
Abstract
The needs of people experiencing homelessness (PEH) are at a modern high, yet health-promotion programs typically operate from clinic-based models that do not reliably reach unsheltered settings. Street engagement, conducted with community partners, can support access to basic needs, trust-building, and continuity of care. We present the BRIDGE framework (Build trust, Rapidly assess, Identify needs, Direct connections, Guide handoffs, Evaluate follow-up), distilled from sustained community outreach with PEH in Milwaukee, Wisconsin, integrating harm-reduction, trauma-informed communication, and warm handoffs through practical tools (approach scripts, packing lists, and safety checklists). We collect feasible process indicators (e.g. number of contacts, referrals initiated, and successful connections) and provide a flow figure and protocol table to guide action. Embedded vignettes from multiple perspectives provide implementation context. BRIDGE operationalizes equitable health promotion for street engagement centered on ethics, safety, and trust and can be adopted by health departments, academic programs, and community partners to systematize outreach and strengthen continuity of care. A clear, replicable framework with minimal metrics can elevate street engagement beyond goodwill to accountable practice that advances health equity.
Keywords
Purpose and Practice Gap
On any night, hundreds of thousands of people in the United States lack stable housing, including people living in shelters, outdoors, or in places not meant for habitation (U.S. Department of Housing and Urban Development [HUD], 2024). Men/boys make 59.6% of all people experiencing homelessness (PEH) in 2024 and 67.4% of people experiencing unsheltered homelessness (HUD AHAR 2024, Exhibit 1-5). People of color constitute the majority of PEH when race and ethnicity categories are considered collectively, including large shares identifying as Hispanic/Latine (any race) and Black (HUD, 2024). Family homelessness increased sharply; the number of families with children experiencing homelessness increased by 39% between 2023 and 2024 (HUD, 2024). Older adults represent a substantial share of homelessness, as roughly one in five PEH in 2024 were of age 55 years or older (HUD, 2024). Data indicate that homelessness increased by 12% from 2022 to 2023 and then by 18% from 2023 to 2024 (HUD, 2024), signaling a growing wave of individuals at risk of becoming unhoused in the future. A severe shortage in affordable rentals, rent increases outpacing wage increases, and sustained shelter inflation have increased homelessness risk, with a $100 median rent increase now associated with a 9% rise in homelessness (U.S. Government Accountability Office [GAO], 2020). Although street medicine and outreach programs are expanding, few published models translate equity, structural determinants, and relationship-centered practice into a concrete, replicable sequence of steps for frontline teams. BRIDGE addresses this implementation gap by specifying a step-by-step sequence with role clarity, feasible tools, documentation fields, and a minimal indicator set that supports learning without overburdening teams. Unlike narrative descriptions of outreach, BRIDGE is presented as an operational protocol designed for replication and local adaptation while maintaining fidelity to consent, dignity, and warm handoff expectations. This article presents an approach and framework for identifying, connecting with, and supporting PEH. The approach described here reflects interdisciplinary practice and community partnership and is presented as a replicable protocol rather than role-specific commentary. The development and application of BRIDGE draw on sustained street engagement with PEH and iterative team debriefs that translate field lessons into tools, procedures, and follow-up rules.
