
Abstract
We share the process of implementing Project Prevent, Engage, Empower, Respond (PEER), a HIV and substance use primary prevention initiative led by Southern University and A&M College in partnership with the University of Iowa. Project PEER was developed to address the emerging needs of Black/African American college students (ages 18–25) residing in Baton Rouge, Louisiana, a federal Ending the HIV Epidemic (EHE) priority area. Planning involved ongoing consultation with relevant Historically Black/College University (HBCU) and community stakeholders and triangulating multimodal primary and secondary data sources to inform implementation and continuous improvement efforts. Implementation included raising awareness about sexual health promotion and substance use prevention, bimonthly mobile HIV testing, disseminating prevention supplies and print-based materials, delivering the Prevention Plus Wellness evidence-based intervention, and broader community and social media outreach and engagement efforts. Lessons from PEER support the value of HBCU-led, community-academic partnerships that are flexible, culturally congruent, and young adult-driven.
Keywords
Description of the Strategy or Innovation
Project Prevent, Engage, Empower, Respond (PEER) is a Historically Black/College University (HBCU)-led effort to develop, implement, and evaluate an evidence-based HIV and substance use primary prevention intervention. Utilizing the principles and practices of community-engaged research (Wallerstein et al., 2020) and implementation science (Stirman et al., 2019), project activities (a) ensured equitable decision-making between implementers and participants, (b) facilitated co-learning including capacity-building efforts, (c) promoted health equity as mutually identified and agreed upon, and (d) adapted and modified evidence-based interventions to improve engagement, sociocultural congruence, and impact. Project PEER is tailored to and prioritizes 18- to 25-year-old Black/African American college students at Southern University and A&M College in a federal Ending the HIV Epidemic (EHE) priority area, Baton Rouge, Louisiana, in partnership with the University of Iowa. Intervention components included mobile HIV testing, substance use education, and status-neutral linkages to care.
Planning
Strategic planning efforts included triangulating multiple primary and secondary sources of data:
epidemiological data on HIV transmission and linkages to care among Black/African American young adults,
input from a newly established community-advisory board and project consultants, and
key informant interviews with HBCU stakeholders.
Findings informed (a) adaptation of the evidence-based intervention while maintaining fidelity (i.e., Prevention Plus Wellness), (b) outreach and engagement strategies to encourage participation among the priority population, and (c) alignment with community needs (e.g., addressing overall health and wellness; emphasizing mental health promotion). For example, HBCU student leaders participated in a community conversation and provided input about the types of events we should offer (e.g., “condom giveaway”), ways to encourage students to get tested (e.g., “incentives for testing verification”), and strategies to educate the campus community (e.g., “table set-ups around campus”). One student stated,
My ideal program would have multiple guest speakers that would talk about the importance of safer sex and substance use prevention. I would want real past users and people who were diagnosed to give their take on how it affected them.
Another student remarked, “Honestly, it’ll have to start with our student leaders. I feel as though if the students saw us actively getting tested on campus, they’d more likely want to get tested as well.”
Implementation
Implementation began with community outreach (e.g., tabling at existing campus and community events). Prevention peer navigators, consisting of HBCU students and staff, also branded and disseminated “pleasure packs” (i.e., internal and external condoms, lubrication, print resources about testing, pre-exposure prophylaxis [PrEP], and post-exposure prophylaxis [PEP]) at popular collegiate functions and established permanent condom distribution stations. Next, we established long-term bimonthly mobile HIV testing with three committed community-based organizations (see Table 1). These partnerships have been critical to enhancing HIV testing infrastructure on campus, providing a mechanism for fast-track, status-neutral linkages to care. Our partners emphasized a status-neutral approach (Myers et al., 2018), ensuring that all participants, regardless of HIV test results or “status,” received customized support tailored to their individual needs, whether for prevention (e.g., health education, navigation services) or treatment (e.g., antiretroviral therapy, case management).
