
Abstract
Political skepticism and legislative threats like the One Big Beautiful Bill Act (OBBBA) currently shake the structures supporting public health. OBBBA seeks to de-professionalize our credentials by reducing federal loan caps from $50,000 to $20,500. It seems the fundamental necessity of our workforce remains undeniable despite these challenges. I address the anxiety of students and early-career professionals by contrasting this hostile political landscape with economic labor realities. I map the educational continuum, noting undergraduate public health degrees surpassed master’s degrees in 2020. They now serve a student body that is over 55% people of color. I measure these trends against 2024 U.S. Bureau of Labor Statistics projections for five core disciplines: biostatistics, epidemiology, health policy, environmental health, and health promotion. Data indicate strong growth across the sector while governmental wages stagnate and loan forgiveness faces legislative peril. Roles like data scientists and medical services managers are projected to grow by 34% and 23%, respectively. Wage disparity is stark. Epidemiologists earn a median of $130,390 in scientific research compared with just $76,180 in local government. I argue market demand and the World Health Organization’s projected global shortfall of 18 million health workers by 2030 validate our expertise. The narrative of de-professionalization likely poses a severe risk to health equity. Our labor is essential, whether we are investigating disease outbreaks or advocating for environmental justice. We must remain resilient and train to become the professionals our communities require to survive.
Introduction
We stand at a precarious moment in the history of our profession. The structures that have long supported the public’s health are shaking under the weight of political polarization and skepticism. Recent administrative shifts have ushered in an era where the core institutions of public health are being dismantled, and the scientific consensus we rely upon is openly challenged by powerful figures (Yamey & Shaffer, 2026). Furthermore, we face legislative threats that seek to redefine “professional degree programs” in a way that excludes the Master of Public Health (MPH) and Doctor of Public Health (DrPH), potentially restricting access to federal loans and signaling a dangerous move toward de-professionalization (Magaña, 2026).
Many students and colleagues wonder if our chosen field will sustain us. As a practicing professional and Doctor of Public Health student who holds a Master of Public Health, I acknowledge a natural incentive to present a positive value proposition for the academic credentials I pursue and the workforce I actively support. Despite these headwinds, the fundamental truth remains: disease, environmental hazards, and systemic inequities do not care about political affiliation. The need for a skilled, compassionate, and resilient public health workforce is not diminishing, but growing, with the World Health Organization estimating a global need for 18 million additional health workers by 2030 (Kedia et al., 2024).
This article is intended for the students and early-career professionals who are stepping into this breach. While the sector is being destabilized, public health remains a critical labor market. Schools and programs will continue to matriculate students because our communities need skilled partners to collaborate in identifying and solving complex systemic health challenges. Here, I outline the primary disciplines of public health, mapping them to specific occupations, compensation, and growth projections based on 2024 data from the U.S. Bureau of Labor Statistics (BLS) Occupational Outlook Handbook (OOH, 2025). By understanding the educational landscape and the economic realities of the field, we can build careers that are not only resilient but also revolutionary.
Undergraduate to Doctoral Public Health Education: A Continuum of Training
Public health education has evolved from a niche graduate field into a robust continuum spanning from associate degrees to doctoral leadership. The undergraduate public health degree surpassed the master’s in 2020, becoming a primary workforce pathway with over 55% of recipients coming from communities of color (Leider, Burke, et al., 2023; Resnick et al., 2018). These programs provide foundational knowledge in health disparities, epidemiology, and global health. Despite fears that bachelor’s graduates might displace master’s-level workers, data show they find distinct roles in diverse sectors like for-profit firms and health care organizations (Leider, Burke, et al., 2023).
Graduate Education: The Professional Standard
The MPH remains the primary professional credential for public health, accounting for 71% of all public health master’s degrees awarded by Association of Schools and Programs of Public Health members (Beck et al., 2020). Although only 14% of the governmental workforce holds a public health degree (Leider, Yeager, et al., 2023), master’s graduates secure these roles at nearly double the rate of bachelor’s graduates, highlighting the credential’s distinct professional weight (Leider, Yeager, et al., 2023). In response to workforce needs, MPH curricula have shifted significantly since 2016; programs are now moving away from siloed disciplines toward integrated, competency-based models that emphasize evidence-based approaches, leadership, and systems thinking (Pennel et al., 2026). This evolution ensures that graduates are not just knowledgeable, but skilled in the practical application of public health science (Meredith et al., 2023).
