
Abstract
Preachers are professional voice users (PVUs) who regularly experience high vocal demands, often leading to vocal difficulties or disorders. Research has established that this often occurs due to a lack of sufficient knowledge of the vocal mechanism and vocal hygiene in this population. Student preachers are therefore also considered to be a potential at-risk group for the development of vocal difficulties once they enter the occupation. This study therefore aimed to determine the knowledge and needs of theology students at a South African institution of higher education regarding voice production and vocal hygiene. A cross-sectional online survey using non-probability purposive and convenience sampling was distributed to participants through email to obtain data on the education, training, needs, and knowledge of voice production, vocal hygiene, and voice use among the participants. A clear need was observed for education and training on vocal health and hygiene amongst the study population. The participants presented with limited knowledge about voice production and vocal hygiene; however, they also reported to not regularly implement this limited knowledge in day-to-day voice use or practice. This study found a willingness among participants to learn more about voice and vocal hygiene. This study confirmed that theology students, as future PVUs, receive minimal-to-no training on voice and vocal hygiene, despite their increased risk for voice difficulties.
Voice production constitutes a fundamental aspect of human identity (Jeffrey, 2017) as it reflects an individual’s age, gender, emotions, and personality (Tiwari & Tiwari, 2012). Voice also plays a critical role in the occupational lives of numerous professionals, such as preachers, who fall within the second level of Koufman and Isaacson’s (1991) Four Level Framework for the Classification of Professional Voice Users (PVUs) which classifies professions according to the vocal demands of their occupation (Zabret et al., 2018). PVUs rely on their voice for executing occupational duties and garnering an income (Ibekwe, 2019). Consequently, even moderate voice impairments could negatively impact their occupational performance (Ibekwe, 2019; Koufman & Isaacson, 1991).
Vocal demands experienced by preachers are especially high as they regularly engage in voice-intensive tasks such as delivering sermons in halls with poor amplification and acoustics, and to large audiences with poor or no amplification (Ibekwe, 2019; Middleton & Hinton, 2008). This increased vocal demand often causes preachers to experience reduced voice quality, hoarseness, and vocal fatigue (Lobo et al., 2017). Vocal fatigue manifests through changes in voice quality, increased vocal exertion, discomfort in the larynx, painful phonation, diminished pitch range, neck and shoulder muscle tension, a dry throat, weakened resonance which usually starts to emerge progressively with voice use during the day, and alleviates with rest (Boone et al., 2020). Recent research found that among participating Catholic priests, most experienced vocal difficulties during their careers (Bȕyȕkatalay et al., 2019). A possible explanation for this could include either (1) overuse due to limited knowledge regarding vocal health and hygiene or (2) ineffective implementation of vocal health and hygiene practices (Ibekwe, 2019).
Internal characteristics such as talkativeness (extent of daily voice use) and vocal loudness place increased strain on the voice and can cause swelling and inflammation in the larynx, negatively impacting voice quality (Lobo et al., 2017). In addition, throat clearing behaviors and coughing could result from reduced vocal hygiene practices, which could further negatively impact voice quality resulting in vocal pathology (Hagelberg & Simberg, 2015). These behaviors bring about vigorous aperiodic vocal fold adduction, which could cause vocal trauma and is associated with long-term vocal difficulties (Devadas et al., 2015). External elements such as air pollution, environmental noise, and air conditioning can also affect the ability of a preacher to produce adequate vocal loudness to be heard during sermons (Ibekwe, 2019). Such environmental factors could further contribute to dehydration of the mucosal lining of the vocal folds, increasing the risk for vocal pathology (Lobo et al., 2017). Interestingly, a recent systematic review by Nair et al. (2024) found that environmental factors such as air conditioning, work factors such as prolonged voice use, and lifestyle factors such as insufficient water intake, an increased consumption of caffeinated beverages, and smoking have a significant association with PVUs such as telemarketers reporting symptoms of vocal fatigue, not only extended periods of voice use. Most factors associated with vocal difficulty in PVUs are preventable by means of education and training (Devadas et al., 2015; Timmermans et al., 2005). Knowledge about vocal health and hygiene is critical to prevent vocal fatigue and hyperfunction and to promote healthy vocal behaviors among PVUs, such as preachers (Pomaville et al., 2020). Such protective-preventative strategies are thus also favored by speech-language pathologists (SLPs) in preventing vocal pathology (Sezın et al., 2018).
