
Abstract
Only 15% of children with hearing loss who could receive a cochlear implant receive one leaving American Sign Language (ASL) as their access to communication. Spanish-speaking families face even greater challenges including learning different languages/cultures and lack of trained Hispanic professionals. This study identifies how Hispanic mothers communicate with their children with hearing loss who use ASL as their primary language. Data for this qualitative study were collected using in-depth, open-ended ethnographic interviews and limited participant observations and analyzed using grounded theory. Results indicated that many mothers did not learn ASL or learned it some years after the diagnosis of hearing loss in their child; therefore, many children had no or limited language early on and were excluded from conversations and activities. Often mothers learned ASL in Spanish resulting in communication that varied in grammar. Language confusion can result in children’s lower overall language skills and poor academic achievement.
Keywords
Introduction
There has been a long-standing debate between the Deaf community and the hearing community on whether all children with hearing loss should learn American Sign Language (ASL; Mellon et al., 2015). For the great majority of children who are candidates for cochlear implants, parents are often advised against teaching the children ASL in lieu of concentrating exclusively on the development of speech through listening with the cochlear implants (Geers et al., 2017). However, for children with severe to profound hearing losses who are not candidates for implants for medical or physical reasons, who choose not to receive a cochlear implant, or who otherwise do not have access to audition and speech, ASL is the most viable option available for them to develop communication. Although ASL is now officially recognized as a complete and distinct language in the United States, the exact number of individuals in the United States who use ASL is unknown.
Children with hearing loss who use ASL and have hearing parents have been found to have poorer language outcomes than those who have deaf parents (Schick, de Villiers, de Villeirs, & Hoffmeister, 2007). Expressive vocabularies of typically hearing children improve with the more adult words they hear from their parents, especially in the child’s first 3 years of life (Hart & Risley, 1995; Hoff, 2003; Newman, Rowe, & Berstein Ratner, 2016; Weisleder & Fernald, 2013). Larger vocabularies often are associated with higher IQ and academic achievement scores (Hart & Risley, 1995). However, children with hearing loss miss this opportunity to learn from the richness (>1,251 words/hour) of their [hearing] parents’ language. If parents use ASL to communicate with their child with hearing loss, these children also can have the opportunity to improve their vocabularies through the richness of their parents’ ASL use. Thus, it is important to understand the way that children with hearing loss and their family members learn ASL.
A large majority of children with hearing loss have been observed to be born to two hearing parents but 71% of family members do not regularly use ASL in the home (Gallaudet Research Institute [GRI], 2011). The GRI’s most recent report states that only 15% of the children who could have a cochlear implant receive one. Thus, many children with severe to profound hearing loss have no access to audition, and subsequently speech, and require ASL for communication, a language that hearing parents usually do not have before their child’s hearing loss is diagnosed. Of children with hearing loss, 30% are Hispanic or Latino (GRI, 2011). Many Hispanic/Latino families in the United States speak primarily Spanish at home. When Hispanic/Latino children with hearing loss attend grade school, they learn English and ASL. Introduction of these two new languages to a primarily Spanish-speaking home may exacerbate any communication difficulties that exist between hearing, Spanish-speaking family members and their child with hearing loss.
Bilingualism in Children With Hearing Loss
There is very little research on bilingual children with hearing loss. Several studies indicate that children with hearing loss can learn more than one language (Kohnert, Yim, Nett, Kan, & Duran, 2005; Korkman et al., 2012; Ohashi et al., 2012; Restrepo & Kruth, 2000).
In a qualitative study, English-speaking parents described how difficult it was for them to communicate with their children with hearing loss who were learning ASL when they themselves did not use ASL (Freeman, Dieterich, & Rak, 2002). Parents expressed frustration and felt ill-prepared to communicate with their children. Parents also described their struggles and systemic barriers that included teachers and clinicians with little training in working with children with hearing loss. Bilingual parents who had limited English were further hampered in their access to resources available through the school and clinicians.
Families often need to develop a variety of strategies to communicate with their children with hearing loss, including learning ASL, writing notes to each other in a common language, or using an interpreter, among others. These strategies may be less accessible to Hispanic families in the United States who lack English proficiency.
Hearing parents of children with hearing loss face many challenges including language and culture, methods of amplification, school placement options, and selection of the best speech instruction methods (Quittner et al., 2010). In addition, everyday communication difficulties between children with hearing loss and their hearing parents can increase stress within the family (Freeman et al., 2002). Parental stress may be exacerbated by their reduced literacy, overprotection of their child, and their imposed limitations of their child’s participation in regular activities (Paul, 1998). Limited support networks, feelings of isolation, and stigmatization often are accompanied by depression, anxiety, and anger for hearing parents (Quittner, Glueckauf, & Jackson, 1990). These difficulties may be magnified for hearing parents with limited use of English and/or ASL when their children are fluent in English and/or ASL.