The BRIDGE Framework
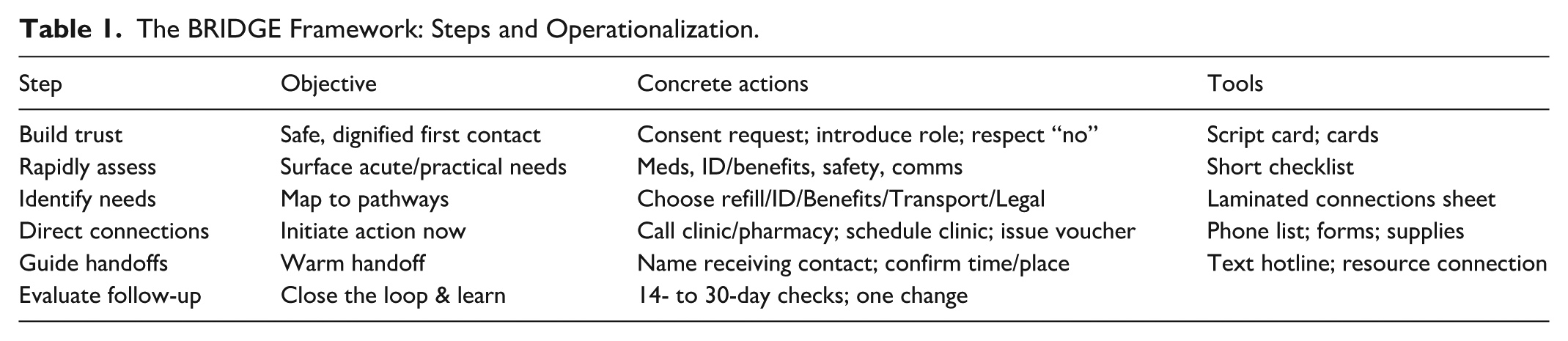
We organize our engagement efforts using the BRIDGE framework (see Table 1): Build trust (approach those we encounter with consent and dignity), Rapidly assess (consider safety, acute needs, documents and medications, and communication), Identify needs (map to existing networks and support pathways), Direct connections (initiate warm handoffs during or immediately after encounters), Guide handoffs (warm connections with consent, including time, place, and contact information), and Evaluate follow-up (brief check within 2 weeks and team debriefs to facilitate learning and process). The BRIDGE systematizes our process of preparation, engagement, connection, and follow-up, creating clear, memorable, and repeatable action steps that facilitate quality improvement in training and outreach.
The BRIDGE Framework: Steps and Operationalization.
Setting, Partnerships, and Outreach Context
The BRIDGE framework was developed through repeated outreach encounters with PEH in an urban environment. An interdisciplinary team of community-engaged faculty, a family medicine physician, trainees, outreach partners, and community volunteers provided care and connection in encampments, shelters, and other nontraditional spaces. The work was anchored in equity, relationship-centered practice, and attention to structural determinants of health, but these commitments were initially diffuse rather than organized into a clear, reproducible sequence that teams could follow and teach.
Framework Development Approach
To make outreach practice more intentional and transferable, the team adopted a structured cycle of preparation, field work, and debriefing. Before each outreach session, the team clarified goals, anticipated safety and basic needs, and reviewed roles and expectations. Immediately after each session, facilitated debriefs invited all team members to reflect on the day and to name what worked, what felt misaligned with equity commitments, where structural barriers were most visible, and what was most impactful. These debriefs consistently surfaced themes related to trust-building, rapid assessment, prioritizing needs, navigating handoffs, and following up in ways that preserved relationships with PEH.
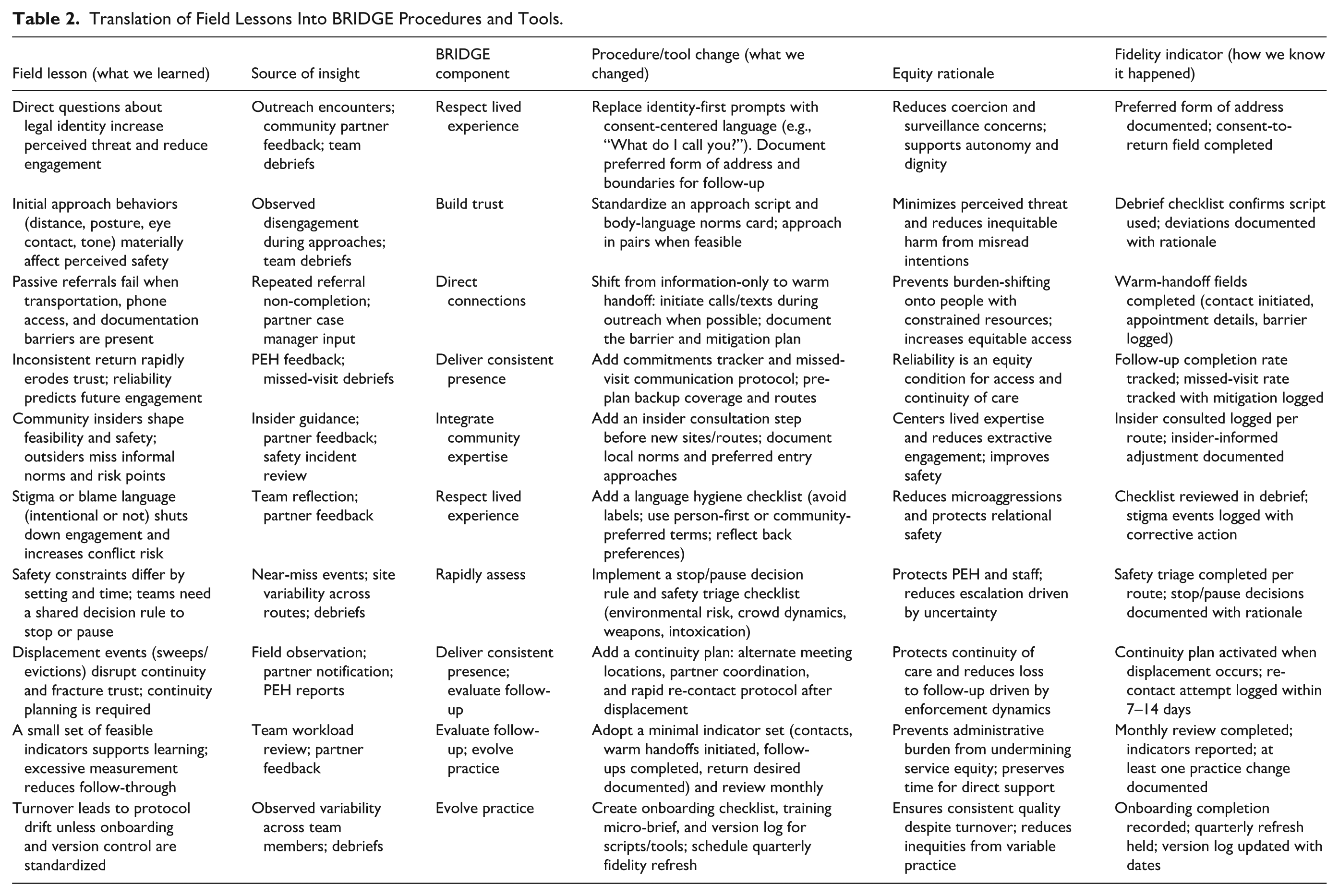
The team documented these themes and paired them with simple process indicators, including counts of outreach events, types and number of contacts, resources offered, handoffs initiated, and follow-up attempts completed (see Table 2). Guided by community-based participatory research principles and Glassick’s criteria for scholarship, related behaviors and decisions were grouped into a small number of steps that could be remembered and enacted in the field. Acronym development was used deliberately to support teaching and team alignment. After multiple cycles of revision and use with trainees and outreach partners, the six-step BRIDGE sequence (Build trust, Rapidly assess, Identify needs, Direct connections, Guide