Knowledge regarding vocal hygiene typically comprises understanding types and amount of voice use, phonotrauma, and lifestyle practices (Rangarathnam et al., 2017). Despite this being critical for the prevention of voice disorders, research has found that many future and current PVUs, including preachers, remain largely uninformed about what constitutes phonotrauma and the effects these behaviors might have on their voice production in the longer term (Cielo et al., 2015). This lack of knowledge may be attributed to the general lack of voice training received by PVUs, which is considered the most significant risk factor for vocal pathology in the population (Devadas et al., 2015).
Research has found a need for programs covering vocal health instruction in the curriculum of future PVUs (Sezın et al., 2018). Still, students in preaching programs remain a mostly unexplored population, with a widespread presence of vocal difficulties, and exposure to high vocal demands during academic activities (Jayakumar & Yasin, 2021).
Research regarding vocal knowledge and behaviors among students of Alimah, a religious Indian profession, found the presence of phonotrauma and poor nonvocal behaviors (Jayakumar & Yasin, 2021). In the study, students were found to possess basic knowledge regarding voice and were aware of the prevalence of voice disorders in their profession but lacked sufficient training on vocal care techniques (Jayakumar & Yasin, 2021). The same study also highlighted the risk of student preachers developing vocal difficulties due to limited knowledge on voice protection and prevention strategies (Jayakumar & Yasin, 2021). In addition, Jayakumar and Yasin (2021) emphasize the need for training on voice care and vocal hygiene techniques in students who are future PVUs. Future PVUs can thus already be considered an at-risk group for the development of voice disorders as their vocal demands increase once they enter their occupations (Bȕyȕkatalay et al., 2019; Cielo et al., 2015).
Vocal care often does not form part of the formal curriculum of theology students (Pomaville et al., 2020; Sezın et al., 2018). Considering the vocal demands of the occupation, the lack of formal training in vocal care amongst theology students internationally, and the risk for vocal pathology in the profession, the following research question was posed: What is the knowledge and needs of final-year theology students at a South African institution of higher education regarding voice use and vocal hygiene?
Method
The aim of this study was to determine the knowledge and needs of theology students at a South African institution of higher education on voice and vocal hygiene. Institutional Review Board (IRB) clearance (HUM024/0121) was obtained before data collection commenced. Prior to participation in this study, all participants provided informed consent.
Participants
All 25 final-year theology students at a South African institution of higher education enrolled in the programs of Bachelor of Divination (BDiv) and Masters of Divination (MDiv) during the 2021 academic term were asked to participate in this study. Seventeen students volunteered their participation (N = 17). To answer the question of what the knowledge and needs are among this population, G*Power analysis (Faul et al., 2007) was used. The achieved power was calculated to be 0.562, which is below the ideal value of 0.8. The sample included 10 males (58.8%), and 7 females (41.2%), between the ages of 19 and 40 years (mean 24.65, SD 3.86).
Materials and Procedures
The authors approached the sample population by delivering a brief informational presentation following one of their regularly scheduled lectures. The presentation introduced the researchers, outlined the study’s purpose, and allowed participants to ask questions. Participants who volunteered to participate in the study shared their email addresses, giving consent for the researcher to distribute the survey hyperlink to them via email. Participants were asked to complete the online survey within 3 weeks of the survey link being shared with them.
