
Abstract
The purpose of this study was to investigate if intervention based on a mobile application would improve the print knowledge and vocabulary of preschool children with and without hearing loss. This was a multiple baseline study that included four preschool children. Two of the children had hearing loss and utilized cochlear implants, while the other two had normal hearing. Clinicians utilized a mobile application to facilitate print knowledge (i.e., sound-symbol relationships) and to acquire new vocabulary. By the end of the study, all four children demonstrated improved familiarity with the targeted letter sounds and improved knowledge of the vocabulary words that were utilized during the study. The results of this study indicate that the mobile application, in combination with clinician scaffolding, was an effective tool for facilitating early literacy skills in preschool children. Prior print knowledge and vocabulary development appeared to be stronger indicators of response to treatment than hearing status.
Keywords
Print knowledge, or familiarity with letter names and corresponding sounds, is one of the earliest and best predictors of early reading success in young children (Foorman, Anthony, Seals, & Mouzaki, 2002). Print knowledge is necessary for automatic identification of letter sounds and transformation of written symbols into language. Young children learn letter names and corresponding letter sounds from a combination of print exposure and direct instruction (Justice & Kaderavek, 2004). Once a strong print knowledge foundation has been established, children are more likely to progress toward eventual mastery of more advanced literacy skills.
It is reasonable to hypothesize that the acquisition of print knowledge in children with cochlear implants (CIs) holds unique instructional considerations, as print knowledge includes mapping sounds to symbols. This linking of symbol and sound is dependent on, in part, efficient and effective sound-signal processing. In a recent study investigating the early literacy skills of children with CIs, Ambrose, Fey, and Eisenburg (2012) compared children with CIs (n = 24) with children with normal hearing (n = 23). The results of this study indicated that print knowledge was associated with oral language, speech perception, and speech production in children with CIs. Interestingly, the children with CIs demonstrated similar print knowledge to children with normal hearing. These results suggest an optimistic expectation for the literacy development of children with CIs. However, because the literacy instruction received by the participants in the study was not available, the influence of hearing loss on the development of print knowledge requires further investigation. In particular, there is a need to identify evidence-based methods that promote print knowledge in children with CIs.
Tucci, Trussell, and Easterbrooks (2014) reviewed publications that evaluated strategies for developing the print knowledge skill of grapheme–phoneme correspondence in children who have hearing loss. The authors identified articles published between 1990 and 2012 through use of search terms related to grapheme–phoneme correspondence (e.g., phoneme, grapheme, morpheme, viseme, orthography, phonological awareness, coding, decoding, and morphology) and hearing loss (e.g., deaf/hard-of-hearing [DHH], hearing loss, hearing impaired, CI, American Sign Language [ASL]) and limited to intervention. Nine articles were identified that included single-case, quasi-experimental, and case study designs. Intervention strategies included visual phonetics, lexicalized fingerspelling, and semantic and iconic representation of phonemes. Each of these interventions demonstrated a positive impact on grapheme–phoneme correspondence; however, as previously stated, only nine intervention studies were identified across the 20-year span, with no two articles evaluating the same strategy through the same study design and with the same age group of children. None of the studies evaluated the use of present-day technologies (e.g., touch-screen input devices), which is an important contemporary clinical consideration. As such, although data from the studies identified by Tucci et al. are promising, the extant evidence does not provide for an adequate evidence base for literacy, specifically print knowledge, intervention with children who have a hearing loss.
Technology as a Tool for Early Literacy Intervention
Speech-language pathologists continue to implement new technologies that are useful for facilitating early literacy skills. Although there are a number of studies suggesting that computers with traditional mouse/keyboard interfaces can be useful in promoting early literacy skills in children with normal hearing (e.g., Levy, 2009; Shamir, 2009), to date, the evidence related to touch-based technology (e.g., electronic tablets, smartphones) is limited. Recently, Chai, Vail, and Ayres (2015) used iPads to teach print concepts to children with significant developmental delays, implementing a multiple-baseline design to evaluate treatment effectiveness. Inclusion criteria specified that the children could hear spoken instructions, but no evidence of having passed hearing screening was provided. One of the children was described as regularly wearing a hearing aid, but there was no information regarding the degree of hearing loss or verification of appropriate device programming and function.
During this intervention, Chai et al. used a custom-made iPad application to present tasks requiring the participants to match two words based on initial sounds (e.g., “Touch the word that begins with the same sound as ‘bee.’”). If a child selected the correct matching word, the application informed the children that the choice was accurate and presented the next word. After incorrect responses, the children were presented with a controlling prompt (e.g., “‘Bagel’ begins with the same sound as ‘bee’”) and a second opportunity. Although researchers were present during the intervention, it is unclear what role they played in familiarizing the children with the application. Regardless, all three participants responded favorably to the intervention, mastering the targeted sound–symbol relationships. However, to date, there is no research investigating the use of touch input technology as a tool to facilitate print knowledge in children with hearing loss (Tucci et al., 2014).
The role of adults during technology-based intervention is an important consideration. Children with disabilities benefit from skilled, individualized intervention. At this time, mobile applications do not provide adequate behavioral, attentional, and instructional supports for children with disabilities who are independently interacting with the application. Therefore, independent learning from mobile applications is likely not as effective as technology-based interventions supported by adult scaffolding. Northrop and Killeen (2013) suggested that in a school setting, teachers should first cover the content and explicitly teach children how to use an educational application. The student can then use the application with adult guidance, and the adult should check for the student’s understanding of how to use the app and its content. In addition, Neumann and Neumann (2014) found that children gain the most benefit from using high-quality apps that are based on pedagogical models and learning theories combined with scaffolding or guidance from an adult.
