
Abstract
This exploratory study examined the effects of Interactive Metronome (IM) when integrated with a traditional language and reading intervention on reading achievement. Forty-nine school-age children with language and reading impairments were assigned randomly to either an experimental group who received the IM treatment or to a control group who did not. Both groups received language and reading intervention, and the experimental group received an additional four hours of IM treatment during a four-week period. Although both groups made gains in reading rate/fluency and comprehension, the extent of the gains was much larger in the IM group. IM training may be useful for promoting the reading rate/fluency and comprehension of children with language and reading impairments.
Keywords
Researchers are interested in investigating the different factors that contribute to or limit a child’s reading achievement. One such area of considerable investigation is that of reading fluency (Catts, Fey, Zhang, & Tomblin, 2001; Hogan, Catts, & Little, 2005; Hook & Jones, 2002; Kamhi, 2003). Kamhi (2003) defined reading fluency as the ability to read with speed and accuracy as well as with the appropriate expression. Hook and Jones (2002) suggested that fluency not only requires automatic word reading but also the use of appropriate prosody. Accordingly, fluency of reading is dependent on the prosodic features of our language, such as intonation, stress, and phrase patterns, which involve variations in timing (Chafe, 1988). From M. Wolf and Katzir-Cohen’s (2001) perspective, the ability to learn to read fluently and ultimately comprehend text depends greatly on the development and integrative function of multiple underlying processes involving perceptual and linguistic components.
Research has documented that children with language impairment (LI) are more likely to experience difficulty in reading achievement, including reading fluency, than typical language learners (Bishop & Adams 1990; Catts, Fey, Tomblin, & Zhang, 2002; Catts, Fey, Zhang, & Tomblin, 1999; Rescorla, 2002). In fact, some findings suggest that children with LI are as much as five to six times more likely to experience difficulties with learning to read than a typically developing child (Catts et al., 1999; Catts et al., 2002). Children with LI struggle with one or more areas of oral language, including morphology, syntax, phonological processing, semantics, and/or pragmatics that mirror similar aspects found in written language (Boudreau & Hedberg, 1999; Cabell, Justice, Zucker, & McGinty, 2009; Rescorla & Lee, 2000). Moreover, there are robust findings in the literature that identify difficulties with phonological awareness as one of the most critical language components for the child with LI in learning to read (Adams, 1990; Castiglioni-Spalton & Ehri, 2003; Catts, 1993; National Early Literacy Panel, 2004). Although it is widely recognized that impairment in phonological awareness is central to the development of reading disorders in many children, a number of researchers contend that this phonological processing deficit does not sufficiently explain the presence of reading disabilities in all children (Catts et al., 2001; Hogan et al., 2005; Lonigan, Burgess, & Anthony, 2000; Rayner, Foorman, Perfetti, Pesetsky, & Seidenberg, 2001).
One notion of considerable interest in this regard is that many children with developmental language and reading impairments have perceptually based problems involving the speed of information processing, especially in the auditory domain, which is believed to underlie their deficiencies in acquiring and manipulating phonological representations normally (Burns, 2007; Cacace, McFarland, Ouimet, Schrieber, & Marro, 2000; Cestnick & Jerger, 2000; Heath, Hogben, & Clark, 1999; Leonard et al., 2007; Miller et al., 2006). Catts, Gillispie, Leonard, Kail, and Miller (2002) found that school-age children with a reading impairment showed slower processing than controls for motor, phonological, lexical, visual, and grammatical tasks. P. Wolf (2002) suggested that children who have a reading disorder not only have deficits in the language system but also have a dysfunction in “timing.” Llinas (1993) indicated that this “timing” problem may result from an underlying temporal processing disturbance in children who have reading impairments.
A major impetus in this ongoing area of investigative inquiry and debate is a series of studies by Tallal and her colleagues that examined the auditory processing abilities of children with specific language impairment (SLI; Tallal & Piercy, 1973a, 1973b) and subsequently those with reading disorders (Tallal, 1980; Tallal, Miller, Jenkins, & Merzenich, 1997; Tallal & Stark, 1982). Their findings that a nonlinguistic auditory temporal processing deficit could be causally related with a phonologically based decoding problem and associated with reading disabilities have spurred numerous investigations focused on determining the nature and scope of the temporal processing difficulties presented by children with LIs and their relationship to the development of literacy skills.
Gaining a theoretical consensus has proven difficult for a number of reasons, including researchers’ varying views of what constitutes a rapid temporal processing deficit and its origin for nonlinguistic and linguistic stimuli (De Martino, Espesser, Rey, & Habib, 2001; Farmer & Klein, 1995; Mody, Studdert-Kennedy, & Brady, 1997; Nittrouer, 1999; Rey, De Martino, Espesser, & Habib, 2002; Studdert-Kennedy & Mody, 1995; Wright, Bowen, & Zecker, 2000). Nevertheless, over the last three decades, a substantial body of research has provided evidence that reading impairments in many children, including deficiencies in phonological processing, may be associated with nonlinguistic, rapid temporal auditory perceptual problems (Berninger, Raskind, Richards, Abbott, & Stock, 2008; Cacace et al., 2000; Cestnick & Jerger, 2000; Heath et al., 1999; McCroskey & Kidder, 1980). For example, researchers have documented that many children with reading disabilities exhibit deficits compared with normal controls in temporal order judgment tasks (Berninger et al., 2008; Cacace et al., 2000; Cestnick & Jerger, 2000; Heath et al., 1999). It also has been reported that children with reading disorders perform poorer than those with good reading skills in tonal frequency discrimination (Cacace et al., 2000; Walker, Givens, Cranford, Holbert, & Walker, 2006) and auditory temporal resolution tasks involving gap detection (Hautus, Setchell, Waldie, & Kirk, 2003; McCroskey & Kidder, 1980), which all require rapid processing of fine temporal properties of acoustic stimuli. Collectively, these findings provide support for the idea that many children with reading disabilities have deficits in processing rapid timing changes in acoustic signals. Such deficits may influence the speed and efficiency of their speech perception and phonological decoding (such as using grapheme to phoneme correspondence rules) and ultimately affect their reading fluency and comprehension. In this regard, Burns (2007) recently noted that “there is considerable evidence that auditory processing skills, especially in the domain of rapid auditory processing, underlie language acquisition and reading mastery” (p. 181). Thus, it appears reasonable that for some children with reading disabilities, training to improve rapid auditory temporal processing may promote the speed and accuracy of their text reading and support their reading development.