Erickson (1984) noted the unique challenges for Hispanic children with hearing loss, suggesting that both hearing loss and differences in cultural and linguistic characteristics must be considered in planning for these children. Akamatsu and Cole (2004) argued that if ASL was learned after the critical language period, it could be difficult for the child to acquire native-like fluency in ASL. Gerner de Garcia (2000) noted that Hispanic children with hearing loss who communicate in home sign or a native country sign language (NSL) may be seen as having no language in U.S. schools.
Florida is reflective of the nation in its distribution and characteristics of deaf and hard of hearing children and youth. Of Florida’s more than 1,570 deaf students, 72% were born to two hearing parents (2010–2011 Annual Survey of Deaf and Hard of Hearing Children and Youth). Florida’s deaf and hard of hearing students are 43% White (non-Hispanic), 27% Hispanic, 24% Black/African American, and 2% “other” or of multiethnic background. At home, 22% of Hispanic families with deaf or hard of hearing children speak Spanish and 3% use ASL. However, in the classroom, teachers use ASL and English language speech, with solely ASL for more than half of the time (2010–2011 Annual Survey of Deaf and Hard of Hearing Children and Youth). In addition, some children with hearing loss who have recently arrived in the United States may use a home sign or NSL rather than ASL (Gerner de Garcia, 2000).
Of Florida’s children population of children with hearing loss, 51% have severe to profound hearing loss, and only 11% of them had received a cochlear implant (2010–2011 Annual Survey of Deaf and Hard of Hearing Children and Youth). Thus, 89% of Florida children with severe to profound hearing loss are unable to use speech for communication, which may pose problems for home and classroom language use. These problems likely are greater for children from Spanish-speaking homes who are learning English in school.
Takala, Kuusela, and Takala (2000), in their 5-year longitudinal ASL intervention project with 81 deaf preschool children in hearing families, found that while the children’s competence in ASL improved, their parents’ ASL skills did not improve significantly. However, families reported that family communication became easier and that they expanded their network of families in similar situations. However, families who do not become fluent in ASL may be further increasing their communication problems with their deaf children. In addition, as most children with severe or profound hearing loss are in special education, the limited number of Spanish-speaking professionals who work in special education may also complicate the situation.
In summary, there is little information on bilingual (especially Spanish-speaking) families’ concerns when a child has a hearing loss. When a child with hearing loss is born to a hearing, Spanish-speaking family in the United States, culture and language issues arise that neither the family nor the Deaf community can easily navigate. These issues have not been addressed in the literature. The limited communication with the child with hearing loss can create conflicts that alienate them from their families, their peer group, and those in the Deaf community. While there are studies on children with hearing loss, studies on communication between Spanish-speaking hearing mothers and their children with hearing loss are lacking. The purpose of this qualitative research was to investigate how Hispanic Spanish-speaking and hearing mothers communicate with their children with hearing loss who use ASL in English as their primary language.
Materials and Methods
Data analyses in the current article address the first research question in the investigator’s larger study (Alfano, 2007). Data were collected using in-depth, semistructured interviews and limited participant observations. With each interview and observation, field notes were generated. Data were analyzed using grounded theory to determine “how the discovery of theory from data—systematically obtained and analyzed in social research—can be furthered” (Glaser & Strauss, 1967, p. 1). Glaser and Strauss (1967) suggest using a general method of comparative analysis, whose purpose is joint coding and analysis to systematically generate theory. Using the constant comparative method, researchers compare incidents applicable to each category, integrate categories and their properties, delimit the emerging theory, and finally write the theory.
Procedure
Following institutional review board (IRB) approval from the University of Miami, study mothers were recruited from community agencies, referrals from other study participants, and through members of the Deaf community in the South Florida area. Inclusion criteria were as follows: Hispanic Spanish-speaking, typically hearing mothers living in the southeastern United States speaking little or no English and their children (5 to 13 years old) with severe to profound hearing loss who used ASL in English as their primary method of communication. Exclusion criteria were as follows: Hispanic mothers with proficient English, and children who had other disabilities, had received a cochlear implant, or used a language other than ASL as their primary method of communication. Mothers’ proficiency in ASL was not a criterion for inclusion to allow wide diversity in this concept because the main focus of the research was to determine how Spanish-speaking mothers were able to communicate with their children with hearing loss, including ASL. Fluency levels for all languages were obtained through self-report and corroborated through observation by the principal investigator (PI).
