
Abstract
A child’s early language environment is critical to his or her life-course trajectory. Quantitative linguistic feedback utilizes the Language ENvironment Analysis (LENA) technology as a tool to analyze verbal interactions and reinforce behavior change. This exploratory pilot study evaluates the feasibility and efficacy of a novel behavior-change strategy, quantitative linguistic feedback, to influence adult linguistic behavior and, as a result, a child’s early language environment. Baseline LENA outcome measures (i.e., adult word count [AWC] and conversational turn count [CTC]) were obtained from a diverse sample of 17 nonparental caregivers and their typically developing children (charges) ages 10 to 40 months. Caregivers participated in a one-time educational intervention focusing on enriching a child’s home language environment, interpreting feedback from the baseline LENA recordings, and setting language goals for the following session. Post-intervention, six additional LENA recordings were obtained weekly to measure linguistic behavior. Caregivers showed a significant and prolonged increase from mean baseline to mean postintervention AWC and CTC as measured by LENA–AWC: mean difference = 395 words per hour, 31.6% increase, t = 3.29, p < .01; CTC: mean difference = 14 turns per hour, 24.9% increase, t = 3.54, p < .01. Preliminary results indicate that a one-time educational intervention combined with quantitative linguistic feedback may have a positive effect on caregiver language output, thus enhancing the child’s language environment. This study represents an initial step in the development and evaluation of a novel behavior-change strategy. We propose that quantitative linguistic feedback will add significantly to the arsenal of clinical and research tools used to evaluate and enrich a child’s early language environment.
Background
A child’s early language environment is critical to his or her life-course trajectory (Forget-Dubois & Dionne, 2009; Law & Rush, 2009; Phillips, 2011). Language exposure not only bears an obvious relationship to a child’s linguistic development but also significantly influences a child’s overall cognitive and educational achievement (Hart & Risley, 1992, 1995; Huttenlocher, Vasilyeva, Cymerman, & Levine, 2002; Kashinath, Woods, & Goldstein, 2006). Hart & Risley’s landmark study demonstrated a significant correlation between the number of words a child hears by age 3 and his or her ultimate IQ and academic success. Equally compelling is the literature linking the qualitative aspects of language exposure, including complexity of speech, adult-to-child interaction and responsive caregiving, with a child’s ultimate educational outcome (Bornstein, Tamis-LeMonda, Hahn, & Haynes, 2008; Huttenlocher, Haight, Selzer, & Lyons, 1991; Kaiser & Hancock, 2003a, 2003b; Landry, Smith, Swank, & Guttentag, 2008; Landry, Smith, Swank, & Miller-Loncar, 2000; Reilly et al., 2010; Snow, 1972). This research demonstrates clearly that a qualitatively and quantitatively rich early language environment is paramount for a child to realize his or her linguistic potential and, ultimately, life-course potential as well.
Disparities in early language environments, along with their profound lifelong consequences, have been demonstrated in children with developmental disabilities such as autism, children with intellectual disabilities, children with hearing loss whose parents are hearing, and children with specific language impairments (SLI), as well as children of low socioeconomic status (SES; DesJardin & Eisenberg, 2007; Hammer, Tomblin, Zhang, & Weiss, 2001; Hoff & Tian, 2005; Huttenlocher et al., 1991; Meadow-Orlans, 1997; Reilly et al., 2010; Rowe, 2008; Spencer & Gutfreund, 1990). These populations have been demonstrated to have significantly reduced quantitative and qualitative parental linguistic input. As such, it has been estimated that children living in poverty will have heard 30 million fewer words by age 3 compared with their more affluent peers (Hart & Risley, 1995). This gap in linguistic input mirrors an academic achievement gap that is evident from the first day of school and persists throughout adulthood (Phillips, 2011). Children with hearing loss in particular, regardless of SES, have been shown to have significant disparities in language experiences when compared with normal-hearing peers. In low-SES children, language disparities are most often associated with less exposure to and facility with academic language (Snow, 1972). For children with hearing loss, however, it is the fundamental development of listening and spoken language that is at risk.
Clinical interventions for children who have speech and language delays often target the adult caregiver as the catalyst for improving the child’s language development (Kaiser & Hancock, 2003a; Kashinath et al., 2006; McWilliam, 2001; Pickston, Golbart, Marshall, Rees, & Roulstone, 2009; Reese, Sparks, & Leyva, 2010; Roberts & Kaiser, 2011). As the primary contributors to their child’s language environment, adult caregivers are able to enrich their child’s home language environment throughout the child’s day. This family-centered approach is fundamental to the federally funded early intervention programs for young children with disabilities (Individuals With Disabilities Education Improvement Act of 2004, 2003). While the intervention literature focuses primarily on parental caregivers, the literature also supports the incorporation of nonparental caregivers (NPCs; Giurolametto, Weltzman, & Greenberg, 2003, 2004; Milburn, 2011). Intervening with NPCs is an important method for improving the child’s language environment as NPCs care for the majority of 0- to 4-year-old American children; 77% of children of employed mothers received care from NPCs in 2010 (Table FAM3.A. Child care: Primary child care arrangements for children 0–4 with employed mothers by selected characteristics, selected years 1985–2010).
The literature strongly supports the potential for improving the child’s language outcome via the adult caregiver (Roberts & Kaiser, 2011). In a meta-analysis of 18 parent-implemented language interventions, Roberts and Kaiser found significant improvements in receptive and expressive language skills of children 18 to 60 months of age (Roberts & Kaiser, 2011). Although the interventions had varied approaches, philosophies, and target populations, overall Roberts and Kaiser found that, with relatively modest training, parents successfully implemented language interventions, which in turn positively affected children’s receptive and expressive language. Most interventional approaches that Roberts and Kaiser reviewed included a broad “social communication focus,” with linguistic strategies designed to be integrated into daily routines (Roberts & Kaiser, 2011). The two most common linguistic approaches aimed to affect “what the parents say” and “how much the parents say” (Roberts & Kaiser, 2011). Interventions also sought to enhance parent–child interaction via increased parental responsiveness to the child’s attempts to communicate.