A linear non-randomized survey was developed by incorporating questions from existing measurement scales used in similar research by Fletcher et al. (2007), Middleton and Hinton (2008), as well as the Vocal Fatigue Index (VFI) version 2 (Nanjundeswaran et al., 2015). The survey consisted of 35 closed and 3 open-ended questions. Four categories of data were collected in the survey (1) demographic information, to obtain background information regarding the participants such as gender, marital status, and history of voice therapy; (2) education and training needs, to obtain insight into the extent of the participants’ exposure to voice and vocal hygiene training, their perception of the importance of good knowledge about voice use and vocal hygiene; (3) knowledge of voice and vocal hygiene, to obtain insight into which factors participants believe might influence their vocal quality; and (4) vocal habits, to obtain insight into the extent of the participants’s daily voice use, the frequency with which participants consume various substances (for example, alcohol, smoking, water), the frequency with which behaviors and symptoms of vocal difficulties occur among the participants, and the VFI.
The VFI consisted of 19 questions which evaluate vocal fatigue in three factors: (1) Fatigue—tiredness of voice and voice avoidance; (2) Pain—physical discomfort associated with voicing; and (3), Recovery—symptom improvement with rest. The VFI raw scores for each factor were calculated and analyzed. Factors 1 and 2 of the VFI indicated a worsening of symptoms of vocal fatigue, and Factor 3 indicated an improvement of vocal fatigue symptoms.
Data Analysis
Inferential statistics were used to draw comparisons within and across survey data using the Statistical Package for the Social Sciences (SPSS) version 27 with a 5% level of significance and sample size of 17 for all statistical tests. The two-proportions z-test was used to test for portions of evidence-based assumptions (Fletcher et al., 2007) between sexes regarding factors influencing voice quality, and non-parametric spearman correlations (rs) were used to test for significant correlations between variables. All qualitative data were analyzed and described descriptively.
Results
More than half of participants (n = 11, 64.7%) indicated that they had not received any education and training on voice use and vocal hygiene. Five participants (29.4%) indicated that they had received some training, of which three received training in the form of informal seminars, one external to their degree program, and one received training as part of their degree program. Of the five participants who reported receiving some training on voice and vocal hygiene only four responded to the follow-up question of when this training was received and whether the training was beneficial to them. Of these four participants, one reported that they received training in their second year of study and three reported receiving training in their third year. Three of the four participants (75%) reported having found this training beneficial.
Almost all participants (n = 16, 94.1%) reported that good knowledge of voice use, and vocal hygiene is important. Most (n = 14, 82.4%) also acknowledged that they think preachers are at high risk for developing vocal difficulties. Furthermore, 15 participants (88.2%) agreed that education and training in voice use, and hygiene should be included in the undergraduate curriculum of theology students. The following reasons for this belief were provided: (1) regular voice use will be an essential part of their future careers; (2) their general lack of knowledge on voice use and hygiene; (3) they were eager to obtain information on how to adequately preserve their voices; and (4) they would like to know how to use their voice optimally. Interestingly, however, only three participants (17.6%) regarded their voices as their primary asset for executing their future occupational duties.
Less than half of the participants (n = 8, 47.1%) indicated that a combination of both formal lectures in their curriculum and informal lectures, such as one-time information talks, should be used in voice training for student preachers. Six participants (35.3%) indicated that voice training should only be delivered through informal methods. The remaining participants (n = 3, 17.6%) indicated that voice training should be delivered formally as part of module requirements.
Participants were asked to rate their perceived influence of various factors on voice quality (Table 1). The measurement instrument used was an interval scale previously employed by Fletcher et al. (2007).
Participants’ Rating of the Influence(s) of Various Factors on Voice Quality (N = 17).

Female participants demonstrated greater awareness than male participants on factors affecting voice quality pertaining to “loud singing” (p = .044) and “good posture” (p = .024).
Three categories of situational voice use were explored: (1) general use, (2) academic use; and (3) social use (Figure 1).

Self-Reported Daily Voice Uses for General, Social, and Academic Purposes (N = 17).
