
Abstract
Data on attaining indicators of early speech, language, and literacy development, notably phonological awareness, among children with visual impairments (VI) are limited. This U.S. study utilized the National Survey of Children’s Health (NSCH), 2016–2020, to observe the distinctive population of children with VI and speech, language, and literacy needs. Chi-square bivariate and multivariable logistic regression analyses established differences between children ages 3 to 5 years with VI (n = 186) and without VI (n = 25,354). Significant differences included lower parental education and higher rates of family poverty for children with VI. Significantly fewer children with VI had attained early phonological awareness (identifying initial sounds in words and word rhyming). Nearly three times more children with VI had been diagnosed with a speech or language disorder. Findings affirm that interventions address speech, language, and literacy development among children with VI, including explicit phonological awareness. Communication disorders research based on population health databases can inform evidence-based practice.
Keywords
Children with visual impairments (VI) may face unique challenges in developing speech, language, and literacy skills (Brouwer et al., 2015; Brouwer & Gordon-Pershey, 2021; Gordon-Pershey et al., 2019). Such challenges may focus largely on the development of phonological awareness, which is demonstrated by a child’s unconscious and conscious sensitivity to the speech sounds in words. Phonological awareness is a multi-stage, foundational speech-language skill for early literacy development that usually matures during the preschool and early school years, ages 3 to 7 (Paulson, 2004; Schuele & Boudreau, 2008). It is notable that phonological awareness provides the auditory-perceptual and cognitive-linguistic bases for learning the letter-sound correspondences that comprise instruction in alphabetics and phonics (National Reading Panel, 2000).
Phonological Awareness in Children With VI
In the first stages of phonological awareness, children demonstrate awareness of speech sounds through, for example, early spoken word rhyming and identifying initial sounds in spoken words. Speech-to-print correspondences develop as children connect the sound structures of words to the visual or tactile properties of written letters and words (Moats, 2005, 2020). Based on their knowledge of the auditory patterns and regularities of speech sounds, children begin to sound out printed or braille words. Phonological awareness is a measurable indicator of early speech-language and literacy development and is widely assessed by the universal screenings and large-scale developmental literacy assessments given by schools and districts (e.g., University of Oregon, Center on Teaching and Learning, 2022) as well as during the individualized speech-language and literacy assessments given by developmental diagnosticians (e.g., Wagner et al., 2013).
A small body of scholarship has examined the link between phonological awareness and VI in young literacy learners. Prior studies have explored whether children with VI may have difficulties developing the phonological awareness that would underlie learning to use the braille alphabet (cf. Dodd & Conn, 2000; Gillon & Young, 2002; Hatton et al., 2010). According to a systematic review of the existing literature on speech, language, and literacy development in preschool children with VI conducted by Mosca et al. (2015), children with VI face challenges in developing speech, language, and literacy skills, particularly in the development of phonological awareness. However, the Mosca et al. review found that there is limited research on the link between VI and phonological awareness.
While other studies do not show measurably significant phonological awareness differences between young children with VI and their age peers without VI (Barlow–Brown & Connelly, 2002; Dodd & Conn, 2000; Gillon & Young, 2002; Hatton et al., 2010), caution must be used when interpreting their results and generalizing to the larger population of children with VI, due to the small samples used in VI research. For example, Hatton et al. (2010) and Gillon and Young (2002) assessed phonological awareness among 22 and 19 children with VI, respectively.
Multiple Factors Affect Speech, Language, and Literacy in Children With Visual Impairments
Another challenge of working with small samples of children with VI is the limited ability to account for other factors that affect the development of children with disorders and disabilities (Brouwer et al., 2015; Brouwer & Gordon-Pershey, 2021; Gordon-Pershey et al., 2019). These factors include parent or caregiver (herein: parents) education levels and/or family socioeconomic status, notably poverty status (cf. Mollborn et al., 2014; Nathan et al., 2004; National Research Council, 1998). It is noteworthy that children with developmental disorders and disabilities regularly experience multiple and intersecting impacts (Crenshaw, 1989) on development and learning (National Center for Learning Disabilities, 2020).