Despite the generally positive outcomes, Roberts and Kaiser (2011) identified a number of weaknesses in the interventions reviewed. They found a lack of detailed descriptions of the interventions, resulting in an inability to pinpoint the intervention components that correlated with specific language improvement (Roberts & Kaiser, 2011). In addition, many studies failed to accurately assess caregiver intervention uptake, sustainability of caregiver language behavior change, or the necessary child intervention dosage, for example, frequency and length of intervention program (Roberts & Kaiser, 2011). Furthermore, the primarily middle-class study participants raised the question of external validity and generalizability of results.
These shortcomings mirror a similar concern in the overall health promotions literature, where studies of complex behavioral interventions often lack clarity in descriptions of behavioral strategies used (Michie, Johnston, Francis, Hardeman, & Eccles, 2008). It has been suggested that the modest behavioral effects often found in interventions are linked to this lack of transparency and well-defined behavior-change strategies used in these interventions (Michie, Fixsen, Grimshaw, & Eccles, 2009). In response to these limitations, the health promotions field has advanced a taxonomy of theoretically based behavior-change techniques (Michie et al., 2011). Michie et al. have proposed a comprehensive group of 40 discrete evidence-based behavior- change techniques, which they term CALO-RE 1 taxonomy. The CALO-RE taxonomy of strategies is not specific to a particular behavioral intervention type (e.g., smoking or weight loss) but is, rather, a methodological tool that can be generalized to any health promotion intervention. The ultimate goal is to eliminate the ambiguities of interventional strategies so the specific factors and their specific effects in an intervention are understood. The literature provides compelling evidence that incorporating these theoretically based behavior change techniques into health promotion interventions is essential to stimulating sustainable behavior-change and advancing the science of behavior change (Abraham & Michie, 2008; Michie et al., 2005; Michie, Jochelson, Markham, & Bridle, 2009).
Aims
It is with appreciation for the critical need for theoretically based behavior-change strategies in caregiver-directed language interventions that we describe our preliminary pilot testing of a novel, multifaceted behavior-change strategy we call quantitative linguistic feedback. This strategy has been developed to facilitate changes in language behavior of adult caretakers and to quantify the impact and sustainability of intervention in adult linguistic behavior. It is designed to be incorporated into and enhance any existing caregiver-directed interventions.
The theoretical underpinnings of quantitative linguistic feedback are Bandura’s social cognitive theory (SCT), the theory of planned behavior (TPB), self-determination theory (SDT), and the health belief model (HBM; Ajzen, 2001; Ajzen, Brown, & Carvajal, 2004; Bandura, 1997; Vansteenkiste & Sheldon, 2006). These theories of behavior change must be factored into the development of successful behavioral intervention techniques (Michie et al., 2008). Guided by such theories, we developed quantitative linguistic feedback with a multifaceted approach that includes a mechanism by which adults can set and respond to goals (TPB and goal setting), utilize cues for action or external prompts for behavior change (HBM), recognize the improved language environment they are providing for their child, and develop a sense of competency and autonomy in facilitating their child’s development (SCT).
TPB describes “intention” as a critical determinant of behavior. Health intention is, itself, determined by beliefs and attitudes about treatment (e.g., medication efficacy and adverse effects), subjective social norms (e.g., concern with the opinions of others), past experience (e.g., previous experience with similar programs), and perceived behavioral control and self-efficacy (Hagger, Chatzisarantis, & Biddle, 2001). Attitudes, both favorable and unfavorable, will affect intention and, ultimately, action and adherence, or the lack thereof (Ajzen, 1996; Hagger, et al., 2001; White & Wellington, 2009). Quantitative linguistic feedback encompasses intention by incorporating goals to be set and accomplished, and, most critically, engages caregivers as goal setters.
HBM maintains that “readiness” to change behaviors is “activated” by motivational feedback and “cues to action” (Janz, Champion, & Stretcher, 2002). External prompts are cues to action, which in turn stimulate behavior change. In quantitative linguistic feedback, “cues to action” are the Language ENvironment Analysis (LENA) data that provide concrete evidence of a child’s language environment and patterns of change.
Finally, Bandura’s SCT recognizes self-efficacy―the “belief in one’s capacity to organize and execute the courses of action required to produce given attainments”―as critical for the success of all interventions (Bandura, 1997). Bandura writes that a sense of self-efficacy is essential any time a parent is to take action on behalf of a child’s education or health status, or act as a child’s teacher and advocate. DesJardin and Eisenberg (2007) also found that caregiver self-efficacy is strongly related to the linguistic skills of young children with hearing loss. Self-efficacy is also associated with more sophisticated language strategies, such as open-ended questioning and parallel talk, which are in turn correlated with improved language outcomes (Hughes & Demo, 1989; Johnston-Brooks, Lewis, & Garg, 2002; Raikes & Thompson, 2005; Wolf et al., 2007).
Given these theoretical foundations, the parent-directed educational intervention was designed to (a) review the importance of a child’s early language environment in relation to later language proficiency, (b) understand how the LENA measures certain critical aspects of this environment (i.e., adult word count [AWC], conversational turn count [CTC], TV Time [TVT]), and (c) discuss strategies to help parents enrich their child’s language environment.
The technological centerpiece of quantitative linguistic feedback’s behavior-change intervention is the LENA System. The LENA is an innovative recording device that, along with its accompanying computer software, can be used to automatically capture and analyze a child’s home language environment (Oller, 2010). The LENA quantifies the number of words to which a child is exposed and the number of conversational turns the child takes with adult(s) over a continuous 16-hr period (Gilkerson & Richards, 2008). The LENA’s quantitative outcome measures are then presented to caregivers, providing them with concrete feedback about where need for greater language exposure exists and where improvement has been made. Thus, the LENA’s value is not simply for scientific quantification but for providing feedback to the adult caregivers. In collaboration with a therapist, caregivers can clearly see a snapshot of the home language environment, consider their role within it, discuss opportunities to enrich that environment, and importantly, chart and track progress toward enrichment. In other words, the quantitative outcome measures are utilized as a type of “biofeedback” used for goal setting and measuring progress toward those goals. Thus, this quantitative linguistic feedback can be used to reinforce traditional approaches used in a wide variety of language-development focused interventions.