handoffs, and Evaluate follow-up) consistently captured the full arc of outreach encounters. The current version of BRIDGE is a practice-derived framework that synthesizes structured team reflection, process data, and equity-oriented conceptual foundations rather than a novel theory. Presenting BRIDGE in this way makes explicit the concrete actions, questions, and quality-improvement routines that operationalize equity commitments during outreach and positions the framework for adaptation, testing, and refinement by other teams working with PEH.
Translation of Field Lessons Into BRIDGE Procedures and Tools.
Step-by-Step Implementation Protocol
We have organized these from-the-field lessons utilizing the BRIDGE framework (Build rapport, Rapidly assess, Identify needs, Direct connections, Guide handoffs, Evaluate follow-up).
Build trust: Trust is the prerequisite for every subsequent step in street engagement and cannot be assumed shortcut or delegated to a resource list. Building trust with PEH requires recognizing that institutional contact has frequently been experienced as surveillance, judgment, or coercion rather than care. Effective trust-building begins with community identity: who individuals are, what they have survived, and what they have learned about which outsiders are safe to engage. Everything we do in the field begins with this foundation.
As an early-career physician, the clinic where I practice is conveniently located near a bus station, making it more accessible for those who lack reliable personal transportation. As such, there are a significant number of patients for whom I care who have unstable housing or are unhoused. From the perspective of an outpatient clinic, I noted times when individuals had their meds stolen and needed early refills, which made their health care difficult. (Physician and StreetLife team member) Systems support for health issues faced at either the individual or community level has often been derived from a single focus space, and many emerged because the U.S. government removed support, specifically in the areas of hunger and housing, starting during the Reagan presidency (Crafton, 2014; Rosenberry, 1983). Failure to recognize the effects of system changes and reductions has led to a transactional approach to support, rather than a relational one. (StreetLife team member)
2. Rapidly assess: Rapid assessment during outreach requires teams to enter the field already calibrated to what they are looking for. Glassick’s criteria for scholarly work (Glassick et al., 1997) establish that adequate preparation is a precondition for meaningful inquiry; the same principle applies in street engagement. Teams that have clarified goals, reviewed available resources, and aligned on roles are positioned to assess acute needs (medications, documents, safety, access to communication) quickly and without losing the thread of a fragile first encounter. Preparation is not administrative overhead; it is the operational foundation of rapid assessment.