Almost half of participants (n = 8, 47.1%) noted a need to raise their voice when speaking in class presentations to ensure they are heard clearly. Three participants (17.6%) only occasionally felt the need to raise their voice. Participants were asked to report on how frequently they experienced vocal fatigue. Most participants (n = 11, 64.7%) reported not experiencing vocal fatigue at the end of the day, while five participants (29.4%) indicated that they occasionally experienced vocal fatigue (Table 2).
Self-Reported Frequency of Vocal Fatigue (N = 17).
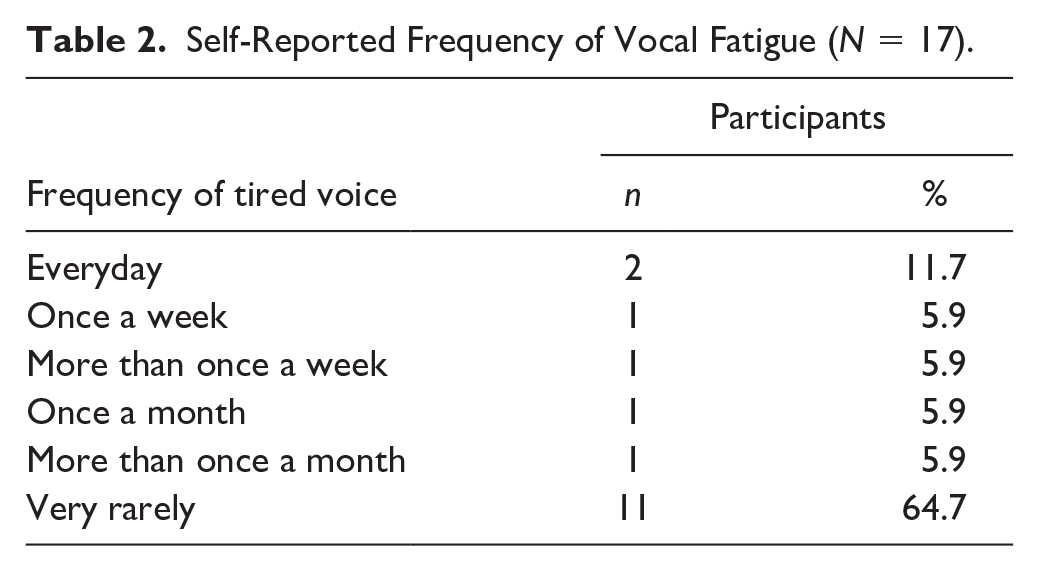
Age did not appear to play a role in the participants’ perception of vocal fatigue (p > .05). One participant (5.9%) reported experiencing vocal fatigue and sore throat at the end of the day, whereas four participants (23.5%) reported only occasionally experiencing a sore throat.
When exploring perceptual voice quality, 11 participants (64.7%) reported experiencing vocal hoarseness or roughness. Most participants (n = 11, 64.7%) reported that hoarseness or vocal problems never affected their social duties, whereas six participants (35.3%) reported that hoarseness or vocal problems only occasionally affect their social duties. The participants were asked how often hoarseness or vocal problems affect their academic duties. Fourteen participants (82.4%) reported no effect of voice quality on their academic duties, whereas three participants (17.6%) reported hoarseness or vocal problems sometimes affecting their academic duties.
Two participants (11.8%) indicated that they smoke more than eight cigarettes a day. The daily consumption of four beverage types—carbonated drinks, caffeinated drinks, water, and alcohol, were evaluated. Most participants (n = 11, 64.7%) reported consuming alcohol occasionally, and seven participants (41.2%) reported not consuming carbonated drinks (Figure 2).

Self-Reported Daily Consumption of Different Beverages (N = 17).
Participants were then asked to rate their vocal health practices during participation in activities requiring extensive voice use. Most participants indicated that they do not warm up their voice before extensive use (n = 15, 88.2%) or cool down their voice after extensive use (n = 16, 94.1%). Eight participants (47.1%) also reported not implementing voice rest after extensive use, whereas seven participants (41.2%) reported occasional voice rest after extensive voice use.
