
Abstract
The purpose of the current study was to investigate the impact of COVID-19 pandemic restrictions (e.g., face mask wearing and social distancing) on individuals who are Deaf or Hard of Hearing (D/HH). The study aimed to describe perceptions of challenges and valued resources to inform efforts to mitigate negative consequences of the pandemic. A survey was used to solicit information about the pandemic-related experiences of 108 individuals who are D/HH and/or parents or service providers of children who are D/HH. Questions elicited perceptions of pandemic related challenges, resources, and supports. Results demonstrated high percentages of respondents reported experiencing substantial impacts of face mask wearing on communication. Additionally, respondents reported negative consequences of social distancing on the way they connected with others. Findings point to the need for increased awareness of risks for impacts on communication and social well-being and consideration of additional supports.
Keywords
According to the World Health Organization, more than 5% of the global population is deaf or hard of hearing (D/HH) and 26.8% of persons above 65 (National Center for Health Statistics, 2021). Given the high incidence of the population with hearing loss, a high proportion of speech-language pathologists (SLPs) have at least one client on their caseloads with hearing loss. Furthermore, SLPs and audiologists are tasked with providing counsel to other professionals on interdisciplinary teams serving individuals who are D/HH. As such, additional examination of the unique impacts of the COVID-19 pandemic is needed to inform the design and use of appropriate resources to mitigate negative impacts and support recovery efforts.
There has been growing recognition that the effects of COVID-19 restrictions may be exponentially greater for individuals who are D/HH, in part due to additional challenges to communication created by mask wearing and social distancing (Homans & Vroegop, 2021). Despite the use of varied communication modalities and languages, burgeoning reports suggest individuals who are D/HH were at risk of experiencing disproportionately large, negative impacts of the pandemic on communication (e.g., Homans & Vroegop, 2021), social-emotional wellness (e.g., Kaya et al., 2021), education, service delivery, health information access (e.g., Panko et al., 2021), and overall well-being (e.g., Shakespeare et al., 2022).
Communication Impacts
Among the domains at risk of being impacted by pandemic restrictions, communication is widely recognized as an area of concern (Chodosh et al., 2020; Homans & Vroegop, 2021; Naylor et al., 2020; West et al., 2020). Specifically, face mask wearing has been studied in relation to pandemic impacts on individuals who are D/HH. In one study of 129 adults with hearing loss in Scotland, 93% of participants indicated speech was muffled by masks and 81% indicated that face masks negatively impacted communication due to the inability to see mouth movements (Naylor et al., 2020). Similar findings were reported in another study of 221 adult cochlear implant (CI) users and found that most respondents (80%) reported face masks to be the cause of considerable problems to communication during activities of daily living (Homans & Vroegop, 2021). Considering such challenges, clear masks were recommended in some situations to potentially reduce the visual barrier of face mask wearing (e.g., Naylor et al., 2020; Pourret & Saillet, 2020); however, other studies found transparent masks to have poor acoustic properties and attenuate sounds to a greater extent than masks made of other materials (e.g., Corey et al., 2020).
Although much of the available research has focused on the attenuation of sound by face mask wearing and/or the obstruction to speech reading, individuals who use sign language may have also been negatively impacted by pandemic restrictions and face masking. Despite a vibrant community of American Sign Language (ASL) users and federal mandates to ensure linguistic accessibility (Americans with Disabilities Act, 1990; Individuals with Disabilities Education Act, 2004), individuals who are D/HH have faced many challenges accessing information through ASL, particularly in health care contexts (Myers et al., 2022; Panzer et al., 2020; Withers & Speight, 2017) that were potentially exacerbated by the COVID-19 pandemic. For those who use sign language, there are many signs that include reference to the mouth that are disrupted by masks. Furthermore, nonmanual signals (NMS) or facial expressions and lip movements are considered fundamental aspects of ASL.
Impacts of Facial Coverings on NMS
Nonmanual signals, such as facial expressions, are one of the meaningful parameters of ASL signs (e.g., Newell et al., 2010). Nonmanual signals in ASL are parallel to intonation in spoken English and help signal the type of information being conveyed. Even the slightest differences in NMS production can indicate significantly different intentions despite the production and order of the manual signs. The range of potential NMS in ASL is extensive and includes relatively straightforward components such as slight head nods to indicate positive statements and slight head shakes to indicate negation. Meanwhile, examples of more complex NMS include intricate positionings of the mouth and lips to indicate that something is relatively near, medium, or far away in distance, similarly, the degree of teeth clenching that a signer uses while referring to an event that has already passed signals just how recently it has occurred. Obstructing access to such integral linguistic and communicative components of ASL with masks and other face-coverings can be expected to significantly skew the information provided in certain constructions and negatively impact communication clarity (National Association of Interpreters in Education, 2020).
