
Abstract
Prenatal education programs are a key component of maternal and newborn health promotion. Although the use of digital platforms for prenatal education increased during the COVID-19 pandemic, evidence for their effectiveness remains limited. In addition, conventional programs often omit content addressing adverse pregnancy outcomes due to concerns about increasing maternal anxiety or worry. This quasi-experimental study aimed to (1) evaluate participants’ satisfaction and perceived acquisition of knowledge and health habits following a novel online prenatal education program delivered via Facebook, and (2) assess the impact of a novel session on managing complications during pregnancy and childbirth—preterm birth, newborn adaptation difficulties, and stillbirth—on participants’ levels of pregnancy-related anxiety and worry. Participants completed the State Anxiety Inventory and Cambridge Worry Scale (CWS) before and after the session on complications (N = 162), and the modified EDUMA2 questionnaire at the program’s conclusion (N = 93). High satisfaction (mean 9.01/10), improved self-rated knowledge and health habits, and high rates of recommendation were found. Post intervention, statistically significant reductions were observed in worry scores (CWS), particularly regarding fetal health, childbirth, and miscarriage, with no significant increase in anxiety levels (State-Trait Anxiety Inventory [STAI-S]). The online modality did not fully meet the social interaction needs of pregnant women and appeared to limit the participation of women’s partners and migrant women. Online prenatal education can effectively promote maternal health literacy and may effectively address sensitive topics such as pregnancy and childbirth complications. Future programs should integrate hybrid formats and strategies to reduce digital access barriers, especially among vulnerable populations.
Keywords
Background
The effectiveness of prenatal education programs, traditionally delivered using in-person group methodologies, for promoting maternal and newborn health (Hooper et al., 2025; Zaman et al., 2025) and for reducing fear of childbirth (Çankaya & Şimşek, 2021; Yörük & Acikgoz, 2023; Zaman et al., 2025) is widely recognized. However, their effects on other significant fears during pregnancy, such as the fear of miscarriage or concerns about fetal health, have received less attention (Mortazavi & Akaberi, 2016; Peñacoba-Puente et al., 2011). This may be because these programs do not sufficiently address concerns about fetal well-being (Artieta-Pinedo et al., 2017).
The COVID-19 pandemic catalyzed the rapid transition to online prenatal education, with many countries suspending in-person classes (Hartz et al., 2022). However, research on the effectiveness of online prenatal programs remains limited. Digital formats offer clear benefits—flexibility, convenience, and broader access (Shahid & Johnson, 2018)—yet questions remain about their ability to ensure engagement, peer interaction, and psychological well-being (Mousavi et al., 2022; Whitworth et al., 2024).
A specific gap in the literature is the lack of education about potential complications during pregnancy and childbirth (Avignon et al., 2023), such as preterm birth or stillbirth (Ellis et al., 2016; Gregory, 2012; Warland et al., 2020). These topics are often avoided in prenatal education programs due to concerns that they may increase maternal anxiety or worry (Ficquet et al., 2015; Warland & Glover, 2015). However, the limited available evidence contradicts this assumption (Pollock et al., 2020).
This study aims to fill these gaps by evaluating a comprehensive online prenatal education program delivered via Facebook during the pandemic in Spain. The program included a novel session on complications in pregnancy and childbirth, in addition to the usual content of the in-person prenatal education program offered by the regional health service promoting the study.
The study had two main objectives: to assess participants’ satisfaction with the online format and perceived acquisition of knowledge and health habits; and to examine the psychological impact of a complications-focused session on maternal anxiety and pregnancy-related worries, using validated instruments. This session, entitled “How to prevent and cope with complications during pregnancy and childbirth: premature birth, newborn adaptation difficulties, and stillbirth,” sought to support pregnant women in addressing their concerns about fetal well-being, as proposed by Artieta-Pinedo et al.’s (2017) framework for the development of perinatal education programs. The development of this innovative session was informed by the Transactional Model of Stress and Coping (Lazarus & Folkman, 1987), which conceptualizes psychological stress as a dynamic interaction between external stressors and perceived coping resources. In other words, supportive and informative content—delivered in a controlled, non-alarming way—can enhance coping with worry about potential adverse pregnancy outcomes.
The study also draws on two other conceptual frameworks. The Health Belief Model provides a rationale for assessing knowledge and behavioral change. According to this model, individuals are more likely to adopt healthy behaviors when they perceive susceptibility to a health issue, understand its seriousness, believe in the benefits of taking action, and perceive few barriers. Online education may help reduce barriers such as time, travel, and access to evidence-based information, thereby facilitating behavioral change (Alyafei & Easton-Carr, 2024). The Digital Health Equity Framework (Crawford & Serhal, 2020) provides a basis for interpreting participation patterns and limitations of digital interventions, which may unintentionally widen health disparities if they do not account for barriers such as low digital literacy, language limitations, or socioeconomic status. The integration of these complementary frameworks provides a solid conceptual basis for the evaluation of both the perceived and psychological effects of a real-world digital prenatal intervention.
Material and Methods
Design
A quasi-experimental, one-group, pre–post design (without randomization of the sample or the control group), based on the evaluation of an online prenatal education program created on a public Facebook profile. The program included a video session on pregnancy and childbirth complications.
Study Population, Sample and Recruitment
The study used a non-randomized convenience sampling technique. From July to September 2020, pregnant women and their partners were invited to participate in the online prenatal course and to complete the questionnaires. Recruitment was conducted via Facebook and directly through community midwives employed by the regional health service, who invited women—along with their partners, indirectly— to take part in the study during routine prenatal visits at 28 weeks’ gestation.
