
Abstract
Objectives:
This study evaluated the Fathers Empowered to Learn, Lead, and Achieve Success (FELLAS®) fatherhood program. Outcomes commonly used in fatherhood program evaluations align with key social determinants of health (SDOH) identified in Healthy People 2030, including economic stability, family functioning, and social relationships. Examining these outcomes provides insight into how fatherhood programs may influence upstream determinants of health behavior and long-term well-being.
Methods:
Fathers participated in a 35-hour, multi-component intervention designed to improve life skills, parenting practices, relationship functioning, and economic stability. The analytic sample included 216 fathers who completed questionnaires at pretest, posttest, and six-month follow-up. Outcomes included five multi-item self-report scales (attitudes toward finances, parenting skills, father involvement, conflict resolution, and communication with partner) and two employment indicators (unemployment and full-time employment). Qualitative focus groups were conducted to assess participant experiences and perceived skill development.
Results:
Participants demonstrated statistically significant improvements from pretest to posttest across all seven outcome measures. Improvements were sustained at six-month follow-up for six outcomes, with attenuation observed for father involvement. Significant reductions in unemployment and increases in full-time employment were observed and maintained over time. Qualitative findings supported these results, with participants reporting improvements in parenting, relationships, communication, and employment-related behaviors.
Conclusion:
FELLAS demonstrated meaningful improvements in outcomes aligned with SDOH domains. These findings suggest that fatherhood programs may contribute to improved family and population health through upstream pathways. Results from this descriptive evaluation provide a foundation for more rigorous future research examining causal effects and mechanisms of change.
Keywords
Introduction
Responsible fatherhood programs are a common strategy for strengthening family well-being by improving parenting skills, father–child involvement, relationship functioning, and economic stability. These domains are recognized as key social determinants of health (SDOH), as defined by Healthy People 2030, which include the conditions in which people are born, live, learn, work, and interact that shape health across the lifespan. Because employment stability, stress, and family functioning are upstream drivers of health, evaluations of fatherhood programs can inform health promotion strategies aimed at reducing inequities. Framing fatherhood programs within an SDOH perspective highlights their potential to influence health outcomes indirectly by strengthening these foundational conditions.
The Office of Family Assistance (OFA) (2024) Responsible Fatherhood initiative targets fathers aged 18 years or older who have at least one child aged 24 years or younger. This includes community fathers—those residing in the community who may or may not live with their children—as well as fathers who are currently or previously incarcerated. Program models vary, but most combine relationship and parenting education with case management and referrals to wraparound supports. As implemented, these programs address multiple SDOH domains, including economic stability, social and community context, and family functioning.
Although the rationale for fatherhood programming is strong, evaluation findings have been mixed. A growing body of research has examined the effectiveness of responsible fatherhood programs. Meta-analytic findings suggest that these programs can produce statistically significant improvements in parenting and co-parenting outcomes, although effect sizes are typically small (Holmes et al., 2010, 2020). Evidence for employment and economic outcomes has been less consistent. Some randomized controlled trials have reported modest improvements in relationship functioning, parenting behaviors, and family outcomes (Cowan et al., 2022; Kohl et al., 2022), while others have found limited or no effects on selected outcomes (Kim & Jang, 2023; Manno et al., 2021). These mixed findings highlight both the promise of fatherhood programs and the need for continued research to better understand when and how these programs produce meaningful change.
In addition, most evaluations of fatherhood programs have focused on proximal program outcomes without explicitly situating these outcomes within a broader health promotion framework. As a result, the potential contribution of fatherhood programs to improving social determinants of health—and, by extension, population health—has not been fully examined. More research is needed to document outcomes over time, incorporate multiple data sources, and clarify the pathways through which fatherhood programs influence family well-being and health.
The FELLAS project was funded as a descriptive evaluation via a grant to the Partnership for Maternal & Child Health of Northern New Jersey, during the 5-year Fatherhood F.I.R.E. (Fatherhood—Family-focused, Interconnected, Resilient, and Essential) grant cycle, which ended September 30, 2025. Descriptive evaluations serve as important pilot studies, allowing programs to assess initial outcomes, identify implementation strengths and challenges, and justify future investment in more rigorous designs.
Conceptual Framework
In the present study, improvements in parenting, relationship functioning, and economic stability are conceptualized as upstream determinants that influence stress, health behaviors, and long-term physical and mental health outcomes. Economic stability may reduce financial strain and improve access to resources; positive parenting practices may support child development and long-term health trajectories; and improved relationship functioning may reduce stress and promote emotional well-being. This framework aligns with a social determinant of health perspective, in which interventions targeting these domains contribute to improved family and population health.