Population Health Data Sets in the Study of Children With Visual Impairments
The limitations of the prior studies and the questions that remain about speech, language, and literacy development in children with VI necessitate establishing a clearer understanding of other potential sources of data on VI and its relationship to speech, language, and literacy development. Without this information, stakeholders, such as education and therapy professionals, researchers, and policy makers, cannot adequately design programs or write guidance statements to support the development of children with VI. The present study capitalizes on an opportunity to address finding answers to questions related to VI and speech, language, and literacy development as evidenced by the results of the large, nationally representative sample found in a publicly available data set, the United States’ National Survey of Children’s Health (NSCH, U.S. Census Bureau, n.d.). The NSCH is one of the few publicly available data sources that collects information on multiple developmental factors, including VI and speech, language, and literacy development, across a sizeable sample of children and across a range of socioeconomic and family circumstances. The NSCH has served as the data source for many high-quality, peer reviewed publications examining the health and wellness of children (e.g., Child and Adolescent Health Measurement Initiative, CAHMI, n.d.). Of note, the NSCH is unique compared with other administrative or clinical data sets in that it includes children who may not be identified clinically but whose deficits are known to their parents.
Population Health Data Sets in Communication Sciences and Disorders Research
Studies that use national databases to explore the characteristics of disorders and disabilities populations are represented in the literature on children’s communication development and disorders (Raghavan et al., 2018). For example, Hammer et al. (2010) used a Head Start Family and Child Services database to review child and family characteristics, occurrence of speech-language impairment, and home literacy environment among children from low-income families. Breit-Smith et al. (2010) used a U.S. Department of Education database to explore the extent to which parent-reported home literacy activities and child emergent literacy skills differ among children with developmental disabilities and those who are developing typically. As such, the present study can contribute to the body of analyses of population health data sets in the field of communication sciences and disorders.
Purpose and Significance
The purpose of the present study is to explore whether the children whose parents identified them as having VI identified them as having less capable performance on the NSCH variables that account for early speech, language, and literacy development than the children without VI, notably in the two phonological awareness tasks of identifying initial sounds in words and rhyming words. Moreover, the present analysis examined whether the children with VI were identified as having speech, language, and literacy concerns in greater numbers proportionally than the children without VI. Furthermore, the developmental and environmental factors that may affect the children with VI were examined for how these differ from the children without VI. As such, significantly more can be known about the early speech, language, and literacy development in children with VI than has been demonstrated by prior small-scale studies. Differences across the populations with VI and without VI could indicate a significant need for preschool intervention programs to support speech, language, and literacy development among children with VI, as well as signal a call to action for parents, educational personnel, and researchers.
Method
The NSCH is sponsored by the U.S. Health Resources and Services Administration’s Maternal and Child Health Bureau and is publicly available through the U.S. Census Bureau (n.d.). The NSCH collects extensive data on the health, health care, development, and education of children from birth to age 17 via parent- or guardian-reported survey responses. In households with more than one child, a single study child was selected for data collection by the survey administrators.
The present analysis included 25,540 children ages 3 to 5 years whose parents or guardians answered the NSCH questions about speech, language, and literacy development and VI in the survey administration of 2016 to 2020. The present analyses excluded data for children reported to have cerebral palsy, Down syndrome, intellectual disability, autism spectrum disorder, brain injury, and hearing impairment, given the far-reaching impacts of these primary diagnoses on the occurrence of speech, language, and literacy disorders among children with VI (cf. Gordon-Pershey et al., 2019). The resulting analytic data set included children whose parents reported that the children were professionally diagnosed as having developmental delay and/or they had received early intervention or special education services, but they had not been diagnosed with the specific primary disorders excluded above.
One difficulty with the NSCH data set is there is no way to identify the order in which the participating children’s disorders or disabilities were diagnosed (e.g., were the initial reasons for early intervention and/or special education placement related to VI, or were speech, language, or literacy concerns the initial reasons, or was another diagnostic condition or a general developmental delay the initial reason). Children’s developmental disabilities were recorded, but not their order of emergence.
The NSCH established the presence of VI by asking whether the child has “blindness or problems with seeing, even when wearing glasses” (by asking parents to provide a yes or no response). To establish a diagnosis of speech or language disorder, the survey asked for a yes or no response to the question, “Has a doctor, other health care provider, or educator EVER told you that this child has . . . a speech or other language disorder?” To establish the presence of speech, language, and literacy skills, the survey asked whether children have demonstrated four developmental skills:
Recognize the letters of the alphabet (parents’ response options were: “All of them,” “Most of them,” “About half of them,” “Some of them,” “None of them”);
Write their names, posed as, “How often can this child write their first name, even if some of the letters aren’t quite right or are backwards?” (response options were: “Always,” “Most of the time,” “About half the time,” “Sometimes,” “Never”);
Perform the phonological awareness task of recognizing the beginning sound of a word, posed as, “How often can this child recognize the beginning sound of a word? For example, can they tell you that the word “ball” starts with the “buh” sound?” (response options were: “Always,” “Most of the time,” “About half the time,” “Sometimes,” “Never”);
Perform the phonological awareness task of rhyming words, asked as, “Can this child rhyme words?” (asking parents to provide a yes or no response).