In Spanish, the PI explained the study to potential mother participants, answered their questions, and obtained informed consent. Mothers agreed to in-home observational visits and audio-recorded interviews at a time that was convenient for them. All mothers requested the interviews be conducted in Spanish. All eligible mothers and children who were contacted agreed to participate and all completed the study.
Data Collection
Using ethnographic data collection methods, the study’s first step involved observations of mothers in their homes communicating with their children with hearing loss. The study PI is fluent in English, Spanish, and ASL, and was able to understand all interactions that took place in those languages. Two children used an NSL and the mothers interpreted for the PI. The sessions generated field notes regarding observed interactions. The PI audio-recorded her impressions upon leaving the home to document fine details that could not be written during the observations. The purpose of the observations was to describe the setting, activities, people in the setting, and the interactions of those in the setting and to check for what was reported during interviews.
The next step in data collection was to interview mothers and their children with hearing loss on the same day after the observations. Each mother and each child was interviewed one time, following the observation. The PI conducted audio-recorded, semistructured interviews in Spanish with the mothers and then in oral English with the children. If the child used ASL, an interpreter was used to capture the child’s responses on the audio recordings. Mother and child interviews were conducted independently of each other. The mothers and their children were allowed in the same room during the interviews and some of the mothers listened to their children’s interviews. None of the children chose to stay for their mothers’ interviews, likely due to the fact that they were conducted in Spanish and the children could neither hear nor understand Spanish.
The mothers’ interview guide was developed based on a literature review and the results of the PI’s earlier pilot study with two mothers, including one observation and two interviews. Data from that pilot study were not included in the larger study. Guiding questions developed for the larger study were open-ended, allowing the mothers to set the tone and to discuss what was most important to them. These questions assisted in the organization of the interview; however, the interview followed the mother’s lead. Prompts were used when more information was needed to keep the conversation moving in a particular direction and to focus the conversation when it began to stray.
For the child interviews, the same strategies were used (e.g., open-ended questions, following the child’s lead, etc.), using ASL and oral English for those children who had sufficient speech skills. For those who had limited speech skills, an ASL interpreter signed the questions and voiced the children’s responses. This was done to have a voice representation on audio recordings and to ensure the PI fully understood the children’s responses. When interviewing the children, the session began by playing an age-appropriate game or by chatting with them about their interests so they could get comfortable with the PI and the interpreter’s presence. When the child began to communicate freely, the interview began.
The guiding questions included timing and setting questions which allowed the informant to describe a particular location and time period (e.g., “Describe for me a typical dinner time.”), example questions which asked for more detailed information regarding something the informant had shared (e.g., “Who might be sitting at the dinner table with you?”), experience questions which asked informants to describe their experience in specific settings (e.g., “When you are signing, what language are you thinking in?”), and native-language questions to learn how the informant’s language was used (e.g., “What methods of communication do you use with your child?”). Follow-up questions and prompts were asked where appropriate. After the mother interviews were completed, demographic information was collected.
A final step (a member check) was completed via an additional visit to four of the homes to (a) observe some aspect of communication identified during the interview but not observed on the first visit; (b) clarify the mothers’ and children’s intended meanings during the past interviews; (c) discuss opinions of emerging themes; (d) and ask any follow-up questions. Mothers were allowed to ask any questions or make clarifications they felt necessary to clearly document the aspects of their lives that were important for them to share. These additional visits occurred within 1 to 2 weeks following their initial observation and interview.
Criteria Quality
In qualitative research, the establishment of trustworthiness in a naturalistic paradigm (Lincoln & Guba, 1985) parallels the criteria in quantitative analyses. However, as Lincoln and Guba explain, the differences are that “qualitative research is conducted not to confirm or disconfirm earlier findings, but rather to contribute to a process of continuous revision and enrichment of understanding of the experience or form of action under study” (p. 278). They state that their guidelines are characterized by the general customs of publishability for qualitative research. For example, internal validity is answered through the establishment of credibility which is supported by detailed descriptions, quotations, and a logical design. Credibility is the qualitative research method’s greatest strength, due to the large volume of data produced. These data can then be reviewed, if necessary, to confirm emerging analyses. However, qualitative research seeks specific participants to gain insight. Making generalizations is not the purpose of qualitative research. In qualitative research, dependability is sought through ascertaining that the findings in the study are supported by the data. Finally, the objective nature of the data is evidenced by a confirmable audit trail.