This article reports findings from the FELLAS end-of-project evaluation conducted in Essex County, New Jersey. Using a one-group pretest, posttest, and 6-month follow-up design, we examined changes in five self-report skill domains: attitudes toward finances, perceived parenting skills, father involvement, conflict resolution, and communication with partner; and two employment-focused outcomes. These outcomes were selected because they represent key domains associated with social determinants of health. To complement quantitative findings and inform practice, we analyzed focus group feedback to capture fathers’ perspectives on program experiences and perceived skill gains. Together, these findings provide applied evidence on outcomes central to fatherhood programming and relevant to health promotion.
Methods
Intervention
FELLAS is a 35-hour fatherhood intervention delivered over 15 weeks (2–3 hours per week). The program includes three components: (a) 24/7 Dad® (24 hours), a father-focused parenting curriculum; (b) Couples Communication 1 (5 hours), a relationship-strengthening curriculum; and (c) economic stability services (6 hours).
Fatherhood Program Specialists (FPSs) are trained staff responsible for participant recruitment, facilitation of group sessions, and provision of case-management services. FPSs were required to have a minimum of an associate’s degree and at least 2 years of experience in case management and group facilitation. Preference was given to candidates holding bachelor’s degrees in health education, social work, or related fields.
Participant Recruitment
Five weeks prior to each cohort, FPSs recruited participants through street outreach, in-person outreach at child care centers and schools, referrals from community partners, and word-of-mouth from prior program graduates. Eligible participants were fathers aged 18 years or older with at least one child aged 24 years or younger. Recruitment was supported by the implementing agency’s long-standing presence in Essex County, New Jersey. Street outreach involved direct, in-person engagement with potential participants in community settings such as neighborhoods, public spaces, and local service locations, with the goal of informing individuals about the program and encouraging enrollment. Each FPS recruited and facilitated programming for approximately 12 fathers per cohort and also served as their case manager. Two cohorts were implemented annually, with a target enrollment of 120 participants per year. Due to staff turnover, the planned number of FPSs was not always achieved.
Measures
Consistent with a social determinant of health framework, measures were selected to capture changes in key domains related to economic stability, parenting, and relationship functioning. Participants completed a self-report questionnaire at pretest, posttest, and 6-month follow-up using Qualtrics survey software.
The evaluation assessed seven outcomes:
Attitudes toward finances (6 items; α = .85)
Perceived positive parenting skills (12 items; α = .91)
Father involvement (3 items; α = .53)
Conflict resolution skills (6 items; α = .82)
Communication with partner (10 items; α = .48)
Employment status (unemployment)
Employment status (full-time employment)
The first five outcomes were assessed using multi-item Likert-type scales. Employment status was assessed using a single multiple-choice item.
Qualitative Data Collection
Two focus groups were conducted to gather qualitative feedback on participants’ perceptions of the program and their application of learned skills. One group included fathers who had recently completed the program, and the second included fathers who had completed the program approximately 6 months earlier. Participants were recruited by FPSs and received a $25 gift card for participation.
Each focus group lasted approximately 1 hour and followed a structured eight-question guide. Sessions were not audio- or video-recorded to protect participant privacy; instead, an experienced assistant recorded detailed notes. Responses were analyzed using inductive coding to identify emergent themes, followed by axial coding to organize themes into broader categories.
Procedures
Participants completed three questionnaires. The first questionnaire was completed immediately prior to the program (pretest). The second one was completed at program completion (posttest). The third questionnaire was completed at 6-month follow-up.
Data Analysis
Frequency distributions were used to summarize participant characteristics. Means and standard deviations were calculated for non-employment outcomes. Repeated-measures analyses of variance (ANOVA) were conducted to test changes across time, with post hoc pairwise comparisons. Chi-square analyses were used to assess changes in employment status from pretest to posttest and follow-up.
Results
Quantitative Results
Participant characteristics at pretest are presented in Table 1. At pretest, participants had a mean age of 36.5 years, and 29% were unemployed. The sample was 86% Black, 2% White, and 12% other races. Additional characteristics are also presented in Table 1. A total of 370 participants completed the pretest questionnaire. The analytic sample consisted of 216 participants with complete pretest, posttest, and 6-month follow-up data. Table 1 also presents characteristics of the 154 participants excluded from the analytic sample due to incomplete data, allowing comparison between included and excluded participants.
Comparison of Baseline Characteristics Between Analytical and Excluded Samples.