It is unknown how the parents of children with VI addressed the questions regarding reading alphabet letters and writing their name. That is, it is not known how parents perceived reading and writing performance in children with VI, including whether they considered the use of braille or other tactile or non-print representations to be equivalent to literacy development.
Data Analyses
Due to the small sample size of children with VI (n = 186), for questions regarding recognizing letters of the alphabet, writing their name, and recognizing the beginning sounds of words, response options were dichotomized into (1) all or most of the time or (2) about half the time, sometimes, or never. Rhyming words was asked as a dichotomous choice of yes or no. Bivariate Pearson’s chi-square (χ2) and multivariable logistic regression analyses established whether there were differences in parental responses for children with VI and without VI that might reveal risks in speech, language, or literacy development. Regression analyses controlled for child age, sex, race, ethnicity, and family poverty status. Analyses were conducted using Stata 15.0 software (StataCorp, 2021), accounting for the NSCH design features and weights. Between groups significance was set at α ≤0.05 to indicate that children with VI and without VI would differ in the occurrence of diagnosis of speech or language disorder and the performance of the four early speech, language, and literacy skills.
Results
As reported in Table 1, of the survey sample of 25,540 children ages 3 to 5, the present analysis accounted for 186 children with VI and 25,354 children without VI. Children with VI were slightly but significantly older (
Sample Characteristics, by Presence of Visual Impairment (N = 25,540).
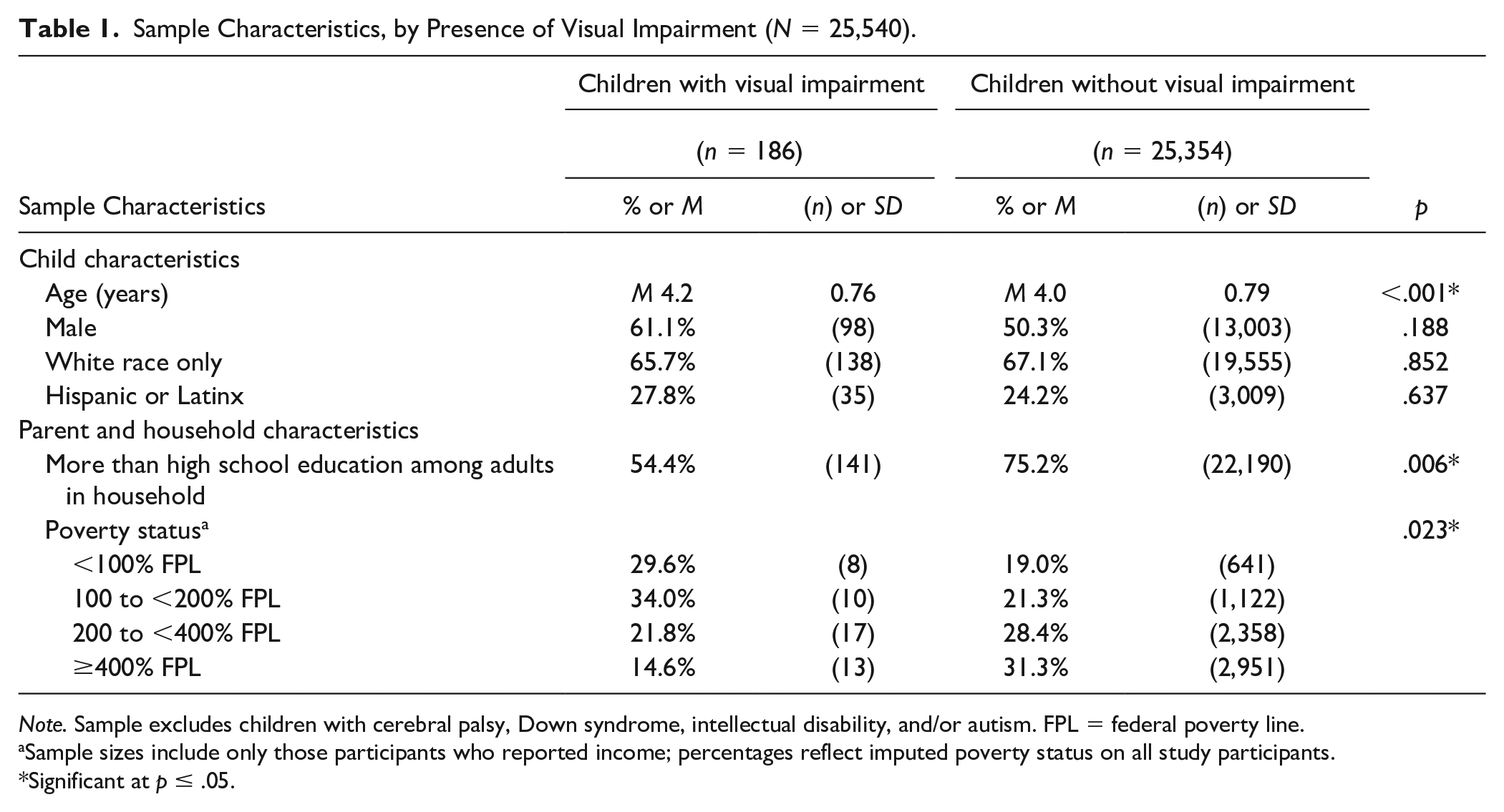
Note. Sample excludes children with cerebral palsy, Down syndrome, intellectual disability, and/or autism. FPL = federal poverty line.