The participants were asked to rate how frequently they encountered vocal difficulties and their associated conditions (Figure 3).
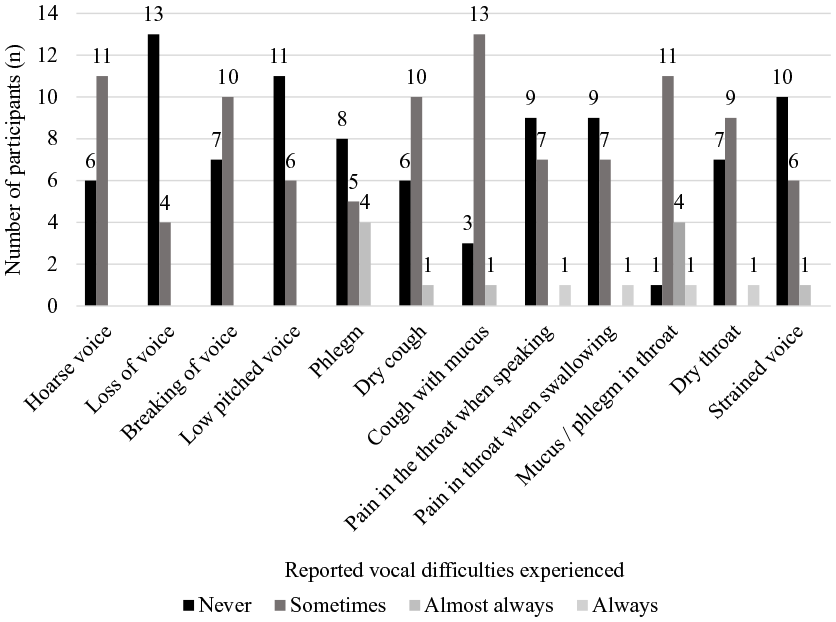
Frequency of Vocal Difficulties Experienced (N = 17).
Participants were then asked to report how often they engage in behaviors associated with phontrauma and misuse (Table 3). However, these behaviors, derived from a previous study, are only considered vocally abusive when they are executed excessively (Middleton & Hinton, 2008).
Self-Reported Frequency of Engaging in Phonotraumatic Behaviors (N = 17).

The VFI (Nanjundeswaran et al., 2015) was administered to gather information regarding the occurrence of vocal fatigue amongst participants. For Factor 1, tiredness of voice and vocal avoidance (mean 12.24, SD 8.30), 11 participants obtained a score between 0 and 14, and six participants obtained a score between 15 and 28. For Factor 2, physical discomfort associated with voicing (mean 4.71, SD 4.85), 15 participants obtained a score between 0 and 10, and two participants obtained a score between 11 and 17. For Factor 3, symptom improvement with rest (mean 6.29, SD 2.87), ten participants obtained a score between 0 and 6, and seven participants obtained a score between 7 and 12. All correlations for each factor of the VFI were statistically significant positive correlations (p < .05). No statistically significant relationship was found between vocal fatigue and participant age (p = .197, rs = .329).
Discussion
A lack of formal vocal training as part of the degree programs under study was confirmed by most participants reporting that they had not received formal education and training on voice use and hygiene. This is supported by literature which found that future PVUs do not receive adequate vocal health training during their education, leading to a need for more vocal health knowledge after graduation (Flynn, 2019). Lack of vocal training may contribute to the development of the vocal pathologies frequently experienced by preachers later in their careers (Carmo et al., 2012). Vocal health education and voice training are considered to be two of the most important strategies to prevent voice disorder and could therefore be implemented as prevention tools for future PVUs specifically (Hazlett et al., 2009). This is significant as research collectively highlights that PVUs demonstrate improved vocal hygiene and health after vocal health education and training (Hazlett et al., 2009; Middleton & Hinton, 2008; Timmermans et al., 2005).