Research suggests that the human brain measures time continuously and that it is difficult to find any complex behavioral process that does not involve mental timing (Mauk & Buonomano, 2004). This capacity is important to a variety of performance mechanisms, including temporal processing and rhythm perception and production. Investigations on mental timekeeping and temporal processing indicate that humans have multiple timing systems that are associated with different behaviors and neurological substrates and that the fastest timing system is interval or millisecond mental timing (Buhusi & Meck, 2005; Mauk & Buonomano, 2004). According to Mauk and Buonomano (2004), “Temporal processing on this scale is required for simple sensory problems, such as interval, duration, and motion discrimination, as well as complex forms of sensory processing, such as speech recognition” (p. 307). Data from perceptual learning studies show that the neural mechanisms underlying mental timing can be fine-tuned or modified with treatment and that interval learning can generalize across modalities, such as spatial to auditory and auditory to motor (Karmarkar & Buonomano, 2003; Meegan, Aslin, & Jacobs, 2000; Nagarajan, Blake, Wright, Byl, & Merzenich, 1998). Similarly, it has been shown that combining auditory processing treatment with direct instruction in language structure can produce significant improvement in the reading skills of children with dyslexia, despite no direct reading intervention (Temple et al., 2003). Another neuroscience-based intervention for improving rapid interval auditory processing and achievement in other modalities is the use of synchronized metronome tapping (Buhusi & Meck, 2005; Taub, McGrew, & Keith, 2007).
Interactive Metronome (IM; 2007) is a neuroscience-based intervention for improving rapid temporal auditory processing and achievement in other modalities through the use of a synchronized metronome tapping. IM is a computerized treatment technique that requires individuals to maintain synchrony of a bimanual motor response with auditory tones. During treatment, participants listen to a reoccurring metronome beat via headphones and match tapping/clapping motions using hand and foot triggers to the beat presentation. Participants receive immediate feedback regarding the accuracy of their tracking primarily through an auditory guidance system which uses varying tones to indicate how closely their interactive physical responses correspond to the metronome beat. The synchronized metronome tapping treatment is designed to minimize the latency between the onset of the regularly occurring beat and a participant’s expectancy response to that beat (IM, 2007) and thereby promote improved temporal processing. A visual feedback of latency response can be used as well. A number of studies have shown that IM treatment is associated with improvements in motor control and coordination and can have a positive influence on higher level cognitive functioning, including reading (Bartscherer & Dole, 2005; Kuhlman & Schweinhart, 1999; Libkuman & Otani, 2002; Schaffer et al., 2001; Taub et al., 2007). In fact, Taub et al. (2007) found that elementary-age children who were provided IM treatment scored significantly higher on standardized tests of word reading efficiency and fluency than those in a nontreatment control group. These findings are consistent with other data demonstrating a relationship between performance measures for continuous, sequential, motor tapping tasks, oral reading, and temporal processing (Schaffer et al., 2001; Stanford & Barratt, 1996). Therefore, it is possible that adding IM treatment to a traditional language and reading intervention may produce clinical gains on improving rapid auditory processing and reading achievement in children with a language and reading impairment.
It is well established that the process of learning to read fluently with comprehension is not an autonomous process of learning one or two cognitive skills independently; rather, it requires the acquisition and integration of a multitude of component skills involving phonological processing, decoding, vocabulary, syntax, morphology, listening comprehension, and discourse and background knowledge (Anthony & Francis, 2005; Bishop & Snowling, 2004; Bus & Van Uzendoorn, 1999; Troia, 1999; Vellutino, Fletcher, Snowling, & Scanlon, 2004; Verhoeven & van Leeuwe, 2008). Reading fluency is considered by some investigators to be an important predictor of reading comprehension in children. In fact, research indicates that the speed and accuracy of decoding words are critical variables as they actually account for a significant amount of variance for reading comprehension (Fuchs, Fuchs, Hosp, & Jenkins, 2001; Kame’enui & Simmons, 2001). When reading fluency is fully developed, so that word decoding with accuracy and speed becomes relatively automatic, then the reader’s attention and other cognitive resources can be directed to comprehending the meaning of the text (National Reading Panel [NRP], 2000; M. Wolf & Katzir-Cohen, 2001). However, when the reader is using most of his or her cognitive resources for decoding, it can be assumed that there are few if any remaining resources that can be allocated to reading comprehension (Fuchs et al., 2001; NRP, 2000).
It is clear that numerous researchers have provided a variety of ways to successfully improve children’s reading fluency and foster their reading comprehension (Kuhn & Stahl, 2003; NRP, 2000; Rasinski & Hoffman, 2003; Robertson & Davig, 2002; Roth, Speece, & Cooper, 2002; Rvachew, Ohberg, Grawburg, & Heyding, 2003; Tyler, 2002). There are many readers who become fluent after receiving reading instruction by their regular classroom teacher; still, there are other readers who struggle and require much more intensive and systematic intervention or instruction to become a fluent and successful reader (Kuhn & Schwanenflugel, 2006; Wexler, Vaughn, Edmonds, & Reutebuch, 2008). Thus, it is important to continue to explore additional methods and techniques that may improve the automaticity and fluency of reading in children who have developmental language and reading impairments. The idea that IM treatment can promote the rate and efficiency of information processing and that these skills may generalize to other cognitive abilities, including reading fluency and comprehension, is intriguing and warrants investigation. This is especially true given the evidence that many children with language and reading disabilities have deficits in rapid auditory processing and given the possibility that combining IM treatment with a language and reading intervention may produce a more effective intervention.
Although evidence indicates that IM treatment may be associated with significant improvement in typically developing children’s reading fluency (Schaffer et al., 2001; Taub et al., 2007), the potential value of providing IM treatment to promote reading fluency in children who have developmental language and reading impairments has yet to be determined. To date, no study has examined the effects of IM treatment as an adjuvant to a traditional language and reading intervention with this population. Accordingly, we designed exploratory research to gain insight as to whether IM treatment when combined with a traditional language and reading intervention is a viable type of intervention for improving reading fluency in children with a language and reading impairment. We were interested in determining whether IM treatment would have an additive value to traditional language and reading intervention and make a significant difference in the treatment outcome. The Interactive Metronome website states, Interactive Metronome (IM) is an engaging, rewarding, and systematic program that improves timing in the brain, thus improving the ability to learn, retain, and apply new information in the academic setting and beyond. IM is used in the schools to improve: Focus & Concentration, Sequencing & Organization, Auditory & Language Processing, Reading & Math Achievement, Handwriting, and Self-Control of Impulsivity and Hyperactivity.” (IM, 2012, para. 3)
The present investigation is an exploratory study to examine the potential effects of IM training related to reading achievement.
The purpose of this study is to examine the effects of IM treatment integrated into a traditional language and reading intervention on the reading fluency of children with a language and reading impairment. More specifically, answers to the following questions are sought:
Research Question 1: Is there a difference between pre- and postintervention measures of reading fluency for school-age children with a language and reading impairment who do and do not receive IM treatment integrated with a traditional language and reading intervention?
Research Question 2: Is there a difference between pre- and posttreatment measures of reading comprehension for school-age children with a language and reading impairment who do and do not receive IM treatment integrated with a traditional language and reading intervention?
Method
Participants
Participants were 49 school-age children (e.g., in Grades 2–5) who had been diagnosed with co-occurring language and reading impairments and who were enrolled in a university clinic’s summer language and reading program. Participants were randomly assigned to either an experimental group (n = 28) who received IM treatment or to a control group (n = 21) who did not receive the treatment. All participants received a traditional language and reading intervention differing only by the IM treatment.