Data Analysis
Each observation was written as detailed field notes for analysis and coding. Each interview was audio recorded, transcribed verbatim in Spanish, and then translated into English to be analyzed and coded in the same manner as the observations. Using open coding, specifics within the data were compared to identify properties of the concepts and relationships among the concepts. Sections of the data were separated into discrete incidents and labeled. The open codes were then placed into subcategories. The data were then organized into levels including open codes, conceptual categories, and theme developments. This procedure allowed themes to emerge.
Results
Sample
The 11 participating mothers and one grandmother represented eight Latin American countries: Nicaragua, Uruguay, Cuba, Santo Domingo, Puerto Rico, El Salvador, Guatemala, and Colombia. The 11 children ranged in age from 5 to 13 years and grade in school from kindergarten to fifth grade; three children had repeated at least one grade. More than half of the children (66.6%) were male. Sixty-six percent of the mothers had more than a high school education. Only two children had been diagnosed with hearing loss by one year of age. All mothers spoke Spanish as their primary language, but several spoke to their children in a mix of English and Spanish. Mothers and children had ASL skills ranging from none to fluent, and English proficiency from none to some fluency (see Table 1).
Demographics.
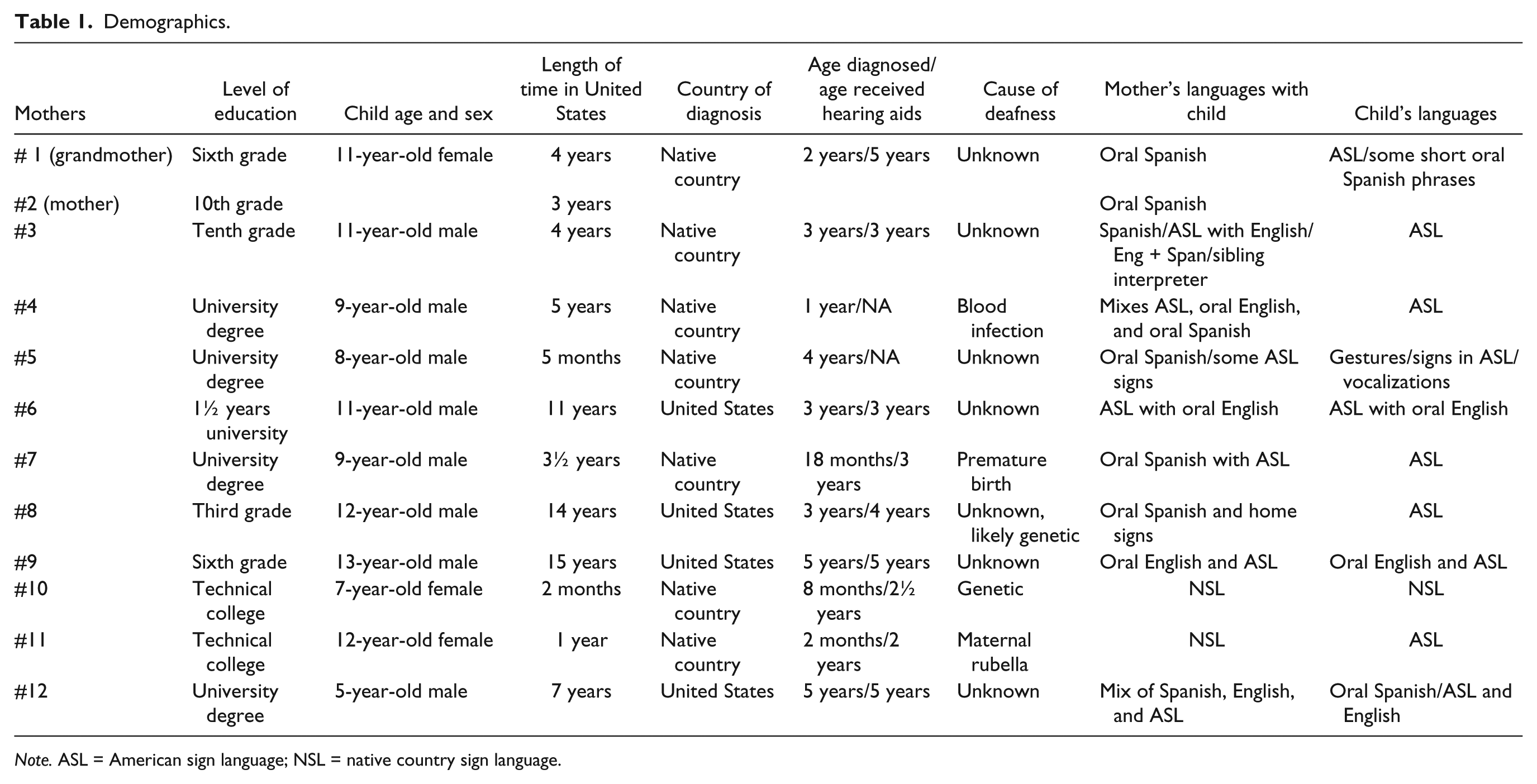
Note. ASL = American sign language; NSL = native country sign language.