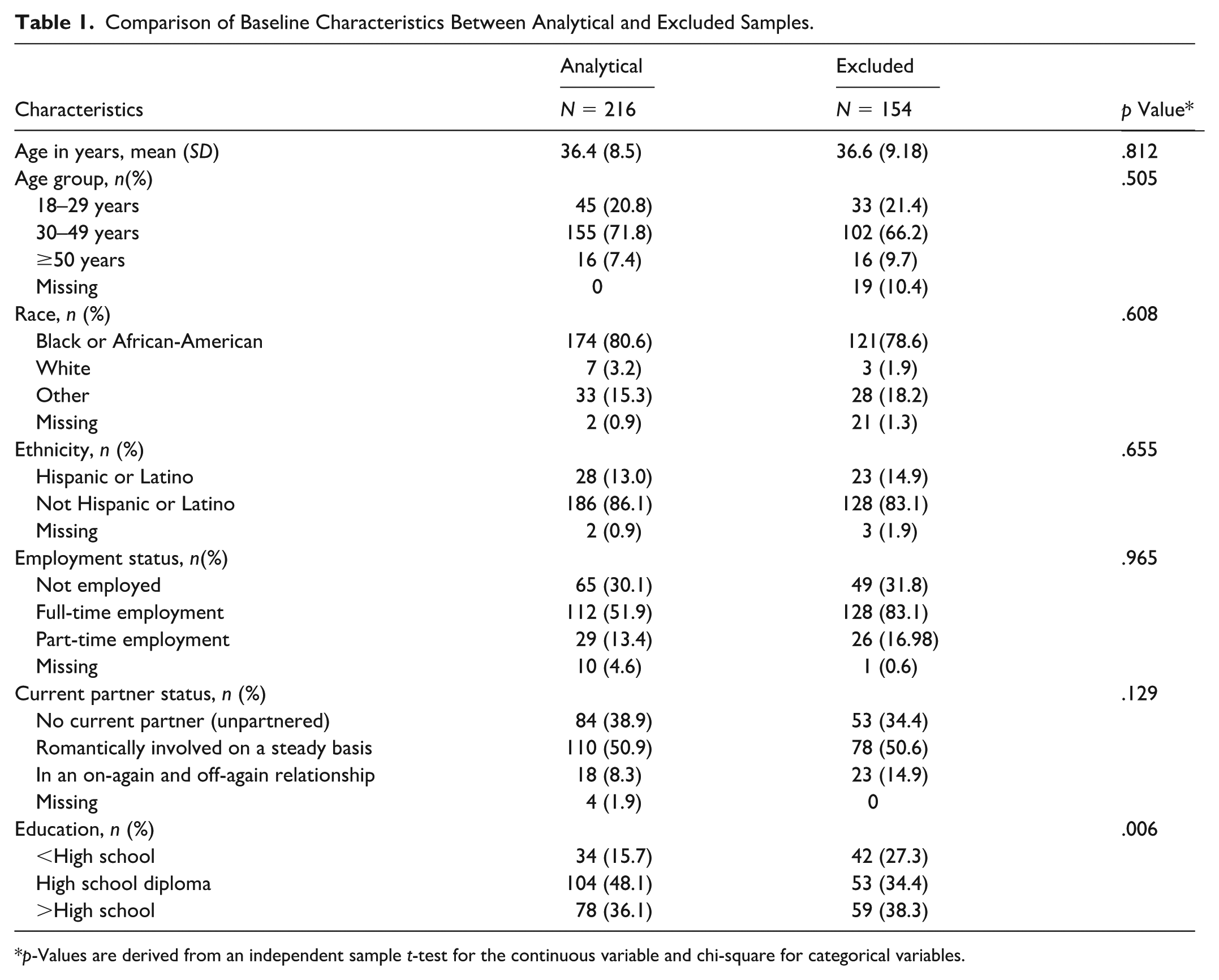
p-Values are derived from an independent sample t-test for the continuous variable and chi-square for categorical variables.
Repeated-measures ANOVA revealed statistically significant changes over time for all five non-employment outcomes (p < .05; see Table 2). Pairwise comparisons indicated significant improvements from pretest to posttest and from pretest to 6-month follow-up for attitudes toward finances, parenting skills, conflict resolution, and communication with partner. Improvements in father involvement were significant at posttest but were not sustained at follow-up (see Table 3).
Improvement After Intervention on Non-Employment Outcome Measures.