Quantitative linguistic feedback is a multifaceted technique for behavior change that may work through a number of different mechanisms as described in the CALO-RE taxonomy (Michie et al., 2011). For adult caretakers, quantitative linguistic feedback offers a mechanism by which they can set and respond to goals, utilize cues for action or external prompts for behavior change (e.g., reviewing LENA outcome measures), and recognize the improved language environment they are providing for their child. It also instills a sense of competency and autonomy in facilitating their child’s development.
Our initial work evaluating quantitative linguistic feedback’s feasibility and efficacy in improving adult quantitative language behavior is presented here. We hypothesized that quantitative linguistic feedback would result in a significant increase in AWC and CTC as measured by the LENA. Subsequent efforts will focus on demonstrating a corresponding qualitative improvement, sustained linguistic change, as well as methods for incorporating this novel strategy into existing interventions. Ultimately, the technique of caregiver-directed, quantitative linguistic feedback holds the promise for significantly improving child language outcomes.
Method and Procedures
Design
The study used a prospective case-crossover design involving two baseline recordings followed by a single educational intervention and six postintervention LENA feedback recordings. This exploratory pilot study was conducted with a group of NPCs who were chosen because of their extensive, focused, and consistent periods of time with the children in their care.
Participants
NPCs
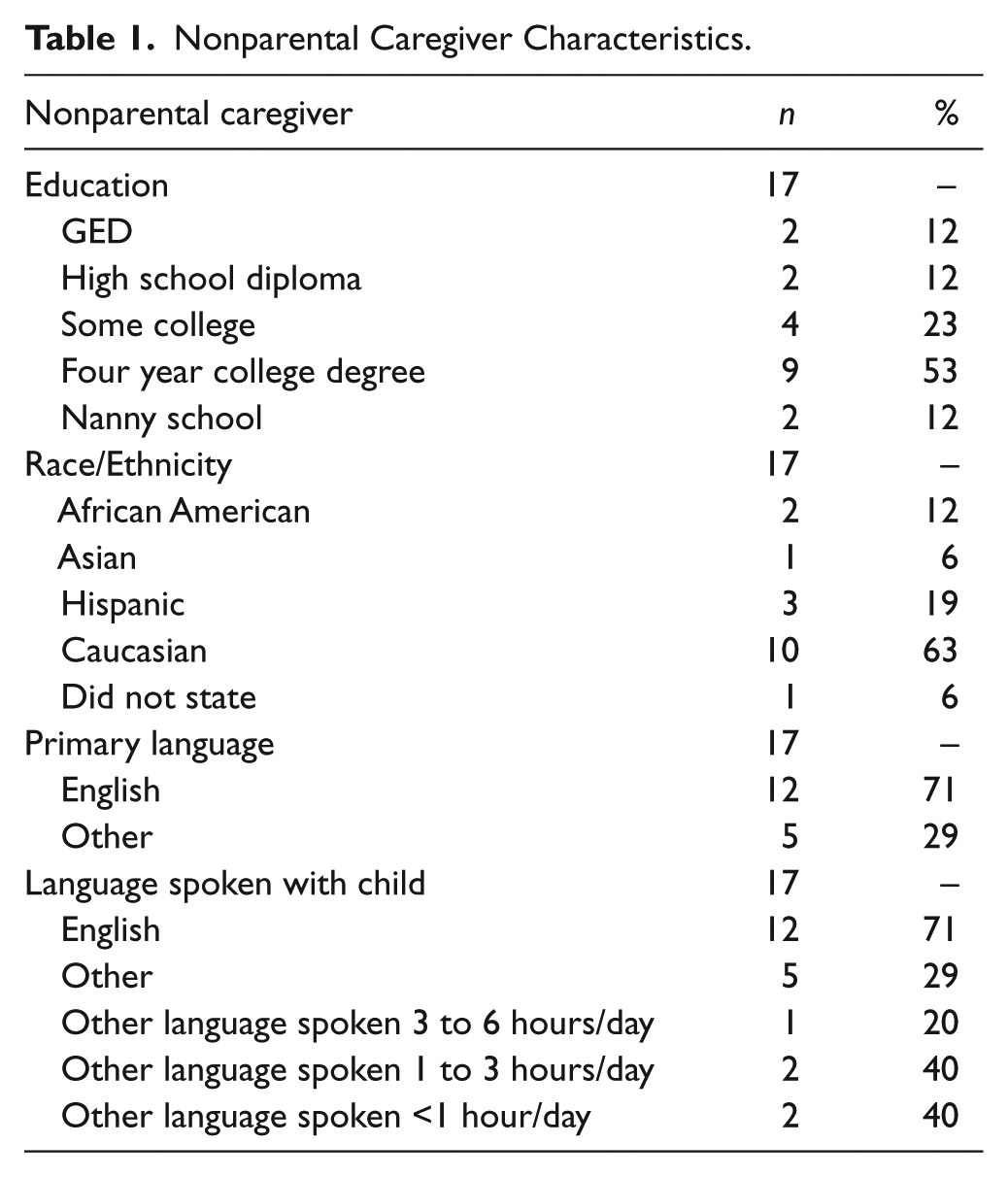
Nineteen English-speaking NPCs caring for typically developing children were recruited for this study. Of the 19 recruited NPCs, 17 (90%) completed the study and are included in the present analysis. One NPC dropped out secondary to pregnancy, and another withdrew due to scheduling difficulties prior to obtaining baseline recordings. A table of NPC demographics is shown in Table 1. All NPCs were women and ranged in age from 23 to 53 years (M = 33.1, SD = 10.1). Their education levels ranged from GED to 4-year college degree, with approximately half having a 4-year degree (n = 9; 53%). Two NPCs (12%) received specialized child care training (i.e., nanny school). Ten NPCs (59%) were Caucasian, with the other 6 representing a range of races and ethnicities, including African American (n = 2; 12%), Asian (n = 1; 6%), and Hispanic (n = 3; 18%). Nearly one third of the NPCs (n = 5; 29%) spoke English as a second language. On average, NPCs had 9 years of experience caring for children (SD = 7, range = 2–28) and a range of 2 months to 3 years caring for the child in this study (M = 1 year, SD = 9 months). Five of the NPCs (n = 5/17, 29%) cared for at least one other child simultaneously with the child in the study.