The following four inclusion criteria were established: being a pregnant woman (regardless of gestational age or parity) or the partner of a pregnant woman; residing in Spain; completion of the online informed consent form and questionnaires; and having watched at least half of the theoretical sessions—a cut-off point that is consistent with that used by the authors of the original EDUMA2 questionnaire. The exclusion criteria included technical, language, sensory, and/or cognitive difficulties that may have prevented access to, viewing of, or comprehension of the videos.
The primary reference population, to which the majority of the sample belonged during the study period, consisted of 2,200 pregnant women residing in the region of the promoting health service.
Description of the Educational Intervention
The online prenatal education program was hosted on a public Facebook page (“Midwives Cantabria”). The program covered the standard topics included in the “Prenatal Education Program of the Cantabria Health Service,” along with a novel session on preventing and coping with pregnancy and childbirth complications: prematurity, newborn adaptation difficulties, and stillbirth. Each of these potential complications was addressed by combining evidence-based prevention and emotional coping strategies (see Table A1, supplementary material).
The full program consisted of 53 short educational videos (approximately 30 minutes each), organized into thematic blocks: theory (38 videos), relaxation (12), and physical activity (3) (see Table 2). The videos were recorded with experienced midwives (n = 28) in the role of presenters. For a period of 8 weeks, one video was published daily and uploaded into a folder (album) corresponding to each thematic block, so that they could be viewed at any time. Participants were advised to watch the videos in the order that they were published and not to begin until they had reached 28 weeks’ gestation, although if participants began or started later than advised, they were not subsequently excluded from the study.
Instruments and Study Variables
The EDUMA2 questionnaire was used to evaluate the overall prenatal program and, through some of its variables—feeling of control and confidence and content evaluation—the session on pregnancy and childbirth complications. The emotional impact of the complication-focused session was evaluated using the Cambridge Worry Scale (CWS) and the State Anxiety Inventory (STAI-S).
EDUMA2 Questionnaire
The EDUMA2 questionnaire—administered at the end of the program—was developed and validated by Fernández y Fernández-Arroyo et al. (2014) to evaluate the quality of in-person prenatal education programs in Madrid (Spain). It consists of 56 variables covering: (1) sociodemographic data, (2) assessment of the program methodology, organization and content of the sessions (Likert-type scale 1–10), (3) satisfaction (Likert-type scale 1–10), (4) perception of acquired health habits (yes/no type answers), and (5) perception of acquired knowledge, feeling of control and confidence, and prenatal bonding (Likert-type scale 1–4). For the variables in the final group, participants retrospectively rated their perceptions prior to the intervention and also rated them again based on their perceptions after the intervention.
Some items that referred to an in-person methodology were modified to adapt them to our online methodology, with input from the original author (see supplementary material: modifications to the original EDUMA2 questionnaire). In our sample, the questionnaire demonstrated good internal consistency (Cronbach’s alpha = .974).
State-Trait Anxiety Inventory and Cambridge Worry Scale
The State-Trait Anxiety Inventory (STAI) consists of two 20-item scales (each yielding scores from 0 to 60) that measure state anxiety (transient emotional state, STAI-S) and trait anxiety (stable disposition; Buela-Casal et al., 2015). This study used STAI-S, as it measures anxiety levels induced by situational experiences or procedures.
The Cambridge Worry Scale (CWS), which has been validated in Spanish (Carmona-Monge et al., 2012), consists of 16 items—each rated on a scale from 0 to 5—assessing the extent and content of worries during pregnancy. In this study, three additional items were added to measure concerns about the adaptation of older children and the impact of the COVID-19 pandemic (2 items).
Data Collection Process
Through the Facebook profile, participants were invited at two specific time points to answer online questionnaires: (1) immediately before and after the session on pregnancy and childbirth complications, they completed the STAI-S and the CWS, preceded by sociodemographic variables; and (2) one month later, at the end of the program, they completed the modified EDUMA2 questionnaire. Participants could choose to complete only one set of questionnaires (either STAI-S/CWS or EDUMA2) or both (see supplementary material: Figure A1—Methodology and intervention flowchart).
The video session on pregnancy and childbirth complications and the STAI/CWS questionnaires were accessed through the same webpage link. Participants first completed the pre-session STAI and CWS, then watched the video, and finally completed the post-session STAI and CWS.
Statistical Analysis
Descriptive statistics (frequencies, means, standard deviations, medians, and interquartile ranges) were used for univariate analysis. Normality was assessed via the Shapiro–Wilk and Kolmogorov–Smirnov tests. Paired t-tests and Mann–Whitney U tests were conducted to assess pre-post changes and differences in the variable feeling of control and confidence based on whether participants watched the session on complications or not. Significance was set at p < .05. Effect size was calculated using Cohen’s d. Qualitative responses to open-ended questions were analyzed using summative content analysis (Hsieh & Shannon, 2005).
Ethical Considerations
The study was approved by the Research Ethics Committee of Cantabria (code 220.229). All participants provided informed consent electronically.
Results
Participant Characteristics
A total of 93 pregnant women completed the modified EDUMA2 questionnaire, and 162 participants (156 pregnant women and 6 partners) completed pre-post assessments (CWS/STAI-S) for the session on pregnancy and childbirth complications. The majority reported having access to the internet (98.9%) and being comfortable using Facebook (97.8%).
