
Abstract
Immunization is a key public health strategy for preventing vaccine-preventable diseases; however, vaccine hesitancy remains a persistent challenge. This study determined the level of vaccine hesitancy among mothers of non- and under-immunized children aged 0–24 months in a third-class municipality in Occidental Mindoro, Philippines. A community-based cross-sectional study was conducted in Magsaysay, Occidental Mindoro, from February to July 2020. A total of 299 mothers participated. Data were collected using a structured questionnaire assessing vaccine hesitancy across the domains of confidence and trust, complacency, and perceived risk. Descriptive statistics summarized participant characteristics and hesitancy levels, while nonparametric tests examined associations between sociodemographic factors and vaccine hesitancy domains at a significance level of p < .05. Results showed that work status was significantly associated with perceived confidence and trust (U = 5408.50, p = .03) and perceived complacency and risk (U = 5122.00, p < .01), with stay-at-home mothers reporting higher ranks in both domains. Marital status was significantly associated with perceived confidence and trust, H(3) = 25.07, p < .01. Geographic location, H(2) = 24.61, p < .01, prenatal visit history, H(2) = 17.20, p < .01, and health information sources were also significantly associated with perceived confidence and trust, H(5) = 19.04, p < .01, and perceived complacency and risk, H(5) = 32.50, p < .01. These findings highlight the importance of targeted health communication strategies that address determinants of vaccine hesitancy. Engaging health care providers and leveraging trusted information sources may strengthen vaccine confidence and improve routine childhood immunization uptake.
Keywords
Introduction
Immunization is a proven tool for controlling and eliminating life-threatening infectious diseases and is estimated to avert between two and three million deaths each year. It is one of the most cost-effective health investments, with proven strategies that make it accessible to even the most hard-to-reach and vulnerable populations. It has clearly defined target groups; it can be delivered effectively through outreach activities; and vaccination does not require any major lifestyle change (World Health Organization [WHO], 2019). In addition to individual protection, vaccination programs also rely on population or “herd” immunity: immunization of large portions of the population to protect the unvaccinated, immunocompromised, and immunologically naive by reducing the number of susceptible hosts to a level less than the threshold needed for transmission (Mallory et al., 2018). Vaccines are essential for preventing infectious diseases at all ages. Yet, nearly 20 million infants miss basic vaccines, and over 14 million receive none at all, despite existing programs. Outbreaks of measles, diphtheria, and polio show the need for strong immunization efforts and effective disease surveillance to achieve high vaccination coverage and eliminate these diseases (Cordero, 2024). The Expanded Program on Immunization (EPI), now reformed into the National Immunization Program (NPI), a Philippine health program that guarantees children and communities in industrialized and developing countries access to immunizations, has been a pillar of global health initiatives. Nevertheless, despite its demonstrated effectiveness, vaccine adoption and uptake have been hindered by a number of problems, the most important of which is vaccination hesitancy (Decouttere et al., 2021). The existence of low immunization rates and delays in vaccine administration, even among fully immunized children, challenges efforts to control vaccine-preventable diseases. Such delays can reduce the overall effectiveness of immunization programs, especially when high-risk children remain unprotected for extended periods. As a result, younger age groups become more vulnerable, and disease transmission increasingly affects these younger populations (Raguindin et al., 2021).
Vaccine hesitancy refers to a situation in which a person delays or refuses to get vaccinated despite the availability of vaccination services. It includes a wide range of elements, such as doubts about the effectiveness and safety of vaccines, religious or philosophical convictions, erroneous information about medical procedures, mistrust of medical institutions, and complacency about the dangers of vaccine-preventable diseases. (Nuwarda et al., 2022). Since it limits the achievement of the high vaccination coverage rates required to create herd immunity and safeguard vulnerable populations, vaccine hesitancy is a complicated and multifaceted problem with potentially serious health implications (Kumar et al., 2016).