Impacts of Social Distancing on Access to ASL
During the pandemic, barriers to accessing information through ASL were potentially exacerbated across at-home, virtual learning, clinical, and work-related contexts due to social distancing. Because 95% of children who are D/HH are born to hearing parents who may not use sign language fluently (Mitchell & Karchmer, 2004), some students who are D/HH rely on the specialized settings, services, and peer groups provided by their schools as their sole or primary source of information through ASL (e.g., Deaf education classrooms, educational sign language interpreters, other classmates who are D/HH). As such, the transition to at-home and virtual learning created increased risk for children who are D/HH to be negatively impacted by limited access to communication and information spanning a myriad of domains (Panko et al., 2021; Stack Whitney & Whitney, 2021).
Access to ASL and qualified ASL interpreters is recognized as essential to ensure effective communication, legal compliance, benefit of care, and reduce liability (Americans with Disabilities Act, 1990; Individuals with Disabilities Education Act, 2004). Given reduced access to ASL interpreters during the pandemic, the use of Zoom or video remote interpreting (VRI) increased as a potentially appropriate short-term mitigation strategy. However, the use of VRI has been controversial, particularly given that its effectiveness is purported to be questionable, and some argue VRI has been overutilized (Myers et al., 2022). Concerns reported in the literature for VRI, and videoconferencing in general, have included problems with technology (e.g., slow speed, poor image quality, freezing screens), logistics (e.g., healthcare providers’ and patients’ unfamiliarity with equipment; interpreter’s inability to reposition themselves to facilitate conversational inclusion), and quality (e.g., interpreter’s difficulty accessing audible information, difficulty with trust-building which can hinder willingness to disclose health-related information, interpreters not specialized for the medical setting) (Kushalnagar et al., 2019; McKee et al., 2020; Myers et al., 2022; National Association of the Deaf, 2016).
Social Well-Being
In addition to impacts of the pandemic on communication, a growing number of studies have also considered potential pandemic impacts on social well-being for individuals who are D/HH (e.g., Homans & Vroegop, 2021). In the study of 221 adult CI users, participants reported increased social isolation and loneliness by face mask wearing which was associated with lower quality of life (Homans & Vroegop, 2021). Furthermore, in a qualitative inquiry of pandemic impacts on individuals with disabilities that included 15 adults with sensory impairments, researchers reported that the pandemic magnified social inequalities for individuals with disabilities and resulted in social exclusion, perceptions of abandonment, and lack of social justice. Among insights on social well-being reported by participations, one respondent emphasized the important role of collective gatherings in groups in relation to maintaining a sense of self and well-being. Considering that the literature suggests that individuals who are D/HH already have limited social groups with whom they can uninhibitedly communicate on a daily basis (Newell et al., 2010), the social and emotional impacts of quarantining and self-isolation were potentially exacerbated.
Research Aims
Although the impacts of physical and social distancing, mask wearing, online learning, and information sharing for individuals who are D/HH continue to emerge (Engelman & Kushalnagar, 2021; Lim et al., 2021; Moreland et al., 2021; Paludneviciene et al., 2021; Panko et al., 2021; Stack Whitney & Whitney, 2021), more research is needed to ensure individuals who are D/HH are not at risk of experiencing disrupted access to information (Murray, 2020). A greater understanding of the pandemic effects on individuals who are D/HH is also required to inform appropriate support for recovery from the health crisis and mitigate potential long-term negative effects. Thus, the current study sought to further examine and describe the experiences and perceptions of individuals who are D/HH and aimed to address the following research questions:
a. Specifically, to what extent did face masking wearing impact communication for individuals who are D/HH? b. To what extent did social distancing impact social well-being and communication with others?
Method
This study was reviewed and approved by the Institutional Review Board of the university’s Human Subjects Committee. Recruitment for the study took place in two waves. The first distribution of the survey included passive invitation by posting an open access link to the Qualtrics (Qualtrics, 2020) survey in Fall 2021 for 4 weeks. Participation was invited through a link displayed on the university ASL Research website, the National Association of Interpreters in Education quarterly newsletter, in deafness-related social media networks, and printed fliers posted in a speech and hearing clinic housed within a university setting. A total number of 47 individuals opened the link and 33 (70%) began the survey and responded to at least one question other than demographic information.
Subsequently, a second wave of recruitment took place in Spring 2022 through invitational emails sent directly to individuals who were D/HH. Using Qualtrics, the investigators sent an email invitation to 300 individuals who were D/HH served by an audiology clinic affiliated with a university. All potential participants were invited to share their experiences and perceptions of how pandemic restrictions affected communication and aspects of daily living by voluntarily completing a survey. A reminder email was sent 2 weeks after the initial invitation, resulting in a total of 77 respondents who responded to the survey invitation. Of these, two were later excluded due to responding only to demographic questions.