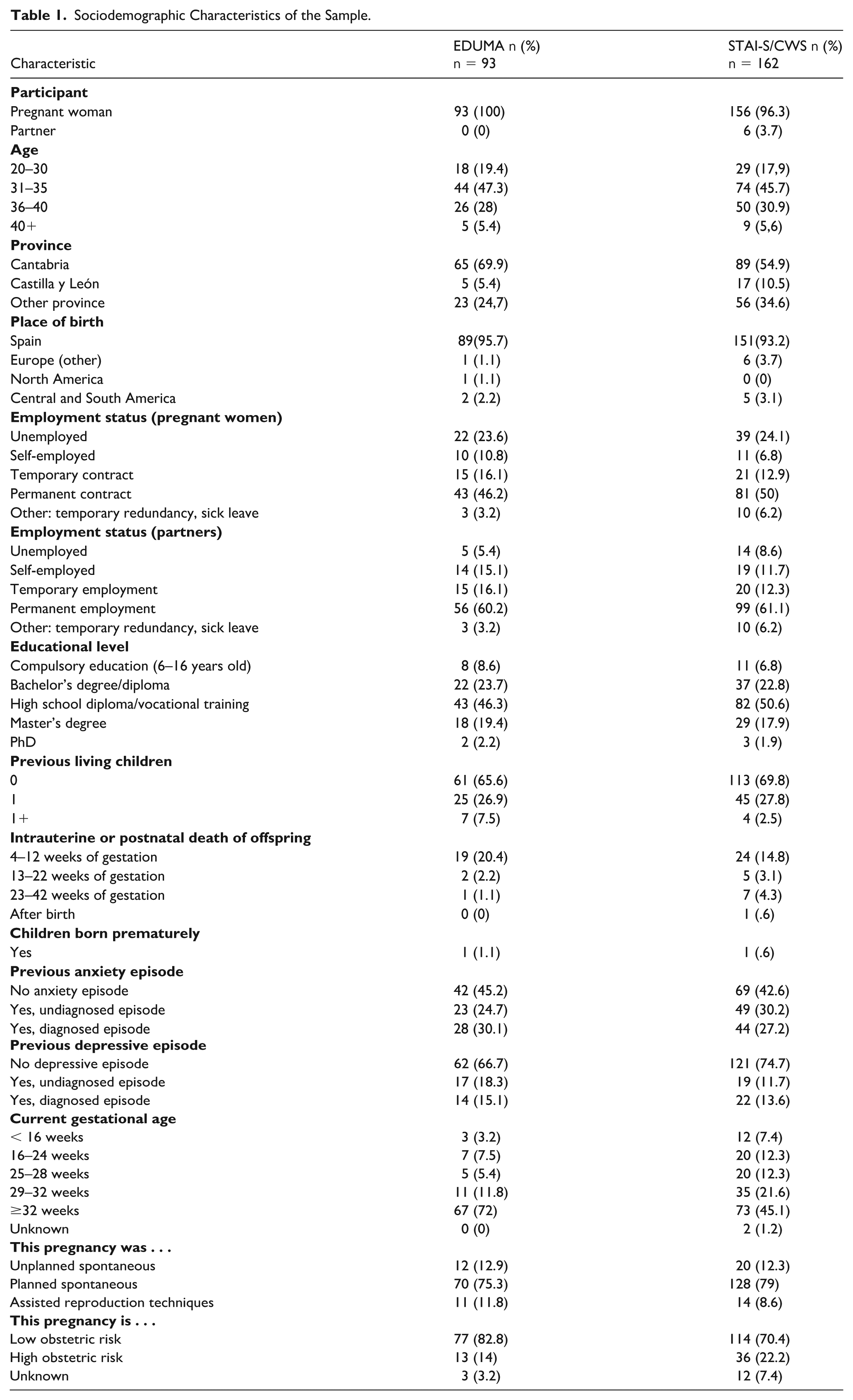
The sociodemographic and obstetric characteristics of the participants are provided in Table 1. The sample primarily consisted of women aged from 31 to 35 years, most of whom were in their first or second pregnancies. The majority had a university-level education and were in permanent or temporary employment. At the time of finalizing participation, gestational age ranged from 33 to 40 weeks.
Sociodemographic Characteristics of the Sample.
Overall Program Evaluation: EDUMA2 Questionnaire
Participants reported high levels of satisfaction with the program’s organization, structure, and content. With the exception of items related to opportunities for interaction with peers and professionals, all evaluated items received mean scores of at least 8 on a 10-point Likert-type scale. The novel session on pregnancy and childbirth complications received a similar average rating to the other sessions. Participants were also asked to identify which online sessions they found most and least beneficial. The sessions on childbirth and breastfeeding were considered the most helpful by 45.2% (n = 42) and 30.1% (n = 28) of participants, respectively. In contrast, relaxation techniques (9.7%, n = 9), physical exercise (10.7%, n = 10) and pregnancy-related content (11.8%, n = 11) were identified as the least helpful. Notably, no participants rated the session on complications as the least helpful, and 5.4% (n = 5) considered it the most beneficial. Table 2 presents the results of participants’ evaluations of the program’s organization, methodology and thematic content.
Assessment of the Program’s Organization, Methodology and Thematic Blocks (EDUMA2).