Nonparental Caregiver Characteristics.
Children and families
Seventeen families participated in this study: 10 girls (n = 10; 59%) and 7 boys (n = 7; 41%). Ages ranged from 10.5 to 40.3 months (M = 20.4 months). In families with multiple children, 1 child between the ages of 10 and 42 months was eligible for inclusion in the study. Eight children (47%) had one sibling, with four of the siblings younger and one older. One child (6%) had two siblings, with one younger and one older (see Table 2). Five children received primary care from their mothers (9%), 1 child from his or her NPC (6%), 10 from their mothers and NPCs (9%), and 1 from his or her mother and father (6%).
Family Characteristics.
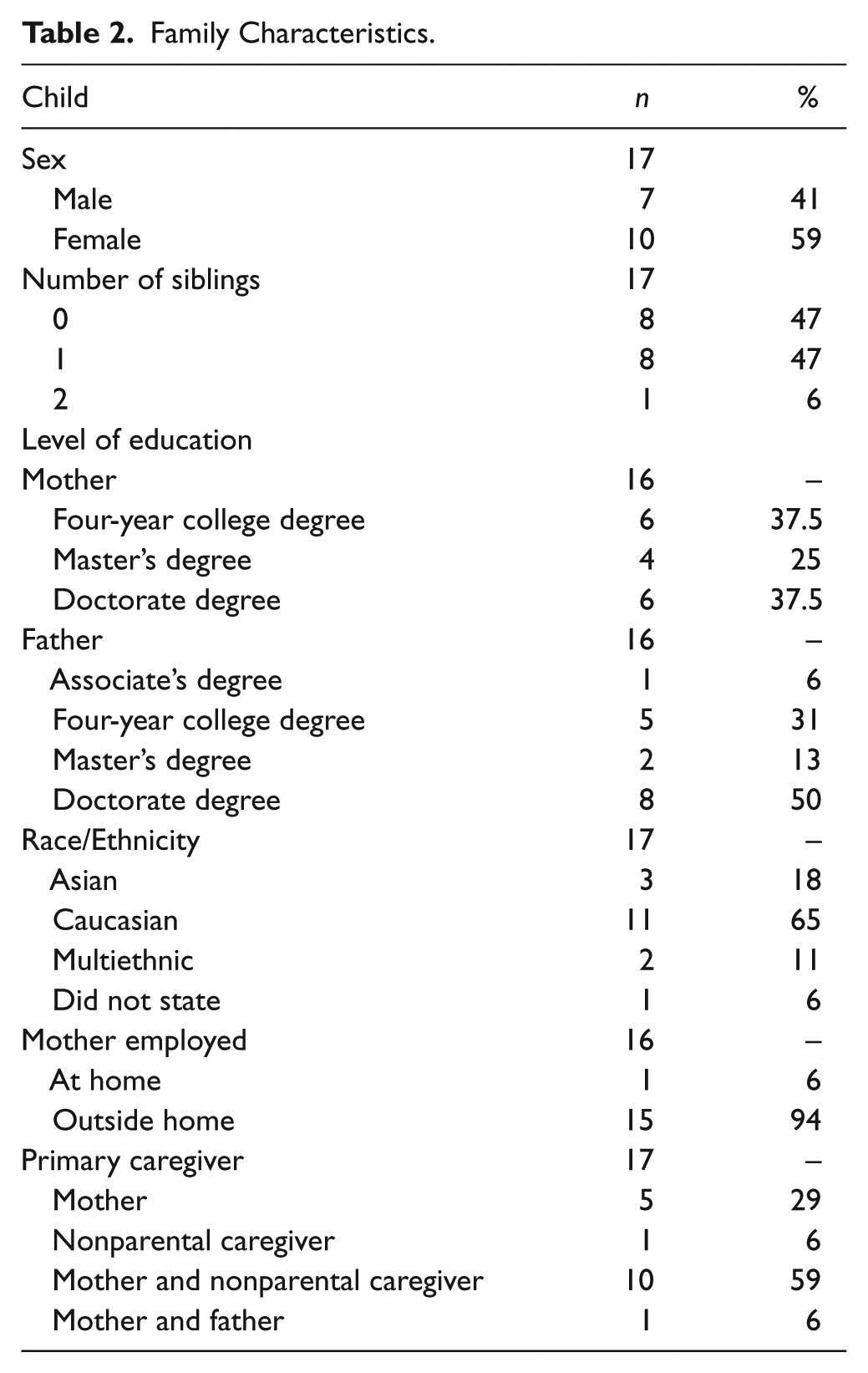
All children were from two-parent households with annual incomes of US$100,000 or more. One parent had an associate’s degree, whereas the rest of the parents in the study had a 4-year college degree or higher. Forty-one percent of parents (n = 14) had attained doctorate degrees. Eleven families responded as Caucasian (65%), three as Asian (18%), two as multiethnic (12%), and one family declined to state (6%). All families spoke English as the primary language at home. Five were bilingual, but reported that they spoke their second language less than 1 hr per day.
Materials and Procedures
Recruitment
English-speaking NPCs caring for typically developing children were recruited through professionals at the University of Chicago and the surrounding area via email, online postings, and word of mouth. NPCs were paid US$100 for completion of the study. Informed consent was obtained from parents and NPCs. The consent forms included an agreement that parents would not know or ask for their NPC’s results or feedback.
Demographic and home language survey
NPCs and one parent from each family completed a demographic survey, which included items about race, ethnicity, education, and household income. The instrument also included a home language survey, which included questions about typical daily schedules, the amount that the child talked, the amount that NPCs and parents spoke to the child, and the amount of time children were exposed to TV during a typical day.
Interventionists
Two graduate-level research assistants involved in the development of the 1-hr educational intervention performed all interventions. Training and practice occurred with the principal investigator (Suskind) prior to commencement of interventions.