Vaccine hesitancy has been studied extensively in various settings; there is a need for context-specific research that delves into the factors contributing to vaccine hesitancy in different communities and regions (Cataldi & O’Leary, 2021; Marzo et al., 2022). While this body of research has significantly enriched our understanding of vaccine hesitancy, it is essential to recognize that the factors contributing to vaccine hesitancy can vary significantly across different contexts. Existing studies have predominantly focused on urban or higher-income settings (Aw et al., 2021; Migriño et al., 2020), leaving a significant gap in the body of knowledge about vaccine hesitancy in the special environment of third-income class communities. By exploring the specific factors impacting parents’ vaccine reluctance in such a municipality, where the interaction of sociocultural, economic, and health care–related influences may emerge differently, the current study aims to close this gap. This study aims to determine the level of vaccine hesitancy among mothers with 0–24 months of non- and under-immunized children in a third-class municipality in Occidental Mindoro.
Methods
Research Design
This research employs a descriptive cross-sectional design to investigate parents’ vaccine hesitancy within the municipality of Magsaysay in the province of Occidental Mindoro, Philippines, a third-income class municipality as of 2021. In the Philippines, local government units (LGUs) were categorized based on their average annual income, as defined by Republic Act No. 11964, with approximate conversions using an exchange rate of PHP 56 = US$1. First-class municipalities refer to those with at least PHP 200,000,000 (≈US$3.57 million). Second-class municipalities have an average annual income of PHP 160,000,000 to less than PHP 200,000,000 (≈US$2.86 million to <US$3.57 million). Third-class municipalities earn PHP 130,000,000 to less than PHP 160,000,000 (≈US$2.32 million to <US$2.86 million). Fourth-class municipalities report PHP 90,000,000 to less than PHP 130,000,000 (≈ US$1.61 million to <US$2.32 million). Fifth-class municipalities have an average annual income below PHP 90,000,000 (≈ <US$1.61 million).
Sample
The study population consisted of mothers aged 18 years and above with non-immunized or under-immunized children. The number of sampled mothers needed in the study was determined using the estimation of the population proportion with the assumption of a 95% confidence interval, 50% response distribution, and 5% margin of error. This yielded a minimum required sample of 384 participants. This calculated sample size was used to guide recruitment. However, participants were not randomly selected, and purposive sampling was used due to field constraints. A total of 299 respondents were successfully recruited and included in the analysis.
Households were identified with the assistance of community health workers within selected lowland, upland, and island communities. Data collectors visited households sequentially within accessible areas of each community. Eligible participants were mothers with at least one child residing in the household. At each household, one eligible respondent was invited to participate. If more than one eligible mother was present, one was selected based on availability and willingness to participate. Recruitment continued across communities until fieldwork was completed.
Research Instrument
Socio-demographic profile questionnaire: maternal age (≤19 years, 20–34 years, 35–2 years, and ≥35 years); marital status (single, married, cohabiting, widow); educational attainment (never been to school, elementary level, elementary graduate, high school level, high school graduate, vocational, college level, college graduate); family income status (poor ≤9520; low income (but not poor) 9,520–19,040; lower middle 19,040–38,080); number of children (less than 2, 3–4, more than 4); history of prenatal visit (zero, 1–3, and 4 above); and type of immediate health information. The type of immediate health information refers to the source from which the respondent first seeks or receives health-related information during a health concern. This variable was categorized as follows: doctor, nurse, midwife, barangay health worker, hilot, or albularyo. Each category represents the primary source the respondent identified for immediate health information. Barangay health worker (BHW) is the local term for community health worker (CHW), referring to non-health-professional community members trained to serve as the first point of contact for patients with the larger health system (Mallari et al., 2020). A hilot is a non-medical individual who practices the age-old indigenous Filipino healing practice associated with elderly healers. Commonly associated with massage, hilot is used to diagnose, treat, and prevent illnesses that manifest as physical ailments or spiritual imbalances. (Zapanta, 2022). An albularyo or folk doctor is the one who practices Folk medicine, traditional healing practices anchored in cultural beliefs of body physiology and health preservation. It includes herbal, animal, and mineral remedies, along with spiritual, manual, and physical therapies, used alone or combined to maintain health or diagnose, treat, and prevent illness (Rondilla et al., 2021).