The participants indicated that hoarseness does not negatively affect their social (n = 11, 64.7%) or academic participation (n = 14, 82.4%). This contradicts previous research, which found that students engaged in preaching courses are an undiscovered population of PVUs with a high prevalence of vocal duties (Jayakumar & Yasin, 2021). The students in the aforementioned study were, however, found to be exposed to higher vocal demands during academic activities than during social activities (Jayakumar & Yasin, 2021). This study did not extensively explore the specific vocal demands experienced by this study population. Future research could thus help to obtain a more detailed understanding of what the specific social and academic demands experienced by the population are.
It is evident that the participants appeared to have good knowledge regarding the effects of voice rest (n = 16, 94.1%) and talking (n = 16, 94.1%) with a tired voice. The negative effects of vocal misuse, including frequent coughing (n = 15, 88.2%), screaming (n = 15, 88.2%), and talking with a sore throat (n = 15, 88.2%), were mostly known to participants. More than half of participants (n = 9, 52.9%) were unaware of the adverse effects that throat clearing (n = 9, 52.9%), consumption of carbonated drinks (n = 9, 52.9%), and the presence of a noisy environment (n = 9, 52.9%), can have on their voice. Most participants (n = 15, 88.2%) were unaware of the potential negative effects of whispering. This indicates poor knowledge of vocal health and hygiene among participants in this regard. The development of targeted intervention programs to provide the necessary education and training for participants as future PVUs could help to reduce their risk of developing vocal pathologies (Hazlett et al., 2009; Middleton & Hinton, 2008; Timmermans et al., 2005). A pretest, posttest research study could be conducted in future to help study the effect of education and training on this topic among members of the study population.
Female participants demonstrated greater awareness pertaining to loud singing (p = .044) and good posture (p = .024). This can be viewed as a positive development of vocal knowledge and could influence their voice use as future PVUs. Benninger et al. (2016) states that PVUs often injure their voices with continued voice use while sick, fatigued, or under strain. Therefore, this highlights the importance of knowledge regarding voice rest for future and current PVUs.
Participants in this study reported rarely experiencing vocal fatigue. These findings could be attributable to most participants being young and not yet having to use their voices to execute occupational obligations as students. This vocal demand might, however, increase once they enter the profession. Vocal fatigue has been described in several ways, such as a list of symptoms present in an individual or concerning physiological characteristics derived from increased vocal use (Nanjundeswaran et al., 2015). The researchers did not provide the participants with a definition of vocal fatigue in this survey and should therefore be further explored in future research.
Most participants indicated that voice use in a noisy environment does not negatively impact their voice, while the majority also indicated that they infrequently or never speak in noisy environments. This could either indicate that (1) the participants are aware of the effects that speaking in a noisy environment can have on their voice or (2) that the participants are unaware of what constitutes a noisy environment for voice production and thus do not know when they are using their voices in such an environment. A noisy environment is typically believed to be one in which environmental factors cause noise levels to exceed 85 A-weighted decibels (dBA) resulting in increased vocal effort to be heard, difficulty having a conversation, or the exertion associated with producing vocalizations at greater intensities over extended periods of time (Chan, 1998; Edwin & Priscilla, 2015). A systematic review found that noisy environments affect vocal behaviors by causing people to speak louder, placing excessive strain on the larynx and vocal folds (Toki et al., 2021). This could lead to increased organic vocal difficulties, negatively impacting occupational performance and overall quality of life (Toki et al., 2021). Future research can focus on determining what this population understands regarding what constitutes a noisy environment for voice production. Most participants (n = 11, 64.7%) reported that they were never exposed to environmental irritants. Environmental irritants such as pollution exposure and temperature changes contribute to dehydration of the mucosal lining of the vocal folds, increasing the risk for the development of vocal pathology and therefore interfering with vocal health (Carmo et al., 2012; Lobo et al., 2017). These results indicate that the participants may be unaware that they are exposed to environmental irritants on a daily basis and that there is a lack of knowledge on environmental risk factors and the effects thereof on voice production.