Participants
A total of 108 individuals completed at least one question other than demographic items on the survey. Of the 105 who responded to the question on hearing ability, 14 identified as d/Deaf (13%), 56 identified as hard of hearing (53%), and 35 (33%) were hearing individuals who indicated they were professionals serving individuals who were D/HH or a parent of a child who was D/HH. All participants were adults (19–93 years old) and identified gender as female (64, 60%) or male (41, 39%). There was a myriad of sensory devices and hearing assistive technologies used among the 70 individuals who were D/HH. Of the 65 respondents who provided information about sensory device use, 50 (77%) used hearing aids, 13 (20%) used one or more CIs, one respondent (1.5%) used a bone-anchored hearing aids (BAHA), and one (1.5%) reported using a supplemental assistive listening device. When asked about their primary communication modality, the majority (n = 81, 75%) used listening and spoken language, while others (n = 21, 19%) used both signed and spoken communication, and three respondents (3%) reported using ASL exclusively for communication. The majority (82%) of participants reported their race/ethnicity to be White (n = 89) and 11 respondents were Black (10%). Few respondents reported being from other racial or ethnic backgrounds (e.g., Hispanic/Latino, n = 1; American Indian, n = 2, Asian, n = 1). Participants reported a wide range of education levels with their highest degree attainment being high school (12%), associate’s degree or trade school (17%), bachelor’s degree (27%), master’s degree (21%), or a doctorate (21%). Of the 68 respondents who worked during the pandemic, 31 reported working remotely (46%), 24 reported in-person (35%), and 13 (19%) worked in a combination of in-person and remote contexts.
Procedures
Design of the Survey
After the initial development of survey items, the items were distributed to an advisory committee who were asked to provide feedback and suggestions for revisions. The committee was composed of seven diverse stakeholders including university faculty in communication science and disorders, an individual who was deaf, and the spouse of an individual who was deaf. The advisory group reviewed the general content for strengths and weaknesses, evaluated the organization of the survey items along with the transitions, identified any unclear items, and made suggestions for additional items that were important to include. Finally, the reviewers rated the length, clarity, and relevancy of the survey.
Soliciting and Collecting Survey Responses
Using Qualtrics, the survey was made available for participants in October 2021 with two waves of recruitment as previously described. The survey was accessed through the direct link that was shared on electronic and printed media. The survey consisted of demographic questions, quantitative questions, as well as qualitative questions. The printed media and online invitation indicated that ASL interpretation was available upon request and contact information was provided to schedule an appointment for ASL interpreter services at no cost.
Survey Instrument
The survey included quantitative as well as open-ended questions aimed at exploring perceptions of the impact of COVID-19 on individuals who are D/HH. Specifically, the survey included questions on three primary sections: demographic characteristics, impact on communication, and impact on social well-being (e.g., changes in how we connect with others). Each section included three to four questions including a yes/no question, a Likert-type scale for respondents to rate the degree of impact, and an open-text comment box for elaboration or explanation of their rating. Among social well-being questions related to communication, participants were also asked about their use of videoconferencing during the pandemic. Finally, two open-ended questions asked participants to describe issues or challenges they experienced related to pandemic restrictions, and to describe any support, resources, or positive outcomes they received or experienced during the pandemic (refer to Supplementary Appendix for survey questions).
Analyses
Descriptive statistics were used to answer the first two research questions. We examined distributions in response to consider the proportion of respondents selecting each response option for scaled questions on the degree of impacts of COVID-19 restrictions on items related to communication and social well-being. Finally, to address the last two research questions, we conducted a content and natural-language processing analysis of open-ended responses to identify the major themes in perceived issues and challenges, resources, and supports that were beneficial that were nominated by respondents. Free-text comments containing participant responses were analyzed using Leximancer v4.5, a natural language software tool (Leximancer, 2020).
The rationale for the use of Leximancer was twofold: (a) to reduce coder bias in identifying recurrent and repeated constructs, and (b) to leverage advanced text analytics methods to allow for the identification of themes that goes beyond word counting (Harwood et al., 2015). Free-text comments were first compiled into Excel spreadsheets based on their corresponding question and exported as comma-separated values (CSV) files. The CSV files were then entered into Leximancer v4.5 for analysis. Leximancer conducted quantitative content analysis of qualitative data using latent Dirichlet allocation, a machine learning technique that learns what the main concepts are in a text and how they relate to each other . . . conducts a thematic analysis and a relational (or semantic) analysis of the interview data . . . [then] provides word frequency counts and co-occurrence counts of concepts present in the transcripts of the narrative interviews. (Ward et al., 2014, p. 119)
The dominant themes and their respective concepts in the text data were then visually represented in two concept maps. The first and third authors then conducted post hoc review of text excerpts, word frequency counts, and concept maps to ensure accuracy and to conduct thematic interpretation by highlighting relevant open-ended responses that exemplify themes generated by the Leximancer software (Owen, 1984).
Results
Descriptive statistics are reported to examine impacts of the pandemic restrictions on individuals who are D/HH. The distributions in respondents’ responses are grouped into questions that related to the potential impacts on communication and social well-being.