Thematic Analysis
Data were analyzed from the 12 mother/grandmother interviews, 12 child interviews, and 12 observations into codes, then grouped into conceptual categories, and then further analyzed. Two themes emerged: (a) Communicating in the Family and (b) Learning Language.
These two themes provide detailed descriptions of the phenomenon of child deafness in family communication and language learning. In each of the homes, due to the child’s deafness, family communication was altered in ways that often required learning a new language for family members. For example, the language that some mothers used with their children was a mixture of several languages, as when they spoke oral Spanish while using signs from ASL. Development of language patterns and conversational topics was limited, and there was a mismatch between parents’ and children’s communication strategies. In some cases, misunderstandings occurred among family members. These communication issues had implications for children’s overall relationships with their families as well as for their success in school. The mixture of languages in the home, combined with the age of learning a language for the children and the language taught in the schools, is often associated with language confusion for the child as they are not accessing complete languages as models. This language confusion can result in lower language skills and, subsequently, poor academic achievement, as the relationship between language and academic skills has been well-established (Dockrell, Lindsay, & Palikara, 2011; Hohm, Jennen-Steinmetz, Schmidt, & Laucht, 2007).
Communicating in the Family
Language usage
The mothers reported that their main challenges were finding a new way to communicate with their child with hearing loss. Challenges included frequent communication breakdowns, mothers’ perceptions of their communication with their deaf children, the depth and breadth of topics they could communicate, and the types of communication strategies that they developed and used.
Three mothers’ comments represented differing levels of language use and perception. One had become involved with the Deaf community and learned NSL to such an extent that Deaf people considered her to be a native NSL user. This mother used NSL in her home so naturally with their two deaf daughters that she often signed to her hearing husband instead of speaking without realizing it. In sharp contrast, another mother, who also had two deaf children, stated that she knew nothing of signs and had virtually no communication with her children. A third mother stated that her communication with her daughter was very good, despite the obvious frequent communication breakdowns and frustration demonstrated by the child during their conversations.
Communication breakdown
Many families found it very difficult to communicate with their deaf children and either had limited communication with them or found other ways to bridge the gap. When asked in ASL if one child understood her mother, she replied that she didn’t always know what her mother was saying and that her mother often didn’t know what she was trying to sign. Several times during their joint communication, the child signed, “I don’t know,” but her mother didn’t redirect or try another way to show her. In this case, the child was having difficulty understanding her mother but the mother was not aware of the breakdowns. Indeed, this mother said that the communication was good between herself and her daughter.
In some homes, communication between the deaf child and the mother was minimal. In one home, there was very little communication between the mother and her child with hearing loss; however, the mother had very fluent communication in Spanish with her young hearing son. The child with hearing loss sat passively and let things happen to her. When the PI signed with the child, the conversation was much more in-depth and lively.
Perception of communication
Mothers had varied opinions about their communication with their deaf children. A few mothers felt satisfied with their communication. Several mothers felt that their current communication was good, but were worried about their future communication with their deaf child. One mother felt that her current communication with her son was adequate; however, she felt that she would need to improve her communication with him as he continued to grow. Another mother felt that her son was starting to leave the family behind in communication as his ASL improved. She described getting a dictionary and books to improve her ASL use.
Conversational topics
Even though many mothers felt that they had good communication with their children, the topics that they could discuss with their children were limited. Few mothers were able to discuss abstract or deep topics with their children that included sexual, religious, and political topics and they expressed their concern about these issues.
Communication strategies
Family members developed a wide range of strategies for communicating. Generally, the method of communication preferred by the child with hearing loss differed from their family’s methods of communication. Signed languages have grammatical rules that differ from those of oral languages. Therefore, if a person was using signs and speaking at the same time, the grammatical structure would be that of the oral language and not the signed language. In addition, some families made up their own home sign languages that Lane, Hoffmeister, and Bahan (1996) state “become idiosyncratic to the families and the child” (p. 39). Lane and colleagues posited that the use of home sign could range from a simple use of gesture, pointing, and charades to a more complex combination of signs specific to the home that could relay much more information.