Recording procedure
At the start of the study, NPCs were each given a LENA digital language processor designed to be worn by the child in the front pocket of a specially made t-shirt. At the beginning of each recording day, NPCs wrote down the recording start time and then placed on the child the shirt containing the LENA device. The LENA device records up to 16 hr of audio, and requires a minimum of 12 hr of data for complete and accurate processing. Because the NPCs all worked less than 12 hr per day, they were instructed to keep the device turned on for the maximum recording duration and to write down the timestamp present on the digital display when their interaction with the child ended for the day (i.e., when they left the child’s home or when the child was put to bed). NPCs each made a total of eight recordings during the course of the study: two baseline recordings prior to intervention and six postbaseline recordings. We used the average of the two baseline recordings as their baseline measure.
Educational intervention
After baseline recordings were completed, each NPC participated in a language-focused educational intervention lasting approximately 1 hr at the child’s home. This session included information on child language development, along with tips for increasing their talk and conversational turn-taking with the child. The educational session was conveyed via a short PowerPoint presentation, and included the following core components: (a) review of the importance of a child’s early language environment (i.e., connection between caregiver linguistic input and a child’s language and educational success), (b) discussion of LENA and its target measures (i.e., AWC and CTC), (c) review of caregiver baseline LENA recordings, and (d) discussion of strategies to enrich a child’s early language environment and raise LENA measures through talking more and increasing conversational turns with a child.
Quantitative linguistic feedback
The research assistant then provided the NPCs with their individual LENA linguistic feedback from the baseline recordings, and facilitated the NPCs’ understanding of the LENA feedback reports and goal setting for the following recordings. LENA feedback reports included raw numbers, percentiles, and graphic representations of mean hourly AWC and CTC. Interventionists discussed with NPCs specific results, methods for increasing AWC and CTC, and goal setting for upcoming recordings. In addition, NPCs demonstrated ability to accurately interpret and understand feedback at the end of the interventional session.
After the educational intervention, NPCs made recordings once weekly for 6 weeks and received their LENA feedback results halfway between each recording session. No active discussion or goal setting was performed by the interventionist beyond providing the results in paper form.
Data Processing
Data were uploaded from the LENA recorders into a study computer. All data were then processed into counts by LENA ADEX software. Audio recordings were discarded to protect the privacy of the participants per IRB-approved research protocol. Language-related outcomes were assessed on three main measures: AWC, CTC, and child vocalization count (CVC). Naptime as well as NPC-child interaction start and end time parameters were set using the information NPCs provided in their initial surveys and on their daily recording time sheets. A computer script was written to filter recordings during nap periods. Once filtered, all counts were then standardized by total relevant interaction time and were expressed as either words per hour (wph) or turns per hour (tph).
Statistical Analysis
Repeated measures ANOVAs were conducted for each of the four LENA measures (i.e., AWC, CTC, CVC, and TVT), with Time (postintervention Sessions 1, 2, 3 to 6) as the within-subject variable, to determine whether there were significant differences among postintervention recording time points. No significant differences were found for any of the four LENA measures. As such, the counts for each of the six postintervention time points were averaged to create a single postintervention score for each of the four LENA measures. Paired t tests were then carried out to compare the pre- and postintervention mean standardized counts.
Outcomes and Results
Home Language Survey
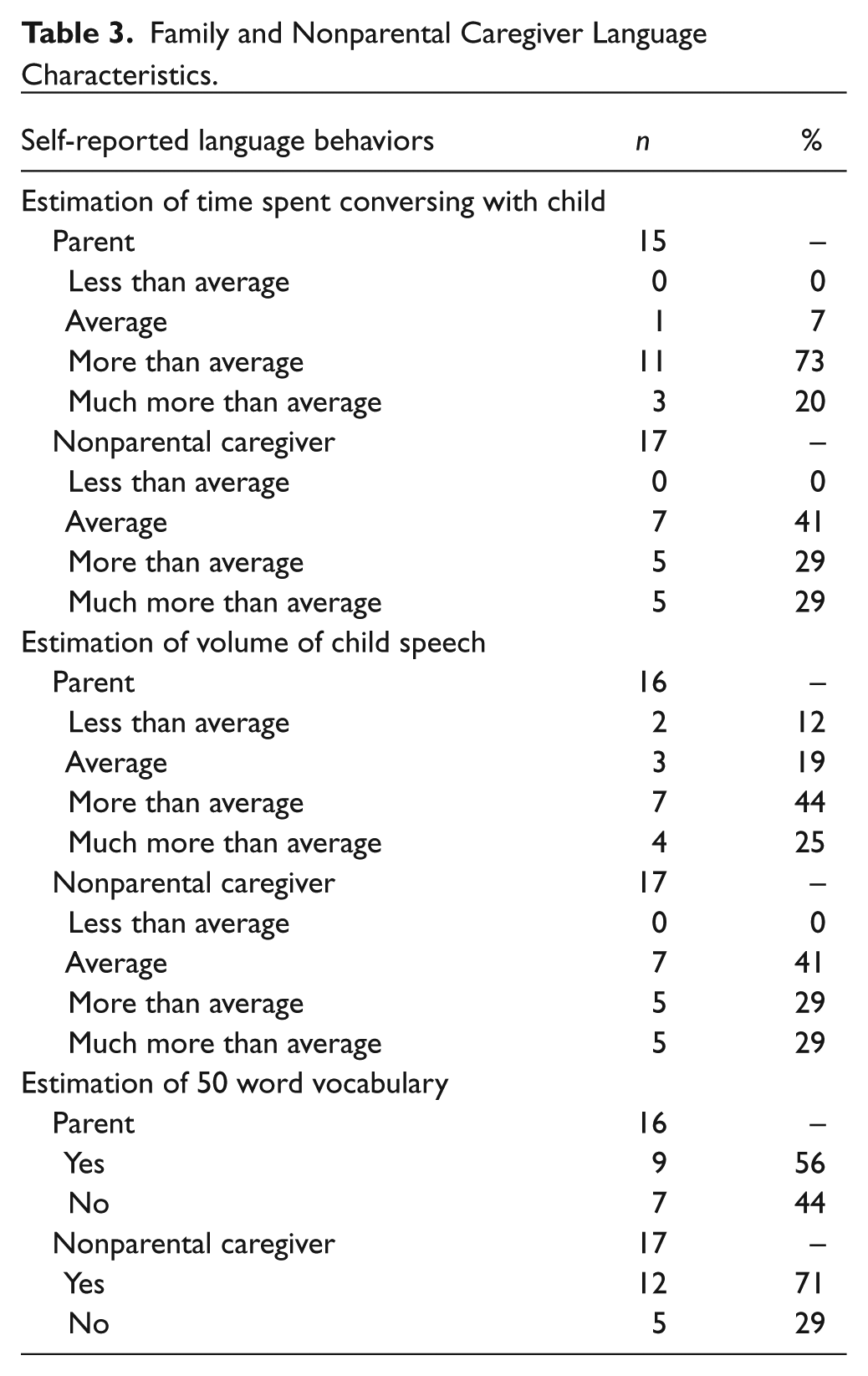
NPCs and parents were asked to rate the amount that the child talked on a 5-point scale from much less than average to much more than average. Their responses are shown in Table 3, with 10 NPCs (59%) and 11 parents (65%) rating their children as above-average talkers. When asked how much they conversed with their child, a majority of parents (n = 11; 73%) stated they talked to their child more than average. One parent (7%) rated herself as average. Three parents (20%) rated themselves as talking to their child much more than average. In response to the same question, 7 NPCs (41%) responded that they talked to the child an average amount, whereas 5 (29%) thought they talked more than average, and the remaining 5 (29%) reported talking much more than average.