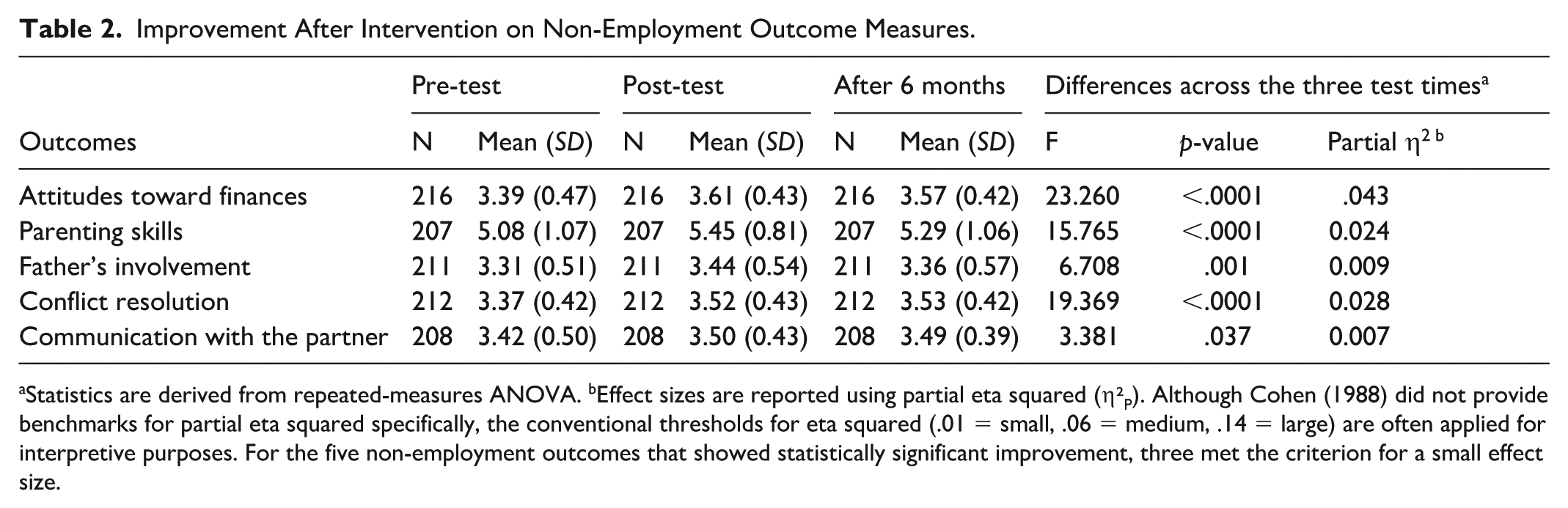
Statistics are derived from repeated-measures ANOVA. bEffect sizes are reported using partial eta squared (η²P). Although Cohen (1988) did not provide benchmarks for partial eta squared specifically, the conventional thresholds for eta squared (.01 = small, .06 = medium, .14 = large) are often applied for interpretive purposes. For the five non-employment outcomes that showed statistically significant improvement, three met the criterion for a small effect size.
Pairwise Comparisons Before and After Intervention.
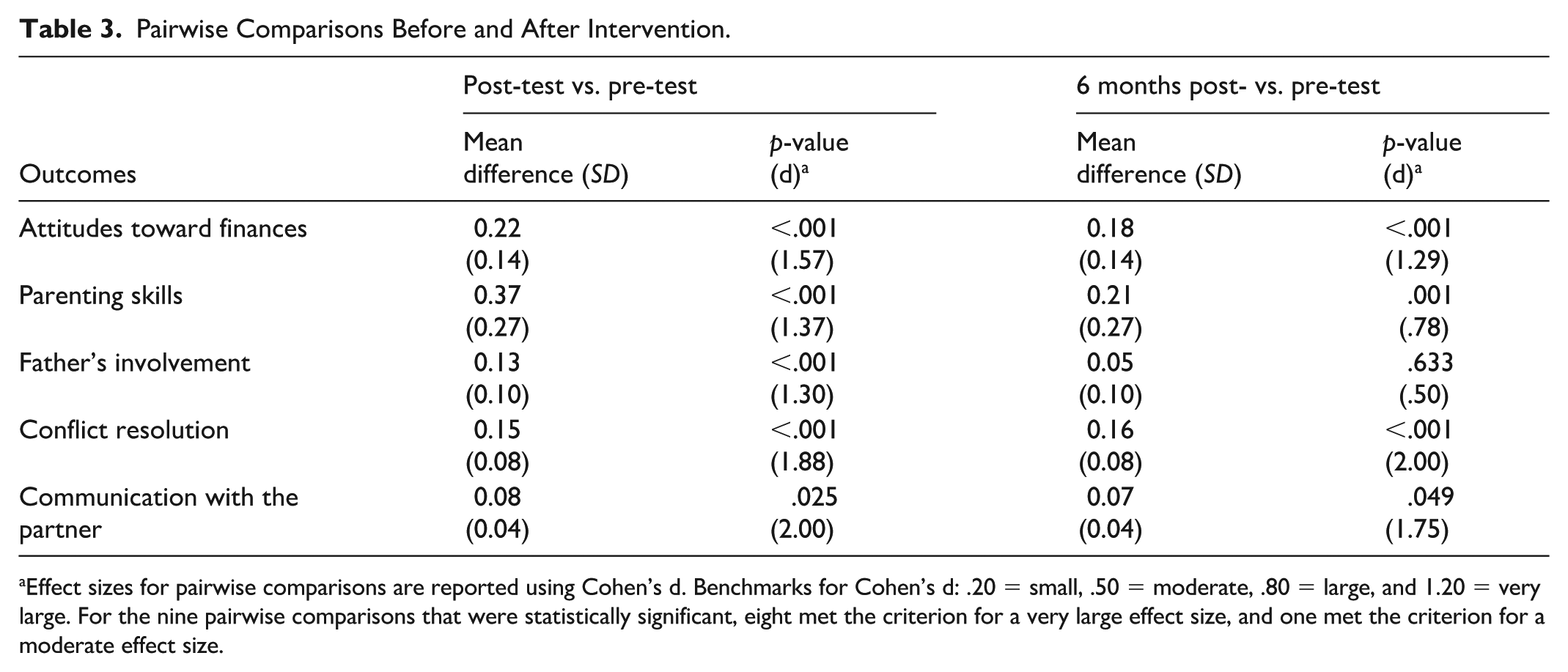
Effect sizes for pairwise comparisons are reported using Cohen’s d. Benchmarks for Cohen’s d: .20 = small, .50 = moderate, .80 = large, and 1.20 = very large. For the nine pairwise comparisons that were statistically significant, eight met the criterion for a very large effect size, and one met the criterion for a moderate effect size.