Sample sizes include only those participants who reported income; percentages reflect imputed poverty status on all study participants.
Significant at p ≤ .05.
Environmental Factors
As shown in Table 1, fewer children with VI (54.4%) were from households in which the highest level of parental educational attainment was more than a high school diploma (e.g., some college, college graduate) than children without VI (75.2% for those without VI, p = .006). There were also differences in poverty status by the presence of VI (p = .023). More children with VI lived in families below the poverty line (29.6%, vs. 19.0% of children without VI) or within 100% to <200% of the poverty line (34.0% with VI vs. 21.3% without VI).
Foundational Speech, Language and Literacy Skills
As shown in Table 2, controlling all analyses for age, sex, and family sociodemographic factors of race, ethnicity, and poverty status, regarding recognizing letters of the alphabet, there were no significant differences in bivariate or multivariate analyses. Children with VI (63.4%) were significantly less likely to be able to recognize the beginning sounds in words (as compared with 78.4% of children without VI, p = .031), but this became nonsignificant in multivariate models. Whether children could write their name did not vary by the presence of VI in bivariate analyses (46.8% vs. 55.2%, p = .315) but did vary in multivariate analyses. Children with VI were 62% less likely to be able to write their names (derived from the odds ratio [OR = 0.38], with a 95% confidence interval [CI] of [0.18, 0.83]). Bivariate analyses showed that children with VI (44.8%) were less likely to be able to rhyme words than those without VI (69.2%, p = .001). This difference remained statistically significant in multivariate models: children with VI were 72% less likely to be able to rhyme words than those without VI (derived from the odds ratio [OR = .28], with a 95% CI of [0.14, 0.56]).
Speech, Language, and Literacy Development by Presence of Visual Impairment, Bivariate and Multivariate Results.