Family and Nonparental Caregiver Language Characteristics.
Overall, NPCs and parents reported low amounts of child television exposure. NPCs reported that the television was on from 0 to 3 hr per day while they were with the child (M = 0.8 hr, SD = 0.9 hr). Similarly, parents reported watching 0 to 3 hr of television per day at home (M = 1.24, SD = 1.02).
LENA Outcome Measures
Caregivers contributed two recordings at baseline prior to intervention and six postbaseline recordings. Baseline recordings were made 4.8 days apart on average (SD = 7.5, range = 1–33). Because of the Hawthorne effect, the average of the two baseline measures was to make pre- and postintervention comparisons (Wolfe & Michaud, 2010). Indeed, AWC was marginally significantly higher for the first baseline session than for the second (M difference = 413 wph, 28.4%, t = 2.25, p < .04). In contrast, the CTC baselines did not differ significantly (M difference = 12 tph, 19%, t = 1.64, p < .12) nor did the CVC baselines (M difference = 26 vph, 10.4%, t = 1.71, p < .11). The six postbaseline recordings were made from 1 to 89 days post-intervention (M = 25 days, SD = 19 days). The average interval between postintervention recordings was 8 days (SD = 6 days).
TVT overall
The TVT recorded in the child’s aural environment during waking hours was low for all children in the study, with an average of 22.8 min at baseline (range = 1–63 min, SD = 16.1 min). Mean amount of TVT did not differ significantly between baseline and postintervention recordings (M difference = 0.57 min, 2.5% decrease, t = 0.14, p < .89).
AWC overall
As seen in Figure 1, mean AWC from postintervention recordings was significantly higher than mean AWC at baseline (M difference = 395 wph, 31.6% increase, t = 3.29, p < .01). Figure 2 shows AWCs at baseline and at each of the six postintervention sessions.
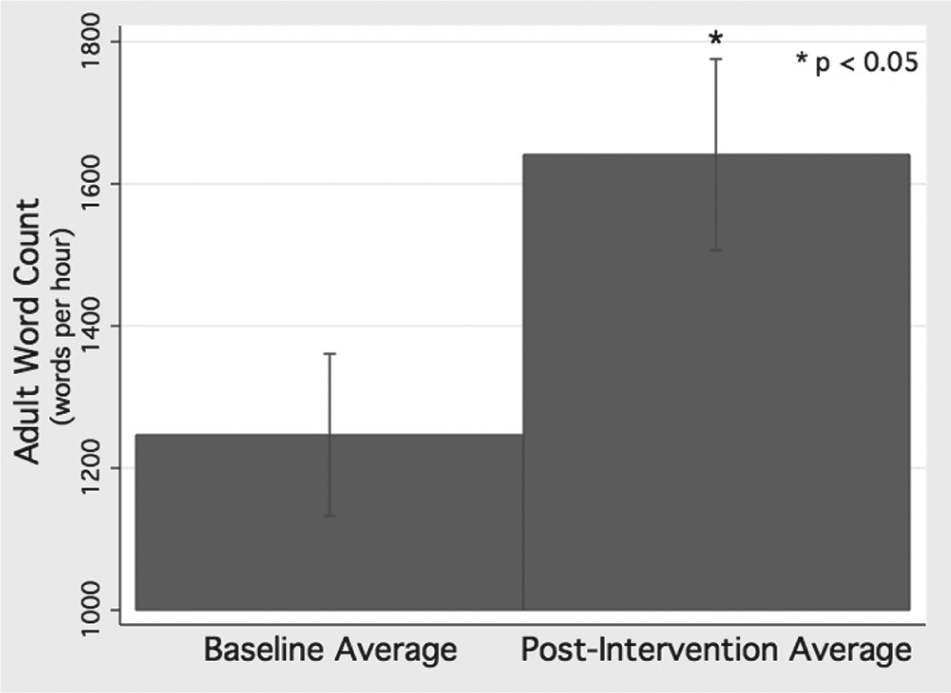
Adult word count baseline and postintervention averages in words per hour.