To determine vaccine hesitancy, the study utilized the WHO SAGE Working Group on Vaccine Hesitancy Survey of Larson et al. (2015). Confidence and trust refer to mothers’ belief that childhood vaccines are safe, effective, beneficial, and that health services and providers delivering them are reliable and competent. Items assessing this construct include statements such as: “childhood vaccines are important for my child’s health,” “childhood vaccines are effective,” and “the information I receive about vaccines is reliable and trustworthy.” Complacency and perceived risk refer to mothers’ perception that vaccine-preventable diseases pose low risk and that vaccination is less necessary, along with concerns about vaccine safety and adverse effects. This construct includes items such as: “New vaccines carry more risks than older vaccines,” “I am concerned about serious adverse effects of vaccines,” and “My child does not need vaccines for diseases that are no longer common.” Responses were measured using a Likert-type scale (strongly agree, agree, neither agree nor disagree, disagree, or strongly disagree). To maintain the original instrument, no modifications were made, and no items were added. The VHS tool was translated into Tagalog in Sentro ng Wikang Filipino – University of the Philippines Manila, so that the questions can be answered by a layman with no formal education.
Data Collection
Data was collected through house-to-house survey interviews from February 2020. However, it was delayed due to the nationwide implementation of the Enhanced Community Quarantine. Data Collection resumed when the research site was classified under Modified General Community Quarantine in July 2020. The researchers ensured that the health protocols were followed during the interview, such as wearing facemasks, maintaining social distancing, and using sanitizer. All respondents were informed that they were well during the interview.
Ethical Considerations
This study was approved by the Research and Extension Council of the Occidental Mindoro State College (2020-SJ-BSM-04). The procedure for the protection of human participants involved securing a signed informed consent from each respondent. Participants received non-monetary incentives consisting of face masks and sanitizers during the survey interview.
Data Analysis
There were assigned codes for each questionnaire to ensure respondent anonymity. The researchers created a database by encoding the collected data into a Microsoft Excel file. The researchers conducted coding assignments and data cleaning to organize the dataset. The researchers also double-checked the survey instrument and the encoded data to ensure consistency between the original responses and the digital entries, ensuring completeness and accuracy of the dataset prior to analysis. The questionnaire was stored in a safety cabinet with a lock whose access is limited only to the researcher and was only to be retained for 3 years after the submission of all required reports. After the retention period, the questionnaire was shredded properly for disposal.
Demographic data was analyzed using descriptive statistics such as frequency and percentage. VHS items were analyzed by their mean per item and subscale. Negative questions such as VH5, VH9, and VH10 were coded in reverse. Normality of the dependent variables was assessed using the Shapiro–Wilk test. Results indicated that perceived confidence and trust significantly deviated from a normal distribution, W(299) = .757, p < .001. Similarly, perceived complacency and risk also showed a significant deviation from normality, W(299) = .966, p< .001. These findings indicate that the assumption of normality was violated for both variables. Therefore, nonparametric statistical tests were employed in subsequent analyses. For comparisons involving two independent groups, the Mann–Whitney U test was used. For comparisons involving three or more groups, the Kruskal–Wallis H test was applied. The study considered a significance level at p < .05.
Results
A total of 299 respondents participated in the study. The majority of respondents were aged 20–34 (67.6%), married (55.2%), and had completed elementary-level education (48.8%). Notably, 81.9% of respondents identified as stay-at-home mothers, and a significant majority reported “Poor” income levels (98.0%). Regarding the number of children, 47.5% had less than two, 23.4% had three to four, and 29.1% had more than four children. In terms of prenatal visits, a substantial proportion had four or more (31.4%), while 27.1% had none. The most common sources of immediate health information were barangay health workers (37.1%) and midwives (23.1%; Table 1).
Profile of the Respondents, Municipality of Magsaysay, Occidental Mindoro, Philippines – Year 2020 (n = 299).