Children used ASL in nearly all their communications with their families. However, many of them used shorter ASL phrases, as their families did not understand longer and faster sign phrases. Only two children used NSL with their families, also mixed with ASL. The children also used oral Spanish and English almost equally to communicate with their mothers, and often in combination with ASL and NSL signs. Children with hearing loss often used lip-reading to understand their mothers and gestures, home signs, and an interpreter (e.g., a sibling) to make themselves clearer to their mothers.
In contrast to their children, mothers generally used oral Spanish most often to communicate with their child with hearing loss. Many mothers used some ASL signs, but often in combination with oral Spanish, using the Spanish grammatical order rather than the ASL or English grammatical order. For example, if the sentence “I see the big dog” was signed, it would look like “Dog big I see” in ASL. However, if spoken in Spanish, the adjective and object would change positions, as in “Yo veo el perro grande” (“I see the dog big.”). English and Spanish grammar would not be the same as the ASL grammar. In addition, mothers used oral English, gestures, a family interpreter (e.g., a sibling), and NSL, but all to a lesser degree. Often several strategies were used at the same time. For example, one mother would speak to her son in oral Spanish and then insert a word in English and ASL. Therefore, a typical sentence she produced could be, “Donde esta el cat (while signing cat)” [which translates to “Where is the cat?”]. Only one family used NSL naturally. While they communicated, they used NSL in grammatical order and did not speak orally. A small number of mothers were observed using a home sign with their children.
Overall, family units used a family interpreter, most often a sibling who used ASL, to communicate with their child with hearing loss if the family members did not understand the child’s ASL. In addition, in the homes where family members had learned NSL, they tended to continue to use their NSL in combination with oral Spanish even though their children were responding to them in ASL.
Learning Language
Issues in learning languages
Parents’ difficulty in learning a new language to facilitate communication with their child with hearing loss was exacerbated by the families’ lack of knowledge of deaf issues or signed languages and the absence of support systems to assist them in learning another language.
Mothers were faced with the challenge of learning a new language to communicate with their children. The challenges surrounding this task included identifying what languages were important to learn or maintain; understanding that there were differences between their native oral and signed languages and the oral and ASL used in the United States; actually learning the new language; using language learning facilitators to ease the process; and overcoming barriers in learning a new language.
The importance of language
For some mothers, it was important that their children continued to learn Spanish or not lose their current skills. One mother stated that it was beneficial for him in his community, while another said her child needed Spanish to be able to communicate with his extended family.
Many mothers felt that it was important for them to learn ASL as their children were using it. Even though mothers had come to the realization that they needed to learn ASL, most did not learn ASL until the children were much older. Therefore, they had no real way to communicate with their children during the early years. Only one mother was fluent in her NSL and used it with native-like proficiency with her daughters. She explained that she wanted her children to keep both ASL, now that they were learning it in the United States, and NSL, as all her family in her native country had learned NSL to be able to communicate with the girls.
Language variety: ASL/NSL/Spanish/English?
The question of which language to focus on presented a challenge for the families. Several families had the opportunity to learn their native countries’ ASL and felt that they had good communication with their children. However, once they moved to the United States, many were very frustrated to find that the sign language they had learned was not a universal language and that sign languages differed from country to country.
One mother explained that she thought that ASL in the United States would be the same but was very disappointed when she found out that it was different from her NSL and now was trying to learn ASL. Her entire family had learned NSL, but in their 3 years in the United States, only his sister learned enough ASL to communicate with her brother with hearing loss. Another issue was whether ASL instruction would be given in English or Spanish, as most mothers didn’t speak or understand English.
Language learning: From whom and when?
Many issues were involved in determining how and when the mothers and children learned ASL. Few children learned ASL from their families. Only two children in the study had learned signs from their parents and the remainder learned ASL at school. Learning ASL at school meant these children spent their first few years with virtually no communication in the home. In addition, those children who had not learned ASL in the home were demonstrating lower language skills likely due to their lack of early experience with language. Parents and children who learned ASL or NSL early were much stronger in their ASL skills.