Example Implementation Strategies and Outcomes
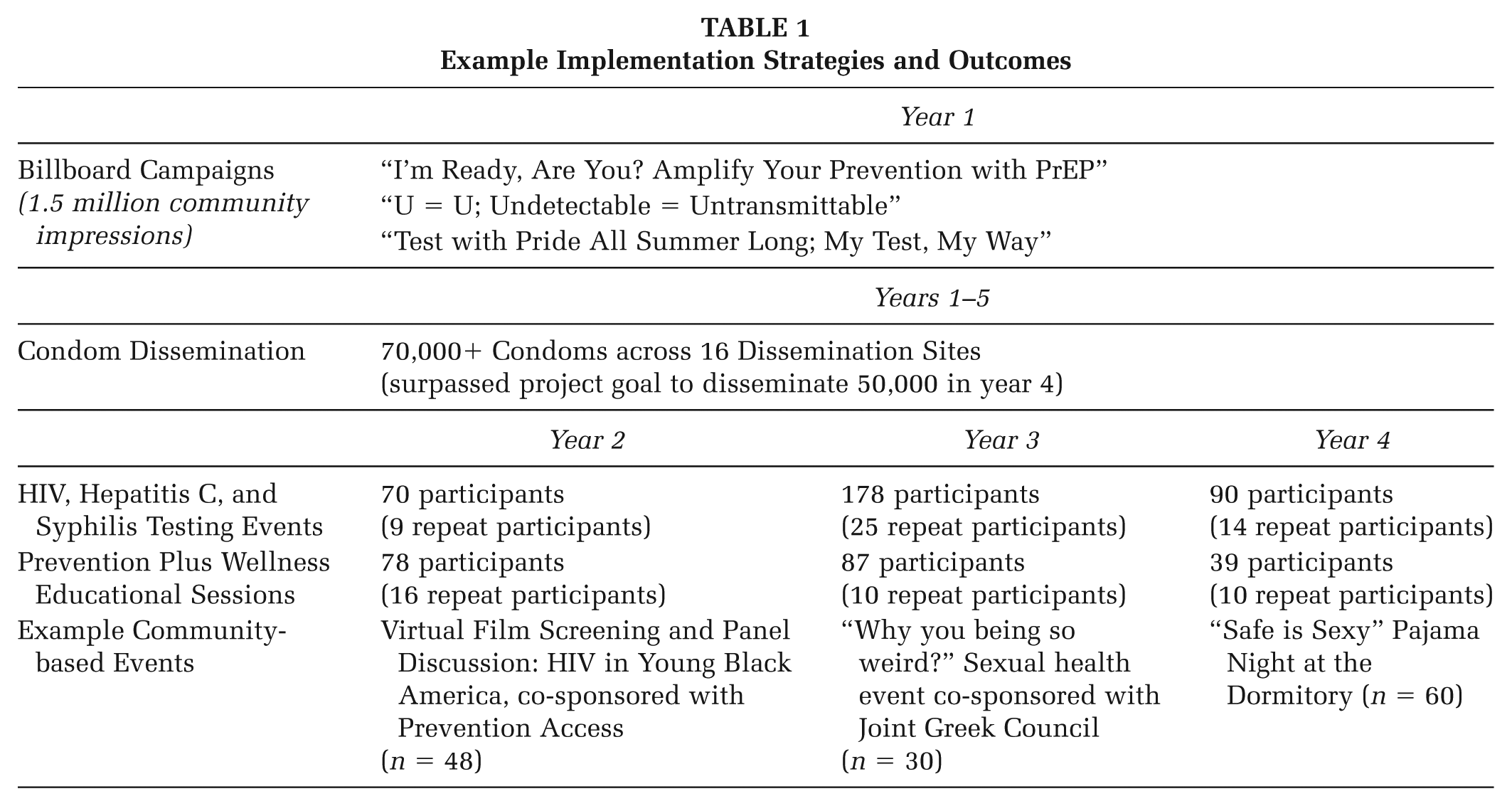
Throughout project implementation, we leveraged social media to engage in outreach, including evidence-informed digital health communication, and to promote project-related events. While accounts were created across multiple platforms, Instagram (@projectpeer) proved most effective. Our prevention peer navigation team developed a content calendar, monitored metrics, and amplified posts during key times (e.g., football season, holidays), when prevention messaging was especially timely. Content was culturally congruent and featured peers in engaging formats such as reels and skits infused with popular songs, dance trends, and trending phrases (e.g., “Talk, Test, Treat”) and hashtags (e.g., #safersexgameplan). Most posts were timed with health observances such as STI Awareness Month in April.
Finally, we partnered with university instructors to implement the evidence-based Prevention Plus Wellness (PPW, 2025) substance use prevention intervention as a guest-lecture series. PPW was selected because it is the only evidence-based, single-session substance use prevention program tailored for young adults and listed on the registry of evidence-based interventions. We expanded PPW to include content related to sexual health and expanded content on marijuana use in alignment with the needs of the project and target population. Adaptations followed the Framework for Reporting Adaptation and Modifications to Evidence-Based Interventions (Stirman et al., 2019) to ensure fidelity while making changes to content (e.g., culturally congruent images) and/or context (e.g., didactic to experiential format changes such as creating artwork to indicate alcohol serving sizes that lead to inebriation versus lecture). During the guest lecture, we introduced the project and provided a verbal overview of the informed consent process, including options to participate with or without data collection or to opt out entirely. Participants then scanned a QR code to e-sign consent and complete a pre-survey assessing targeted outcomes. Participation was voluntary, not linked to their course requirements, and students could opt out of the session or survey at any time.