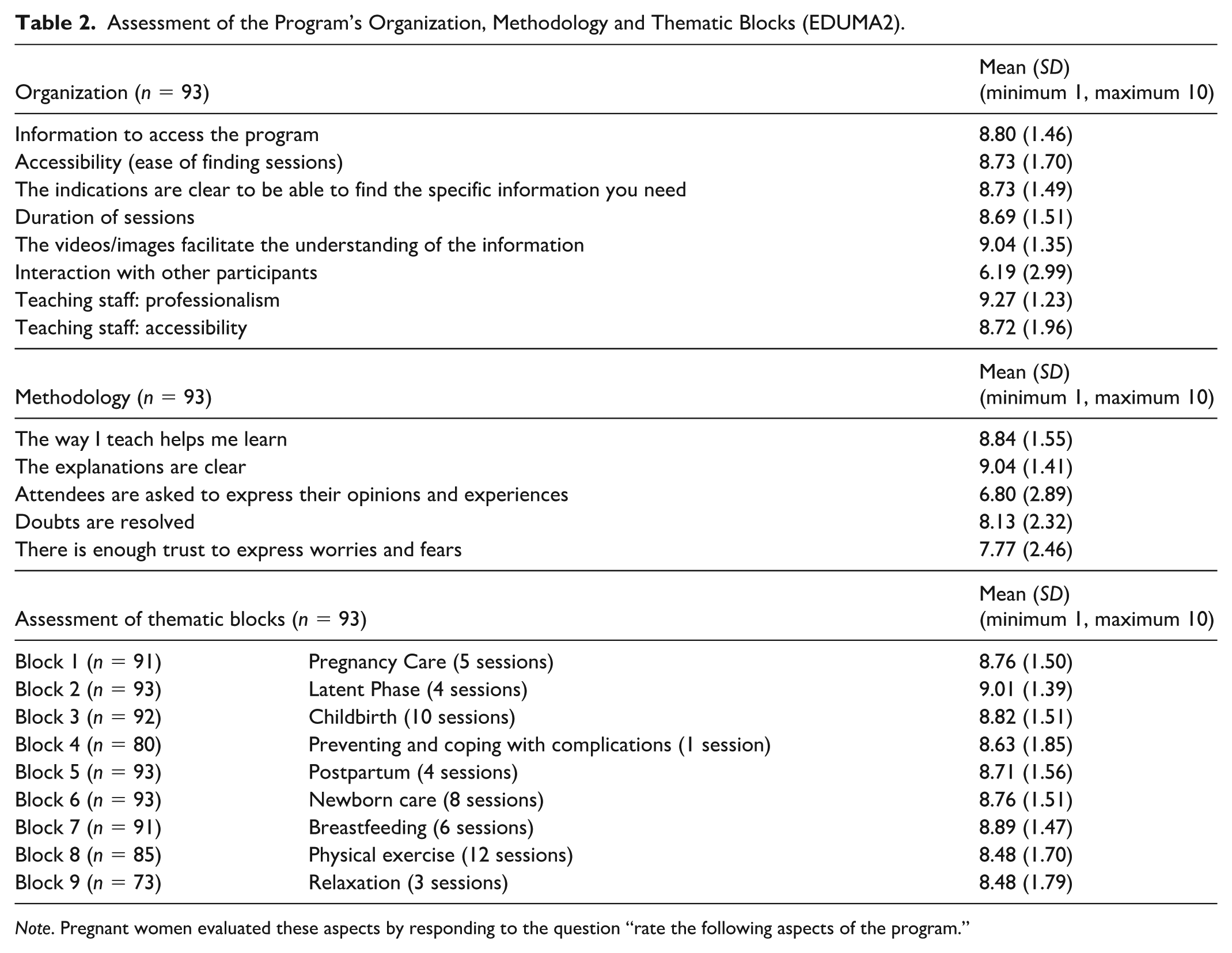
Note. Pregnant women evaluated these aspects by responding to the question “rate the following aspects of the program.”
Regarding self-reported changes in knowledge and health habits, statistically significant improvements were observed across all knowledge areas, with a large effect size. The most notable changes in perceived health habits concerned tobacco use, exercise, and pregnancy care. However, no perceived changes were reported for the substance use item. A statistically significant increase was also found in participants’ feelings of control and confidence, affective bonding with the baby, and intention to breastfeed. No significant difference in feeling of control and confidence was observed between attendees (n = 80) and non-attendees (n = 13) of the pregnancy and childbirth complications session (see Table 3, notes). Pre-post perceived changes for each item assessed in knowledge, health habits, feelings of control and confidence, affective bonding and intention to breastfeed are presented in Table 3.
Knowledge, Feeling of Control and Confidence, Affective Relationship With the Baby, Intention to Breastfeed and Health Habits (EDUMA2) a .