Although there is evidence for the use of interactive computer technology to teach literacy skills to children, there is a gap in the evidence base regarding children with CIs who are at a disadvantage when learning sound–letter correspondences. Furthermore, the burgeoning category of educational apps in Apple’s App Store is full of language and literacy training apps with little more to recommend them than a subjective collection of stars. Given these deficits in the literature, the purpose of this study was to investigate the effectiveness of an iPad application as a tool for intervention for preschoolers with normal hearing, as well as preschoolers with CIs, to improve their print knowledge and vocabulary skills, specifically through letter–sound correspondence. This multiple-baseline study provides a detailed description of how the preschool participants responded to clinician-directed intervention using tablet technology with a touch-screen. The following were the primary research questions of this exploratory study:
Method
Participants
Participants were recruited at a university speech-language and hearing clinic and included four preschool-aged girls, ranging from 3 years 11 months to 4 years 3 months. Two of the participants wore CIs and were receiving services related to their CI at a university clinic (CI-1 and CI-2). The two additional participants were peers with no hearing loss (NH-1 and NH-2) who had recently passed hearing screenings at 20 dB HL at octave frequencies from 500 to 8,000 Hz. CI-1, NH-1, and NH-2 were seen at their common day care and were provided the intervention by the same clinician who followed a specific script. The other participant with a CI-2 was seen in her home by another clinician who was trained by the first clinician, and also followed prepared scripts (Appendices A and B).
CI-1 was 4 years 0 months of age at study enrollment. Review of clinical records indicated an unremarkable pregnancy and delivery. She was diagnosed with profound sensorineural hearing loss (SNHL) at 1 year of age. The age of onset of hearing loss was unknown. Due to the severity of loss, CI-1 was implanted bilaterally with Advanced Bionics HiRes 90k HiFocus 1J internal devices sequentially at age 1 year 4 months (right) and 2 years 2 months (left). At the time of study enrollment, CI-1 was wearing Naida CI Q70 processors, bilaterally. Neptune processors were worn during periods of water exposure. Review of clinical records indicate that electrical dynamic range (i.e., mapping) was established from measurement of electrically evoked stapedial reflex threshold (ESRT) for comfort levels, and threshold levels were set at 15% of comfort levels. Electrodes 15 and 16 were deactivated in the right ear due to absent ESRT and no response to fricative sounds by the participant when these electrodes were activated. Clinical records indicated that CI-1 consistently used her device on each ear with data logging indicating average wear time of approximately 12 hr per day. Testing completed at an appointment with her CI audiologist during the study period indicated thresholds with her CIs between 10 and 20 dB HL across test frequencies of 500 to 6,000 Hz for each ear individually. Speech testing completed at this appointment, using Word Intelligibility by Picture Identification (WIPI) test (Ross & Lerman, 1970), revealed 67% correct with left CI and 75% correct with right CI. Scores for the bilateral condition were not available, as clinic notes indicated that the participant would not tolerate speech testing with both CIs. Additional information regarding CI-1’s vocabulary development may be seen in Table 1. According to parent report, she did not have experience with the application used in this study prior to participation.
Participant Hearing Status, Age, PPVT-4 Score, and Number of Letter–Sound Correspondences Known at the Beginning of the Study.
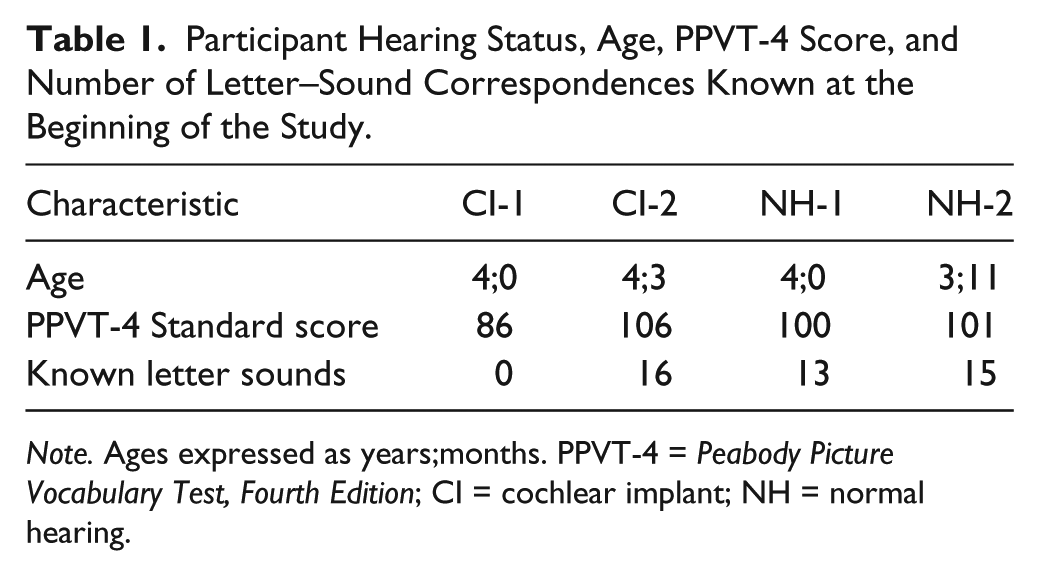
Note. Ages expressed as years;months. PPVT-4 = Peabody Picture Vocabulary Test, Fourth Edition; CI = cochlear implant; NH = normal hearing.