Once I better understood my goal, I found assessing the needs of PEH to be a challenging task. Most individuals are not those I would see in my clinic or the hospital until they were already unstable or quite ill. Some of my logistical preparation involved accessing existing street medicine resources to better understand what medications or supplies would be most needed. (Physician and StreetLife team member) Foundational to our process is respect: We respect those we encounter and engage each person in an empathetic and humanistic way. This alone highlights the need for contextual cueing of trainees, as the strategies we commonly employ to show respect and care in work and educational spaces (e.g. eye contact, handshakes, hugs, making ourselves “big”) are often the opposite of our approach on the street. (StreetLife team member)
3. Identify needs: Identifying needs requires presence. Secondary data and published literature provide useful contextual framing, but the immediate, actionable needs of PEH (a stolen medication, a missing ID, a safe location for the night) are not visible from a desk or a clinic. Clinicians who treat patients in the clinic rarely see the environments those patients return to; thus, systematic outreach to those environments is essential to close the gap between documented health status and lived experience. Identifying needs begins the moment the team enters the community, not when an intake form is completed.
Going into the community was certainly eye-opening. I was admittedly a bit nervous and unsure what steps to take. What questions would we ask? Would people want to talk with us? We took quite a few bag lunches, and I was surprised how many people were thrilled to have the food and how fast we ran out. (StreetLife Team Member) Community engagement in the space of homelessness involves engaging with people that many in our society actively avoid and make efforts to overlook. Nearly nobody, however, is “invisible.” Part of our work relies on trusting relationships with community insiders, including those who have lived unhoused and are familiar with the areas, survival skills, and patterns often exhibited by PEH. Signs, once seen, cannot be unseen. Our teams venture under bridges, along waterways, behind buildings, and other areas, always in teams, whenever possible, with a trusted community insider, to seek those in need of support. (StreetLife Communities Founder and team member)
4. Direct connections: Getting out of the clinic or office is the first step, and the following means talking to people. We met some people outside in a park and struck up a conversation. After providing lunch, we asked if they knew of places where others might be, and they did so, willingly telling us where they were and what they liked to be called. Being seen as trustworthy also means being polite and respectful. In this instance, it was reciprocated. (StreetLife Communities Founder and team member)
We eventually encountered a group at a park gazebo who were listening to a small radio while smoking and happily chatting. One of the people was a patient of mine, and while it was nice seeing him healthy with friends, it reminded me that for some of my patients, this was their everyday experience. It was a world removed from easily accessible prescriptions and concerns about the next annual physical, replaced by caution for the few things you could carry and uncertainty about the next meal. (StreetLife Communities Founder and team member) Meeting community members and engaging people where they exist represents one of the greatest joys and challenges we face in supporting PEH. Existing systems designed to help health are replete with diverse elements that present significant barriers to access for those living on the margins. Safety in this space also requires respect and open-mindedness on the part of our trainees, as many of the people we encounter are engaged in activities and behaviors that fall outside the “normal” patterns we commonly see, including substance abuse, sex work, actions identified as criminal, violence, and others. Withholding judgment in these instances is paramount, as we cannot know the circumstances and context that have led people to their current situations. (StreetLife Communities team member)
5. Guide handoffs: Guiding a warm handoff requires knowing where someone can be found again. Unlike clinic-based referral, which assumes a fixed residence and phone number, outreach handoffs depend on spatial and relational knowledge: Where does that person regularly shelter, what routes to they travel, and who will they trust? Physical traces of habitation (items left at consistent locations, evidence of repeated use of shelter spaces) constitute longitudinal data about presence and pattern (Derrien et al., 2023; California Department of Resources Recycling and Recovery [CalRecycle], n.d.). Teams that read and document these traces are positioned to return to a known location with a specific referral, a named contact, and a realistic time and place rather than a general offer with no follow-up plan.