A gap was identified between knowledge of vocal health and practical application of this knowledge among the participants. Fourteen participants (82.4%) reported knowing that warming up their voice before extended voice use was important. However, most participants reported not warming up their voices before extended voice use (n = 15, 88.2%). This knowledge-practice gap should be addressed in future education and training programs for this population. Vocal warm-ups are effective for improvements in overall vocal quality, improved vocal performance, reduced recovery times after extended voice use, and self-perceived overall improvement in general vocal health (Ragan, 2016; Van Lierde et al., 2011).
Singing forms part of the occupational duties of preachers (Lobo et al., 2017). This may explain why most of the participants (n = 14, 82.4%) reported singing either occasionally or frequently. Although singing has been related to positive well-being, preachers may have to participate in prolonged singing sessions that can be regarded as vocally demanding, requiring them to maintain strong, clear voices for extended periods (Kang et al., 2018; Kwok & Eslick, 2017). The majority of the participants (n = 12, 70.6%) knew about the harmful effects “loud (or excessive) singing” can have on their voice. Female participants were significantly more aware of this than male participants (n = 7, 41.9%, p = .044). This sex difference may be related to the way in which males and females perceive the use of effortful voice, respectively (Hunter & Banks, 2017). Research has found that females are more likely to change their voices according to their environment and make use of more effort in doing so (Bottalico, 2017; Bottalico et al., 2016). Therefore, the sex difference could be attributable to females singing in a more effortful way than males and being more aware thereof (Hunter & Banks, 2017).
Evidence shows that excessive whispering can have a negative effect on voice quality, as it could lead to supraglottic hyperfunction (Rubin et al., 2006). The participants of this study’s lack of knowledge are evident in this domain, as a majority (n = 15, 88.2%) reported that whispering does not affect their voice quality. Consequently, this might also indicate that they would not consider the effects of excessive whispering on voice production. These results indicate a need for future education and training in this population. Seeing that most of the participants (n = 13, 76.5%) did not engage in loud talking during respiratory infections, is of satisfactory value [9, 20, 33].
Lifestyle behaviors such as the consumption of tobacco, caffeine, alcohol, and high-fat and acidic foods may lead to gastroesophageal reflux disease (GERD), where stomach contents enter the esophagus and, in certain instances, reach the pharynx resulting in laryngopharyngeal reflux (LPR) (Mendell & Logemann, 2002; Taraszewska, 2021). A connection between LPR and voice exists, but the precise strength and nature of this relationship remain unclear, and warrants further examination (Schneider et al., 2016). Furthermore, alcohol consumption and cigarette smoking increases the risk for developing head and neck cancer in the oral cavity, larynx, and hypopharynx (Maasland et al., 2014). These evidence-based assumptions (Fletcher et al., 2007) appear to be known by the research participants as most of them reported knowing that smoking and alcohol consumption have a negative effect on vocal hygiene. Research regarding student preachers and substance use is limited, but these results are consistent with other studies on PVUs such as singers (Ferreira et al., 2009; Santos et al., 2019). Although student preachers in this study did not make such a connection, the consumption of coffee, tea, or carbonated drinks can exacerbate reflux symptoms (Taraszewska, 2021). Research has also noted acoustic variations in voice following acidic beverage consumption, along with reported voice discomfort 1 hour later (Barbieri, 2021). Although the participants in this study did not report consuming carbonated drinks frequently, the daily intake of caffeinated beverages was still reported to be high. Contrary to traditional vocal hygiene practices suggesting the avoidance of caffeine due to its perceived dehydrating effects on the voice, recent studies have found that moderate caffeine intake, up to 480 mg, does not negatively impact voice production (Weston & Schneider, 2023). Despite extensive research, the precise impact of lifestyle, diet, and eating habits on reflux and voice remains ambiguous, with conflicting findings (Taraszewska, 2021) warranting further research. The majority of participants (n = 14, 82.4%) indicated that sucking on medicated throat tablets, such as menthol lozenges, does not negatively influence voice quality. Although the employed measurement tool’s “evidence-based outcomes” as set out by Fletcher et al. (2007) states that this is an incorrect statement and that this behavior does negatively affect voice quality, a more recent cross-sectional observational study uncovered a notable prevalence of menthol-containing cough drop use among individuals with cough illnesses, where higher menthol exposure was associated with increased cough severity (Johnson et al., 2018). More than half of the participants (n = 9, 52.9%) indicated that throat clearing does not impact voice. This could indicate an apparent lack of proper knowledge of vocal hygiene that needs to be addressed in future education and training programs for this population.