To examine whether improvements varied by demographic characteristics, repeated-measures analyses were conducted by age group, education level, and employment status. With one exception (conflict resolution among participants aged 18–29), no significant within- or between-group differences were observed.
Changes in employment outcomes were examined using chi-square analyses. From pretest to posttest, there were significant reductions in unemployment (p = .00032, φ = .177) and increases in full-time employment (p = .0014, φ = .121). These gains were sustained at 6-month follow-up, including reductions in unemployment (p < .00001, φ = .233) and increases in full-time employment (p = .00031, φ = .178) (see Table 4).
Changes in Employment Status at Different Stages of Intervention.
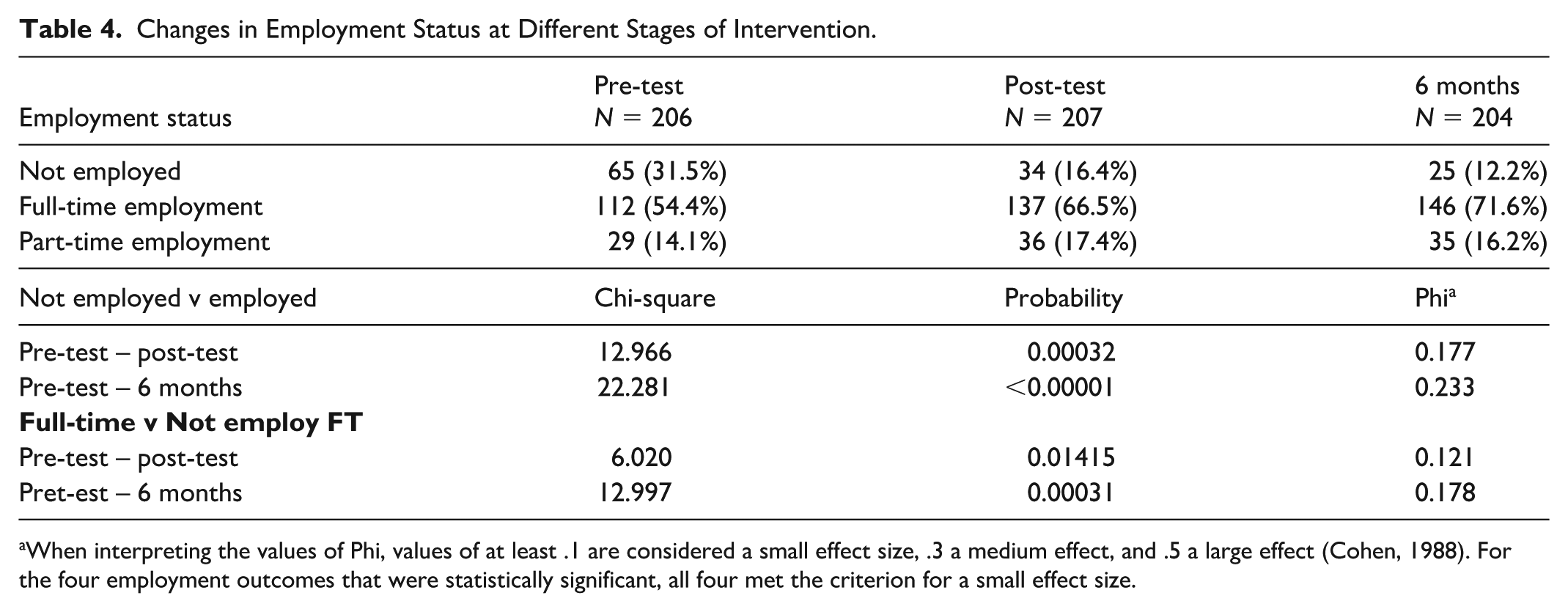
When interpreting the values of Phi, values of at least .1 are considered a small effect size, .3 a medium effect, and .5 a large effect (Cohen, 1988). For the four employment outcomes that were statistically significant, all four met the criterion for a small effect size.