Evaluation
Over the five project years, 282 students participated in HIV testing and status-neutral linkages to care, and 217 students participated in the PPW substance use prevention intervention, with the highest participation levels in Year 3. These participant numbers only reflect those who opted in for data collection and long-term follow-up during the informed consent process; therefore, the total number reached over the 5 years is higher. Participants completed an online pre- and post-test survey, distributed via QR code at testing events and workshops. Surveys included demographic data and validated instruments measuring perceived HIV risk, PrEP knowledge, and alcohol and substance use behaviors. Data revealed that most HBCU students, pre-intervention, have a low perceived risk of acquiring HIV (m = 17.49, SD = 5.93, range = 5–33), and report low knowledge about PrEP (m = 3.50, SD = 2.17, range = 0–8); 91.4% reported little to no substance use. We also found differences in perceived risk by student sexual orientation. These data helped to inform our health communication campaigns via social media, raising awareness as a universal primary prevention strategy.
Challenges and Successes
A core challenge involved navigating the administrative infrastructure of two institutions in two distinct regions. Any delays in processing (e.g., purchasing or invoicing) at one institution can cause a delay at the other institution. Staff time needed to navigate administrative challenges sometimes impacted the project implementation timeline. Another challenge involves broader social determinants of health. National survey data (e.g., National College Health Assessment) and key informant feedback highlight common concerns among the priority population, such as meeting basic needs, balancing work and school, and managing stress and mental health. These pressing concerns can overshadow sexual health and substance use prevention efforts. Addressing this challenge requires intentionally integrating prevention efforts with broader initiatives that respond to these pressing concerns.
Despite these challenges, Project PEER achieved key successes, particularly in the areas of community outreach and engagement and social media engagement.
Outreach and Engagement
Our project coordinator’s leadership was critical to the success of outreach and engagement efforts. For example, she partnered with the Louisiana Department of Public Health for multiple on-campus tabling events including the dissemination of prevention-related digital and print resources. Other examples include working with local organizations to disseminate resources and raise awareness around TelePrEP to ensure HBCU students received rapid access to PrEP and to expand at-home testing accessibility by disseminating free testing kits during tabling events. Recognizing that college is a time for fun and self-discovery, our engagement efforts also included music and dancing at tabling events encouraging visitors to showcase the latest trends, an educational “spin the wheel” game to win swag (e.g., cups, T-shirts) at tabling events, and co-hosting fun activities such as a Let’s Get Physical Sports Tournament and Sexual Wellness Clinic (n = 27 students tested). A key to engagement success was partnering with student organizations including sororities, fraternities, athletics, and clubs, which already have civic and social engagement goals each semester.
Social Media Outreach and Engagement
Throughout the project, we increased our social media presence across multiple platforms. To date, our Instagram social media account has 955 followers. Reels and videos created by our prevention peer navigators have a wider reach. For example, in partnership with a campus sorority collaborator, an Instagram reel scripted, produced, and posted to educate students about PrEP as a prevention tool was viewed 24,500 times by 10,373 accounts.
Implications for Practice
Our insights and recommendations from PEER that we hope will inform practice in similar settings include:
Be intentional and consistent in community engagement and outreach efforts.
Recognize that sexual health promotion and substance use prevention may not be a pressing concern for college students, but these initiatives can be infused and embedded with interventions that align with their needs and priority areas (e.g., mobile HIV testing during a food or personal hygiene product dissemination event).
Acknowledge that college is simultaneously a time for fun and self-discovery—we recommend infusing fun activities in prevention efforts.
Leverage existing collegiate infrastructure and associated events (e.g., homecoming) and campus leaders (e.g., student government) for planning and staffing.
Build capacity for young adults to grow into leadership roles, as their work in campus prevention can lead to career pathways in the behavioral and public health workforce.
Our lessons from PEER support the value of HBCU-led, community-academic partnerships that are flexible, culturally congruent, and young adult-driven.
Footnotes
Authors’ Note:
We would like to thank the local, state, and federally funded prevention and linkages to care agencies that provided consultation, expertise, and HIV and STI testing services. Special thanks to the administration of Southern University and A&M College, project consultants, members of the community advisory board, team of prevention peer navigators, field experience students, interns, and volunteers for their aid in the conceptualization, development, implementation, evaluation, and sustainability of the project. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was made possible by the Substance Abuse and Mental Health Services Administration (1H79SP082109). The views expressed do not necessarily reflect the official policies of, or endorsement by, the U.S. Department of Health and Human Services.