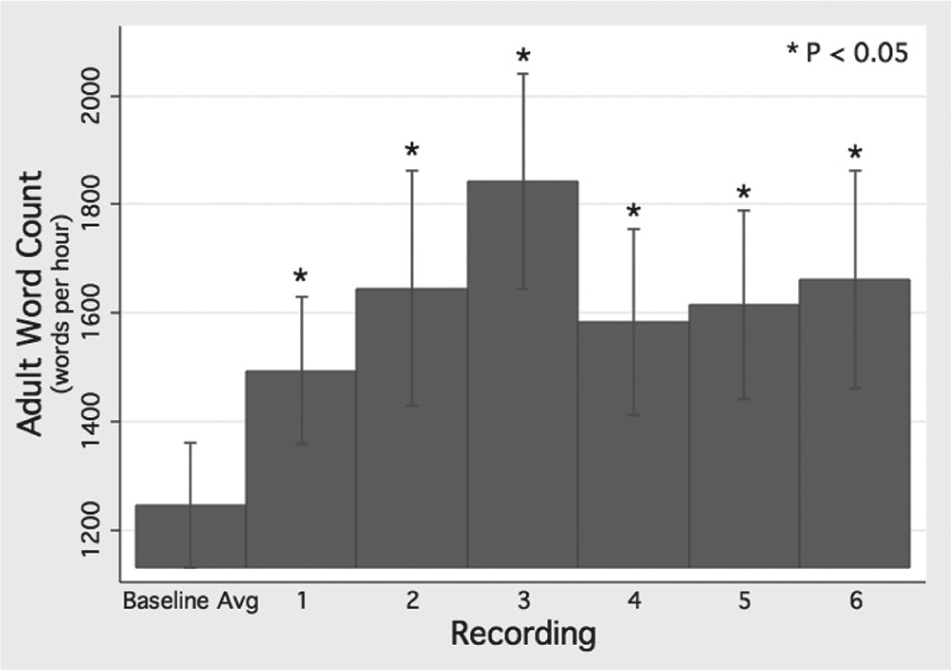
Adult word count in words per hour at baseline and 6 weeks post-intervention.
CTC overall
The mean postintervention CTC was significantly greater than the baseline average, shown in Figure 3 (M difference = 14 tph, 24.9% increase, t = 3.54, p < .01). Figure 4 graphs CTCs at baseline and at each of the six postintervention sessions.
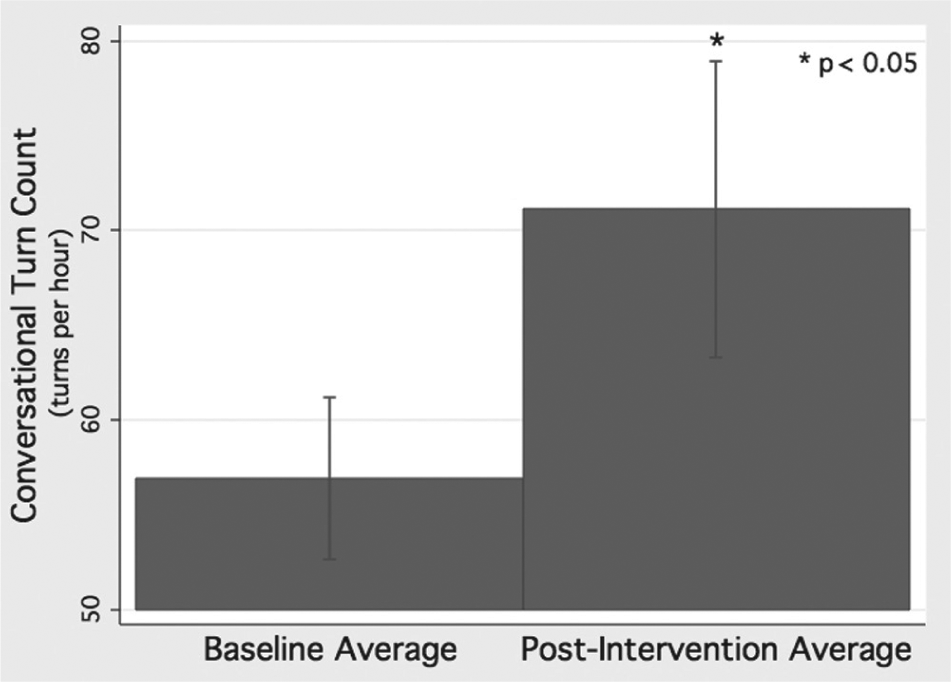
Conversational turn count baseline and postintervention averages in turns per hour.
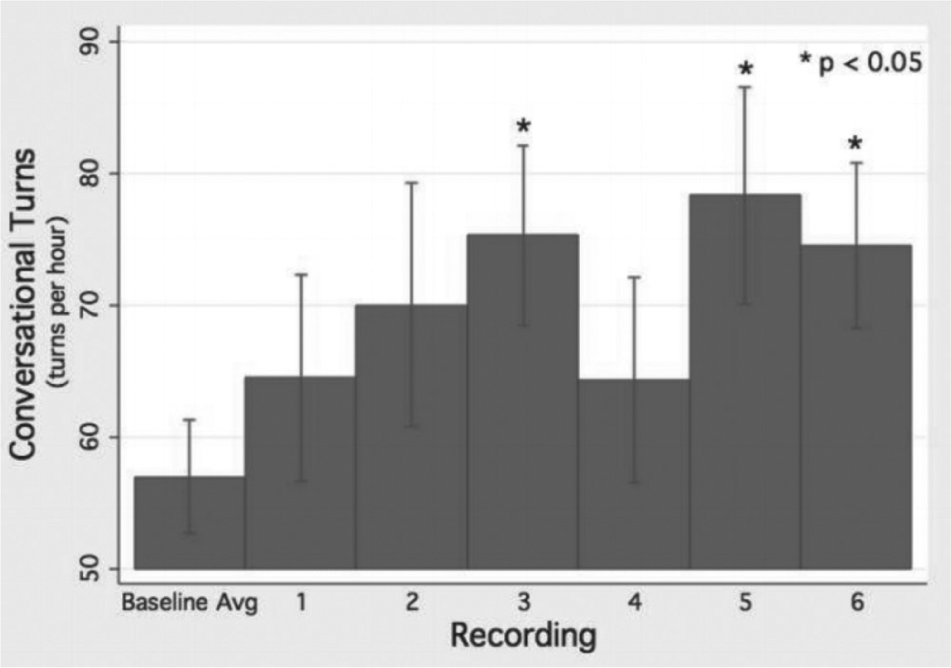
Conversational turn count in turns per hour at baseline and 6 weeks post-intervention.