Qualitative Results
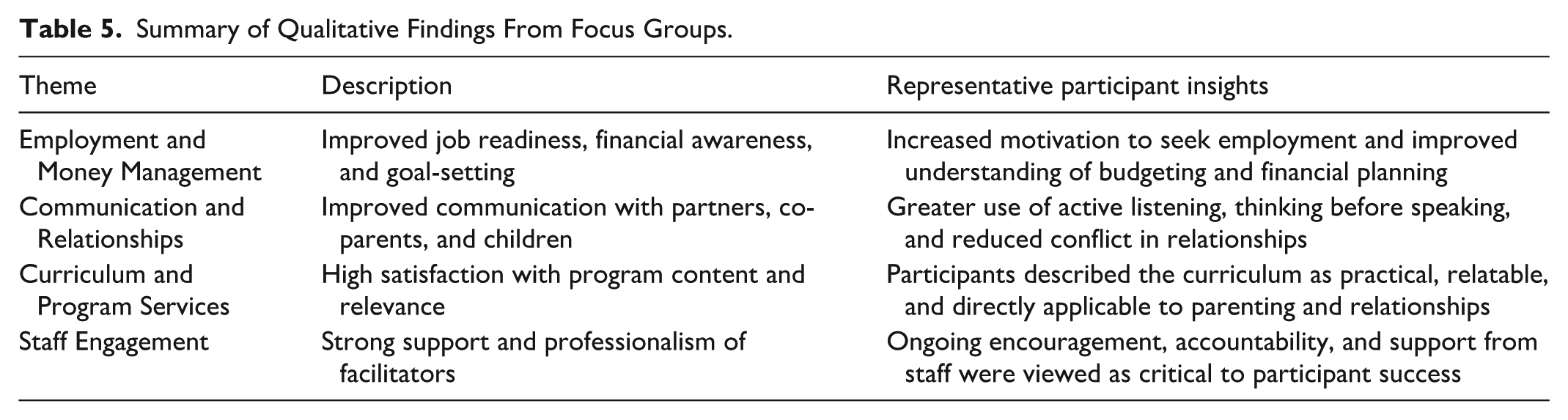
Four themes emerged from focus group analyses. These included (a) employment and money management; (b) communication and relationships; (c) curriculum and program services; and (d) staff engagement.
Participants described improvements in job readiness, financial management, parenting practices, anger management, and relationships with partners, co-parents, and children. They expressed strong appreciation for the curriculum content and emphasized the importance of staff professionalism and ongoing support.
Participants in the delayed focus group highlighted the value of peer relationships formed during the program and noted that continued contact with staff after program completion was particularly meaningful. Several participants emphasized that sustained improvement required intentional, ongoing application of learned skills in daily life. These qualitative results are summarized in Table 5.
Summary of Qualitative Findings From Focus Groups.
Integration of Quantitative and Qualitative Findings
Qualitative findings aligned closely with quantitative improvements observed across multiple domains. Fathers described using active listening, de-escalation strategies, and non-punitive parenting techniques, which they perceived as improving communication and reducing conflict. Participants also reported improved communication with children and co-parents. These qualitative insights reinforce observed improvements in parenting skills, conflict resolution, and employment outcomes.
Discussion
The purpose of this pilot study was to evaluate the effects of the FELLAS fatherhood program. Specifically, the study first examined changes in seven outcome variables. Second, the study assessed whether pretest–posttest improvements were maintained at 6-month follow-up. Finally, the study explored whether changes varied by demographic characteristics.
All five non-employment outcomes showed statistically significant improvement, and four of the five were sustained at follow-up. In addition, significant reductions in unemployment and increases in full-time employment were observed and maintained over time. These outcomes correspond to key social determinants of health, including economic stability, family functioning, and social relationships. Improvements in these domains represent plausible pathways through which fatherhood programs may influence both short- and long-term physical and mental health outcomes.