Doctoral Education: Research and Leadership
At the doctoral level, a clear distinction exists. The PhD focuses on generating new knowledge through research, while the DrPH is designed for advanced practice leadership. DrPH programs equip leaders to manage complex organizations and advocate for evidence-based policies in challenging environments (Park et al., 2021).
The Durability of the Public Health Workforce
The narrative of “de-professionalization” poses a risk we cannot afford to ignore. Excluding public health degrees from professional designations threatens to widen health disparities and weaken our defense against future pandemics (Magaña, 2026). However, the labor market tells a story of continued demand. The reality of an aging population, the inevitability of future infectious outbreaks, and the deepening crisis of chronic disease necessitate a workforce trained in prevention and systems thinking.
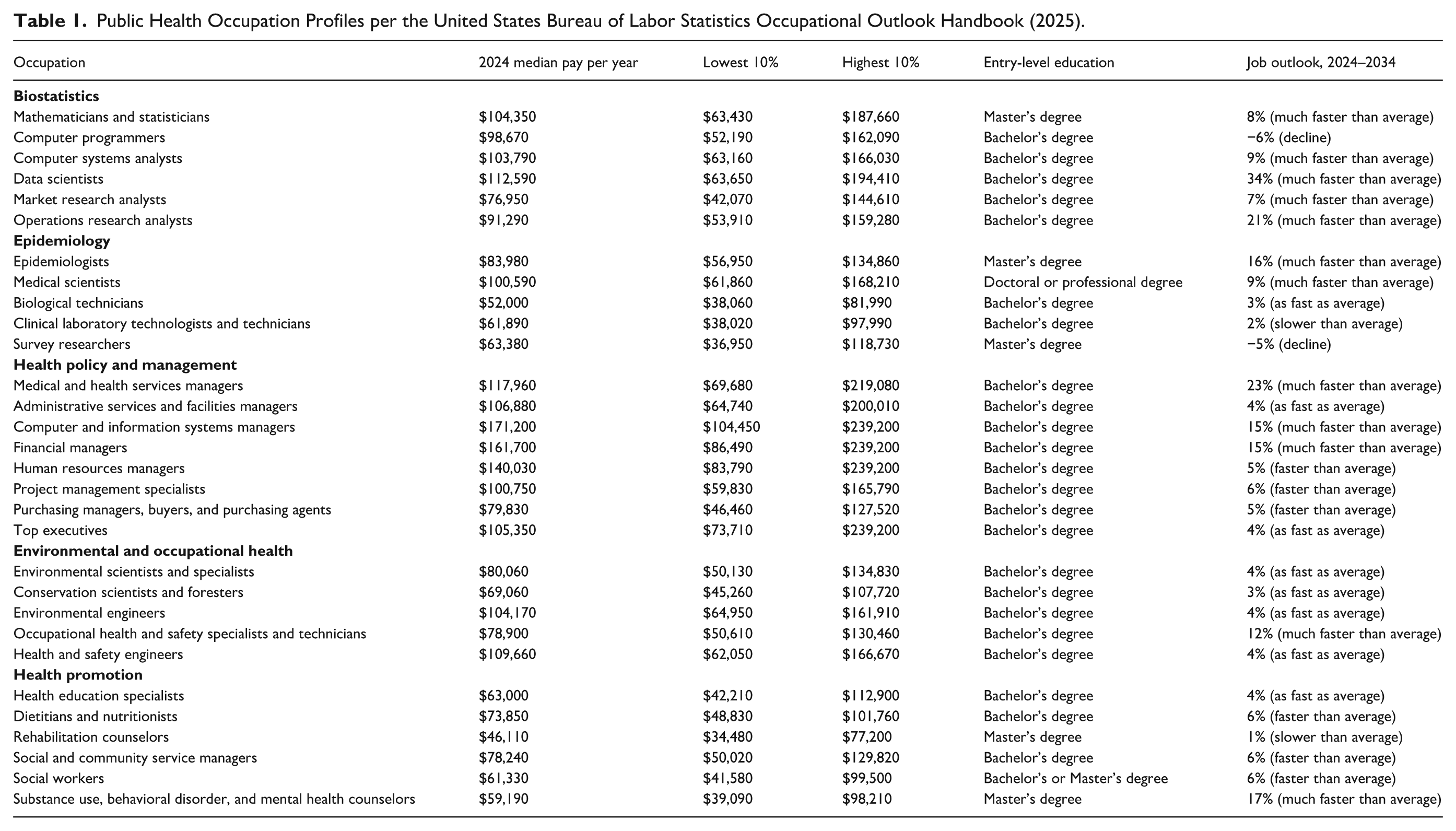
We must remain clear-eyed about the challenges, including stagnant governmental wages and high student loan burdens that necessitate policy interventions like loan forgiveness (Leider et al., 2026), but also confident in the value of our labor. The following sections highlight five core disciplines, with full wage and growth projections detailed in Table 1 (OOH, 2025).