Impacts on Communication
Table 1 reports the distribution of responses on the impact of wearing masks on communication across participants and by participants’ characteristics. The majority of respondents (87%) reported experiencing negative impacts of mask wearing on communication with 67 (62%) responding that masks made communication very difficult and hard to understand, and an additional 27 (25%) reporting that masks had some effect on communication. Only three participants (3%) reported masks had no effect on communication. Service providers and parents responded similarly with 21 (60%) reporting that masks had a large effect on communication. Responses appeared similar across groups of respondents differing in communication modalities (refer to Table 1 for specific percentages by group) although subgroups were too small to draw meaningful conclusive comparisons.
Distribution of Responses on Impact of Wearing Masks by Participants’ Characteristics.
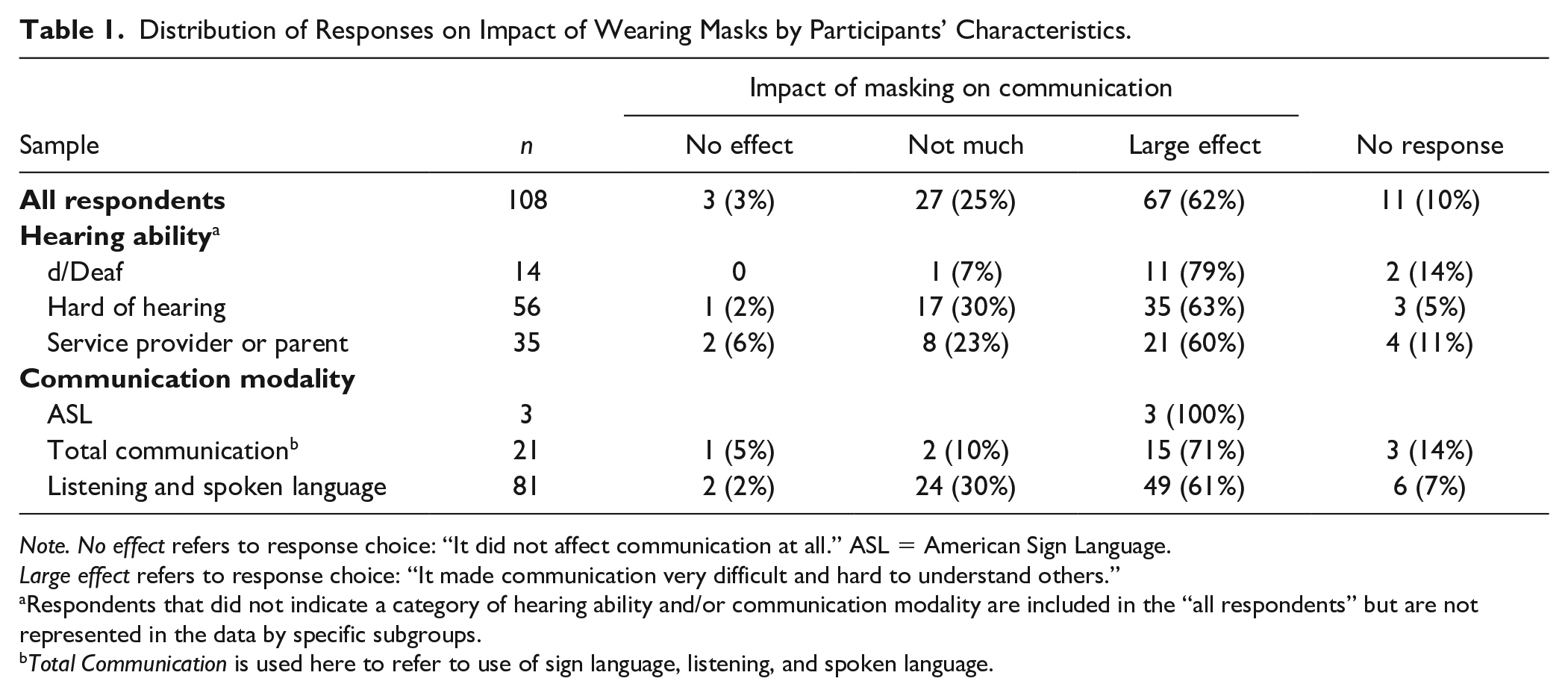
Note. No effect refers to response choice: “It did not affect communication at all.” ASL = American Sign Language.
Large effect refers to response choice: “It made communication very difficult and hard to understand others.”
Respondents that did not indicate a category of hearing ability and/or communication modality are included in the “all respondents” but are not represented in the data by specific subgroups. bTotal Communication is used here to refer to use of sign language, listening, and spoken language.