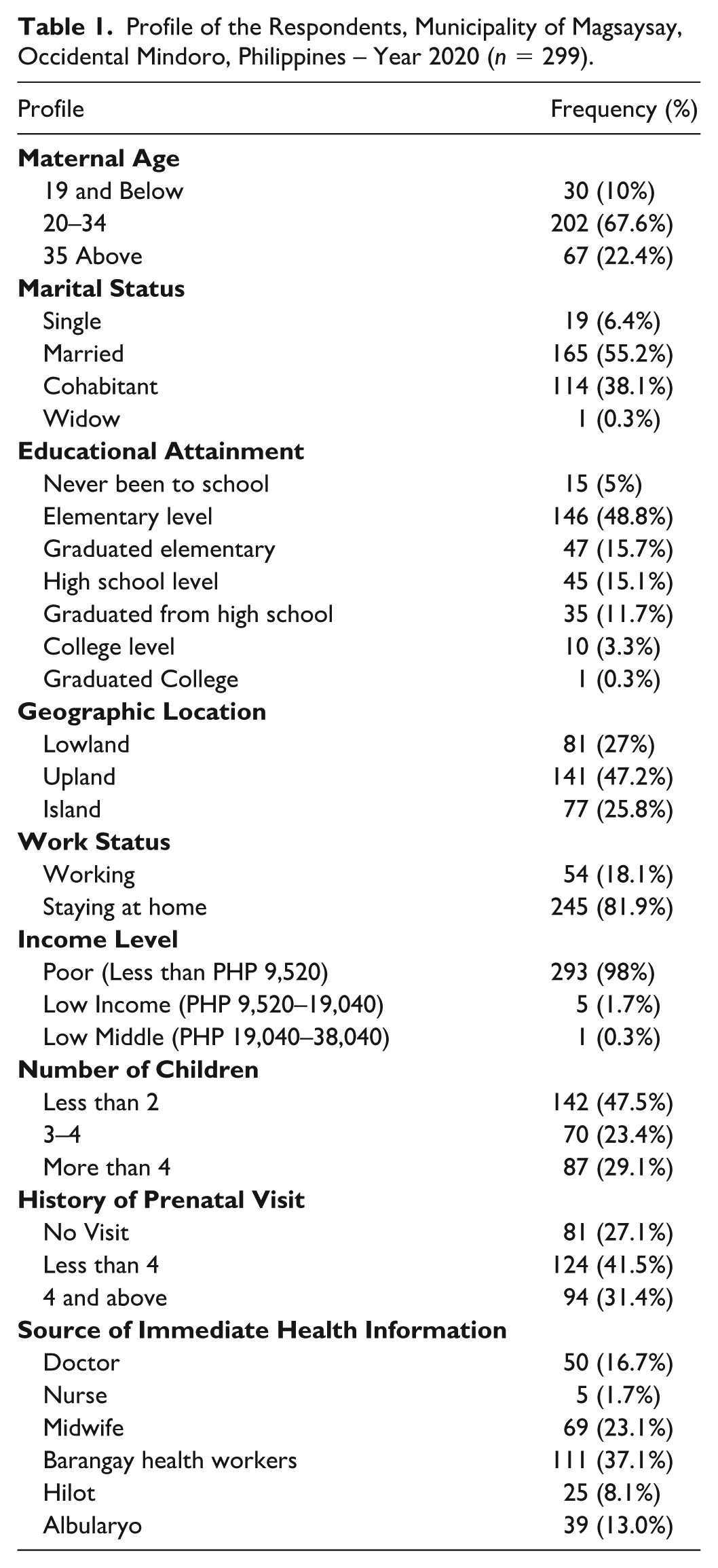
Table 2 shows high levels of confidence and trust (M = 4.34 ± 0.56) but lower complacency and risk (M = 2.84 ± 0.64).
Level of Vaccine Hesitancy (Municipality of Magsaysay, Occidental Mindoro, Philippines–Year 2020).