Public Health Occupation Profiles per the United States Bureau of Labor Statistics Occupational Outlook Handbook (2025).
Biostatistics: The Architecture of Evidence
Biostatistics provides the quantitative foundation for public health decision-making. Biostatisticians translate complex data into actionable insights, a skill set that is highly transferable across sectors. According to the BLS, the outlook for mathematical and data-oriented roles is robust. Mathematicians and statisticians earn a median annual pay of $104,350, with a projected job growth of 8% between 2024 and 2034 (OOH, 2025). Even more striking is the demand for data scientists, a role increasingly filled by public health graduates with strong quantitative skills. The median pay for data scientists is $112,590, with a projected growth rate of 34%, classified as “much faster than average” (OOH, 2025). For students engaged in this discipline, the message is clear: your skills are in high demand. Whether in clinical settings, tech companies, or research institutions, the ability to make sense of data is a currency that retains its value.
Epidemiology: The Disease Detectives
Epidemiology remains the cornerstone of public health practice. Despite the political backlash against infectious disease control measures (Yamey & Shaffer, 2026), the biological reality of disease transmission ensures that epidemiologists are essential. Epidemiologists investigate patterns, identify outbreaks, and provide the evidence base for interventions.
Current employment trends validate the critical demand for these skills. Epidemiologists see a median annual pay of $83,980, with a job outlook projected to grow by 16% over the next decade (OOH, 2025). The BLS OOH lists median wages for those working in “scientific research and development services” at $130,390, and $76,180 for those working in “local government, excluding education and hospitals.” For those advancing to doctoral levels, medical scientists earn a median of $100,590 and are expected to see 9% growth (OOH, 2025). While some related roles like survey researchers face a decline (−5%), the core analytical roles in disease control remain strong (OOH, 2025). Despite potentially hostile environments, employment trends confirm society’s ongoing need for disease surveillance and control.
Health Policy and Management: Steering the Systems
Professionals in this discipline manage health care systems, advocate for policy changes, and oversee the administrative functions of public health organizations. In the face of budget cuts and policy retractions, skilled managers are vital to maximize limited resources. This discipline offers some of the highest financial compensation within the field. Medical and health services managers earn a median of $117,960 per year, with a massive projected growth rate of 23% (OOH, 2025). Financial managers within health sectors earn upwards of $161,700, also with strong growth prospects (OOH, 2025). These roles often require navigating complex bureaucratic and political landscapes, including fighting on the front lines to keep clinics open and programs funded.
Environmental Health: Guardians of the Commons
Environmental health professionals tackle issues ranging from toxicological risks to the climate crisis. As regulations protecting air and water are threatened, the work of environmental scientists becomes an act of defense for our most basic life support systems. The BLS data indicates stable growth in this sector. Environmental scientists and specialists earn a median of $80,060, with a 4% growth rate (OOH, 2025). Environmental engineers command higher salaries at $104,170 (OOH, 2025). Notably, occupational health and safety specialists are projected to see 12% growth, reflecting a continued need for workplace safety expertise (OOH, 2025). Environmental degradation disproportionately affects marginalized communities. Entering this field is a commitment to justice, ensuring safe air and water for everyone.
Health Promotion: The Heart of Community Health
Health promotion serves as the bridge between scientific consensus and community action. It involves education, behavior change, and community organizing. Health promotion specialists are critical messengers who rebuild relationships and foster community resilience.