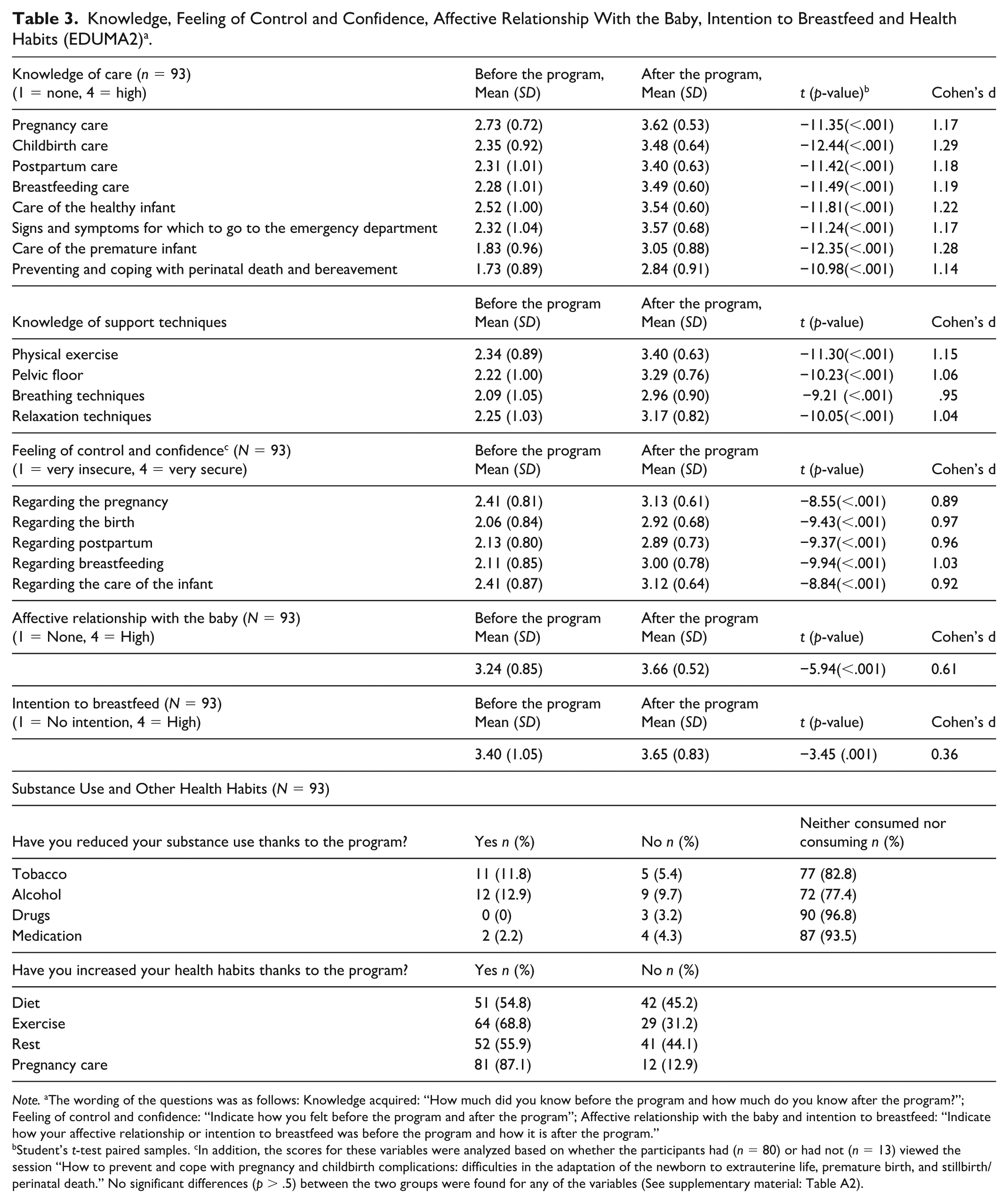
Note. aThe wording of the questions was as follows: Knowledge acquired: “How much did you know before the program and how much do you know after the program?”; Feeling of control and confidence: “Indicate how you felt before the program and after the program”; Affective relationship with the baby and intention to breastfeed: “Indicate how your affective relationship or intention to breastfeed was before the program and how it is after the program.”
Student’s t-test paired samples. cIn addition, the scores for these variables were analyzed based on whether the participants had (n = 80) or had not (n = 13) viewed the session “How to prevent and cope with pregnancy and childbirth complications: difficulties in the adaptation of the newborn to extrauterine life, premature birth, and stillbirth/perinatal death.” No significant differences (p > .5) between the two groups were found for any of the variables (See supplementary material: Table A2).
Overall satisfaction with the program was high (M = 9.01, SD = 1.46), with a very large majority of participants (97.8%) indicating they would recommend it to others. The main strengths of the online format were identified as flexibility of attendance times (88.2%, n = 82) and convenience (63.4%, n = 59). In response to two open-ended questions on the EDUMA2 questionnaire regarding the digital format—“Why would you recommend this program?” (n = 36) and “What do you think online education offers compared to in-person education?” (n = 17)—the most frequent responses included safety from COVID-19 (n = 8), access to a reliable repository of information when needed (n = 9), and the view that online formats should not replace in-person sessions (n = 15).
Evaluation of the Impact of the Pregnancy and Childbirth Complications Session on Anxiety and Worry
A total of 162 participants completed the STAI-S and CWS questionnaires before and after the session. Their sociodemographic characteristics are summarized in Table 1.
Worries During Pregnancy
The post-session mean total CWS score was significantly lower, with a moderate effect size. A similar result was observed for the three-scale items most closely related to the content of the pregnancy and childbirth complications session: possibility of a problem with the baby, giving birth, and the possibility of spontaneous miscarriage (see Table 4).
Pre- and Post-Session CWS and STAI-S Score and Difference.