Although 60 children were originally recruited to participate in this study, 11 participants withdrew from the study prior to completing all treatment due to vacation activities and illness. The IM treatment group (n = 28) consisted of 19 males and 9 females who ranged in age from 7 years 1 month to 11 years 4 months (M = 9 years 2 months, SD = 1 year 3 months). The control group (n = 21) comprised 15 males and 6 females who ranged in age from 7 years 2 month to 11 years 9 months (M = 9 years 6 months, SD = 1 year 3 months). In all, 42 of the participants were Caucasian, 3 were African American, 3 were Hispanic, and 1 was Asian American. As determined by self-report in the case history interview, the participants’ families were described as lower to middle class. The parents of the participants were fully informed about the study and were required to sign a parental consent form giving permission for their child to be involved in the research. The investigation protocol was reviewed and approved by the university internal review board.
Inclusion Criteria
A battery of standardized tests was administered to all participants prior to the intervention to establish their language and reading scores. Receptive and expressive language skills were assessed using the Clinical Evaluation of Language Fundamentals–Fourth Edition (CELF-4; Semel, Wiig, & Secord, 2003). The four subtests for the Core Language score (Concepts and Following Directions, Word Structure [age 5–8] or Word Classes [age 9 and up], Recalling Sentences, and Formulated Sentences) were administered for this purpose. Expressive vocabulary was assessed using the Expressive Vocabulary Test–Second Edition (EVT-2; Williams, 2007). The Gray Oral Reading Test–Fourth Edition (GORT-4; Wiederholt & Bryan, 2001) was used to obtain reading rate, accuracy, fluency, and comprehension standard scores. The participants met the following selection criteria for inclusion:
Core Language score at or greater than 1 SD below the mean (16th percentile or less) on the CELF-4, and an expressive vocabulary score at or greater than 1 SD below the mean (16th percentile or less) on the EVT-2.
A minimum of 1 SD below the mean (16th percentile or less) for reading fluency or reading comprehension scores on the Gray Oral Reading Test–Fourth Edition (GORT-4; Wiederholt & Bryan, 2001).
No suspected intellectual disability or history of neurological disorder (i.e., stroke, traumatic brain injury, or seizure disorder) as determined by parent report.
No hearing impairment or major physical impairment.
Monolingual English speaker.
Procedures
Preintervention testing was completed 1 week before treatment was initiated. After both the experimental and control groups had completed the intervention program, all participants were retested on the same measures of reading fluency and comprehension. All language and reading measures with the exception of Read Naturally (Read Naturally Inc., 2005) were administered by three trained graduate research assistants in a single session, using standard assessment procedures for the participant’s age group. The graduate assistants were pursuing their master’s degree in communication sciences and disorders and were supervised by a faculty member holding a state license and Certification of Clinical Competence from the American Speech-Language Hearing Association (ASHA). The Read Naturally Software Edition (Read Naturally Inc., 2005) was administered and analyzed by a certified reading specialist for all participants. The total assessment time ranged from 60 to 90 min. The examiners for the assessment and test scoring were blind to the participants’ assigned groups, and each child was assigned a number that was used in place of his or her name on all test forms. The order of the tests remained constant.
Three reading outcome measures were individually administered, using standard assessment procedures as stated in their perspective manuals. The outcome measurements consisted of the Dynamic Indicators of Basic Early Literacy Skills–6 Oral Reading Fluency (DIBELS-6 ORF; Good & Kaminski, 2002), Read Naturally Test (Read Naturally Inc., 2005), and GORT-4 (Wiederholt & Bryan, 2001).
The DIBELS-6 ORF is a standardized, individually administered assessment of reading fluency using connected text. The participants read a passage aloud for 1 min. Three 1-min reading samples were obtained, and the median of the three was calculated for correct words read per minute. The participants’ current grade level (second through fifth grade) was used as a determinant of the selection of the passage read. The alternate form of the DIBELS-6 ORF was used for the post-testing.
The Read Naturally software was also used to evaluate each participant’s oral reading fluency. It consisted of a computerized reading assessment that was uploaded to a computer hard drive. The participants’ current grade level determined the selection of the passage read. The Read Naturally is also timed over three 1-min reading samples, and the median score was used as the fluency measure.
The GORT-4 is a standardized instrument that measures rate, accuracy, fluency, and comprehension of reading. Alternate forms were used in the pre-testing (Form A) and post-testing (Form B) to gain a measurement of each participant’s rate, accuracy, fluency, and comprehension of reading. The group’s pre- and posttreatment reading measures for the three tests were compared to determine gains in reading fluency and comprehension.
Reliability
All language and reading measures were administered and scored according to the procedures stated in the manual. All examiners received additional training in test administration over a 3-day period prior to the initiation of this study by the first author. All scoring was rechecked by the examiner and then by two graduate assistants working independently. Fifty percent of each assessment session was supervised by one of the supervising faculty, and 20% of those sessions were randomly selected and supervised 100% of the time to further establish reliability of test administration and scoring. Analysis indicated a range of 91% to 100% agreement with an average of 96% agreement for the pre- and posttest scores. All points of disagreement were discussed and resolved and brought to an agreement of 100%.
Intervention
The intervention used in this study for the experimental group was the IM treatment (IM, 2007), which was combined with a traditional language and reading intervention. The control group received the traditional language and reading intervention only. Both the IM treatment and the language intervention were provided by trained graduate clinicians under the supervision of faculty holding a state license, a Certification of Clinical Competence in Speech-Language Pathology from the ASHA and trained by IM Corporation to implement IM treatment. The graduate clinicians completed a total of 7 days of intensive training in implementing the IM intervention, and each aspect of the language intervention protocol with the first author of the study prior to the initiation of the intervention. The reading intervention was conducted by three reading professionals holding a master’s degree in education.
IM
The experimental group participated in 15-min IM treatment each day for a total of 4 hr during the 4-week intervention. During the control group’s designated snack time, the experimental group participated in the IM treatment. Treatment was provided to each participant in a quiet environment as stated in the IM training manual (IM, 2007). Treatment sessions followed a prescriptive guide that controlled the structure and implementation of each IM session. Specifically, the IM treatment involved a laptop computer, IM software, a hand and foot contact sensor trigger, and two sets of headphones. During the treatment, each participant listened to a computer-generated, reoccurring metronome beat via headphones and matched clapping/tapping motions to the beat presentation while using the hand or foot trigger. A patented guidance system provided immediate real-time auditory feedback for response rhythm and timing. Response accuracy was measured to the nearest milliseconds. The IM computer setting was adjusted so that the pace and complexity level of the treatment was appropriate for each participant’s processing abilities.
Each IM treatment session consisted of three to five different tasks that included both hand and foot triggers (e.g., clapping both hands together, tapping one hand to upper thigh, toe taps, alternating toe taps, heel taps, and alternating heel taps using the foot trigger, a combination of the hand and foot movements using both the hand and foot triggers). The participants were instructed to listen to the metronome beats and the guide sounds triggered by their hand and foot movement accuracy. The guide sounds changed in pitch and left/right headphone location according to the accuracy of the participants taps/claps. The IM program displayed the participant’s accuracy of response after each task was completed. Verbal feedback was provided to each participant during and following each task. To ensure accuracy and reliability, participant training was provided by graduate clinicians who were trained in IM usage procedures, and all sessions were supervised by the first author.