Similarly, the majority of respondents indicated experiencing negative impacts of social distancing on communication (refer to Table 2 for specific percentages by group). Of those reporting negative impacts (n = 86), the degree of impact ranged from not much or some negative impact on communication to reporting that social distancing made communication very difficult. Notably, 15 respondents (14%) indicated that social distancing did not have much impact on communication and 12 (11%) reported that they experienced no effects of social distancing on communication (refer to Table 2). Respondents who were service providers or parents reported mixed perceptions of the impact of social distancing with 34% reporting not much of an effect on communication and 29% reporting a large impact. Although there appear to be potential numerical differences between groups by hearing ability and communication mode, with 64% of individuals who were d/Deaf reporting large impacts of social distancing compared with 36% of respondents who were hard of hearing, these do not necessarily reflect statistically significant differences. An analysis of group differences and consideration of an interaction effect between hearing ability by communication mode was not conducted given that the sample included only three individuals who used ASL.
Distribution of Responses on Impact of Social Distancing on Communication.
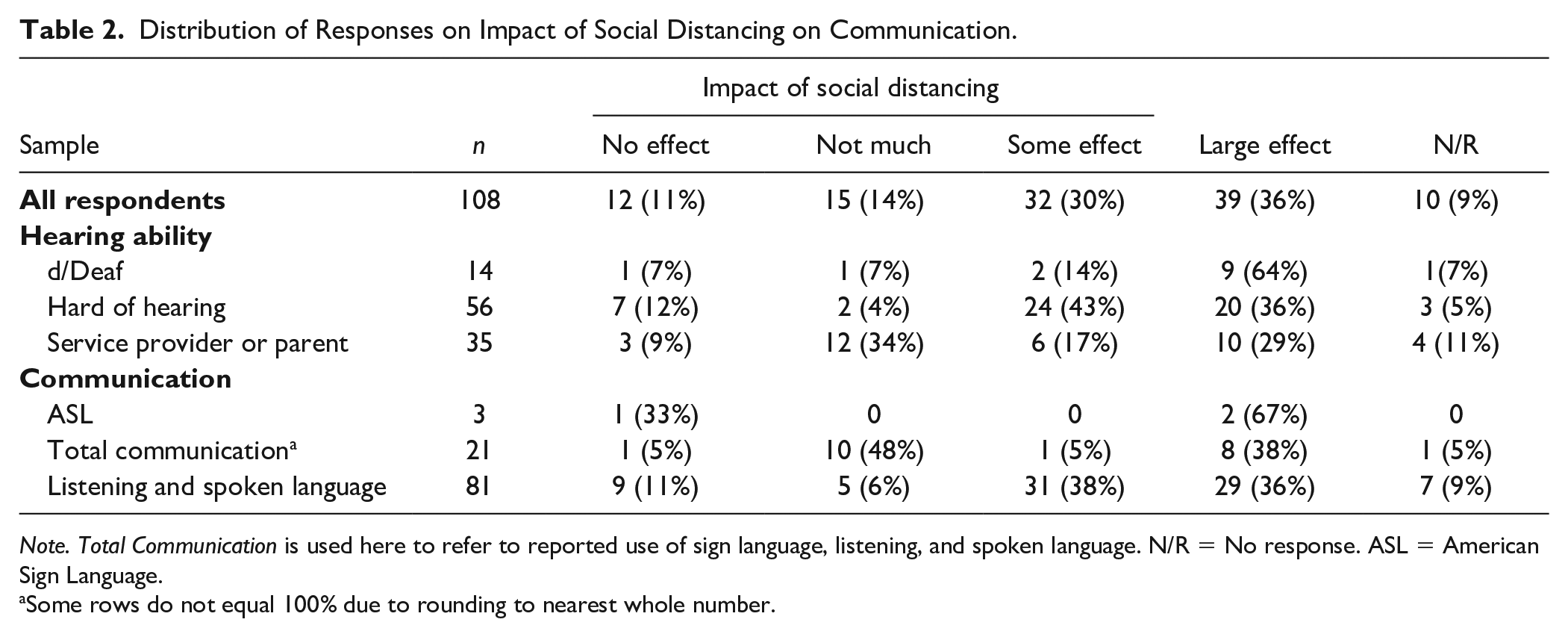
Note. Total Communication is used here to refer to reported use of sign language, listening, and spoken language. N/R = No response. ASL = American Sign Language.
Some rows do not equal 100% due to rounding to nearest whole number.
Impacts on Social Well-Being
The large majority (72%) of respondents (n = 85) reported some impact of the pandemic on how they connected socially with others. Specifically, of those who reported an impact, 29 (34%) indicated that the pandemic significantly changed how they connected with others, while the remaining respondents confirmed some impact on social interactions or mild changes to how they connected with others. Only 12 (11%) responded that there were no changes to how they connected with others and three respondents (2%) indicated that they were unsure.
Related to social interactions, the survey items also elicited information about respondents’ use of Zoom or other videoconferencing technology as a potential buffer of negative impacts or a resource to mitigate social isolation. The majority (83%) of respondents reported utilizing videoconferencing during the pandemic or as a result of the pandemic (n = 90). Written comments were also provided by 51 respondents regarding their experiences using videoconferencing who commented on positive benefits or features (31%) and negative experiences or challenging aspects of videoconferencing (69%).