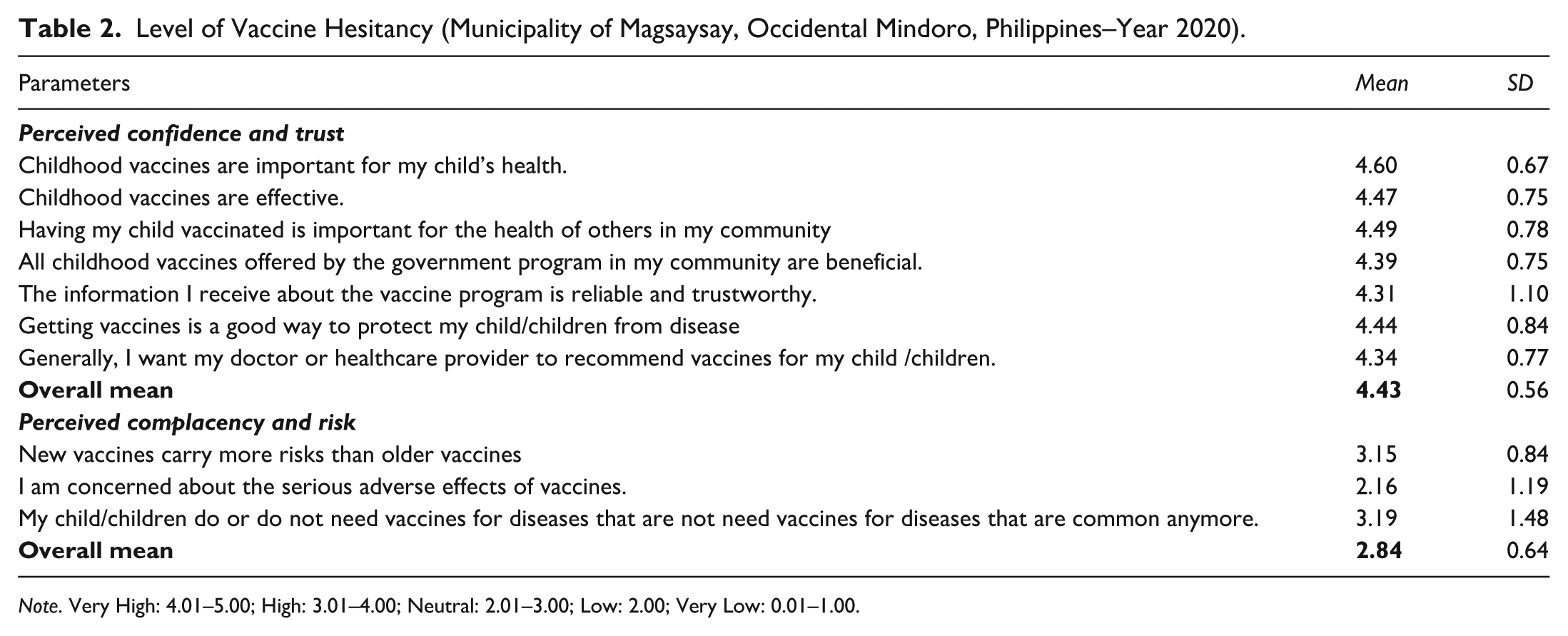
Note. Very High: 4.01–5.00; High: 3.01–4.00; Neutral: 2.01–3.00; Low: 2.00; Very Low: 0.01–1.00.