Language and reading intervention
The children in both the IM and control groups received a traditional language and reading intervention 4 days a week over a 4-week period for a total of 48 hr of intervention. The children participated in a 1-hr individual language intervention session, a 1-hr small group language intervention (3–4 participants), and a 1-hr reading intervention session (4–6 participants). Participants were combined in the small group interventions based on their language and reading severity levels.
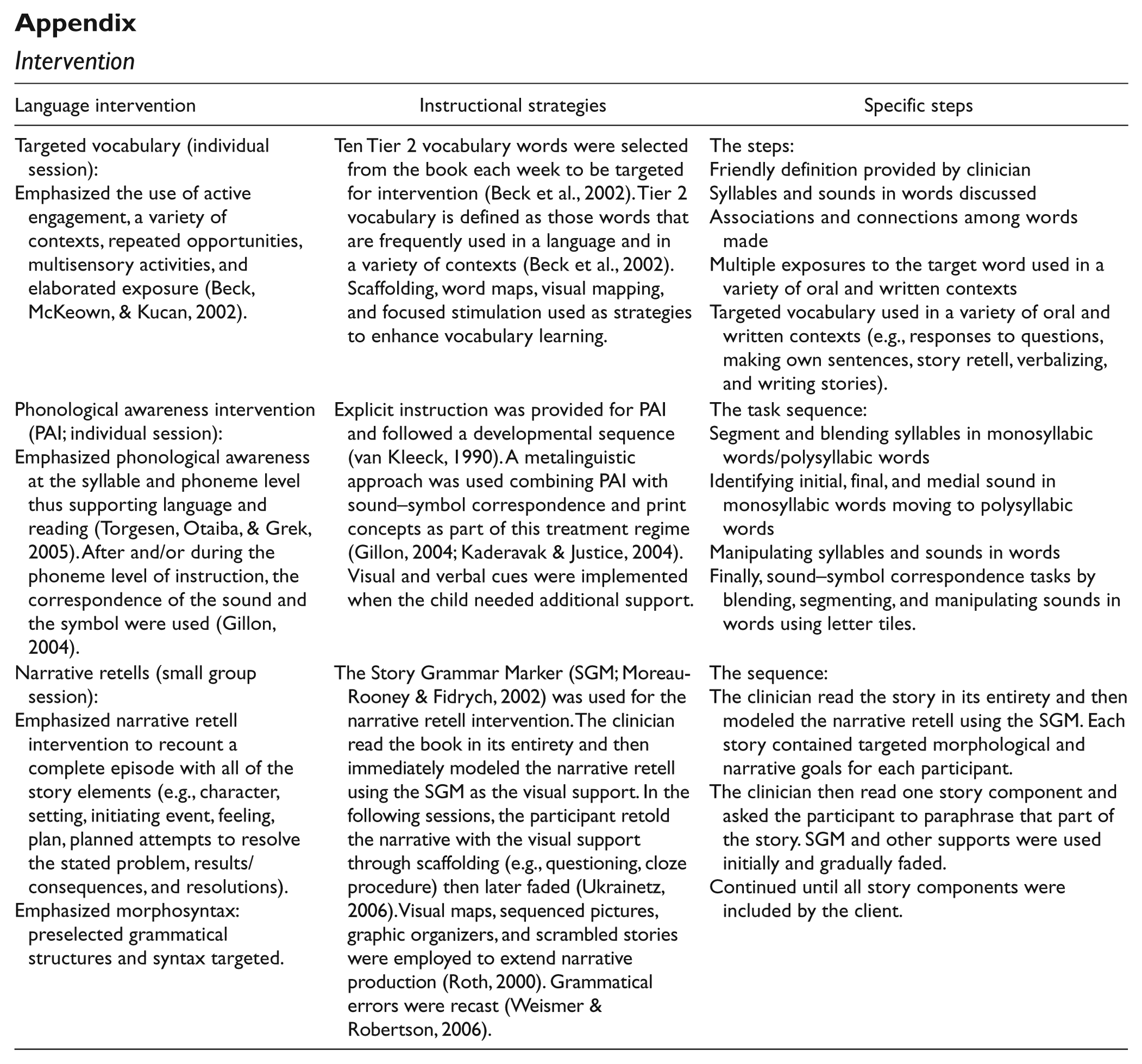
The language intervention utilized a narrative (story book) platform and focused on vocabulary, narrative retells, and phonological awareness. The narrative platform provided an authentic learning opportunity and encouraged active participation in the intervention (Gillam & Ukrainetz, 2006; Pretti-Frontczak & Bricker, 2004). Thus, each week of intervention, a specific book (e.g., Cowboy Camp, Sauer, 2005) was chosen for the narrative-based intervention in accordance with a particular theme. The individual language intervention targeted vocabulary and phonological awareness, and the group language intervention targeted narrative structure. The reading intervention was based on a structured reading program, the Sequential English Education (SEE) curriculum (Pickering, 2001). Each participant received 16 scripted lessons following the SEE curriculum as related to decoding and reading words and sentences based on that individual’s current reading level. The appendix provides a description of the intervention.
Treatment fidelity
The 49 participants attended all 16 sessions for a total of 48 hr of language and reading intervention. The experimental group received an additional 15 min of IM treatment while the control group received a snack time. To further ensure that the intervention was implemented consistently and with fidelity, each graduate clinician was responsible for providing the language intervention to one child in the experimental group and one child in the control group. Each trained graduate clinician was supervised for a minimum of 30% of the time by the supervisory faculty. For each supervised session, an evaluation form was completed and discussed with the graduate clinician regarding the consistency, execution, and adherence to the intervention protocol.
Statistical considerations
The effects of IM treatment integrated with a traditional language and reading intervention on each measure of reading fluency and comprehension (i.e., Read Naturally, DIBELS-6, and GORT-4) were determined by conducting a series of mixed-model ANOVA with one between-subjects variable (group) and one within-subjects variable (time). We used partial eta square (η p 2) to determine the strength of significance. Values of .01, .06, and .14 are by convention interpreted as small, medium, and large effect sizes, respectively (Green & Salkind, 2003).
Results
Pretreatment Reading Measures
To check for randomization bias, potential pretreatment differences between the two groups in regard to their language scores, chronological ages, and reading scores (fluency and comprehension) were examined using a series of t tests. No significant group differences were noted for the three subtests of the CELF-4 at the significance level of .05: Concepts and Following Directions, t(47) = 0.025, p = .980; Recalling Sentences, t(47) = 0.794, p = .431; and Formulated Sentences, t(47) = 0.456, p = .650]. Subsequently, two groups were not significantly different on the CELF-4 Core Language composite score, t(47) = 0.164, p = .871, and the EVT-2, t(47) = 0.148, p = .883. A comparison of the group means and standard deviations (SDs) for all language measures and chronological age is presented in Table 1.