CI-2 was 4 years 3 months of age at study enrollment. Review of clinical records indicated an unremarkable pregnancy and delivery. She was diagnosed with a profound SNHL at age 1 year 3 months; age of onset of hearing loss was unknown. Clinical records indicate that CI-2 was implanted bilaterally with Cochlear Nucleus Freedom Contour Advance CI124 RE internal devices sequentially at age 1 year 4 months (left) and 1 year 6 months (right). CI-2 wore N5 CP810 processors bilaterally. Clinical records indicate that electrical dynamic range (i.e., mapping) was established from measurement of ESRT for comfort levels and behavioral thresholds via conditioned play audiometry for threshold levels. Furthermore, clinical records indicate that CI-2 consistently used her device on each ear; data logging was not available, but parent report indicated average wear time of 12 to 13 hr per day. Testing completed at an appointment with her CI audiologist during the study period indicated CI thresholds between 15 and 25 dB HL across test frequencies of 500 to 6,000 Hz for each ear individually. Speech testing completed at this same appointment using the WIPI revealed 90% correct with her right CI and 67% correct with her left CI; however, it was noted that poor attention may have contributed to lower scores in the left ear (it was tested after the right ear). Scores for the bilateral condition were not available, as clinic notes indicated that the child would not tolerate speech testing with both CIs. Review of chart notes indicate this was likely due to fatigue as bilateral speech testing was the last measure attempted during the appointment. Additional information regarding CI-2’s language performance may be seen in Table 1. Based on parent report, CI-2 did have prior knowledge and familiarity of the app used in this study before she was enrolled; however, she had not been actively using the app in the months leading up to this study. Furthermore, the parents reported they had not provided scaffolding when CI-2 had used the app in the past.
Two participants with typical hearing, NH-1 and NH-2, were enrolled in the study to allow for comparison with the participants with CIs. These two participants attended the same preschool and day care as CI-1. NH-1 was 4 years of age at the start of the study and was only 1 day older than CI-1. NH-2 was slightly younger, 3 years and 11 months at the onset of the study. Both of these children had recently passed a hearing screening conducted at a university clinic, and parents reported typical developmental histories. That is, no history of speech, language, physical, or cognitive delays. Additional information regarding language development for NH-1 and NH-2 is presented in Table 1. Investigators confirmed that neither child had prior experience with the application.
Technology
Technology used in the study included two Apple iPads (second generation) and the application “Endless Alphabet.” One Apple iPad was used for recording the intervention time with each participant, and the other iPad was equipped with the app. “Endless Alphabet” was created by Originator Inc (2013) and was the sole intervention under the clinician’s direction throughout the course of treatment. None of the authors were affiliated with this application, and it was chosen for this study due a hypothesized match between the participants’ early literacy skills and the skills targeted by the application.
“Endless Alphabet” is an application for iPad that is designed to improve children’s alphabet knowledge and vocabulary. A primary component is letter characters that produce their corresponding letter sound as the child is manipulating them on the iPad screen (See Figure 1). The letters spell a word, which is outlined on the display with the letters scattered around it. The child touches and drags an animated letter to its outlined shape, while the sound effect plays the letter’s phonetic sound. For example, in the word “Bellow,” the letters are spread around the screen, with the outline of the word in the middle of the screen. The child then touches and drags the letter, “w,” and while dragging, the letter is producing the letter sound, /w∧ w∧ w∧/. When the letters are in place to form a complete word, the application provides the word’s definition and plays an animated demonstration.
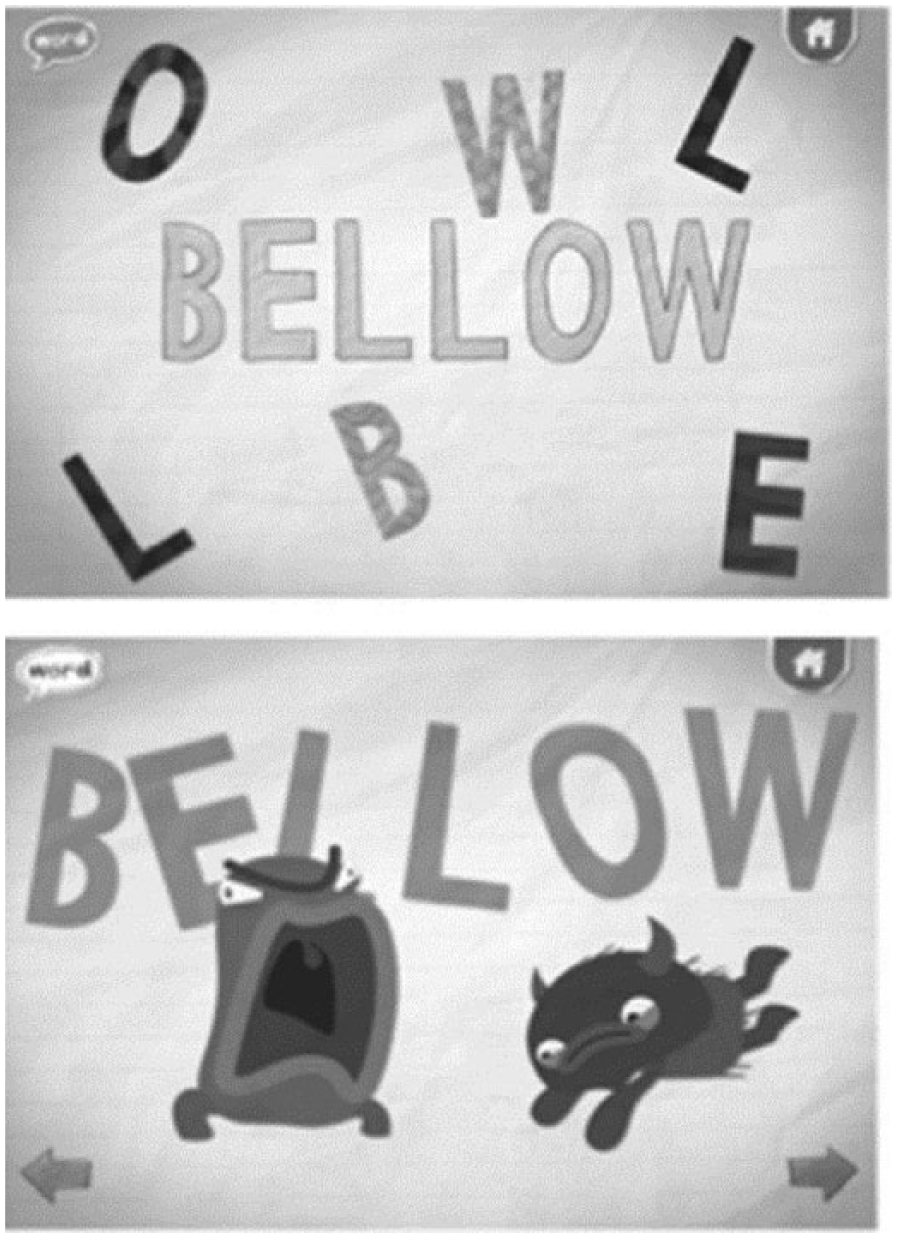
Screen shots of “Endless Alphabet” app.