Factors of Vaccine Hesitancy
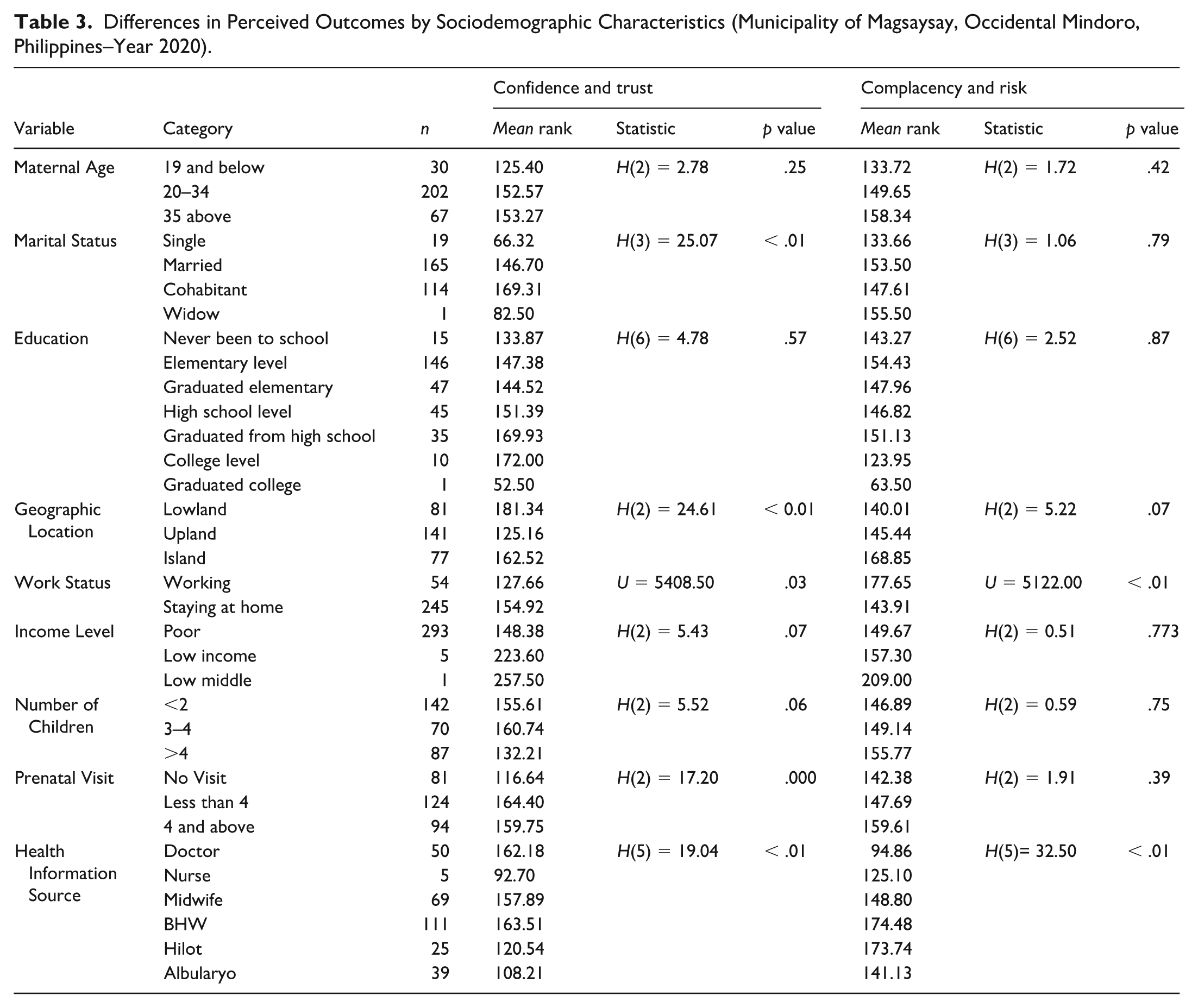
Work status showed a significant difference in both outcomes, with staying-at-home respondents reporting higher ranks for perceived confidence and trust (U = 5408.50, p = .03) and perceived complacency and risk (U = 5122.00, p < .01). Marital status showed a significant difference in perceived confidence and trust, H(3) = 25.07, p < .01. Geographic location, H(2) = 24.61, p < .01, and prenatal visit history, H(2) = 17.20, p < .01, were also significantly associated with perceived confidence and trust. Health information source showed significant differences in perceived confidence and trust, H(5) = 19.04, p < .01, and perceived complacency and risk, H(5) = 32.50, p < .01 (Table 3).
Differences in Perceived Outcomes by Sociodemographic Characteristics (Municipality of Magsaysay, Occidental Mindoro, Philippines–Year 2020).