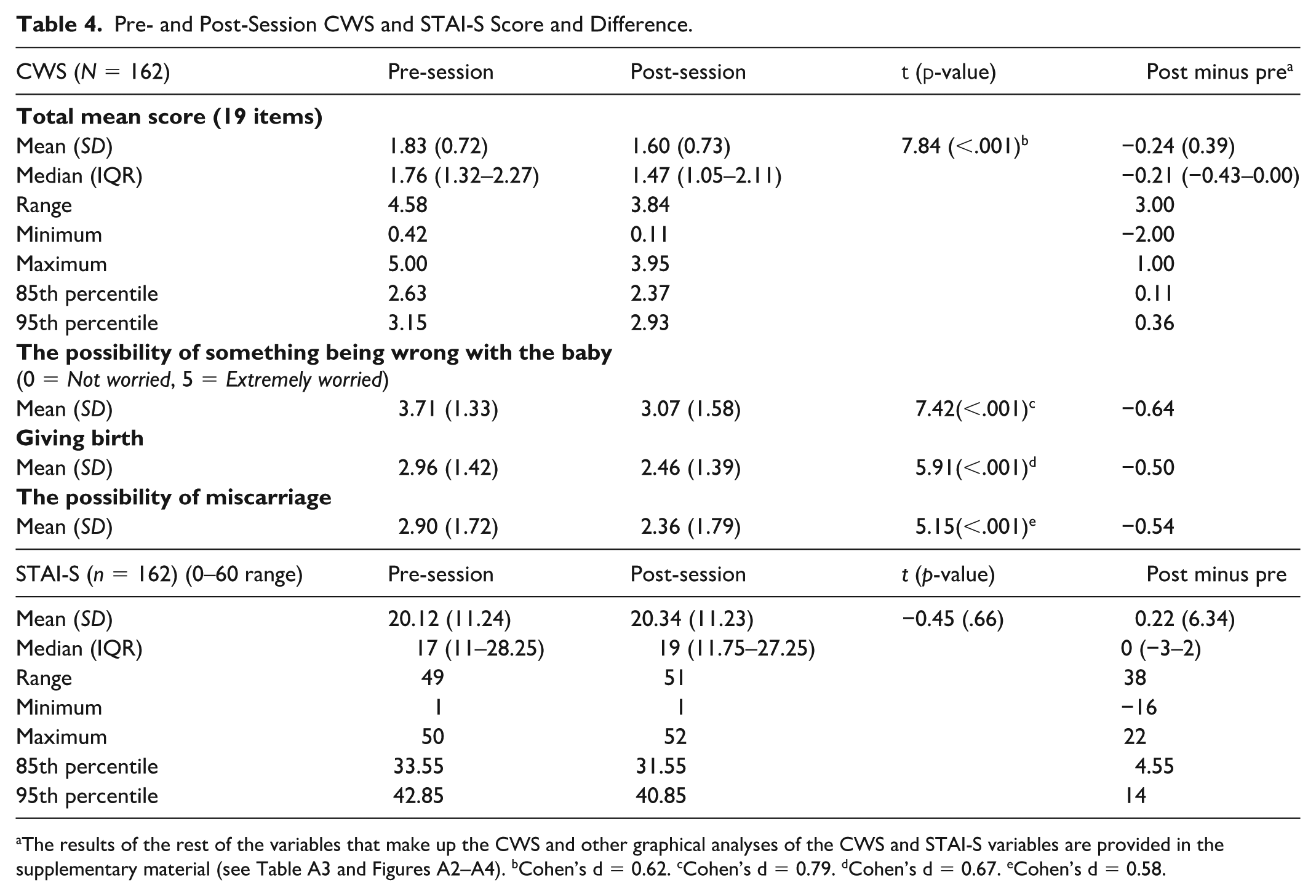
The results of the rest of the variables that make up the CWS and other graphical analyses of the CWS and STAI-S variables are provided in the supplementary material (see Table A3 and Figures A2–A4). bCohen’s d = 0.62. cCohen’s d = 0.79. dCohen’s d = 0.67. eCohen’s d = 0.58.
Furthermore, following the complications session, the mean total CWS score decreased for 72.2% of participants (n = 117), with 22.2% (n = 36) showing a reduction of 10% or more (≥0.5 points). In contrast, 23.5% (n = 38) experienced an increase, although only three participants had an increase of 10% or more (specifically, increases of .58, .63, and 1 point).
Anxiety
The mean STAI-S score was very similar in the pre- and post-session measures (see Table 4). After the session, the STAI-S score decreased for 48.1% of participants (n = 78), with 13% (n = 21) showing a reduction of 10% or more (≥6 points). In contrast, 41.4% (n = 67) experienced an increase, with 14.2% (n = 23) showing an increase of 10% or more. Notably, those whose scores increased by 10% or more had a lower mean pre-session score (M = 15.83; SD = 6.99) than the group whose scores decreased by 10% or more (M = 26.86; SD = 9.08). Finally, only 11 participants (6.8%) experienced an increase of 20% or more (≥12 points) in their STAI-S scores.
In addition, we analyzed the groups that might have a higher level of psychological distress or vulnerability—participants who reported previous episodes of anxiety and depression, intrauterine fetal death, or whose current pregnancy was high obstetric risk. The analysis found that these four groups had higher CWS and STAI-S scores in the pre-test than the sample as a whole. Overall, these groups experienced similar changes in anxiety and worries between the pre- and post-tests as the total sample (see Table 5).
Evaluation of the Impact of the Session on Pregnancy and Childbirth Complications in Subgroups With Possible Psychological Distress.