The relative consistency of findings across demographic groups suggests that, to the extent improvements can be attributed to the program, FELLAS was broadly effective across participant subgroups. Qualitative findings further support these results, with participants reporting meaningful improvements in parenting, relationships, and employment-related behaviors.
Consistent with prior research, fatherhood programs tend to produce modest effects overall. However, the magnitude of improvements observed in this study is comparable to or greater than those reported in prior evaluations. These differences may reflect variation in program design, dosage, population characteristics, or measurement sensitivity.
To provide greater insight into how the FELLAS program influenced specific domains aligned with social determinants of health, findings are examined by outcome area below:
Attitudes Toward Finances
FELLAS participants showed improvement in attitudes toward finances from pretest to posttest and from pretest to follow-up. This low-income group of fathers was highly motivated to improve their economic situation. Staff reported that, particularly in financial education sessions, they attempted to meet the individual needs and interests of participating fathers.
From an SDOH perspective, attitudes toward finances can be viewed as an aspect of financial health and economic stability. Weida et al. (2020) identified financial health as an important social determinant of health, with strong associations to both physical and mental health outcomes, including self-rated health and symptoms of depression.
Perceived Parenting Skills
FELLAS participants showed improvement in perceived parenting skills. A motivating factor for many fathers was the opportunity to spend more time with their children, which they believed depended in part on demonstrating improved parenting to the child’s mother.
Previous research on parenting outcomes in fatherhood programs has been mixed. Some studies report improvements regardless of intervention type (Kohl et al., 2022), while others report limited or no effects (Kim & Jang, 2023; Manno et al., 2021). Meta-analytic findings indicate small but statistically significant effects for parenting and co-parenting outcomes (Holmes et al., 2020).
Improved parenting practices are also associated with downstream health outcomes. Marmot (2016) suggests that enhancing parenting skills may improve child development, leading to higher educational attainment, economic stability, and healthier lifestyles. These pathways illustrate how parenting interventions may contribute to long-term population health.
Father Involvement
FELLAS participants showed an increase in father involvement from pretest to posttest, followed by attenuation at 6 months. Prior research on responsible fatherhood programs has generally found small but statistically significant short-term improvements in father involvement, although longer-term effects are less consistently documented (e.g., Holmes et al., 2020), making the pattern observed in the present study unsurprising.
Father involvement is widely recognized as important to children’s well-being. This includes physical, cognitive, emotional, and social outcomes (Lansford, 2021; Osborne et al., 2014), as well as health-related outcomes (Garfield & Isacco, 2011; Yoon et al., 2018).
Conflict Resolution
FELLAS participants demonstrated improved conflict resolution skills at posttest that were maintained at 6-month follow-up. While some large-scale programs (e.g., Building Strong Families) have found no long-term differences in conflict behaviors (Wood et al., 2012), other studies have reported sustained improvements (Cowan et al., 2022).
Conflict resolution interventions have also been associated with reductions in violence (Harmon-Darrow, 2022). Such findings suggest that improvements in these skills may confer both physical and emotional health benefits for fathers, partners, and children.
Employment
FELLAS participants showed a decrease in unemployment and an increase in full-time employment. Although job training was not a primary component of the program, emphasis on responsibility and economic support for children may have contributed to these outcomes. Through case management, participants were also referred to job training programs when appropriate.
Employment is a central social determinant of health, and returning to work has been associated with improved physical and mental health outcomes (Rueda et al., 2012). Additional research indicates that employment can enhance financial security, provide a sense of purpose, and promote healthier behaviors.
Communication With Partner
Communication with the partner improved significantly from pretest to posttest and from pretest to follow-up. Improved communication has been associated with reduced stress and better physical and mental health among adults (Robles et al., 2014).
Improved couple communication may also benefit children by supporting effective parenting and stronger parent–child attachment. These factors are both linked to better social and emotional adjustment (Neppl et al., 2019).
Summary and Integration of Findings
Taken together, these findings indicate that the FELLAS program produced improvements across multiple domains that function as key social determinants of health, including economic stability, parenting practices, and relationship functioning. While the magnitude and sustainability of effects varied by outcome, the overall pattern suggests that multi-component fatherhood programming can influence family well-being through multiple, reinforcing pathways. The alignment between quantitative results and qualitative participant experiences further strengthens confidence in these findings, as fathers described applying skills related to communication, conflict management, and goal-setting in their daily lives. Viewed collectively, these results support the potential for fatherhood programs to contribute to broader health promotion efforts by addressing upstream determinants that shape long-term health and well-being.