For the mothers who did learn ASL, they learned either through their children or by taking classes. The overwhelming majority of mothers had learned ASL from their children or along with them while only two were teaching ASL to their children. In addition, although most mothers said that they knew that they needed to learn ASL when their children were diagnosed, many of them did not learn ASL until their children went to school and the children taught it to their families at home. One mother explained that she had learned ASL by having her daughter physically move her hands for her to shape the signs. One child described how she communicated with her mother and it was clear that she didn’t feel very competent in any of the languages that her mother reported using.
Language learning facilitators
Learning a new language was typically a difficult thing for the mothers to do. However, some facilitators were identified that allowed them to learn more easily. Mothers learned through their children; many of them reported that their children would manipulate their mother’s hands to make the correct signs and would correct them when they made an incorrect sign. In addition, some mothers had taken classes or used books and videos to learn ASL or NSL. One common facilitator for mothers to learn ASL was to have the ASL vocabulary they were learning translated into Spanish. In addition, the use of a Deaf mentor in the home was cited as a facilitator for learning ASL. Although most of the mothers did not participate in any Deaf cultural events, those who did participate stated that signing with others helped them learn ASL. Several mothers who had learned NSL in their native countries stated that their learning of NSL was obligatory at their children’s school and was offered as a free service. In addition, they said that NSL taught in Spanish was much easier for them to learn.
Language learning barriers
Many mothers reported that learning ASL was very difficult for them because ASL is based on American English and generally taught in English. For some mothers the time needed to learn another language was too great, while for others, ASL being taught in English meant they could not understand. Still others reported that their children signed too fast for them to understand. Another barrier was a lack of ASL classes in their area. Several mothers also stated that their work schedules, child care problems, or lack of transportation hindered their participation in an ASL class.
It appeared that most mothers had the same barriers to language learning. Nine of the 12 mothers/grandmother had full-time jobs outside the home and one mother was searching for a job. Half of the mothers did not own a car, and seven spoke little or no English. Some mothers allowed the barriers to keep them from learning while others found ways around the barriers, not allowing them to be hindered from the process.
Consequences of Late Language Learning
Several consequences emerged for the children who were learning language at a later age. Many children had difficulty communicating, participated in conversations that had frequent communication breakdowns, and had behavioral issues.
Academic history
Many of the children in the study were currently or had already repeated one or more grades. In addition, some of the children did not receive formal schooling until the children were older.
Communication breakdown
Some of the children were not able to answer questions during their interview. They had difficulty understanding the questions posed to them, often commented off-topic, and had difficulty formulating their thoughts. One child who used ASL to communicate with his parents would ask his parents, “What is she saying?” when the interpreter or PI would address him in ASL. It was unclear if he truly didn’t understand what was being said or if perhaps he was not comfortable with new people’s signing and automatically was asking his mother to translate for him.
Behavioral issues
Several mothers indicated that their children had frustration and behavioral issues related to not being understood. However, many mothers reported that the behavioral issues subsided once they could communicate. One mother stated, “When he started school, he had many problems. He would say something and we didn’t understand him and he would hit the walls and the refrigerator, because he was upset with his lack of communication.”
Discussion
The purpose of this study was to investigate how Hispanic Spanish-speaking and hearing mothers communicate with their children with hearing loss who use ASL in English as their primary language.
Twelve mothers (including one grandmother) and 11 children participated in this study. Most shared similar experiences and concerns. However, a few mothers were able to communicate well with their children with hearing loss despite the difficulties. Nine of the 12 mothers worked outside the home and one was looking for work. Some working mothers were able to find time in their schedules to learn to communicate with their children.
The themes that developed characterize the nature of the communication between Hispanic Spanish-speaking mothers and their children with hearing loss who use ASL. Mothers’ initial difficulty learning to communicate with their children led to limited mother–child interactions. This finding has further implications for how these children relate to their mothers and participate in activities with them. The mixture of languages used in the home combined with the children’s age of learning a language and the language being taught in the schools may lead to language confusion in the child with hearing loss, and perhaps, lower language skills and poorer academic achievement.
Implications of Limited Family–Child Communication
Many mothers stated that they felt it was important for them to learn ASL; however, most did not learn more than a basic level and the difficulty communicating with their children limited mother–child interaction. This is consistent with findings from Takala et al.’s (2000) longitudinal study where ASL was taught to deaf preschool children and their families concurrently. At the end of the 5-year study, the children had improved their ASL skills, but their parents had not significantly improved. The same was observed with the families in this study. Most of the parents were learning ASL through their children, who continued to improve their skills.