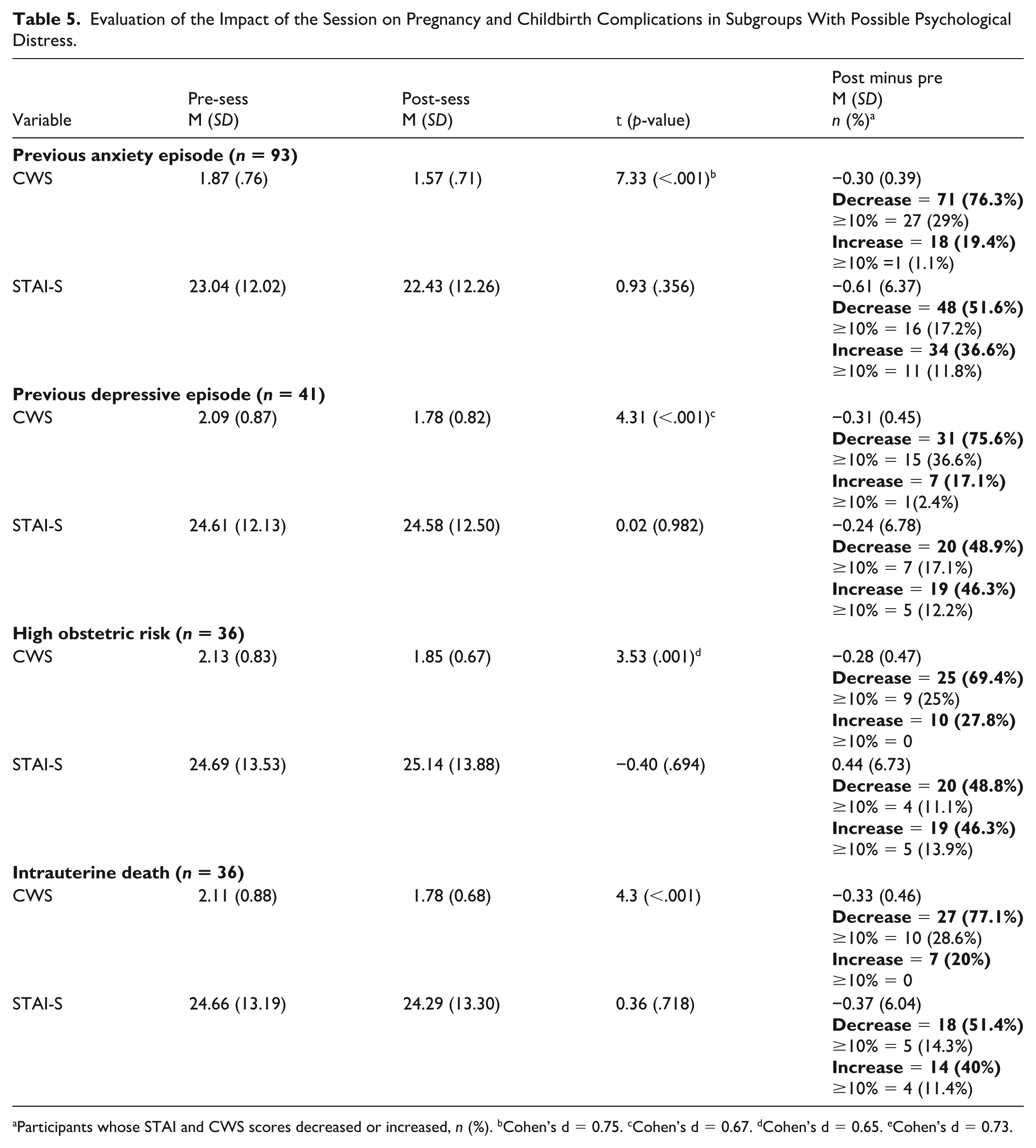
Participants whose STAI and CWS scores decreased or increased, n (%). bCohen’s d = 0.75. cCohen’s d = 0.67. dCohen’s d = 0.65. eCohen’s d = 0.73.
Discussion
This study evaluated a comprehensive online prenatal education program delivered via social media, as well as assessing the impact of a specific session on pregnancy and childbirth complications. The findings contribute to the growing body of evidence on digital health promotion strategies during pregnancy, particularly in contexts with limited access to in-person care, such as during the COVID-19 pandemic.
Consistent with previous literature on in-person prenatal education, participants reported high satisfaction with the overall program, along with improvements in perceived health knowledge and habits, prenatal bonding, and intention to breastfeed (Fernández y Fernández-Arroyo et al., 2014; Hooper et al., 2025; Zaman et al., 2025). Our program’s failure to engage women’s partners may have been due to increased precarious employment during the pandemic, as research suggests that they tend to seek prenatal information online (Hashmi & Cataletto, 2021). These outcomes support key tenets of the Health Belief Model, which posits that increasing access to evidence-based information and reducing structural barriers—such as time, work and distance—can facilitate the adoption of health-promoting behaviors during pregnancy (Alyafei & Easton-Carr, 2024).
The study participants rated the program’s methodology and organization highly, with the exception of items related to opportunities for peer and professional interaction. This is an important finding, as previous research has shown that pregnant women value prenatal classes that facilitate peer interaction and the development of social networks (Avignon et al., 2023; Spiby et al., 2022). The findings of our study are consistent with those of Whitworth et al. (2024). They found that an online methodology could enhance interaction, but that most participants still stated that it should not replace in-person sessions. They also found that flexibility of attendance times and the ability to revisit information were among the most valued aspects of an online program.
Despite the platform being open-access, low participation among migrant and other vulnerable social groups highlights the need to prioritize digital health equity. According to the Digital Health Equity Framework (Crawford & Serhal, 2020), digital interventions must take into account contextual factors such as language, literacy, connectivity, and cultural relevance. The study findings suggest that simply offering content online is not enough to ensure equitable access. Structural interventions—such as providing multilingual formats, targeted outreach through community networks, and digital literacy support—are essential to bridging the digital divide (Tuan et al., 2022; Whitworth et al., 2024).
Evaluation of the Session on Pregnancy and Childbirth Complications
Participants who watched the pregnancy and childbirth complications session rated it highly and reported an increase in feelings of control and confidence following the program, with no statistically significant difference compared to those who did not watch the session. The high rating likely reflects the session’s emphasis on providing information and tools to prevent and cope with a major source of fear during pregnancy: “the possibility that something will go wrong with the baby” (Peñacoba-Puente et al., 2011). Participants also reported an increased perception of knowledge gained regarding premature infant care, perinatal death, and grief. Spain’s premature birthrate (7.3%) and pregnancy and perinatal loss—around 80,000 women annually—underscore the importance of this type of program (Cassidy, n.d.; Ohuma et al., 2023).