The Means, Standard Deviations, Chronological Ages, and Standardized Test Scores on the Receptive and Expressive Language and Vocabulary Tests for the Two Groups
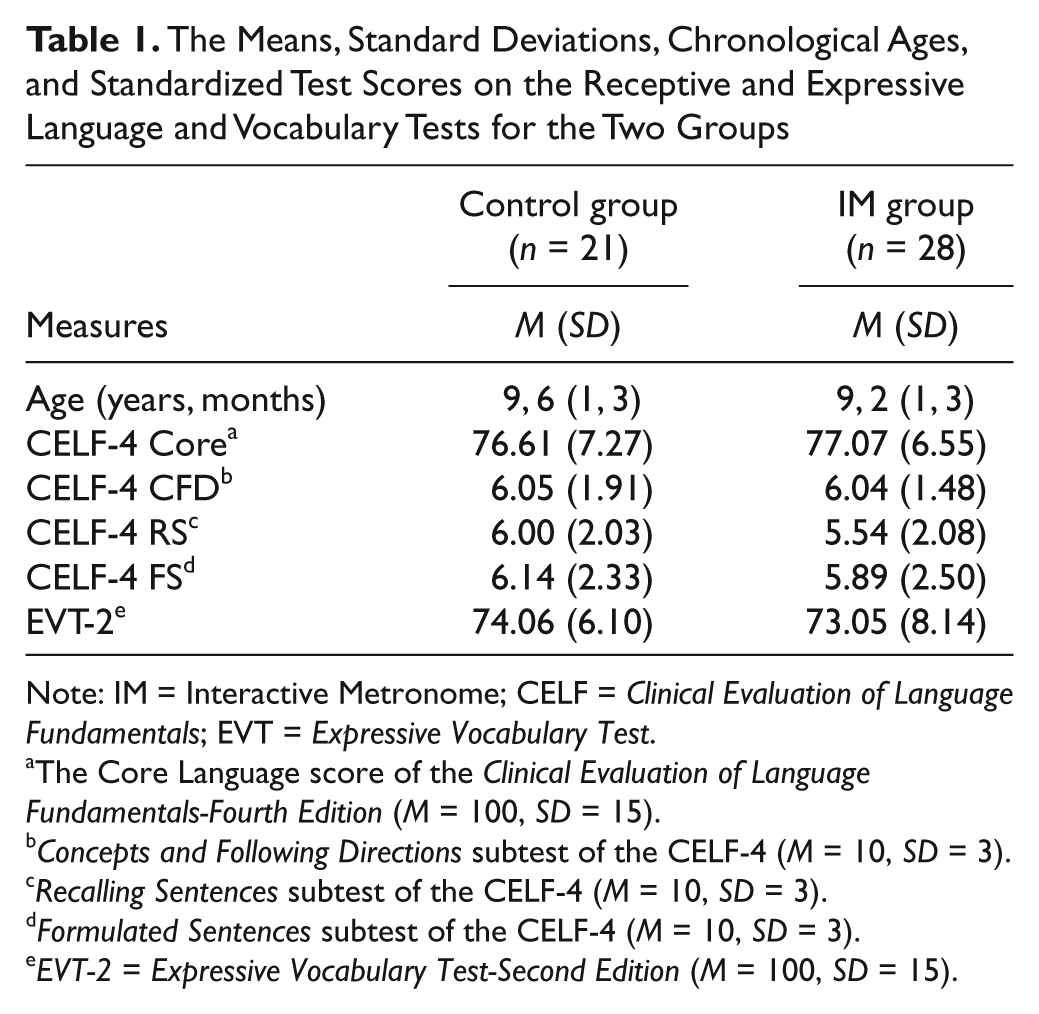
Note: IM = Interactive Metronome; CELF = Clinical Evaluation of Language Fundamentals; EVT = Expressive Vocabulary Test.
The Core Language score of the Clinical Evaluation of Language Fundamentals-Fourth Edition (M = 100, SD = 15).
Concepts and Following Directions subtest of the CELF-4 (M = 10, SD = 3).
Recalling Sentences subtest of the CELF-4 (M = 10, SD = 3).
Formulated Sentences subtest of the CELF-4 (M = 10, SD = 3).
EVT-2 = Expressive Vocabulary Test-Second Edition (M = 100, SD = 15).
In addition, no group differences were noted at pretest on any of the reading outcome measures used in this study: Read Naturally scores, t(47) = .525, p = .602; DIBELS-6 ORF scores, t(47) = 1.31, p = .198; GORT-4 rate scores, t(47) = .578, p = .566; GORT-4 accuracy scores, t(47) = .297, p = .768; GORT-4 fluency scores, t(47) = .941, p = .352; and GORT-4 comprehension score, t(47) = .695, p = .491. Thus, the randomization procedure appeared to achieve equivalence of the groups at baseline on these specific variables (see Table 2).
Group Means, Standard Deviations, and Mean Gain Scores for the Reading Fluency and Comprehension Measures at Pre- and Post-Treatment
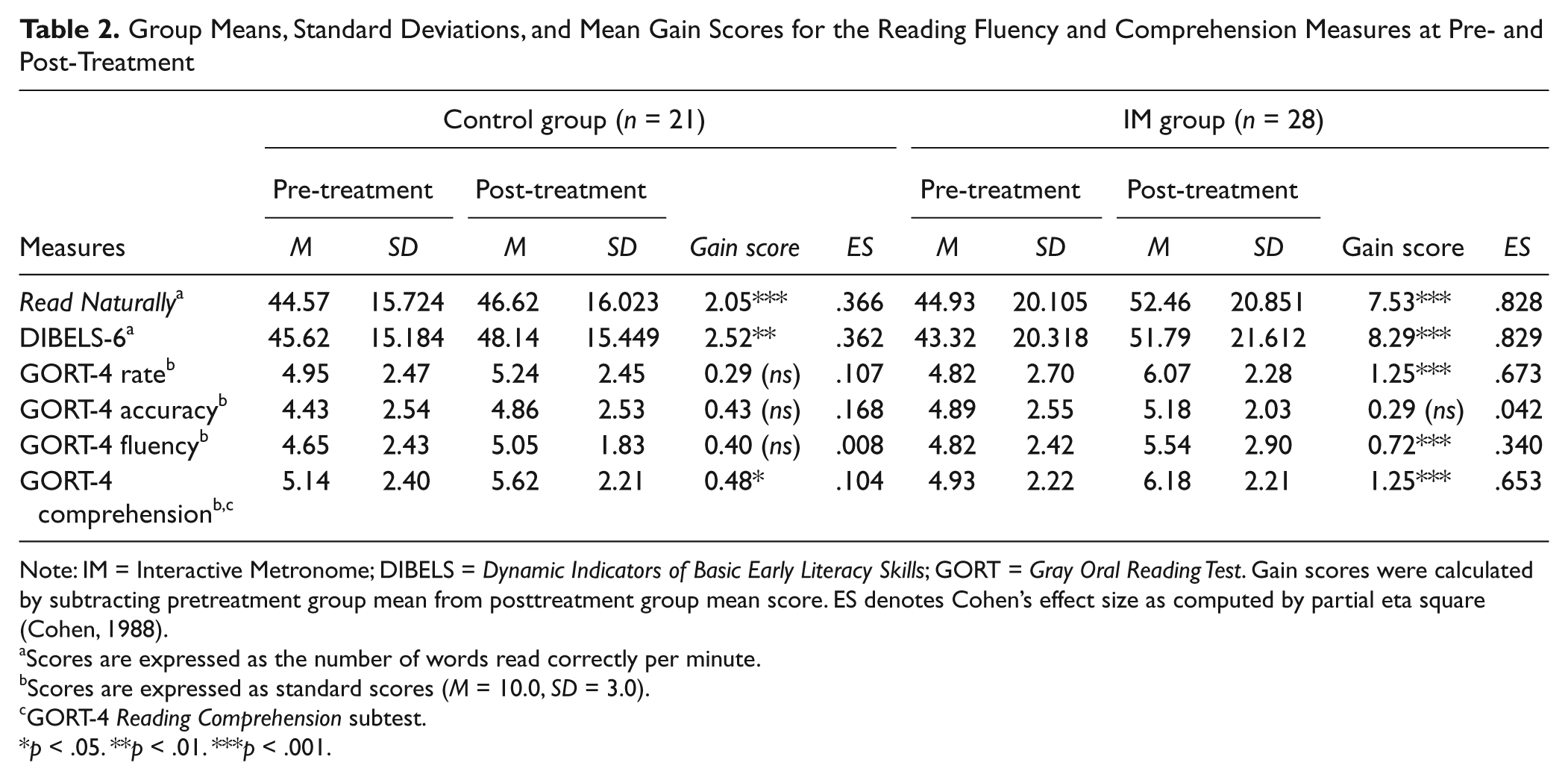
Note: IM = Interactive Metronome; DIBELS = Dynamic Indicators of Basic Early Literacy Skills; GORT = Gray Oral Reading Test. Gain scores were calculated by subtracting pretreatment group mean from posttreatment group mean score. ES denotes Cohen’s effect size as computed by partial eta square (Cohen, 1988).