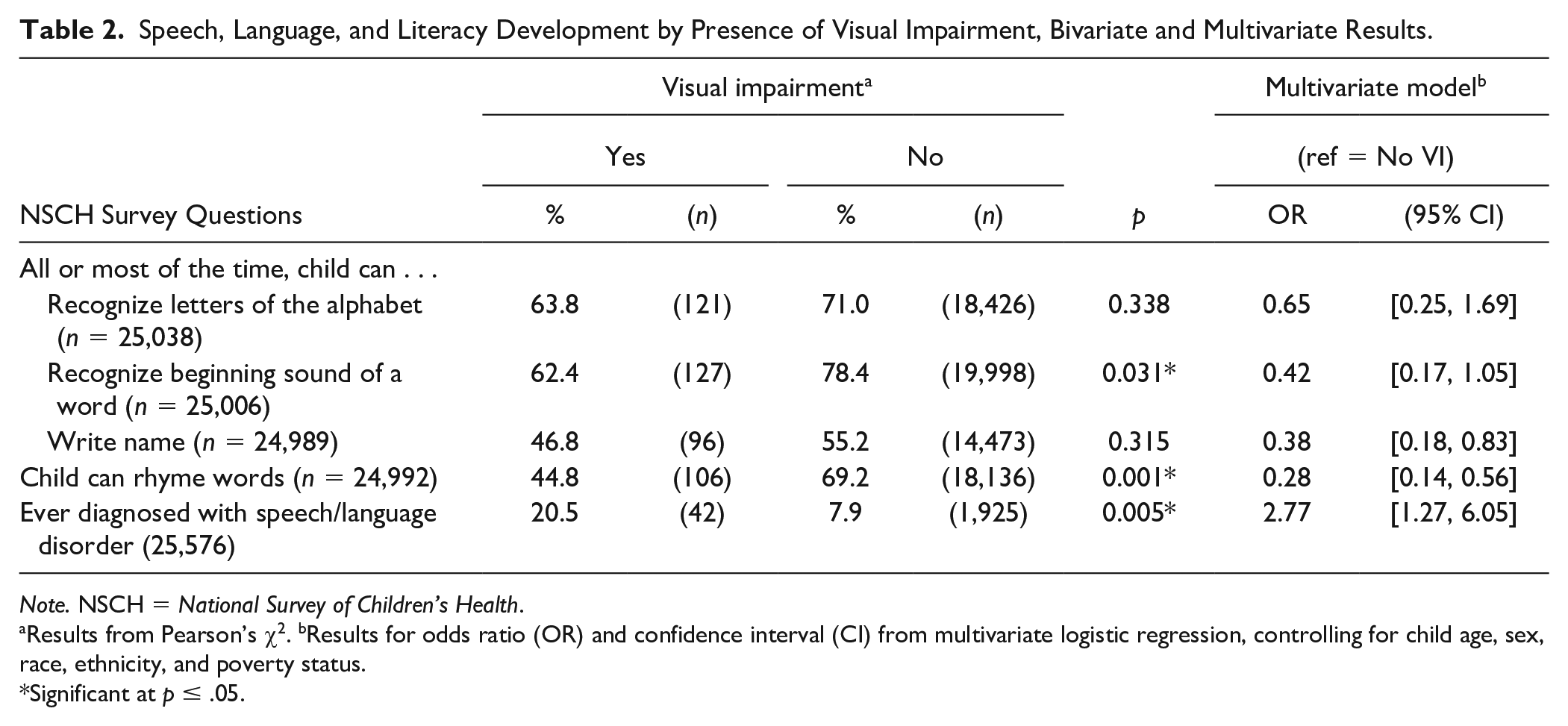
Note. NSCH = National Survey of Children’s Health.
Results from Pearson’s χ2. bResults for odds ratio (OR) and confidence interval (CI) from multivariate logistic regression, controlling for child age, sex, race, ethnicity, and poverty status.
Significant at p ≤ .05.
History of Speech or Language Disorders
As noted in Table 2, significantly, 20.5% of children with VI had ever been diagnosed with a speech or language disorder, compared with 7.9% of children without VI (p = .005). This difference remained statistically significant in multivariate analyses, showing that children with VI were nearly three times more likely to be diagnosed with speech or language disorders (as derived from the odds ratio of almost 3; OR = 2.77; 95% CI [1.27, 6.05]).
Discussion
This report entails the first known population health study to identify a representation of how the national population of preschool children exhibits the co-occurrence of VI and speech, language, and literacy developmental concerns. Using a nationally representative sample of children ages 3 to 5 years old, controlled to include children who manifest VI along with speech, language, and literacy concerns but excluding children with primary disorders that may account for the presents of the co-occurrence of VI and speech, language, and literacy difficulties, the distinctive population of children with VI and speech, language, and literacy needs can be observed. Moreover, a specific focus on measures of phonological awareness helps further delineate the population’s developmental characteristics.
Importantly, the present research accounts for the impact of sociodemographic variables, including parental education and family poverty, which can independently put children at risk for delayed speech, language, and literacy development (National Center for Learning Disabilities, 2020). These parental and family factors must be explicitly addressed in the development and dissemination of programs to support preschool speech, language, and literacy, to ensure that children who face the intersectionality (Crenshaw, 1989) of VI and environmental challenges benefit from appropriate and effective teaching and therapies.
Given that the children with VI in the NSCH sample were significantly older than those without VI, the current findings evidenced their risk for delayed speech, language, and literacy development. The children with VI were nearly three times more likely to be diagnosed with speech or language disorders than their age peers without VI. Children with VI exhibited delayed early phonological awareness skills compared with their age peers that were significant for recognizing the beginning sound of a word and word rhyming skills.