Discussion
According to the data, mothers have high confidence and trust in immunization. However, the perceived complacency and risk is neutral, which means the mothers are neutrally satisfied when they are unaware of the serious or adverse reactions due to immunization. The interviews with mothers/caregivers revealed that although those interviewed were aware of the benefits of vaccination, most of them also had some concerns about the risks. Parents had concerns relating to the risks of vaccination and expressed a lack of trust in health authorities. It is important that strategies to improve confidence in vaccines focus on these concerns and are therefore adapted to the specific political, social, cultural and economic context of the country or region. Improving vaccine confidence among the community is crucial, as they have been shown to have the potential to influence patient vaccination uptake. Ongoing research is needed to develop the most effective strategies to confront vaccine acceptance (Vlasak et al., 2023). The most salient sociocultural issue contributing to defaulting from immunizations programs is the lack of male partner involvement in child health matters, particularly vaccination. Poor counseling of mothers, unsupportive client–provider relationships, poorly arranged and coordinated immunization services, and vaccine supply stockouts have also caused mothers to default on child vaccinations. The lack of functional immunization defaulter tracking mechanisms and poor intra-facility referral linkages were critical gaps in the health system (Zewdie et al., 2016).
The findings show significant differences between sociodemographic characteristics and parental attitudes toward childhood vaccines. Employment status is associated with differences in both confidence and trust and complacency and risk, with staying-at-home respondents showing higher levels of both outcomes compared with working respondents. Marital status shows a significant difference only in confidence and trust, with variation across categories. Prenatal visits are associated with differences in confidence and trust, where respondents with no prenatal care report lower levels compared with those who had prenatal visits. Health information source also shows significant differences in both confidence and trust, and complacency and risk, with variation depending on the source used. Overall, these correlations underscore the influence of personal and contextual factors on parental attitudes toward vaccination, emphasizing the importance of tailored communication and education strategies to address concerns and build trust in vaccine programs (Cooper et al., 2021; Leask et al., 2012).
The findings show that marital status is associated with differences in confidence and trust toward childhood immunization. This aligns with previous studies suggesting that married individuals often benefit from stronger social networks and support systems, which may shape more favorable attitudes toward health-related decisions, including vaccination. This result agrees with studies that claim social networks and family dynamics are important factors in vaccine acceptability (Smith et al., 2011). Employment may increase exposure to health information and access to health care services, which can strengthen confidence in vaccines and trust in immunization programs. This is consistent with research indicating that individuals with stable employment often have better access to health care services and are more likely to trust health care providers’ recommendations (Dubé et al., 2015). Employed individuals may also have more exposure to information that promotes vaccine confidence through workplace wellness programs or insurance benefits.
The positive association between a history of prenatal visits and confidence in vaccines suggests that exposure to antenatal care may strengthen parental trust in immunization through repeated contact with health care providers and consistent health education during pregnancy. This aligns with research emphasizing the importance of health care provider recommendations during prenatal and postnatal care in influencing vaccination decisions (Glanz et al., 2013). The negative correlation between specific sources of immediate health information and confidence and trust highlights the influence of information sources on vaccine attitudes. In this study, many respondents reported consulting non-medical individuals, such as hilot and albularyo, as primary sources of health advice. These providers often serve as accessible and culturally trusted figures within the community. However, their knowledge of vaccination is not always grounded in biomedical evidence (Kawi et al., 2024). Misinformation or biased information sources can erode confidence in vaccines. This finding corresponds with studies that have shown that the source and quality of health information significantly affect vaccine decision-making (Stasiuk et al., 2021; Ye et al., 2023). Thus, investigation of sources of health information and health-seeking behaviors continues to require further examination for better clarity to inform health programs and policy.
