Implications for Practice and Future Research
With mental health needs escalating and provider shortages persisting globally (WHO, 2022), this evaluation demonstrates that lay health strategies can mitigate gaps at the community level through culturally responsive, peer-to-peer mental health promotion. Results support global studies that examined lay approaches to interventions for schizophrenia (Balaji et al., 2012), peer-delivered programs for perinatal depression (Fuhr et al., 2019), and community interventions promoting mental health through upstream prevention (Castillo et al., 2019). Mobile-friendly technology integration with lay health strategies offers scalable solutions for expanding support to reach more people (Early et al., 2019).
Results from the current study revealed significant improvements across all measures, with self-efficacy showing the most substantial gains (d = 0.70–0.96). This outcome is particularly significant for community-level mental health promotion. Research demonstrates that self-efficacy predicts both initiation and maintenance of health behaviors (Bandura, 2001), suggesting that confident navigators are more likely to engage in early intervention activities within their social networks—identifying individuals in distress and facilitating access to support before crises develop. This distributed capacity for early intervention extends prevention reach beyond clinical settings into the everyday contexts where mental health needs first emerge.
In addition, the PMHN program achieved sustained engagement over 12 months, with 97% reporting interest in continued participation. The measure of continued program engagement is rarely reported in existing literature on lay health models (Balaji et al., 2012; Early et al., 2019; Patel et al., 2023). Post-training engagement strategies such as community roundtables, outreach events, and discussant opportunities in PMHN trainings may have helped to sustain navigators’ interest over time. In terms of social support and navigation, 94% met conversation goals and 77% approached referral goals, demonstrating population-level reach with room for strengthening referral pathways. Future studies could examine what facilitates or hinders continued participation and referral-making to inform targeted support strategies.
Community capacity building—the characteristics of communities that affect their ability to identify, mobilize, and address social and public health problems (Goodman et al., 1998)—occurs through multiple mechanisms in this model. Navigators reduce stigma through everyday conversations, challenging misconceptions and normalizing help-seeking and preventive strategies (Castillo et al., 2019; WHO, 2022). The training strengthens social support networks by equipping trusted community members with skills and knowledge to connect peers to resources and care. Critical to building capacity, the bilingual, culturally responsive design addresses barriers that often limit participation in health promotion efforts; qualitative findings revealed the training often represented participants’ first opportunity for mental health education in their primary language. Furthermore, graduates may return as peer co-facilitators or for involvement in program events, reinforcing community ownership. By centering cultural strengths and community assets rather than deficits, this capacity-building approach aligns with calls for transforming mental health systems through community-driven models (Patel et al., 2023).
Implications for Policy
While this study demonstrates promise, the PMHN model represents one component of comprehensive mental health systems, not a replacement for clinical services. The program shows adaptability potential for other linguistic and cultural contexts, although effectiveness also depends on authentic community partnerships, sustained funding, and local adaptation to specific community needs.
These findings support investment in evidence-informed, frontline approaches at the community level. Washington State’s 2025–2027 budget allocation for community-based mental health services and programs demonstrates growing policy recognition at the state level of the value of upstream strategies (Washington State Office of Financial Management, 2024).
Limitations and Future Directions
This study had several limitations. First, the lack of a comparison group or randomization prevents controlling for confounding factors and limits the generalizability of results. The researchers are pursuing external funding for a more expansive study that includes a control group. Second, survey measures lacked extensive validation, although items were adapted from established instruments and showed acceptable internal consistency. Third, ceiling effects may have limited detection of changes among participants who entered with positive attitudes and strong intentions. Fourth, the 12-month follow-up achieved a 49% response rate, which could introduce bias favoring highly engaged participants. Fifth, data on conversations and referrals are self-reported and can be difficult to triangulate with more objective measures due to privacy constraints. Future studies could explore tracking methods through partnerships with local service organizations while protecting participant privacy. Finally, the study did not measure participants’ experiences with structural barriers or how the program helped them navigate these challenges.
Conclusion
This study contributes evidence toward the limited number of U.S. studies evaluating lay mental health promotion interventions and supports global evidence of their effectiveness (Balaji et al., 2012; Castillo et al., 2019; Fuhr et al., 2019; Patel et al., 2023). As traditional clinical models alone are insufficient to address escalating population mental health needs nationally and globally, culturally responsive community interventions, such as the PMHN program, provide complementary strategies that support a more comprehensive, inclusive, and equitable mental health ecosystem.
Footnotes
Authors’ Note:
We wish to thank the team at Mental Health Matters of Washington: Sandra Huber, Ana Thompson, Nohemi Rivera, Edith Huerta, Chaze Timbol, Clarissa Carlos, and Monika Starr, along with all of the Peer Mental Health Navigators who are helping to create healthier communities. Funding to support this research was provided by grants from the University of Washington’s Population Health Institute, North Sound Accountable Communities of Health, Skagit Public Health, and Verdant Health Commission.
Authors’ Roles and Contributions
Jody Early conceived of the intervention and this article. She led all aspects of research, including the intervention implementation and evaluation, and oversaw the data collection, analysis, and synthesis. She took the lead on writing the introduction, background, methods, analysis, implications for practice, and conclusion.
Janessa Graves provided consultation on methods, data analysis, and synthesis, as well as contributed to the discussion and editing of the manuscript.
Carmen Gonzalez supported the qualitative data analysis and synthesis, as well as contributed to the discussion and implications section.
Julia Simoes assisted with qualitative data analysis as well as cross-checking references and formatting the article for publication.