When asked to comment or elaborate on their experiences, respondents’ comments noted several benefits of videoconferencing. Three respondents noted that having the option for closed captioning was advantageous. Among other benefits of videoconferencing, respondents identified being able to adjust the volume, the ability to place the interpreter in view while simultaneously viewing other screens (e.g., chat box, speaker, attendees), the absence of masks, ease of access to health care providers using Zoom, and the reduction in transportation/travel time to meet in-person. One respondent noted that Zoom worked best with four or fewer participants so all videos of participants could be easily viewed at the same time and were large enough. To further illustrate, one respondent wrote, “I liked that it made it a little easier to hear. I could ask people to either adjust their microphone or turn up my volume.”
In contrast, numerous challenges with using videoconferencing were noted in the written comments of respondents. Ten respondents commented on frustrations with technological glitches (e.g., delays in connectivity, lag times, freezing, and the poor quality of audio). Four respondents expressed difficulty in speech reading while using videoconferencing technology. Among other challenges, respondents noted difficulty seeing facial expressions, poor quality of microphones on personal devices, background noise, overlapping speech, too many people to view at once, and listening fatigue. Two respondents commented on the reduced quality of the personal interaction over Zoom, noting that it was hard to “connect and have meaningful discussion” and difficulty picking up on more subtle communication nuances.
Although closed captioning was mentioned as a strength, other respondents highlight problems including frequent errors in the content of the closed-captioning text, lags in caption text, and at times experiencing a lack of permission/access for live captioning options. Furthermore, two respondents noted experiencing difficulties learning how to turn on captions, particularly considering that there were different procedures across different videoconferencing systems.
Challenges, Resources, and Supports During COVID-19
To address the last two research questions, we examined open-ended responses regarding issues or challenges experienced related to the pandemic and resources or supports that were beneficial and/or advantageous. The Leximancer software (2020) identified two primary themes related to challenges (physical and social) with text related to communication, masks, interpreters, work, and difficulty. Comments regarding the most significant issues or challenges related to pandemic restrictions substantiated two primary themes of Physical and Social challenges. The majority of comments were strongly associated with Social challenges that described social isolation and a loss of connection with friends and professional colleagues. For example, one respondent stated that restrictions due to the pandemic changed my social status from managing without drawing attention to my disability to having to divulge my disability several times a day in order to get accommodations. The pandemic changed my self-perception [and] has made me consider myself as a person with a disability, as opposed to an independent, successful person.
Similarly, numerous respondents reported losing their jobs during the pandemic while one respondent who works in the schools noted that “keeping the same amount of contact with students’ families” was difficult once schools closed and instruction transitioned to a virtual environment. Comments about factors that negatively affected the physical act of communication were strongly associated with the Physical theme. The use of masks, that is, “Masks make it impossible to read lips and distort even loud speech,” and technological barriers, that is, “There were more things I had to do over the phone. Since I was in AVT [Auditory Verbal Therapy] after a CI activation, this was extremely difficult,” represented the most significant hindrances to communication during the pandemic.
Similarly, two overarching themes emerged from comments regarding the most beneficial resources and supports for individuals who were D/HH during the pandemic: Work and Communication, with text containing key words such as online work, skill development, ability to work at home, and Zoom. The written comments suggested that overall, remote work from home and an increase in perceived freedom and time for family represented most comments in the Work theme, that is, “More time with my husband and I really liked remote working as I had more time to do other things.” Advances in technological accommodations (e.g., online professional development courses, telehealth services, live audio transcription) were also highlighted as beneficial Work-related resources and supports. Finally, comments in the Communication theme referenced the benefits of videoconferencing that allowed respondents to reconnect with family and friends in different locations, that is, “I could Zoom with friends from college in different states.”
Discussion
Impacts on Communication
Most respondents reported experiencing negative effects of pandemic restrictions on communication. The results of the current study substantiate burgeoning reports in the literature that reveal disproportionately negative impacts of pandemic restrictions on communication for individuals who are D/HH (e.g., Chodosh et al., 2020; Homans & Vroegop, 2021; Naylor et al., 2020). Similar to previous reports of muffled speech and difficulty speech reading with face mask wear (e.g., Naylor et al., 2020), respondents in the current study experienced similar effects of mask wearing and social distancing on communication. Most notably, mask wearing during the pandemic significantly hindered respondents’ ability to lip read and comprehend speech even at loud volumes. Considering the importance of NMS reported in the literature (e.g., Newell et al., 2010), it was not surprising that respondents who used ASL also reported experiencing negative impacts of masking on clarity of communication.