Measures
Letter knowledge
Letter knowledge was first assessed by administering the grapheme subtest of the Phonological Awareness Test–2 (PAT-2; Robertson & Salter, 2007). This assessment was used to determine intervention targets (i.e., letter–sound correspondences) by identifying unknown letter sounds. As seen in Table 1, three of the children could identify between 13 and 16 letter sounds, but CI-1 did not know any letter–sound correspondences. During each subsequent session with the participants, the clinician assessed the participants’ knowledge of the targeted sounds prior to providing any intervention. Letter knowledge during this baseline-intervention phase was assessed by presenting the letters selected for intervention one at a time on flash cards to the participants and asking them to name the corresponding letter sounds. Each letter was presented in random order, and the clinician did not provide any feedback related to the accuracy of the children’s answers. Each letter was presented three times, meaning there were nine total opportunities during each session’s probe (i.e., three letters presented three times).
Vocabulary
The Peabody Picture Vocabulary Test, Fourth Edition (PPVT-4; Dunn & Dunn, 2007) was administered to determine a general estimate of each participant’s vocabulary development. Prior to intervention, we also measured the participants’ familiarity with the target vocabulary words, which was assessed by presenting the animations (without sound) of the selected words from the app, then giving the children three choices (see Table 2). None of the targeted sound–symbol relationships or vocabulary words were part of the preschool curriculum during the study period. These vocabulary words were then assessed using identical procedures once the intervention phase had been completed.
Pre- and Postassessment Procedures for Vocabulary Knowledge.
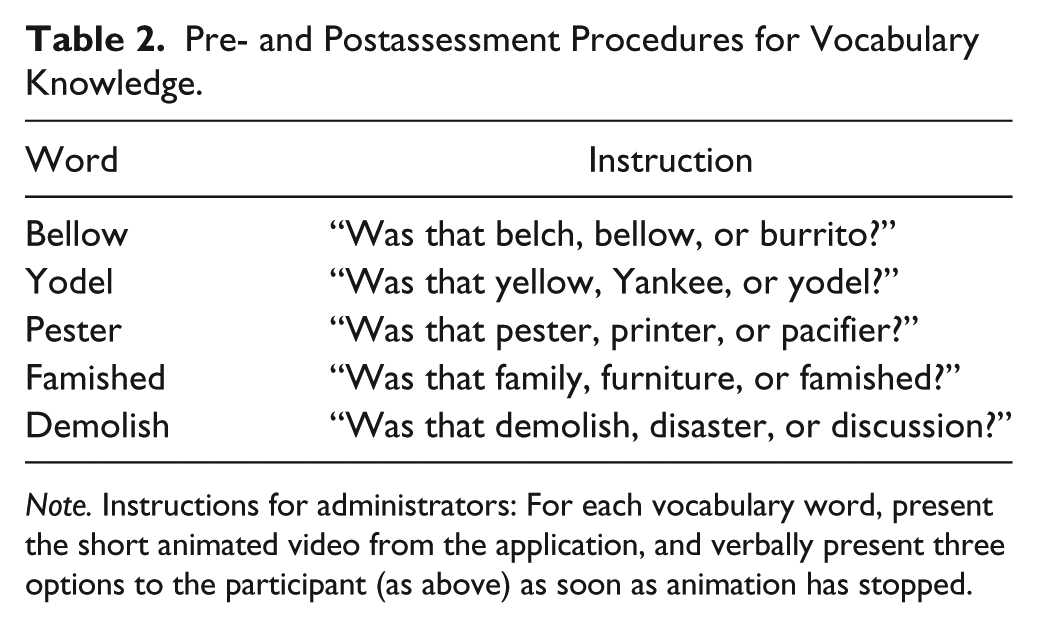
Note. Instructions for administrators: For each vocabulary word, present the short animated video from the application, and verbally present three options to the participant (as above) as soon as animation has stopped.
Intervention sessions
The participants were seen three times a week within a range of 3 to 5 weeks, and each individual treatment period was an average of 15 min. The length of the overall treatment period varied among the participants due to their differing rate of progression in mastering the targeted letter sounds. Each session began by moving to a quiet room at the child’s day care or house, and setting up one iPad to record the session. As described earlier, the clinician began by probing the child’s ability to name the sound corresponding to both treated and untreated letters. The clinicians then utilized “Endless Alphabet” to treat the participants’ vocabulary and letter knowledge. Each session included three different word scenes within “Endless Alphabet,” with each word containing the targeted letter for the session. For example, during a session targeting “w,” the “Endless Alphabet” words were belo
The clinician targeted the same letter sound across sessions until the child achieved the predetermined criterion level of accuracy for that letter, which was correct identification during two of three opportunities during each session’s preintervention probes. Once the child met the criterion, treatment was directed toward the next letter sound using three new words. In addition to these three words, one review word that contained the previously mastered letter sound(s) was included in the session to promote retention. This resulted in sessions that included three words, four words (one review and three new), or five words (two review and three new).