The experiences of the families in the present study demonstrate limited communication based on concrete messages. Lane et al. (1996) felt that even in the homes where home sign was more developed, there would still be “frustrated attempts to communicate even simple ideas” (p. 40). Many mothers in this study expressed their concern regarding being able to communicate with their children about abstract and sensitive topics. Few mothers, if any, expressed concerns about implications for their future relationships with their children. In addition, many of the mothers who did sign did not use it at the dinner table unless they were specifically communicating with their child with hearing loss. By leaving their child with hearing loss out of the family dinner conversations and limiting their ability to participate, they were decreasing their child’s opportunities to learn incidental language and family matters. This might be why children with hearing loss don’t pick up incidental language, because it is inaccessible to them, which may contribute to behavioral problems.
Unfortunately, most of the children in this study learned ASL after the critical language period and very few learned NSL during that time. For those children that had learned NSL along with their parents, living in the United States with no language support meant that NSL had faded out of the children’s repertoire while ASL increased, although the parents still held onto NSL. Many of these children faced a home of mixed languages. For example, one child might lip-read his or her father’s oral Spanish, then watch his or her mother use ASL signs while speaking in Spanish, altering the ASL into Spanish grammatical order. This same child could then have a sibling who used ASL signs while speaking English, altering the ASL into English grammatical order, and all the while learning to read in English and use ASL at school. This lack of consistency in language use could easily lead to language confusion and reduced language skill, as was often seen in the children in this study.
Recommendations for Practice
This study’s findings identified many of the concerns and issues that need to be targeted to improve the communication in homes of Hispanic Spanish-speaking families with children with hearing loss. Suggestions for improving the communication between children with hearing loss and their families include parent workshops to highlight general communication tips that include having the child participate in language, involving the whole family, assuring that children do not miss what is happening in their surroundings, and including children in all family activities and conversations. Family get-togethers with other families from all areas of the city that would include support group meetings for parents in Spanish, child care for younger siblings, and joint activities for deaf and hearing siblings would be very helpful. Meetings could include people from the Deaf community, both Hispanic and non-Hispanic, so that families could see how Deaf adults participate in the community and offer other adults with whom the parents could practice their ASL skills.
ASL and Deaf culture taught in Spanish in the home including parents, siblings, extended family members, caregivers, and all other members of the household would be beneficial. In addition to the home learning, class meetings with other families in the same area every few weeks could be helpful in promoting social contacts and networks. Transportation could be provided for those in need by families that have transportation. Game playing activities could be used to promote ASL learning and practice. This type of natural language use could be powerful, as well as facilitate family–child interactions.
Future Investigations
Future research is needed to investigate siblings’ experiences with deaf brothers or sisters; experiences of middle/high school deaf students and young adults; comparison of experiences of Hispanic Spanish-speaking families with non-Hispanic families with children with hearing loss; longitudinal research measuring language skills of children with hearing loss to identify language dominance and to determine differences in language performance by age of diagnosis, age of language learning, mode of language used, parental language skills, and parents’ education levels.
Study Limitations
All mothers and children in this study were Hispanic. More than half of the children (66.6%) were male. Sixty-six percent of the mothers had more than a high school education. Only two children had been diagnosed with hearing loss by one year of age. Study findings may not hold in non-Hispanic mothers whose primary language is also not English, who are less educated, or in older children, or those groups that have more female representation.
Conclusion
There are numerous difficulties to consider when working with Hispanic Spanish-speaking families who have children with hearing loss who use ASL. Knowing that children with greater vocabularies have higher IQs and academic achievement makes it imperative to support and facilitate family communication. As only 15% of the children eligible for a cochlear implant receive one, there are many children with hearing loss who require ASL for communication. ASL is a language that hearing parents usually do not have knowledge of before a child with hearing loss is diagnosed. This is exemplified in the 71% of family members who do not regularly use ASL in the home, effectively making it impossible to communicate with their children with hearing loss. In addition, many of the mothers who did use ASL did not use it at the dinner table unless they were specifically communicating with their child with hearing loss. This practice left their child with hearing loss out of the family dinner conversations, limiting their ability to participate. By doing this, the child’s opportunity to learn incidental language and family matters were kept at a minimum. When taking all of this into consideration, much work needs to be done to increase home communication in Hispanic Spanish-speaking families with children with hearing loss using ASL.
The findings from this study present a picture of tremendous challenges for Hispanic Spanish-speaking hearing mothers of children with hearing loss. These challenges often resulted in limited mother–child communication, language mismatches, and lower academic skills. Study data provide an increased understanding of the needs of Hispanic Spanish-speaking mothers with children with hearing loss, as well as knowledge important for the development of improved services and support.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.