While the financial compensation in this discipline is generally lower than in policy or biostatistics, the growth is steady. Health education specialists earn a median of $63,000, with average growth projections (OOH, 2025). Social and community service managers, who often oversee health promotion programs, earn $78,240 and are seeing faster-than-average growth at 6% (OOH, 2025). Furthermore, the demand for substance use and behavioral disorder counselors is skyrocketing, with a 17% projected growth rate, reflecting the deepening mental health crisis in the United States (OOH, 2025). Although often under-resourced, this work is the vital human connection where we translate data into dignity.
Implications for Policy
The Department of Education recently proposed narrowing the definition of “professional degree programs” under the One Big Beautiful Bill Act (OBBBA), a move that specifically excludes the MPH and DrPH (Magaña, 2026). This legislative shift carries severe financial consequences, as OBBBA caps annual federal loans at $20,500 for nonprofessional graduate students, compared with $50,000 for professionals (Cooper, 2025). Stripping public health degrees of their professional designation restricts access to necessary federal loan resources and makes these degrees fundamentally less attainable for many students (Magaña, 2026). These policy changes risk dismantling the pipeline of future public health workers exactly when the labor market demands their skills most (Magaña, 2026).
Implications for Practice
The implications of this analysis for public health practice and education are immediate and existential. The data reveal a clear reality for public health practice: despite federal instability, demand for public health professionals in areas like biostatistics, epidemiology, and health management is growing rapidly. Practitioners and local health departments must recognize they operate in a highly competitive labor market where private sector entities frequently recruit public health graduates (Krasna & Fried, 2021). Public health agencies need to adapt their recruitment strategies to capture this talent. Organizations must streamline notoriously slow hiring processes and build funded internship pipelines that connect students directly with the practice community (Krasna & Fried, 2021).
Furthermore, new graduates face substantial barriers to entry, particularly the growing expectation that even low-level positions require significant practical experience. Many internships or practica in government public health remain unpaid (Krasna & Fried, 2021). This creates a systemic barrier that excludes students who are eager to work in public service but cannot afford to do so without compensation (Krasna & Fried, 2021). A lack of accessible, paid field experience prevents diverse talent from gaining the applied skills necessary to secure entry-level employment.
We must also fiercely defend the professional status of our degrees against legislative attempts at reclassification. This de-professionalization threatens both our financial viability, by restricting loan access, and the very legitimacy of our expertise during times of crisis (Magaña, 2026). However, defense alone is insufficient; we must also adapt. Educational institutions have already begun this pivot, with nearly half of accredited schools fundamentally redesigning core curricula since 2016 to emphasize integrated, cross-cutting competencies over siloed knowledge (Pennel et al., 2026). This pedagogical shift must accelerate, particularly for DrPH programs, to cultivate leaders who possess not just technical acumen but the strategic capability to advocate for evidence-based policy in the face of political hostility (Meredith et al., 2023; Park et al., 2021). Simultaneously, we must address the economic precariousness of our workforce; with student loan debt averaging nearly $50,000 among those with balances, and significantly higher for graduates of color, the failure to provide robust loan forgiveness mechanisms actively dismantles the diversity and retention of the governmental workforce (Leider et al., 2026). Consequently, while graduates increasingly find stability in the for-profit and health care sectors (Leider, Burke, et al., 2023), the field must forge new pathways that allow these professionals to apply their essential skills, whether in data science or health management, toward the public good, regardless of their employer. Students and established practitioners are not simply building careers; we are safeguarding the survival of our communities.
Conclusion
The storm we are weathering is fierce. The attacks on public health science and the attempts to strip our degrees of their professional status are real threats to the infrastructure of our nation’s health (Magaña, 2026; Yamey & Shaffer, 2026). However, data from the BLS confirms that the labor market still values our expertise (OOH, 2025).
We must not let the current political climate deter us from this calling. Whether you are analyzing data to track a new pathogen, managing a rural health clinic, or organizing a community for environmental justice, your work matters (Beck et al., 2020). We will continue to train, we will continue to show up, and we will continue to be the professionals that our communities deserve.
Footnotes
Acknowledgements
I would like to acknowledge the courage of the public health student body and workforce to persevere.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: I am deeply grateful to the university for its generous support through the DrPH Fellowship and the Felix and Helen Juda Endowed Fellowship. In addition, I would like to thank the Crossing Boundaries Research Award, which is funded by the Richter Memorial Funds Master Code, Bank of America, N.A., Trustee.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.