Scores are expressed as the number of words read correctly per minute.
Scores are expressed as standard scores (M = 10.0, SD = 3.0).
GORT-4 Reading Comprehension subtest.
p < .05. **p < .01. ***p < .001.
Posttreatment Comparisons of Reading Measures
The groups’ means and SDs for the pre- and posttreatment scores on reading fluency and comprehension measures are shown in Table 2.
First, a two-way (group and time) repeated measures ANOVA comparing the Read Naturally scores showed no significant main effect for group: F(1, 47) = .334, p = .566. There was a significant effect for time, F(1, 47) = 119.926, p < .001, η p 2 = .718, however, and the interaction Time × Group was also significant, F(1, 47) = 39.32. p < .001, indicating that there were significant differences in performance over time between the two groups. Post hoc univariate ANOVAs revealed that the Read Naturally mean fluency scores increased significantly in both groups: the IM group, F(1, 27) = 129.715, p < .001, and the control group, F(1, 20) = 17.443, p < .001. However, the effect size of the IM group (η p 2 = .828) was much larger than that of the control group (η p 2 = .366). Figure 1(a) shows the pre- to posttreatment changes in each group’s Read Naturally fluency scores. The IM group showed superior performance post-treatment and the control group did not show the same degree of improvement.
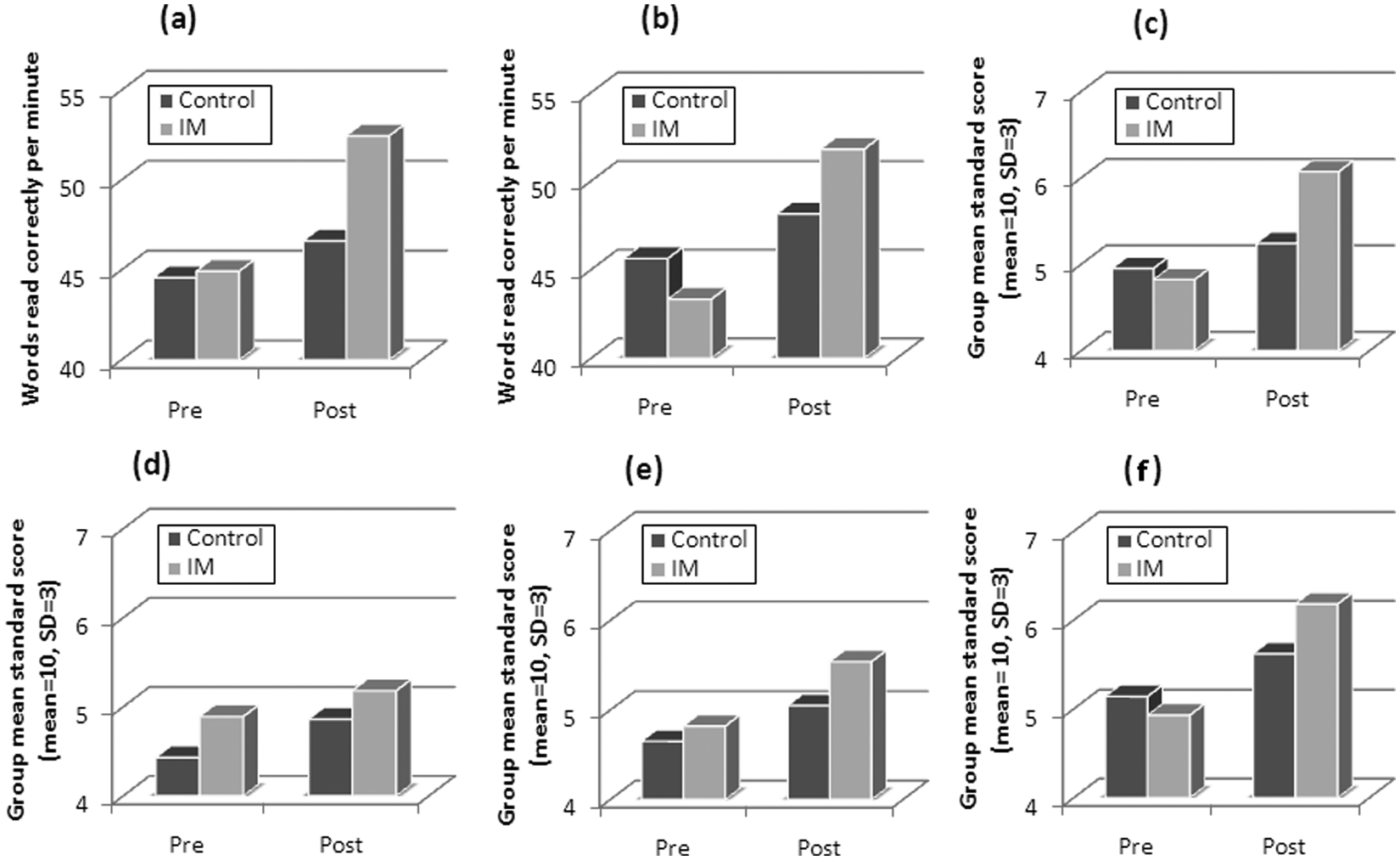
Pre- and postintervention performance on the Read Naturally, DIBELS-6 ORF, and the GORT-4 subtests (rate, accuracy, fluency, and comprehension) for the IM and control groups.