Limitations
This descriptive study has several limitations. First, all measures were based on self-report data, and no external sources were used to corroborate participant responses. Reported improvements may reflect true change or may be influenced by social desirability bias. Second, the study did not include a control group, limiting the ability to attribute observed changes directly to the intervention. Third, focus group participants were volunteers and may not be representative of the full sample.
Finally, the analytic sample (n = 216) included only participants who completed all three assessments, raising concerns about attrition and generalizability. Although a 6-month follow-up was included, longer-term effects remain unknown. Despite these limitations, findings from this pilot study suggest that the FELLAS program warrants further evaluation using more rigorous designs.
Implications for Practice
Findings from this evaluation suggest several important considerations for the design and implementation of responsible fatherhood programs, with direct relevance for health promotion practice. First, the consistent pattern of improvement across multiple domains—including parenting skills, conflict resolution, communication, and employment—indicates that multi-component fatherhood programs can yield meaningful short- and medium-term benefits, even in the absence of explicit health-focused curricula. Because these domains align with key social determinants of health (SDOH), programs that integrate relationship education, parenting support, and economic stability services may serve as effective platforms for addressing upstream drivers of health among fathers and families.
Second, the relative consistency of effects across age, education, and employment subgroups suggests that programs such as FELLAS can be implemented broadly without extensive demographic tailoring. For community-based organizations operating with limited resources, emphasis on facilitator quality, culturally responsive delivery, and individualized case management may be more critical than subgroup-specific adaptations.
Third, the attenuation of father involvement at 6-month follow-up highlights the importance of post-program reinforcement strategies. Booster sessions, peer support opportunities, and continued staff contact may help sustain gains over time. Qualitative findings suggest that ongoing relationships with staff and peers are particularly valuable and may represent an underutilized mechanism for maintaining behavior change.
Fourth, improvements in employment outcomes—despite the absence of formal job training—suggest that strengthening motivation, goal-setting, and personal responsibility may indirectly support workforce engagement. Strengthening partnerships with workforce development agencies and embedding structured referral processes within case management may further enhance economic stability, a key SDOH domain.
Finally, sustained improvements in partner communication, along with qualitative reports of improved relationships with children and co-parents, underscore the central role of relational skills in family well-being. Although FELLAS was not designed as a health promotion intervention, the observed improvements in these domains are closely linked to physical and mental health outcomes. These findings suggest that fatherhood programs may serve as natural entry points for integrating health promotion content, such as stress management, healthy coping, and preventive health behaviors. Health promotion practitioners should consider fatherhood programs as strategic settings for engaging fathers, a population that has historically been underrepresented in health promotion efforts.
Implications for Research
This study evaluated the FELLAS fatherhood program by examining changes in participant outcomes from pretest to posttest and at 6-month follow-up. Fathers demonstrated improvements across multiple domains, including parenting, relationship functioning, financial attitudes, and employment status. Although the intervention did not include explicit health components, these outcomes are closely aligned with established social determinants of health and may represent pathways through which fatherhood programs influence both paternal and child health.
Future research should build on these findings in several ways. First, studies should incorporate direct measures of health behaviors and health outcomes for both fathers and their children. This would allow for more explicit testing of the pathways linking fatherhood programming to health promotion and population health outcomes.
Second, researchers should examine the effects of fatherhood interventions that intentionally integrate health promotion components, including stress management, mental health support, and preventive health behaviors. Understanding how these additions influence both family functioning and health outcomes would strengthen the evidence base for fatherhood programs as health promotion interventions.
Third, future evaluations should employ more rigorous study designs, including randomized controlled trials, to isolate the effects of specific program components and strengthen causal inference. The findings from this descriptive study provide a strong foundation for such work.
Fourth, additional research is needed to examine long-term outcomes beyond 6 months, particularly in domains such as father involvement, where initial gains may attenuate over time. Identifying strategies to sustain improvements represents an important area for future investigation.
Finally, broader questions remain regarding the role of fatherhood programming within community and public health systems. Future research should explore how fatherhood programs can be more fully integrated into service delivery systems and community infrastructure, and how they may contribute to improvements in community health and well-being at the population level.
In addition to advancing the research literature, it is essential that findings from these studies be disseminated to program developers, practitioners, and policymakers. Evidence-based decisions informed by this work have the potential to significantly improve outcomes for fathers, their families, and the communities in which they live.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the U.S. Department of Health and Human Services, Administration for Children and Families, Office of Family Assistance (Grant No. 90ZJ0040-01-02). The Fathers Empowered to Learn, Lead, and Achieve Success (FELLAS) fatherhood project was developed and implemented by the grantee, Partnership for Maternal & Child Health of Northern New Jersey, with support from program officers and coordinators affiliated with the grant.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.