The present findings are relevant to evidence-based practice and indicate a need for educational and intervention programs to support speech, language, and literacy development among children with VI, and point to the need to include explicit phonological awareness instruction in these efforts. This recommendation aligns with Moats (2005, 2020), who stressed the explicit teaching of conscious phonological awareness, including rhyming, during preschool and early elementary education for all children. The findings herein indicate that explicit training must be included for preschoolers with VI.
Moreover, the present investigation reinforces the urgency of implementing actions to involve parents, medical service providers, educational personnel, and researchers. For parents, these data suggest that being proactive in obtaining speech, language, and literacy services for young children is recommended, and to not wait for delays to occur. According to the present data, families of children with VI may be in economic circumstances in which they are less likely to have access to care and professional supports (National Center for Learning Disabilities, 2020), making advocacy on the part of all service providers imperative.
The conclusions offered by this study suggest that as soon as a young child receives a VI diagnosis, medical and educational service providers and family caregivers would collaboratively develop an individualized family service plan that empowers the caregivers and provides a referral for the necessary levels of monitoring, screening, diagnosis, and treatment by a speech-language pathologist (SLP). Professional development for SLPs needs to address designing screenings, assessments, and intervention methods that are specific to the speech, language, and literacy development in children with VI (cf. Brouwer et al., 2013). Caregiver empowerment would include developmental knowledge regarding early speech, language, and literacy development, along with practical facilitative techniques to implement at home.
For researchers, this study opens new and exciting avenues of investigation. First, researchers need to design more refined measures of early speech, language, and literacy skills as related to vision status. The current study relied upon parent responses to survey questions; administering expanded skill-based measures for children would provide greater clarity regarding risk factors and skill development. For example, measures may help ascertain the relationship between different types of VI and the nature of early speech, language, and literacy development. It is likely that speech, language, and literacy development are related to VI in nuanced ways.
Second, the extant literature on the relationship between early speech, language, and literacy skills and VI has relied upon case reports, cross-sectional methods, and survey methods (cf. Gordon-Pershey et al., 2019). Longitudinal research is imperative to understand the nature of development in this population, to identify contextual variables that influence development, and to assess the effectiveness of early intervention. Toward this end, researchers and large-scale public database administrators need to include vision status within their population characteristics and outcomes data. For example, the American Speech-Language-Hearing Association (ASHA) initiates numerous efforts to document population characteristics and outcome data for individuals with communication disorders, but vision status as a variable appears not to be currently among the collected information. Expanding the data available will lead to better studies, whose findings will empower caregivers and service providers to make better early intervention decisions and provide more effective services.
Finally, the current study highlights the need for more interprofessional collaborations between SLPs and the medical and educational specialists who serve children with VI. The literature is sparse regarding the existence and effectiveness of these interprofessional collaborations, but SLPs have reported feeling unprepared to effectively serve the VI population and that discipline-specific professional development opportunities are extremely rare (Brouwer et al., 2013).
Limitations
One limitation of the NSCH data is that it does not identify different levels of VI. There is no indication of the severity of the child’s vision loss. Subgroups of abilities may exist in the NSCH data that are not identified. Children with potentially very different levels of visual ability may learn literacy in very different ways and at different rates of development. Second, although there are limitations to parent-report data, including uncertainty about the information and perceptions that parents had in mind when responding to the survey questions regarding reading development among children with VI (e.g., whether parents considered the use of braille or non-print communications to be equivalent to literacy development), the findings align with previous studies. That children with VI had a higher likelihood of being diagnosed with speech or language disorders than their peers without VI is a robust and reliable result attained in prior research (Brouwer et al., 2015; Brouwer & Gordon-Pershey, 2021; Gordon-Pershey et al., 2019).
Conclusion
This study of population health found that children with VI are at risk for delayed speech, language, and literacy skills. Importantly, many children with VI experience the intersection of disorders, disability, and poverty and may be less likely to be able to access care and professional supports. Policy makers and advocates can use this study’s information as evidence to inform resource allocation and access to care for children with VI. Findings advance the current literature available to stakeholders seeking to develop evidence-based services, publish higher quality research, and ultimately improve outcomes for children with VI.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors’ financial disclosures entail their employment at their affiliated organizations. The authors have no other financial disclosures relevant to this publication.