Next, examination of the DIBELS-6 fluency scores with a mixed-model ANOVA revealed a similar result. There was a significant main effect for time, F(1, 47) = 105.054, p < .001, η p 2 = .691, and a significant Group × Time interaction effect, F(1, 47) = 30.705, p < .001, η p 2 =.395. There was no main group effect, F(1, 47) = .015, p = .902, η p 2 =.0001. Planned follow-up ANOVAs showed a significant treatment effect in both groups: the IM group, F(1, 27) = 131.157, p < .001, η p 2 = .829, and the control group, F(1, 20) = 18.30, p < .001, η p 2 = .501. Again, the IM group outperformed the control group postintervention as evidenced in the larger effect size. As seen in Figure 1(b), the amount of change in the IM group’s mean scores was greater than that of the control group.
Next, a two-way mixed ANOVA examined differences in the groups’ GORT-4 rate scores. Similar to the DIBELS-6, the results revealed a significant main effect for time, F(1, 27) = 37.431, p < .001, η p 2 = .443, and a Group × Time interaction, F(1, 47) = 14.758, p < .001, η p 2 = .239. Planned post hoc ANOVAs revealed a significant time effect for GORT-4 rate in the IM group, F(1, 27) = 55.588, p < .001, η p 2 = .673, but not in the control group, F(1, 20) = 1.21, p = .137, η p 2 = .107, indicating that IM treatment was associated with score gains on the GORT-4 rate of the experimental group only. Figure 1(c) illustrates the differences in the two groups’ posttreatment GORT-4 rate scores.
Examination of the GORT-4 accuracy mean scores indicated no significant main effects for time, F(1, 47) = .4.061, p = .056, η p 2 = .080; Group × Time interaction, F(1, 47) = .162, p = .689, η p 2 = .003; and group, F(1, 47) = .883, p = .352, η p 2 = .018. As illustrated in Figure 1(d), no noticeable difference between the groups was found on GORT-4 accuracy following intervention. In addition, a mixed-model ANOVA was computed to explore the effect of IM treatment on the GORT-4 fluency composite mean scores. Even though the effect sizes were relatively smaller, significant main effects were found for time, F(1, 47) = 7.173, p = .01, η p 2 = .132, and Group × Time interaction, F(1, 47) = 4.195, p = .046, η p 2 = .082. There was no main effect for group, F(1, 47) = .163, p = .689. Follow-up post hoc ANOVAs revealed that the GORT-4 fluency scores increased significantly only in the IM group, F(1, 27) = 13.918, p < .001, η p 2 = .340, and there was no significant increase in the control group, F(1, 20) = .16, p = .693, η p 2 = .008. Finally, a 2 (group) × 2 (time) repeated measures ANOVA on data from the GORT-4 comprehension subtest showed that the difference in performance across time (i.e., pre- and post-treatment) was significant, F(1, 47) = 37.776, p < .001, and did not interact with subgroups, F(1, 47) = 7.591, p = 0.008. Follow-up tests revealed a significant time effect in both the IM group, F(1, 27) = 26.19, p < .001, and the control group, F(1, 20) = 1.21, p = .047. However, effect size of the IM group (η p 2 = .653) was much larger than that of the control group (η p 2 = .104). Figure 1(f) illustrates the group data on the GORT-4 comprehension scores of the two groups of children.
Discussion
This exploratory study examined the potential benefits of IM treatment when integrated with a traditional language and reading intervention on the reading fluency and comprehension of school-age children with a language and reading impairment. A major finding of this preliminary investigation was that although both the IM and control groups made significant gains in reading fluency and comprehension, the extent of gain was larger in the IM group.
Reading Fluency Outcome
In reference to our first research question, our results show that both the IM and the control groups made statistically significant gains in reading fluency; however, the IM group made greater gains with larger effect sizes than the control group. The children in the IM group demonstrated statistically significant gains in their ability to fluently read paragraph-level material on all three measures (e.g., Read Naturally, DIBEL-6, and GORT-4 fluency). Interestingly, children in the IM group did not show any treatment effect in the accuracy component of the GORT-4. This suggests that the primary source of clinical gains in the IM group’s fluency performance, which is composed of rate and accuracy, was that of rate. In other words, the experimental group did not improve their level of reading accuracy but increased their efficiency and rate of reading paragraph-level material. Similar findings were reported by Taub et al. (2007) in their investigation of the effects of IM training on reading achievement. Statistically significant results were found on reading previously known words faster, but no improvement was found in overall word recognition skills.
The children in the control group who received only the traditional language and reading intervention did not show significant improvement on the GORT-4 measures of reading fluency; yet, their reading fluency scores were statistically significant on the measures of Read Naturally and DIBELS-6 ORF. One possible explanation is that as the GORT-4 measures use standard scores rather than “number of words correctly read per minute” as found on the Read Naturally and DIBELS-6 ORF, the scoring protocol of the GORT-4 may not be as sensitive to gains in reading fluency as the other two measures. Nevertheless, there were obvious differences in the pattern of change of those fluency measures that appear to pertain to the effects of the IM treatment. Specifically, both groups showed significant improvement in their Read Naturally and DIBELS-6 ORF with large effect sizes reported, but again, the IM group outperformed the control group with a relatively larger effect size for both measures.
Reading Comprehension Outcome
Our second major finding was that both groups improved significantly in their reading comprehension; however, similar to the results found on the fluency subtests, the IM group outperformed the control group with a much larger effect size for the GORT-4 Comprehension subtest. This finding supports other research that suggests that as reading fluency increases, comprehension improves due to the availability of additional cognitive resources (Fuchs et al., 2001; Nation & Snowling, 1997). When the reading process becomes more automatic and fluent, the reader’s attention and other cognitive resources can be directed toward the task of reading comprehension (NRP, 2000; M. Wolf & Katzir-Cohen, 2001). When interpreting these findings, it should be noted that a single measure of reading comprehension was used in this study.
Plausible Explanations for Findings
Over the past 20 years, there has been considerable evidence that processing speed limitations are contributing factors to reading difficulties experienced by children with language and reading impairments. Research suggests that the nonphonological component of processing speed contributes to the automaticity and/or efficiency of the reading process (Buhusi & Meck, 2005; Catts, Gillispie, et al., 2002; Miller, Kail, Leonard, & Tomblin 2001; Montgomery 2005; Shanahan et al., 2006; P. Wolf, 2002). Relatedly, intervention research linking interval timekeeping with reading achievement (Schaffer et al., 2001; Taub et al., 2007) has demonstrated the potential value of IM training (i.e., a synchronized metronome tapping intervention) to use as a possible option for reading fluency intervention in school-age children. Although few in number, these intervention studies have addressed how a nonacademic treatment (i.e., IM training) could positively affect reading achievement (Schaffer et al., 2001; Taub et al., 2007).
The findings from the current study that only the IM group showed significant improvement in their rate score of the GORT-4 fluency measure and no significant change in their GORT-4 accuracy score indicates that IM treatment may be associated with improvements in speed of processing as suggested by earlier research (Buhusi & Meck, 2005; Shanahan et al., 2006; Taub et al., 2007; P. Wolf, 2002). Thus, processing speed may be the contributing factor for the greater gains in automaticity and efficiency of reading made by the IM group when compared with the control group. This interpretation is consistent with that offered by Taub et al. (2007), suggesting that increases “in the clock speed of the master internal clock” (p. 857) contribute to improvements in reading fluency and efficiency. Taub et al. reported that IM treatment appears to “demonstrate transfer effects on reading fluency/efficiency of existing word recognition skills but not increase the overall level of word recognition skills in a students’ repertoire” (p. 857).