These findings are important for a lower-income municipality in the Philippines, where health care access and information flow depend heavily on local systems and community actors. Although respondents reported high confidence and trust in vaccines, this trust appears closely linked to interpersonal sources such as community health workers, which explains the significant association between hesitancy and source of health information (Acacio-Claro et al., 2025). At the same time, moderate levels of complacency and perceived risk suggest that gaps in health education and inconsistent exposure to reliable information persist, especially in resource-constrained settings where formal health care contact may be limited. This pattern indicates that vaccine hesitancy in this context is not driven by strong opposition but by uneven access to trusted information and services. These results show that, in lower-income settings, strengthening local health communication and supporting frontline health workers may be more effective than broad national campaigns (Brumbaugh et al., 2025). More broadly, this supports the need to adapt vaccine hesitancy frameworks to account for structural constraints and community-based information pathways that are less prominent in high-income settings.
While this study offers valuable insights into parental vaccine hesitancy in a third-income class municipality, several limitations should be noted. First, the use of a cross-sectional design with convenience sampling may introduce selection bias, limiting the generalizability of findings. Second, relying on self-reported data may lead to recall and social desirability biases. In addition, the survey instrument primarily focused on specific vaccine hesitancy factors and demographics, neglecting potential cultural and vaccine-related determinants. Finally, the study did not comprehensively explore complex social and cultural influences on vaccine hesitancy, suggesting a need for in-depth qualitative analysis. Nonetheless, these findings can still guide targeted interventions and future research efforts to address vaccine hesitancy’s multifaceted challenges in similar contexts and beyond.
Implication for Practice
There is a need for health care providers to prioritize culturally sensitive and trust-building communication strategies in vaccine counseling. Enhancing access to prenatal care positively influences vaccine confidence; thus, integrating vaccine education into routine maternal health services represents a strategic and effective intervention point (Parsekar et al., 2024). Community-based education and counseling, especially involving both parents, can address misinformation and strengthen vaccine confidence (Tuckerman et al., 2022). Frontline health workers should also receive continuous training on effective, empathetic communication to reduce perceived risks and complacency among caregivers.
Health promotion practitioners should translate these findings into concrete actions at the community level. They should conduct regular household mapping and defaulter tracking to identify children with missed vaccinations and follow them up through home visits. They should deliver small group education sessions during prenatal visits, immunization days, and barangay gatherings that directly address common fears, misinformation, and low perceived risk of vaccine-preventable diseases. They should use simple, locally understood messages and visual materials suited to the literacy level of parents. Community health workers should build trust by maintaining a consistent presence, providing clear explanations of vaccine benefits and side effects, and responding to concerns without judgment. Practitioners should also engage barangay leaders, religious figures, and parent champions as credible messengers to reinforce positive vaccine norms (Niu et al., 2023). At the system level, they should coordinate with local health offices to ensure reliable vaccine supply, maintain functional defaulter lists, and strengthen referral linkages between facilities. Continuous monitoring of missed doses, reasons for refusal, and community feedback should guide adjustments in communication and outreach strategies to improve vaccine uptake (Dadari et al., 2021).
Conclusion
This study offers valuable insights into the landscape of vaccine hesitancy among mothers in a third-income class municipality. The demographic and socioeconomic profiles of respondents have provided valuable context for understanding the factors that influence vaccine hesitancy in this specific setting. Trust in vaccines and health care providers, perceived risk of vaccine-preventable diseases, and access to reliable information directly influence parental decisions. While this research has advanced our knowledge of the issue, it is essential to recognize its limitations, including the use of cross-sectional data, self-reporting, and a limited scope of variables.
Nonetheless, these findings hold significance for public health efforts in similar contexts. Health promotion efforts should focus on strengthening trust through consistent and transparent communication from local health workers, delivering community-based education that addresses misconceptions and risk perceptions, and engaging barangay leaders and peer influencers to reinforce positive vaccine norms. Communication strategies must be tailored to the literacy level and media habits of parents to improve reach and impact. Shifting from general awareness campaigns to targeted, behavior-focused interventions, supported by routine monitoring of community attitudes, can improve vaccine acceptance and guide more responsive immunization programs in similar low-resource settings.
Footnotes
Acknowledgements
The authors would like to thank the Occidental Mindoro State College for providing technical support in conducting this study. The authors also extend their appreciation to their colleagues who provided valuable feedback during the early stages of this paper.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.