I also was struck by the evidence left behind throughout the city that someone had used a spot—be it in a park, near a walkway—for a temporary respite from the elements. There were signs all around if one knew where to look. A blanket nestled near a monument with an overhang was more obvious, but occasionally an area of park-soil near a stone wall would be clearer than its surroundings—someone had slept there. A few crushed cans alongside running water were a spot someone had taken a break before moving on. (Physician and StreetLife team member)
6. Evaluate follow-up: Systematic follow-up closes the loop between outreach encounter and sustained connection. Within 2 weeks of any initial contact or referral, teams conduct a brief re-contact to confirm whether the warm handoff was completed, identify barriers encountered, and document outcomes. This step is not punitive or evaluative of the individual; it is a structured quality-improvement routine designed to surface what worked and what failed. Team debriefs following each outreach session review a minimal indicator set aligned to BRIDGE steps: number of contacts initiated, warm handoffs completed, referrals accepted versus declined, and return interest documented. Evaluate follow-up transforms one-time service interactions into a learning system, embedding accountability into outreach practice without overburdening frontline teams.
Implications for Practice
Implement BRIDGE as a protocol, not a one-time service event. (a) Conduct outreach in pairs to protect safety and reduce unilateral decision-making. (Centers for Disease Control and Prevention, 2021) (b) Use autonomy-supporting norms of approach, consent, and naming to reduce perceived threat and protect dignity. (c) Standardize warm handoffs by documenting referral actions and barriers (transportation, communication access, eligibility friction). (d) Close the loop through brief, scheduled debriefs that translate field lessons into tool and process revisions. Prioritize a minimal indicator set aligned to BRIDGE steps (contacts, warm handoffs initiated, follow-ups completed, and return interest documented) to preserve feasibility. When a society intends to reduce “homeless” populations in their municipal area, several common tactics are employed, including sweeps (clearing living areas including dispossession and destruction of property, gentrification, legislation, and enactment of restrictive policies and laws), all of which serve the purpose of masking the issue of homelessness via an “out of sight, out of mind” approach (Bailey et al., 2017).
Implications for Policy
The BRIDGE framework highlights outreach to PEH as an essential public health function rather than an optional addition. Policy structures that treat outreach as discretionary or episodic limit what teams can do in the field regardless of skill or commitment. To sustain equity-oriented outreach, local and state policies should explicitly recognize outreach, navigation, and follow-up as core components of response to homelessness and safety-net systems, with stable funding streams to support them. BRIDGE makes visible how team roles, warm handoffs, and follow-up are shaped by policies that govern eligibility, reimbursement, and documentation. Policymakers can use BRIDGE to examine where current regulations create avoidable barriers, such as restrictive ID requirements, rigid visit definitions, or fragmented funding for medical, behavioral health, and social services. Alignment of payment and reporting requirements with BRIDGE steps would support outreach teams in prioritizing relationship building, rapid assessment of structural needs, and guided handoffs rather than maximizing billable encounters devoid of context. The framework also underscores the importance of shared accountability across sectors. Data collected at each BRIDGE step can inform policy decisions about where encampment responses, shelter policies, and service placement are helping or harming PEH. Policymakers should invite outreach teams, people with lived experience of homelessness, and community-based organizations into formal planning and oversight processes, using BRIDGE as a common language for what effective, equity-focus outreach entails. In this way, a policy can move beyond episodic initiatives toward sustainable structures that support consistent, humane, and structurally informed engagement with living without stable housing.
Limitations and Transferability
BRIDGE is a practice protocol developed to increase consistency, equity, and follow-through in street engagement, but transferability depends on local context. Implementation may be constrained by staffing capacity, safety considerations, limited referral infrastructure, and policy-driven displacement events that disrupt continuity and fracture trust. Teams should plan continuity strategies (partner coordination, alternative meeting locations, and rapid re-contact workflows) and document adaptations during debriefs to reduce protocol drift while maintaining fidelity to consent, dignity, and warm handoff expectations.
Conclusions
Street engagement is most effective when initial connections become sustainable via a relational approach. The BRIDGE framework operationalizes what many street teams already do in a repeatable, measurable system. Utilizing clear pathways to resources and connections, assessable metrics, and continuous, reflexive debriefing, partners can standardize outreach, increase trust, and improve quality of care for PEH. These steps are both scalable and transferable and provide a basis for sustainable quality improvement and evaluation.
Footnotes
Acknowledgements
We thank StreetLife Communities for their partnership in this effort.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.