The trends in respondents’ free-text comments on the strengths and challenges of videoconferencing, videoconferencing interpreting (VRI), and other forms of teletherapy for individuals who are D/HH were consistent with concerns present in the literature (e.g., Myers et al., 2022). Logistical and technological barriers due to service providers’ and patients’ unfamiliarity with equipment, like CI-compatible telephones and disruptions to AVT, appeared to be exacerbated by the COVID-19 pandemic (Withers & Speight, 2017) and proved problematic for many respondents. Likewise, some of the challenges that surfaced in written comments (e.g., delays in connectivity, lag times, freezing, and the poor quality of audio) mirrored concerns raised in the existing literature regarding the use of VRI (Myers et al., 2022).
Social Well-Being
The finding that respondents reported increased social isolation and loneliness associated with pandemic-related restrictions is considered a key finding and substantiates existing evidence in the literature (e.g., Homans & Vroegop, 2021). Like prior qualitative inquiries and empirical reports of pandemic impacts (e.g., Homans & Vroegop, 2021; Kaya et al., 2021), the major themes that emerged from free-text responses were strongly associated with challenges that threatened social well-being. Losses of self-perceived independence and success, including reports of pandemic-related unemployment and job loss, are alarming and necessitate a need for more resources to reduce social inequalities for individuals with disabilities. In addition, given that respondents in the current study also described social isolation and a loss of connection with friends and professional colleagues, the findings lend support for the need for deliberate efforts to facilitate interactions and communication access to bolster social well-being. Although this study did not test effects of different types of support, the previous literature points to benefits of peer-to-peer support on reducing stress and improving social-emotional well-being for families that include a family member who is D/HH (e.g., Jackson, 2011; Jackson et al., 2008).
Despite the negative effects of pandemic restrictions on communication highlighted in the current study, our findings also suggest that advances in technological accommodations (e.g., live audio transcription) and workforce flexibility (i.e., remote work) provided respite for many respondents. Accessibility to remote work from home, web-based professional development, and virtual meetups were advantageous for most respondents’ as they improved perceptions of individual freedom and social well-being. Although causal inferences cannot be made with the current design, increased access to telehealth services during the pandemic was also reported to be a substantial benefit and a potential remedy to previously reported barriers to information access (e.g., Myers et al., 2022). Although the current survey did not specifically focus on healthcare contexts, such results may offer insights for service providers in the health care sector. However, more empirical evidence is needed with consideration of steps for improvement to accessible, effective information sharing for professionals serving individuals who are D/HH.
Implications
Given the reported negative impacts of face mask wearing on communication, results suggest additional efforts may be needed to ensure that individuals who are D/HH have access to clear shields or other supports designed to diminish or prevent further negative effects on communication. Additional support or resources may need to be further considered and widely implemented to ensure equitable access to communication. The current findings provide further rationale for additional research on adaptive or assistive support designed for individuals who are D/HH. The reported negative impacts of face masking on attenuation of speech and obstruction of speech reading support the need for consideration of materials or fabrics that are less obstructive to sound wave transmission (Corey et al., 2020) and/or ensure visual access for speech reading, facial expressions, and other NMS. Minimally, the current findings suggest service providers should be mindful of the degraded sensory access to the speech signal and mouth movements while mask wearing (Goldin et al., 2020). In addition, service providers could consider potential supplemental efforts toward ensuring equitable access to communication, such as providing an accompanying written message (i.e., text or email), summarizing and paraphrasing spoken messages, and frequently checking for understanding.
The written comments of respondents in the current study offer insights for service providers who are working or communicating with individuals who are D/HH over videoconferencing platforms. Given the highlighted challenges of using videoconferencing, service providers may want to consider minimizing background noise, avoiding overlapping speech, pausing to adjust for lags, monitoring technical glitches closely to minimize disruptions to communication, and being sensitive to the need for wait-time during such delays and freezing. As respondents in the current study reported having trouble learning how to turn closed captioning on, service providers may want to consider offering tutorials or instructional briefs and inquiring about desired support with clients and their family members.
The findings of the current study substantiate the need for service providers to consider appropriate support and resources to ensure equitable access for individuals who are D/HH. In light of communication access challenges experienced by respondents in the current study, it may be beneficial for educators and service providers to consider available best practice guides such as National Deaf Center (NDC) for suggestions on retaining access to accommodations and supports (Sutton, 2020). Among suggestions included in the NDC practice guide, service providers should ensure that interpreters are available in online meetings or hybrid meeting spaces, provide live captioning on all media (not relying on auto-captioning services), check in regularly with individuals who are D/HH, set up clear protocols for requesting accommodations, and connect individuals who are D/HH with each other to assist in forming social connections, reliable allies, and foster positive social wellness (Sutton, 2020).