Originally, all children were to receive training for “w,” “y,” and “x.” These letters were chosen because they were unknown across all four children. However, “x” became the “letter of the week” for CI-1, NH-1, and NH-2 at their preschool within the timeline of the study. Therefore, “s” was the third letter for CI-1 and “u” was the third letter for NH-2. Because NH-1 enrolled in the study approximately 1 week before the other participants and progressed relatively quickly, she still received intervention for “x” before it received attention at preschool. CI-2 also received “x” intervention because she did not attend the same preschool and it was not in her preschool curriculum during the intervention period.
Validity and reliability
To strengthen and ensure validity, the first author monitored the letters being targeted at the preschool where the participants attended to prevent overlapping learning opportunities and exposure. The third author attended or watched the video of 90% of the treatment sessions, ensuring treatment integrity and interrater reliability of probe responses. Interrater reliability was 100%, which would be expected due to the nature of the probes (identification of letter sounds).
Results
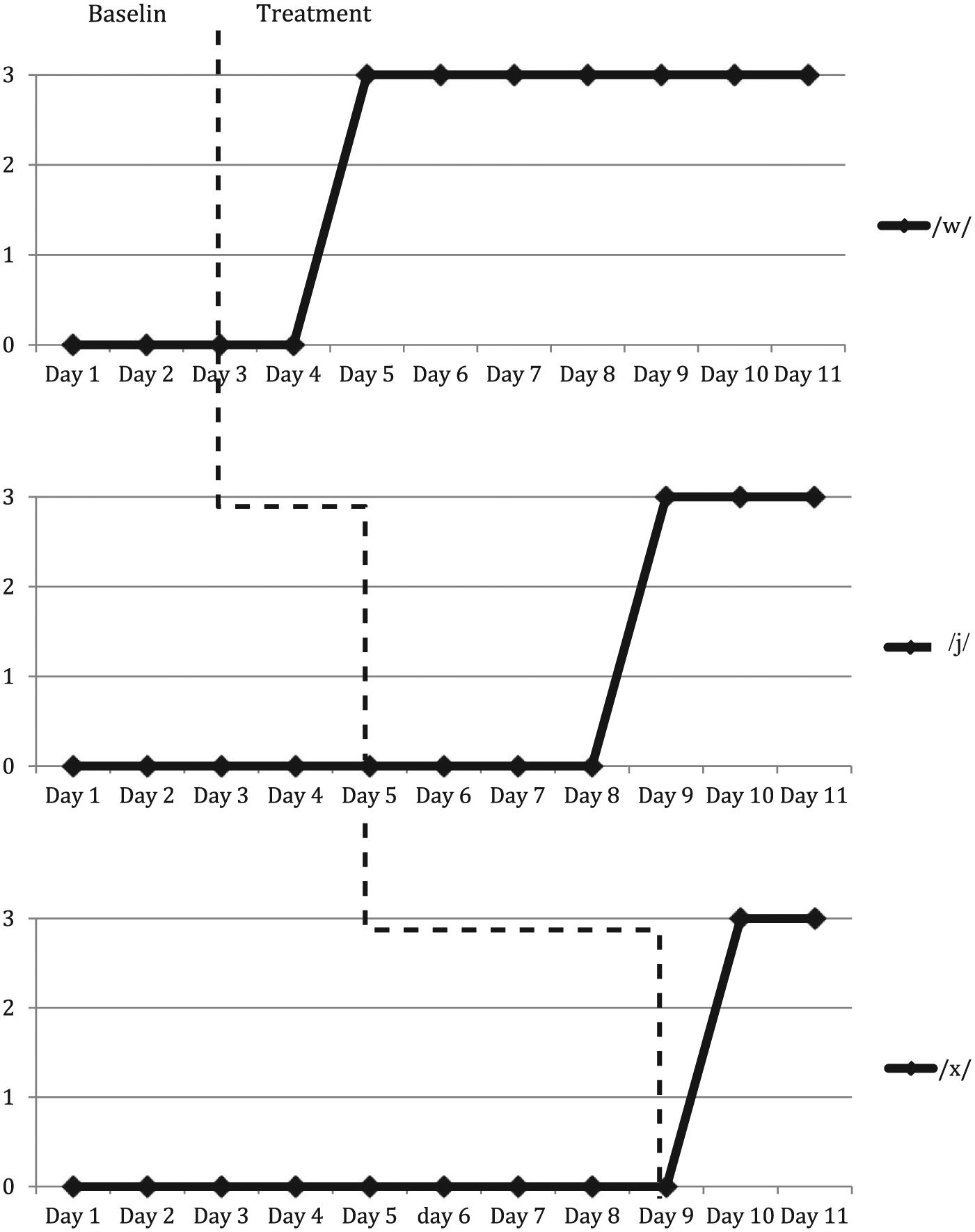