Conclusion and Implications
Discussion
The primary goal of our exploratory pilot was to evaluate the novel behavior-change strategy of quantitative linguistic feedback and its effect on adult linguistic behavior. Our study comprised an initial 1-hr educational session, six weekly LENA recordings, and the use of quantitative feedback from those recordings to improve language outcomes. The significant increases seen in adult quantitative language output for AWC and CTC indicate the potential of the quantitative linguistic feedback technique to inform adults to motivate them to modify their interactions with children and provide a richer language environment.
Pedometers offer a useful analogy for understanding the quantitative linguistic feedback technique and clarifying its impact. Pedometers provide a quantified, easily grasped conceptual framework for behavior change; hence, the health promotion concept of “10,000 steps a day” (Shape Up America, Get Up and Go! 10,000 Steps a Day, 1994). Behavior-change literature evaluating the pedometer as a form of quantitative feedback shows that pedometers have been very successful in encouraging sustained physical exercise and movement in all populations, including low-income individuals (Clarke et al., 2007; Duru, Sarkisian, Leng, & Mangione, 2010; Strath et al., 2011). Adults are rarely conscious of their own “word count,” even if they understand its impact on their children’s development. With LENA feedback technology, as with pedometers, they can see the language environment they provide for their child, begin to understand their critical role, and make appropriate behavioral changes. Although the LENA feedback is not instantaneous like the pedometer, it gives adults unprecedented insight into and concrete appreciation of their child’s language environment and overall development.
However, an enriched early language environment requires more than a purely quantitative measure. It is a complex interplay of rich qualitative language and responsive behaviors. Linguistic feedback is designed to significantly increase adult language quantity to provide a foundation on which qualitative behavioral strategies may be layered. It is the combination of quantity and quality in a child’s early language environment that will lead to optimal cognitive and educational outcomes.
We view quantitative linguistic feedback not as a “silver bullet” but rather as a strategy to increase the effectiveness of behavioral interventions. As an effective addition to clinical therapy sessions, it can provide parents and therapists additional proof of behavioral change. Analyses of LENA audio recordings can also provide greater insight into the qualitative changes. The LENA technology’s ease of use and automated software processing make it ideal for inclusion in all caregiver-directed interventions involving language feedback. Although privacy protections maintained under IRB protocols for this pilot precluded qualitative analysis by requiring the deletion of audio recordings, future projects will include such evaluation.
This pilot study has demonstrated the potential of quantitative linguistic feedback, laying the groundwork for its continued iterative development as an evidence-based behavioral approach. Quantitative linguistic feedback may also have an even greater role in areas such as individual therapy. Because of the wide diversity of client populations and the limited insight therapists may have into individual home environments, they are often forced to use a generalized therapeutic approach rather than one tailored to the specific family. This is especially true regarding the child’s early home language environment. The LENA may allow therapists to gain greater understanding of a family’s baseline linguistic style so they can personalize their clinical approach. In addition, the LENA provides ongoing information to therapists with regard to their clients’ therapeutic uptake. Just as personalized medicine lets oncologists individually adapt therapeutic regimens to specific cancer characteristics, so also does quantitative linguistic feedback provide insights that help therapists provide the appropriate therapy to each patient.
Quantitative linguistic feedback may also be a valuable tool for the greater scientific community. As Roberts and Kaiser (2011) noted, advancing the science of evidence-based behavioral interventions requires transparency of strategies used and quantifiable outcome measures of parental behavioral uptake to quantify intervention dosage. Quantitative linguistic feedback is a concrete behavioral strategy that corroborates fidelity of implementation of interventional strategies as well as gauges parental behavioral uptake. Although a current limitation of the linguistic feedback is its lack of qualitative measurement, in future studies, the LENA’s audio recordings may be analyzed for qualitative changes as well. This pilot represents only the beginning in the iterative development and testing of this novel multifaceted approach. The results of this study suggest that the LENA has the potential to be a valuable addition to the world of speech and language intervention.
Considerations
The study was limited in three areas: participant sample, potential Hawthorne effect, and variance accounted by the educational intervention. Although our sample size was small, we were encouraged by the ability to demonstrate a statistically significant increase in our selected adult language parameters. In addition, caregivers with and without a college education appeared responsive to the behavioral strategy. We plan to investigate with a larger sample size the issues of external validity related to the inclusion of NPCs as opposed to parents. We hypothesize that parents will be more invested and motivated for behavioral change when it is their own child who benefits.
An important issue to consider is that of overall linguistic implications, in terms of the sustainability of the linguistic behavior change and the true nature of this effect on a child’s early language environment. There is the issue of the “Hawthorne effect,” which states that individuals positively modify their behavior when they are knowingly being observed. An individual’s knowledge that one is being recorded and will be receiving feedback may result in caregivers increasing linguistic input only during the recording times. Quantitative linguistic feedback will never entirely avoid this issue, although sustaining increased talk for a 10-hr recording day is much less likely than being on best behavior during the 1-hr videotaped session typical in most intervention studies. In addition, the NPCs in our study knew that their employers would not have access to their results. To address this limitation, future studies will include greater number of LENA recordings to habituate caregiver response as well as LENA recordings without feedback to assess sustainability of behavioral change.
Finally, the 1-hr educational intervention and initial baseline LENA feedback were inseparable in this study. We are unable to isolate the impact of the LENA feedback from the educational session on NPC behavior recorded over the six remaining recordings. However, the behavioral literature has shown that lack of continued feedback results in attenuation of effect. We suspect that quantitative linguistic feedback was responsible for the sustained changes in the AWC and CTC. To address this limitation, in future studies, we will experimentally manipulate the number of times caregivers are provided with quantitative linguistic feedback after the educational intervention. Future embedding of quantitative linguistic feedback into established interventions, inclusion of a control group and analyses of child outcomes will also help address these limitations and confirm the effects of intervention.
Conclusion
Enhancing a child’s early language environment represents an extraordinary opportunity to affect the life trajectory of a child. Pilot testing of the innovative behavioral strategy—quantitative linguistic feedback—demonstrates its potential for stimulating changes in adult language behavior. Because of these encouraging results, we will continue the development and study of this promising strategy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflict of interest with respect to the research, authorship, and/or publication of this article: The LENA recorders used in this study were on loan from the LENA Foundation.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received internal funding from the Department of Surgery at the University of Chicago as well as funding from the Hemera Foundation.