Another plausible explanation for the finding that the experimental group had larger gain scores than the controls for reading rate/fluency and comprehension may be attributed to an increase in focus and attention as a result of IM treatment, which is consistent with prior research (Bartscherer & Dole, 2005; Schaffer et al., 2001; Taub et al., 2007). Similarly, Schaffer et al. (2001) found that students with attention deficit hyperactivity disorder (ADHD) who received IM treatment demonstrated improvements in attention, language processing, and reading. Therefore, it is possible that following IM treatment, improvement in the experimental group’s focus and attention may have led directly to an increase in their reading rate, which also could account for the increase in reading comprehension. Thus, it is conceivable that following IM treatment, improvement in the experimental group’s focus and attention may have led directly to an increase in their reading rate, which also could account for the increase in reading comprehension. Importantly, the results of our study highlight the possible additive effect that IM treatment can have on reading fluency and comprehension when integrated into a traditional language and reading intervention.
Limitations and Future Directions
The first limitation involves the lack of an untreated control group. Both the IM experimental group and the control group received the language and reading intervention and differed only in use of the IM treatment. As statistically significant gains were realized by both groups, it is not possible to conclude that IM treatment was the sole reason for the increase in reading fluency (rate) and comprehension and should be viewed with caution. Nonetheless, we argue that the results are meaningful and suggest that IM treatment does have value for improving reading fluency as suggested by earlier research (Schaffer et al., 2001; Taub et al., 2007) and does in fact facilitate an improvement in reading comprehension (NRP, 2000; M. Wolf & Katzir-Cohen, 2001).
The small clinical sample used for this study restricts the ability to generalize these findings to other populations; however, the results are consistent with previous research on IM treatment effects for improving reading fluency in typically developing children (Taub et al., 2007) and children with ADHD (Schaffer et al., 2001). An additional limitation of the study is the lack of a detailed description of each participant’s environmental influences as related to his or her motivational level and amount of literacy engagement in the home environment. Further examination of these variables may contribute to a deeper understanding of the reading fluency outcomes.
We did examine the immediate clinical effects of the integrated IM treatment after a 4-week intervention period, but it is possible that IM treatment does not provide long-lasting effects on the reading fluency of this population and this should be addressed in future investigations. The significant change in the experimental group’s GORT-4 rate and comprehension score was associated with a small amount of IM treatment (4 hr) relative to the total amount of language and reading intervention (48 hr) provided in the study. Thus, combining even a limited amount of IM treatment with a language and reading intervention proved beneficial. It is possible that extending the length of the IM treatment sessions to 45 to 50 min each day for a total of 15 to 18 hr of treatment (Taub et al., 2007) may have a greater impact on children’s reading rate/fluency and comprehension than observed in the current investigation. These considerations are critical and necessary to examine for future studies.
Clinical Implications
As stated on the IM website (IM, 2012), reading educators and speech-language pathologists are using IM training solely or as an adjuvant to a language/reading intervention to improve a child’s reading achievement. There is a great need for intervention research that clearly demonstrates the efficacy and effectiveness of IM training for improving reading in different populations. The results of this current investigation can be viewed only as a first step involving IM as a complimentary treatment to improve reading fluency and comprehension in children with language and reading impairments.
From a clinical perspective, the preliminary findings of this study highlight the benefits of IM treatment as an adjuvant to a traditional language and reading intervention in school-age children with language and reading impairments. The results of this study are the first to show that children with language and reading impairments who receive IM treatment as part of their intervention make greater gains in their reading fluency (rate) and comprehension than those who do not. However, because of the above-mentioned limitations used in this study, caution should be used in generalizing these results. To demonstrate further the effectiveness of the IM treatment, future studies with larger participant groups are necessary that focus on the long-term benefits of the treatment and the effects of a more intensive treatment extended over a longer time period.
Footnotes
Appendix
Intervention
| Language intervention | Instructional strategies | Specific steps |
|---|---|---|
| Targeted vocabulary (individual session): | Ten Tier 2 vocabulary words were selected from the book each week to be targeted for intervention (Beck et al., 2002). Tier 2 vocabulary is defined as those words that are frequently used in a language and in a variety of contexts (Beck et al., 2002). Scaffolding, word maps, visual mapping, and focused stimulation used as strategies to enhance vocabulary learning. | The steps: |
| Emphasized the use of active engagement, a variety of contexts, repeated opportunities, multisensory activities, and elaborated exposure (Beck, McKeown, & Kucan, 2002). | Friendly definition provided by clinician | |
| Syllables and sounds in words discussed | ||
| Associations and connections among words made | ||
| Multiple exposures to the target word used in a variety of oral and written contexts | ||
| Targeted vocabulary used in a variety of oral and written contexts (e.g., responses to questions, making own sentences, story retell, verbalizing, and writing stories). | ||
| Phonological awareness intervention (PAI; individual session): | Explicit instruction was provided for PAI and followed a developmental sequence (van Kleeck, 1990). A metalinguistic approach was used combining PAI with sound–symbol correspondence and print concepts as part of this treatment regime (Gillon, 2004; Kaderavak & Justice, 2004). Visual and verbal cues were implemented when the child needed additional support. | The task sequence: |
| Emphasized phonological awareness at the syllable and phoneme level thus supporting language and reading (Torgesen, Otaiba, & Grek, 2005). After and/or during the phoneme level of instruction, the correspondence of the sound and the symbol were used (Gillon, 2004). | Segment and blending syllables in monosyllabic words/polysyllabic words | |
| Identifying initial, final, and medial sound in monosyllabic words moving to polysyllabic words | ||
| Manipulating syllables and sounds in words | ||
| Finally, sound–symbol correspondence tasks by blending, segmenting, and manipulating sounds in words using letter tiles. | ||
| Narrative retells (small group session): | The Story Grammar Marker (SGM; Moreau-Rooney & Fidrych, 2002) was used for the narrative retell intervention. The clinician read the book in its entirety and then immediately modeled the narrative retell using the SGM as the visual support. In the following sessions, the participant retold the narrative with the visual support through scaffolding (e.g., questioning, cloze procedure) then later faded (Ukrainetz, 2006). Visual maps, sequenced pictures, graphic organizers, and scrambled stories were employed to extend narrative production (Roth, 2000). Grammatical errors were recast (Weismer & Robertson, 2006). | The sequence: |
| Emphasized narrative retell intervention to recount a complete episode with all of the story elements (e.g., character, setting, initiating event, feeling, plan, planned attempts to resolve the stated problem, results/consequences, and resolutions). | The clinician read the story in its entirety and then modeled the narrative retell using the SGM. Each story contained targeted morphological and narrative goals for each participant. | |
| Emphasized morphosyntax: preselected grammatical structures and syntax targeted. | The clinician then read one story component and asked the participant to paraphrase that part of the story. SGM and other supports were used initially and gradually faded. | |
| Continued until all story components were included by the client. |
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.