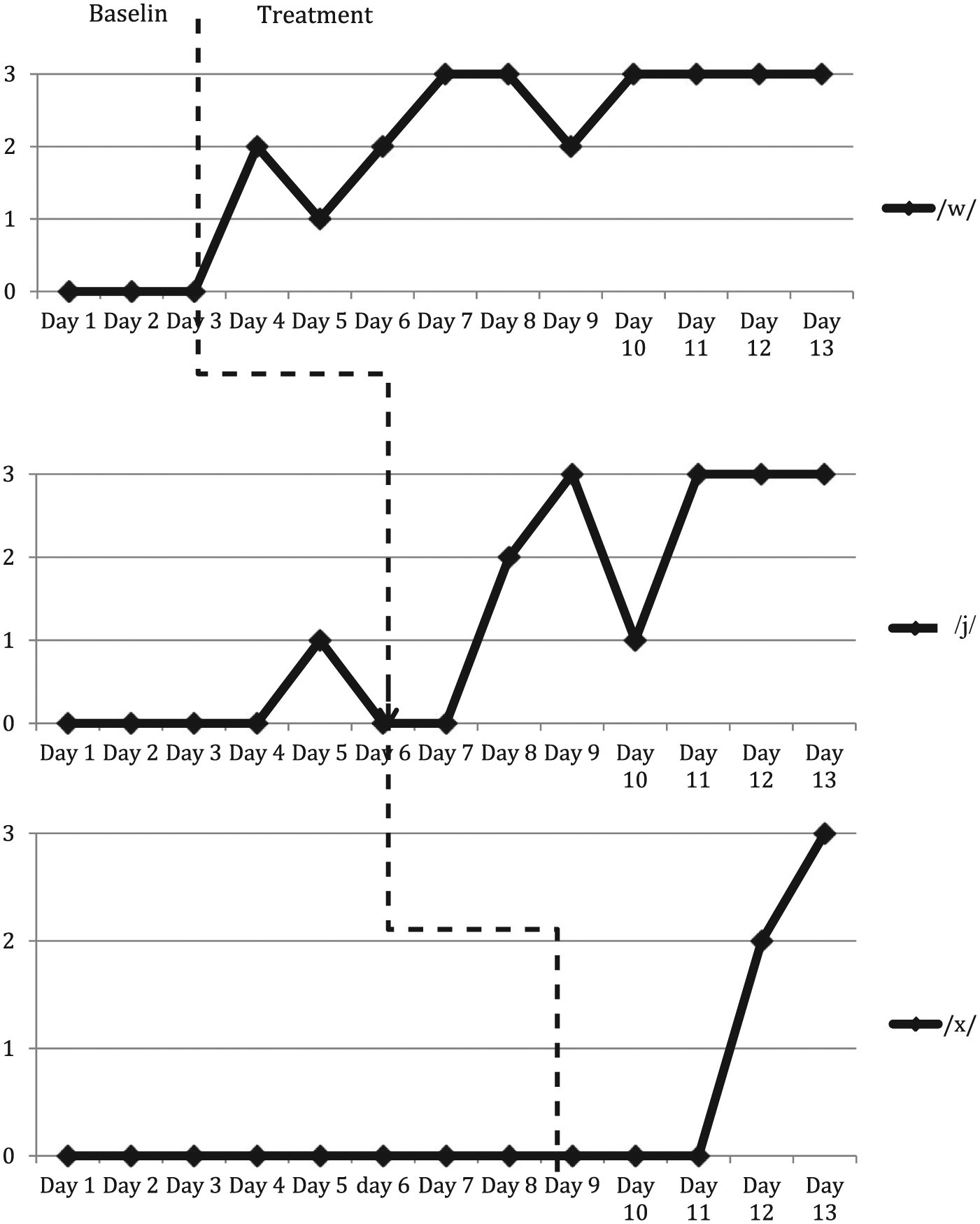
Results show that all participants demonstrated improvement in their knowledge of all targeted letter–sound relationships. All four participants started at 0% accuracy and reached 100% on each of their three targeted sounds, but at different rates (see Figures 2-5). CI-1, who wore CIs and had the lowest assessed vocabulary of the four participants, required the most sessions to reach this level of proficiency. CI-1 achieved 100% accuracy for “w” by Day 6. Treatment for “y” began on Day 5, but that target did not reach criterion (i.e., two of three probes) until Day 11. Following the progress for “y,” treatment on the third target, “s” started. Progress was faster for “s” with criterion reached on Day 13 (Figure 2). Interestingly, the other child with a CI and a higher vocabulary, CI-2 (Figure 3), demonstrated similar or better rate of skill acquisition than the two participants without a CI (NH-1 and NH-2; Figures 4 and 5, respectively), and typically reached the mastery criterion (two out of three opportunities correct) after two or three sessions with the target letter. All four participants scored 0% on the vocabulary pretest, but correctly identified all vocabulary posttest (100%), conducted on the last day of their intervention.