Limitations
Although insightful, results of this study should be interpreted cautiously for several reasons. Limitations common to survey design methodology should be considered such as the difficulty assessing accuracy and truthfulness of responses, recognizing that impacts are self-reported, and individuals may tend to over- or underestimate the degree of impact. Furthermore, potential limitations in generalizability should be noted due to using a nonrandom sampling procedure. As participants were recruited in two waves, second-wave respondents (i.e., D/HH respondents) may have experienced pandemic impacts for a longer period of time compared with first-wave respondents (i.e., service providers); thus, reported challenges may have varied between groups. Although it is considered a strength that different communication modalities and sensory devices were used by respondents, many of the survey respondents used spoken language as their primary mode of communication and therefore it cannot be assured that trends in the current findings would adequately generalize to individuals in the Deaf community who predominantly use ASL. It is possible that individuals who chose to respond were drawn to the topic of the survey and therefore it cannot be assumed that results would be similar with a random sample. In addition, it should be noted that the respondent pool did not include a highly diverse sample in terms of participants from diverse racial and ethnic backgrounds. Although the participant sample was diverse in some characteristics (e.g., communication modality and education level), it cannot be assumed that the results would generalize to the larger population of individuals who are D/HH from different racial, ethnic, and linguistic backgrounds.
Conclusion and Future Directions
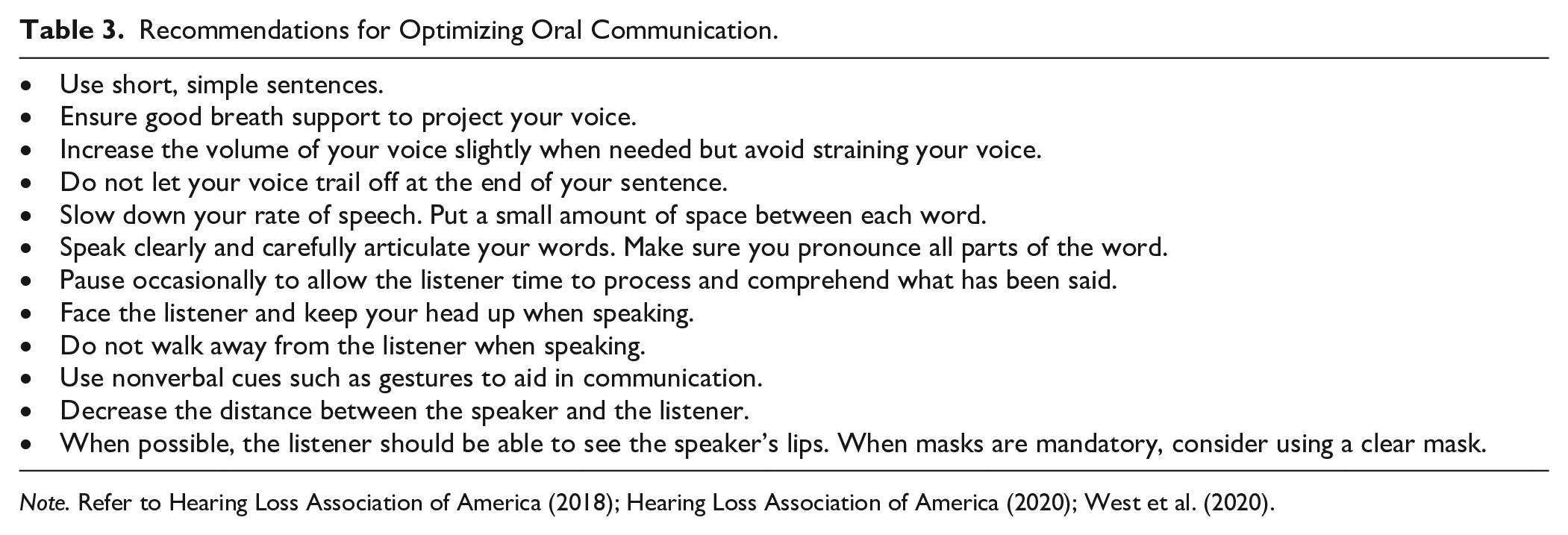
Findings of the current study further substantiate the need for the development and implementation of innovative supports to minimize communication and social wellness barriers for individuals who are D/HH. Although the current study was not specifically designed to identify appropriate communication supports, Table 3 offers potential supports for service providers to consider based on the broader available literature. In light of the additional challenges to communication brought on by health precautions of face mask wearing and long-standing challenges to patient–provider communication during hospitalization (Shukla et al., 2019), public service announcements and health information may need to be considered that would bolster health care workers awareness of ways to reduce communication barriers with D/HH individuals as well.
Recommendations for Optimizing Oral Communication.
Supplemental Material
sj-docx-1-cdq-10.1177_15257401231181506 – Supplemental material for Pandemic Impacts on Communication and Social Well-Being: Consideration for Individuals D/HH
Supplemental material, sj-docx-1-cdq-10.1177_15257401231181506 for Pandemic Impacts on Communication and Social Well-Being: Consideration for Individuals D/HH by Carla Wood, Kristen Guynes, Victor Lugo, Lindsey Baker and Selena Snowden in Communication Disorders Quarterly
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The third author, Victor Lugo, was supported by Grant# H325D190011, funded by the U.S. Department of Education. The opinions expressed are those of the authors and do not represent views of the U.S. Department of Education.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.