Among the 162 respondents to the STAI and CWS, a statistically significant reduction in CWS scores was observed following the session. The STAI scores did not show statistically significant changes. Overall, more participants experienced a decrease in CWS/STAI scores than an increase, and only a small proportion showed increases of 10% or more. This subgroup had a lower mean pre-session STAI-S score than those whose anxiety decreased by 10% or more.
The findings of this study support the limited prior evidence and challenge the notion that information on complications such as stillbirth necessarily causes undue fear among pregnant women (Pollock et al., 2020; Warland et al., 2020; Warland & Glover, 2015). Moreover, elevated anxiety levels do not always indicate pathology; anxiety can stimulate reflection and behavioral change, thereby contributing to well-being. In fact, addressing anxiety through information, deliberation, and action may foster well-being more effectively than avoidance (Carmona-Monge et al., 2012; Kurth & Pihkala, 2022), an approach that is consistent with the Transactional Model of Stress and Coping (Lazarus & Folkman, 1987).
Limitations and Strengths
This study has several limitations that should be considered when interpreting the findings. First, it lacked a control group. Second, self-selection bias may have occurred, as participation was voluntary—likely overrepresenting more motivated or digitally literate individuals, while migrant and partner populations were underrepresented. Third, video view counts, or completion rates, were not linked to individual participants—limiting the ability to assess dose-response effects—and no shared identifier was used that would have allowed the data between both questionnaires to be linked. Finally, the program was implemented during the COVID-19 pandemic—a period marked by heightened uncertainty and restricted access to in-person care—which may have influenced participants’ stress levels and the perceived value of the intervention.
Despite these limitations, the study has several strengths. It evaluated a real-world intervention using validated instruments to assess satisfaction and psychological outcomes, adding methodological rigor. The study also introduced and evaluated a novel session on pregnancy and childbirth complications, an under-researched area of knowledge. Finally, the integration of behavior change theory, stress and coping models, and digital equity frameworks provides a comprehensive conceptual framework for interpreting results and guiding future practice.
Implications for Practice
Online prenatal education programs can effectively promote maternal knowledge and healthy behaviors, while also addressing emotionally sensitive topics such as pregnancy and childbirth complications. Health promotion practitioners should not avoid discussing such complications; rather, they should address them proactively within structured educational frameworks that provide clear information, prevention guidance, and coping strategies. When approached constructively, providing appropriate prevention and coping strategies, these discussions can enhance pregnant women’s sense of preparedness and psychological resilience.
The strengths of the online format included access to a repository of reliable information and flexibility of attendance times. However, it posed challenges for social interaction among pregnant women and for the participation of migrants and their partners. Health promotion practitioners should integrate hybrid models that combine the reach of online platforms with the relational benefits of in-person formats, incorporating specific strategies to engage underserved groups—such as linguistically and culturally adapted content, providing digital literacy support, and partnerships with community-based health workers to enhance access and trust.
Health promotion practitioners are also encouraged to integrate relevant theoretical frameworks into program design and evaluation—particularly those related to behavioral change, emotional coping, and social determinants of health—to strengthen the impact, equity, and inclusivity of digital maternal health promotion initiatives.
Implications for Research
Future researchers should employ more robust study designs, including randomized clinical trials, to strengthen the evidence base for online prenatal education programs. Longitudinal studies are also needed to assess whether observed improvements in knowledge, anxiety, or pregnancy-related worries are sustained over time.
Given the underrepresentation of migrant populations and partners in this study, future researchers should prioritize inclusive recruitment strategies and participatory approaches that engage these groups in the co-design of digital prenatal interventions.
Researchers should also explore how hybrid formats, combining online and in-person components, affect outcomes across diverse populations. Finally, further investigation is warranted into the impact of providing information on pregnancy and childbirth complications among diverse prenatal populations.
Supplemental Material
sj-docx-1-hpp-10.1177_15248399261459044 – Supplemental material for Evaluation of an Online Antenatal Education Program Implemented Through a Social Network
Supplemental material, sj-docx-1-hpp-10.1177_15248399261459044 for Evaluation of an Online Antenatal Education Program Implemented Through a Social Network by Manuela Contreras-García, Paula Alonso-González, Eva Caballero-Molano, Beatriz Corona-Gómez, Lara Del Valle-Clemente, Maria Ángeles Díez-Mateos, Andrea Díaz-Pérez, Maria Aránzazu Mouriz-Moleón, María Torres-Lacomba and Carmen Sarabia-Cobo in Health Promotion Practice
Footnotes
Acknowledgements
We are grateful to the midwives who made this online antenatal education program possible. To the Drs. Warland and Fernández and Fernández-Arroyo, the University of Cantabria, and the IDIVAL (a public health research institute) for their advice.
Author Contributions
All persons named as authors meet the requirements for authorship.
Manuela Contreras-García: Conceptualization, Methodology, Validation, Formal analysis, Investigation, Data Curation, Writing–Original Draft, Supervision, Visualization
Carmen Sarabia-Cobo: Resources, Conceptualization, Methodology, Validation, Formal analysis, Investigation, Writing–Review and Editing, Supervision.
Paula Alonso-González, Eva Caballero-Molano, Beatriz Corona-Gómez, Lara Del Valle-Clemente, Mª Ángeles Díez-Mateos, Andrea Díaz-Pérez, M. Aranzazu Mouriz-Moleón, María Torres-Lacomba: Conceptualization, Methodology, Formal analysis, Investigation, Writing–Review and Editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.