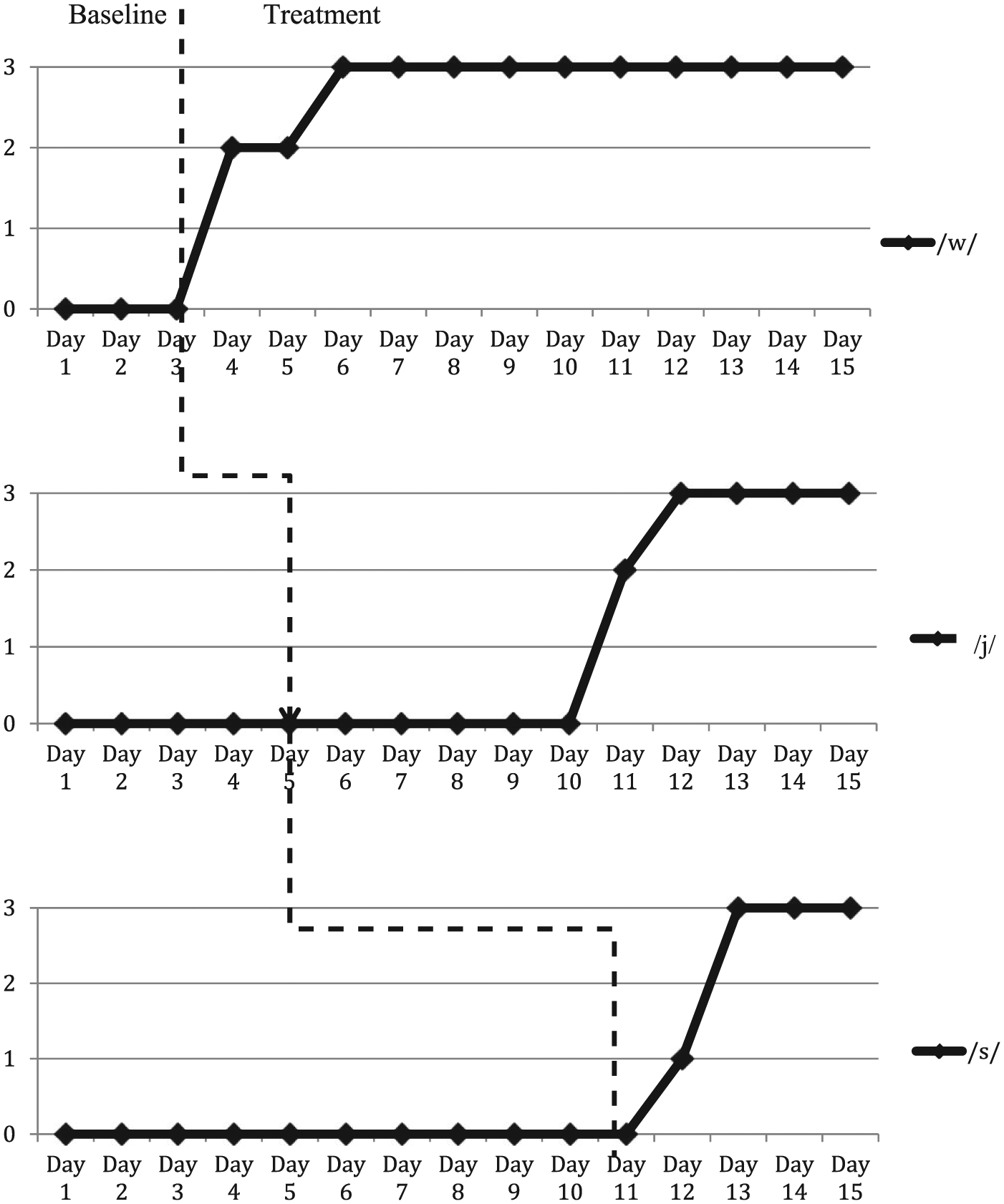
Results for participant with cochlear implant (CI-1).
Results for participant with cochlear implant (CI-2).
Results for participant with normal hearing (NH-1).
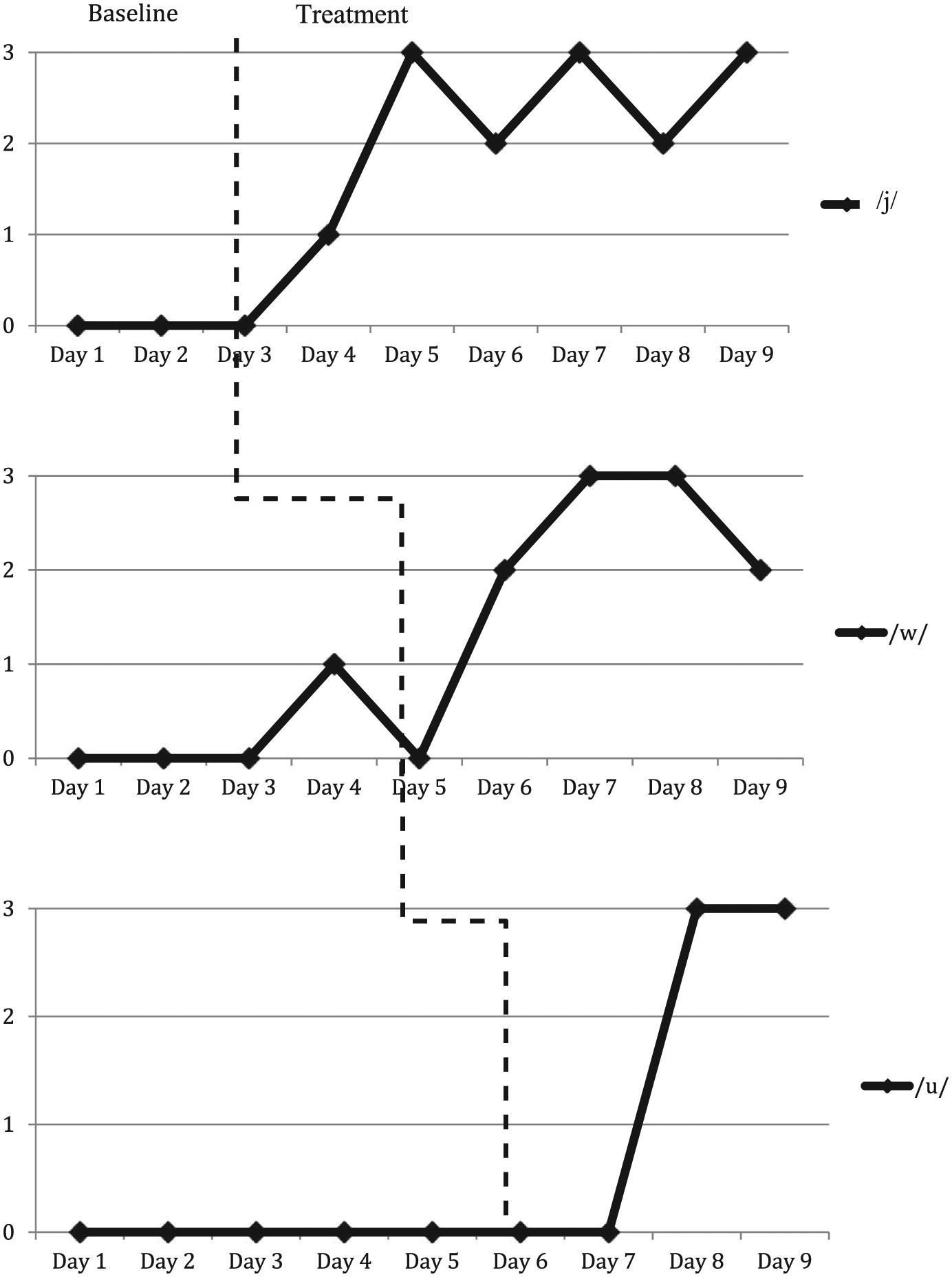
Results for participant with normal hearing (NH-2).