All correlations for each factor of the VFI were statistically significant positive correlations (p < .05). Thus, if participants achieved a high score in one VFI factor, they also achieved a high score in the other two VFI factors. Conversely, if they achieved a low score in one VFI factor, they also achieved a low score in the other two VFI factors. This could indicate that the participants were aware of vocal fatigue symptoms and that they could improve after periods of voice rest. Alternatively, these results could also reflect natural spontaneous physiological recovery that occurs between intermittent periods of high vocal demands. This could be further explored in future research on this population. No statistically significant (M: 24.65, SD 3.86, p > .05) relationships were found between vocal fatigue and participant age, which is consistent with the findings of Hunter and Banks (2017), who reported an almost zero coefficient for all factors compared to their participants’ ages. Age, therefore, does not appear to influence the probability of this population experiencing vocal fatigue. No statistically significant (p > .05) relationships were found between vocal fatigue and phonotraumatic behaviors reported by the participants. This warrants further investigation in future research.
The small sample size obtained in this study could be a result of the limited scope of this study’s sample population. Only 25 students were sampled from one institution of higher education. This negatively affects the generalizability of the results obtained to the larger theology student population. Future research based on the knowledge and needs amongst this population should therefore focus on obtaining a larger sample size by including participants from Theology programs at other South African institutions of higher education. The survey employed in this study lacked comprehensive variables assessing vocal hygiene practices. Future research concerning this population or topic should enhance the survey by incorporating a broader range of variables to gauge participants’ vocal hygiene habits and the need for further education and training on this topic in more depth. Furthermore, the focus of these studies should be expanded to obtain evidence-based intervention programs for remedying this need.
Conclusions
The findings of this study suggested a need for the inclusion of formal education and training regarding vocal health and hygiene in the curriculum of student preachers. As discussed, the participants’ low self-reporting of symptoms of vocal fatigue, and a limited effect of environmental factors on their current vocal performance, may be as a result of poor knowledge of what exactly constitutes symptoms of vocal fatigue as well as what effects various environmental factors could have on their voice production. The need for such training among the students is therefore strongly emphasized as this educational gap exposes the students to an increased risk for the development of vocal fatigue, vocal hyperfunction, and subsequent vocal pathologies throughout their prospective careers as preachers. A potential solution entails modifying the curricula of the BDiv and MDiv programs at the South African institution of higher education to include comprehensive education on vocal health, voice training, and prevention of vocal injury. Speech-language pathologists could have a significant role to play in advocating for this need. Furthermore, SLPs could also contribute to the development of intervention programs to satisfy this need in the formal education of preachers.
This study also found that student preachers have limited knowledge about vocal health and hygiene which did not translate into everyday vocal health and hygiene practices. It is currently unknown how the students obtained this knowledge, or why they do not utilize this knowledge in everyday practice. Future research in this population should focus on why student preachers might not apply this knowledge. Furthermore, future research should prioritize exploring strategies aimed at enhancing the implementation of knowledge pertaining to voice and vocal hygiene within this population, with the goal of mitigating their susceptibility to the development of vocal pathologies.
Footnotes
Data Availability
Ethical Approval
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.