Discussion
Educational applications for tablet technology can provide structured activities that are engaging and motivating to help speech-language pathologists target language and literacy skills for young clients. However, to date, there is a need for more intervention studies to guide evidence-based practice, particularly for children with unique communication profiles. The current study contributes to this line of research by investigating the effectiveness of an iPad application, “Endless Alphabet,” for two preschool-aged children with CIs and two peers with normal hearing to improve their knowledge of sound–letter correspondence and vocabulary skills.
All four participants demonstrated relatively fast gains in their letter–sound knowledge when “Endless Alphabet” was used. Preschools often teach one new letter–sound combination for a week before introducing a new combination. By comparison, the study participants learned three new letter–sound targets in less than 4 hr (i.e., three, 15-min intervention sessions per week) using “Endless Alphabet” and clinician scaffolding.
The results of this study could reasonably suggest that prior letter knowledge and vocabulary development were more predictive than hearing status in these four participants. The participants with CIs exhibited letter–sound learning and vocabulary growth comparable with the two participants who had normal hearing, as each participant reached 100% accuracy for all vocabulary and print knowledge targets. CI-2 exhibited similar preintervention vocabulary and letter knowledge compared with the participants with normal hearing. These three children (CI-2, NH-1, and NH-2) learned the second target letter, “y,” more efficiently than CI-1, the participant with lowest PPVT and letter knowledge scores at the onset of the study.
However, CI-1’s progress is promising when the context of the study is considered. The intervention was provided in spring, toward the end of the participants’ preschool academic year. At that time, CI-1 could not correctly name any letter–sound correspondences, while the other three could identify more than half of the sounds in the English alphabet. However, CI-1 exhibited similar progress in letter–sound acquisition compared with the other participants during this study, requiring only a few more sessions to master the same number of letter sounds.
Tablet technologies are not a substitute for clinical expertise (Neumann & Neumann, 2014; Northrop & Killeen, 2013). Children benefit most when knowledgeable clinicians guide learning and skillfully integrate technology and learning activities with appropriate scaffolding and reinforcement. This principle was validated by CI-2 who had been exposed to the “Endless Alphabet” app, without guidance or scaffolding, prior to the start of this study yet did not differ from the others in alphabet knowledge at baseline.
Finally, educational apps, such as “Endless Alphabet,” have potential to be tools that promote carryover at home. Parents will be able to use this app by following an easy script as they work with their child. This would allow the child to practice the new letters at home and enhance letter–sound knowledge.
Limitations and Future Directions
This study included a child with a CI who had used the app without adult guidance prior to enrollment in the study, which provided additional insights into the role of skilled intervention combined with app use related to the dependent variable. However, this situation was serendipitous and did not allow us to document the duration of use, targeted letters, and baseline letter–sound knowledge without app exposure. A study investigating treated versus untreated letters would help disambiguate the interplay of educational apps and intervention techniques in participant learning. Another limitation of the current study is that the investigators were unable to treat the same three letters across all four participants. Although it would have been ideal to use the same letters across participants, reasonable conclusions can still be drawn due to the similarity of instruction provided for each letter.
Two different clinicians provided intervention to the children, which may have been a factor in the results. However, the researchers attempted to mitigate this effect by implementing a very specific set of intervention procedures, making a video recording of 100% of the intervention, and conducting treatment fidelity checks with great frequency. Future research could replicate these procedures to determine their effectiveness across a number of clinicians, which would further establish the external validity of the methods. The procedures outlined in this study could also be modified in subsequent studies to determine a methodology that is maximally effective and efficient. In addition, future research could compare clinician-scaffolded intervention with application-only experiences to evaluate the effect of a skilled adult during instructional application time.
Although the outcome of this multiple-baseline study is encouraging, the results should not be generalized to other educational apps. Each client has unique attributes regarding learning and communication needs, and what is motivating to one child may not engender the same response in another. The thoughtful clinician needs to design treatment accordingly.
With that caution in mind, the participants’ progress in sound–letter correspondence skills and vocabulary development during the short duration of this study is promising and warrants similar future similar investigations. Educational applications, in the hands of skilled and knowledgeable clinicians, may prove to be motivating and interesting contexts to provide evidence-based early literacy intervention for children with CIs and with NH.
Footnotes
Appendix A
Appendix B
Authors’ Note
This study was conducted in fulfillment of research requirements for a Leadership Excellence in Neurodevelopmental Disorders (LEND) traineeship.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.